Labor
1/183
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
184 Terms
Why does labor start?
- fetal hormones release
- uterine distention, pressure, and aging placenta = myometrial irritability
- progesterone decreases, estrogen and prostaglandins increase
What does progesterone do to smooth muscles?
relaxes them
What are signs that labor is coming?
- lightening
- bloody show
- passage of mucus plug
- possible rupture of membranes
- nesting
- weight loss
- diarrhea, indigestion, n/v
Lightening
Baby dropping to pelvis, putting pressure on cervix
Bloody show
blood tinged material that is a result from the capillaries in the cervix starting to break (NOT BLOOD)
Passage of Mucus Plug
physical and chemical barrier that is held in by cervix
Might come out a week or two before labor starts
Nesting
burst of energy toward end of pregnancy to prepare for baby arrival
Why is their weight loss toward labor?
because baby is taking over abdomen and stomach cannot expand as much; baby hungry all the time
What is the one thing you have to have for it to be true labor?
cervical change
What are the signs of true labor?
- contractions at regular intervals that become more frequent and increase in intensity and duration
- discomfort starts in lower back and radiates around to abdomen
- increased activity increases progression; frequency, duration, and intensity of contractions increase despite rest/relaxation
- CERVICAL CHANGE
cervix is effacing, dialated, showing progress toward delivery
Describe contractions of true labor
at regular intervals that become more frequent and increase in intensity and duration
What does false labor look like?
- contractions are at irregular intervals with little to no change in frequency and little to no change in intensity and duration
- discomfort is usually in the abdomen
- rest or activity has little effects on contractions
- no cervical change
Describe contractions of false labor?
at irregular intervals with little to no change in frequency and little to no change in intensity and duration
What are maternal cardiovascular physiological adaptation to labor?
- increased BP during uterine contractions
- avoid supine hypotension
Why do we have higher BP during uterine contractions?
- muscle fibers in uterus constrict around mom's spiral arteries that supply the placenta -> shunts mom's blood back to her circulation
- pain of contraction
How to avoid supine hypotension?
lots of positional changes
What are maternal hematologic system physiological adaptation to labor?
increased WBC
Why do we see increased WBCs during labor>
body is amounting defenses against infection bc there is a high risk of infection during labor
What are maternal respiratory physiological adaptation to labor?
- high stress, oxygen consumption
- hyperventilation
What are maternal GI physiological adaptation to labor?
- decreased motility, absorption
- aspiration risk with general anesthesia
- n/v
What foods do we give mom during labor?
light snacks
What are maternal renal physiological adaptation to labor?
- up to +1 protein WDL
- full bladder will impeded infant's descent
- decreased bladder emptying
Why do we want to keep mom's bladder empty during labor?
because full bladder will impeded infant's descent, which acts as a road block for baby
What nursing intervention do we do with an epidural?
place foley catheter (bc mom might not feel urge to pee) and remove it when they start to push
What are maternal neurological physiological adaptation to labor?
- emotional changes
- endorphin surge
What are maternal endocrine physiological adaptation to labor?
- metabolism increases
- glucose decreases
How often should cervical assessment be done?
only as necessary and with sterile gloves, especially ROM
What are the cons of cervical assessment?
- can introduce infection
- uncomfortable
- we don't know what the person has gone through
Dilation
cervix starts at 0 cm, or "closed" and must get to 10 cm to be "complete"
Effacement
cervix also needs to go from thick, closed (0% effacement) to paper thin, complete (100% effacement)
100% Effacement and 10 cm Dilation
if plate cervix, all you feel is baby head
When would cervical assessment be contraindicated?
- placenta previa
- bleeding
- sparingly with preterm labor pts
- pt declines
Why is a cervical assessment contraindicates with placenta previa?
if placenta is close to cervix and you go poking around, you can poke a hole in it and cause a lot of issues
Why is a cervical assessment contraindicated with bleeding?
bc could mean placenta previa (get more info!)
What are the stages of labor?
1. Onset of labor to 10 cm
2. 10 cm to birth
3. Birth to delivery of placenta
4. Approximately 2 hrs after placental delivery
Describe the latent phase of labor
- 0-6 cm dilated, mild discomfort
- can take hours to days
- contractions gradually increase in frequency, duration, and intensity
- roughly 5 mins apart toward end of phase
- possible SROM, AROM
- patient initially feels excited,e easily follows directions
What are the 2 phases of stage 1 of labor?
latent phase and active phase
When is the latent phase?
earlier in stage 1 --> 0-6 cm dilated, mild discomfort
How long can the latent phase last?
hours to days
Describe contractions during the latent phase of labor
gradually increase in frequency, duration, and intensity; roughly 5 mins apart toward end of this phase
SROM
water breaks on its own, spontaneously
AROM
provider breaks water
When is the active phase of stage 1?
after Latent phase --> 6 to 10 cm dilated, more painful
How often are contractions during the active phase of labor?
q 2-5 mins
When do we typically give an epidural?
Stage 1 (Onset of labor to 10 cm); Active Phase
Describe the active phase of labor
- 6 to 10 cm dilated more painful
- contractions q 2-5 mins
- typical time for epidural
- fetal descent is progressive
- more anxiety; has to focus
What do we see by the end of phase 1 (Onset of labor to 10 cm)?
- bloody show
- shaking, irritable, tired, may feel out of control
- rectal pressure, urge to push have BM
- n/v
Describe Stage II (10 cm to birth)
- may "labor down"
- duration greater in nulliparas bs multiparas
- bulging perineum; bursning sensation
- sense of relief with pushing
- contractions may cause involuntary pushing
- offer many positions for pushing
- monitor maternal breathing
- lots of encouragement needed (mom and support person)
Labor Down
take a rest from pushing and let the uterus do the work
Describe contractions during stage II
cause involuntary pushing
What do we want to monitor in stage II of labor?
maternal breathing
How fast is stage III (birth to delivery of placenta) of birth?
should be completed within 30 mins of birth of baby
What are the signs of placental separation?
- spherical shape of uterus
- firm funds/fundal rise in abdomen
- gush of dark blood
- descending umbilical cord
What does a retained placenta mean?
hemorrhage
What happens during stage IV (delivery of placenta through 1-4 hrs after birth) of labor?
- blood redistribution into venous beds
- shaking chill
- assess for urinary retention
- assess for s/sx of hemorrhage
- assess pain
- promote bonding
What might we see d/t blood redistribution into venous beds?
monitor BP drop and moderate tachycardia
What do we assess during stage IV (delivery of placenta through 1-4 hrs after birth) of labor?
- urinary retention
- s/sx of hemorrhage
- pain
What are the 5 Ps of labor?
passageway, passenger, powers, position, psychological response
How can we asses the passenger?
external abdomen assessment
internal vaginal assessment
well-being assessment
What does the external abdominal assessment of the passenger consist of?
fetal lie
fetal presentation
fetal attitude
leopold's maneuvers
ultrasound
fetal heart location
External abdominal assessment: fetal lie
mom's spine in relation to baby's spine
How do we want baby to lie in relation to mom's spine?
longitudinal lie
What would a transverse or oblique lie result in?
c-section
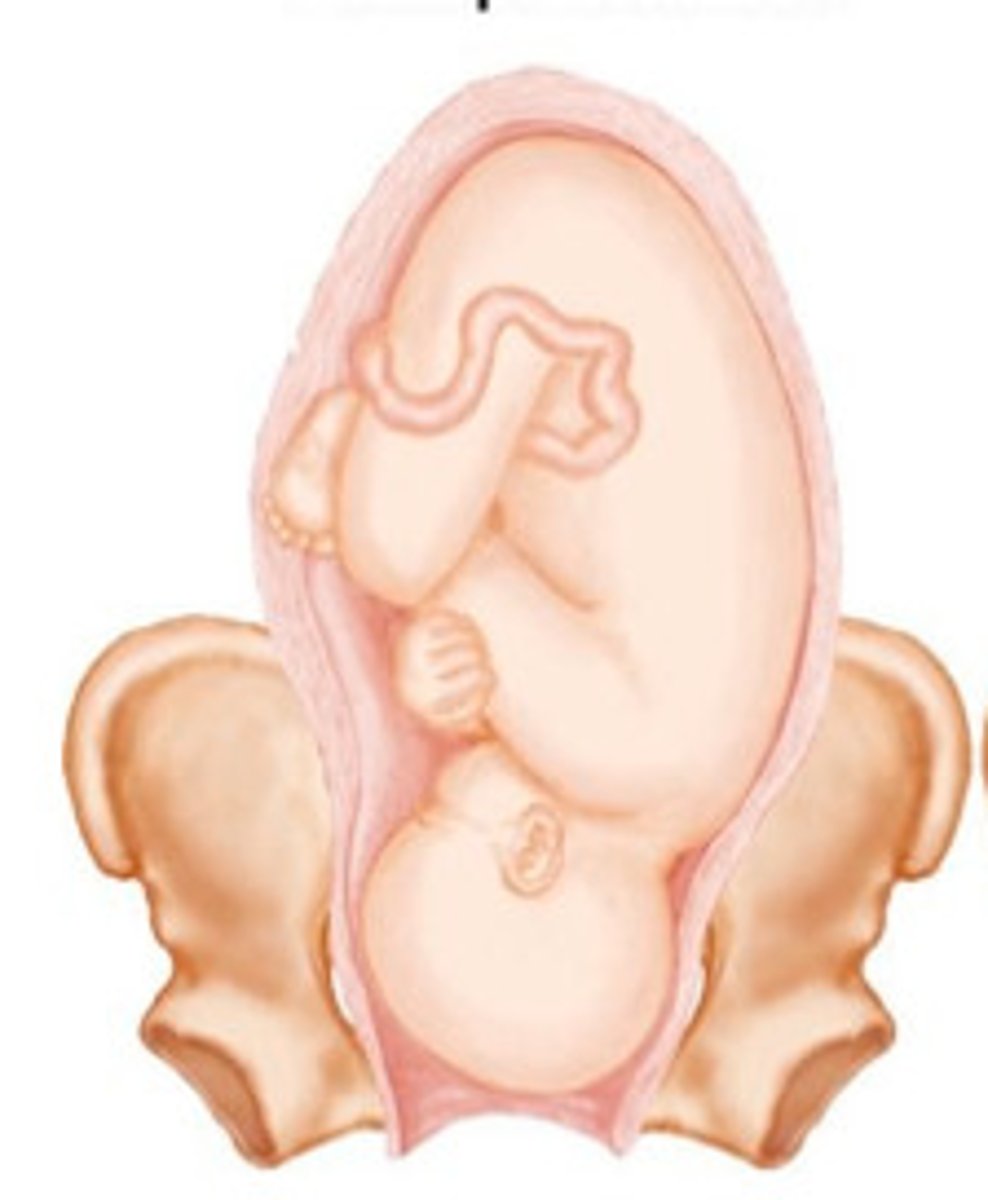
External Abdominal Assessment: Fetal Presentation
fetal body part that enters the pelvis first
What type of fetal presentation do we want?
cephalic
What does a cephalic fetal presentation mean?
head comes out first; longitudinal lie
Breech Presentation
butt is down, coming out first

Shoulder Presentation
shoulder is heading toward the pelvis
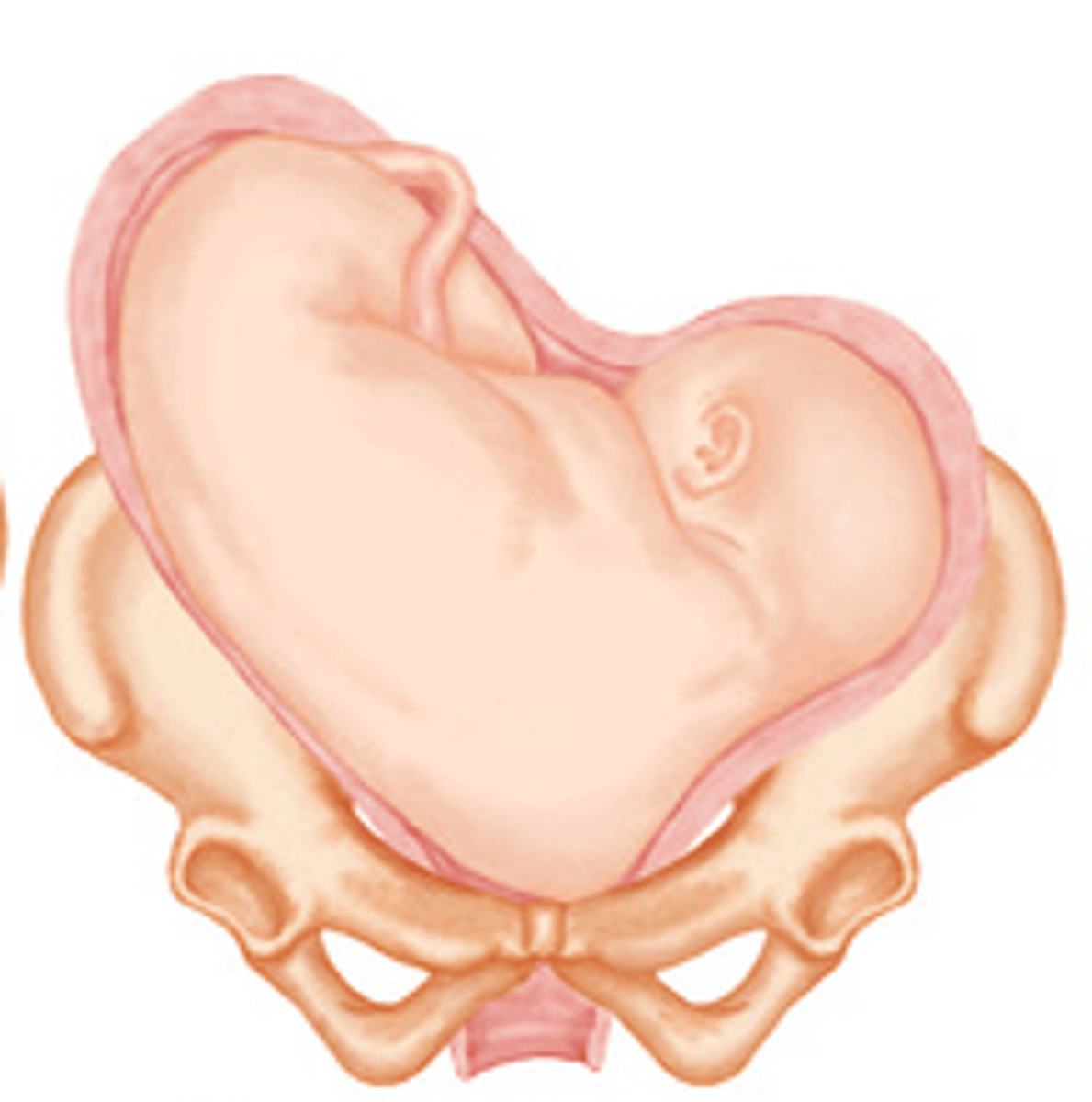
What type of delivery will happen with a breech or shoulder presentation?
c-section
External Abdominal Assessment: Fetal Attitude
what is the baby's head position?
What is the ideal position for baby to be in when head down?
flexed (chin to chest)
Rank the position for baby to be in when head is down
1. Flexed
2. Neutral
3. Brow
4. Facial/Mentrum
What is the fancy word for head down and flexed?
vertex postion
External abdomen Assessment: Leopold Maneuvers
4 step process to palpate baby's position
Describe the 4 step process to palpate baby's position
1. What passenger part is in the fundus?
2. Fetal lie: where is baby spine?
3. Fetal presentation: What is by the pubic bone? Engaged or floating?
4. Which way is baby facing?
If a nurse is palpating to see what passenger part is in the fundus, what will a head feel like?
rounded and firm
If a nurse is palpating to see what passenger part is in the fundus, what will a breech position feel?
lumpy, soft, foot?
How does a baby's spine feel?
curved and bumps
What's the whole point of doing leopold maneuvers?
1. wanna know if there is a safe setup for vaginal delivery
2. help determine where we might start to find the maximal impulse
Where is the maximal impulse for babies in utero?
upper back
Where do we listen for heart if baby is breech?
right and left upper quadrant
Where do we listen for heart if baby is in cephalic?
right and left lower quadrant
Fetal Position
relationship between the designated landmark on the presenting fetal part and the front, sides, and back of the maternal pelvis
How is fetal position documented?
with three letters describing the landmark's direction, presenting part, and location in the mother's pelvis
What does the first letter of fetal position indicate?
whether the landmark is directed toward the left (L) or right (R) side of the mother's pelvis
What does the second letter of fetal position indicate?
the presenting part or landmark of the baby
What does the third letter of fetal position indicate?
whether the landmark is directed anterior (A), posterior (P), or transverse (T) in the mother's pelvis
What is the landmark for a vertex presentation?
occiput (O)
What is the landmark for a face presentation?
mentum (M)
What is the landmark for a breech presentation?
sacrum (S)
What is the landmark for a shoulder presentation?
scapula (Sc)
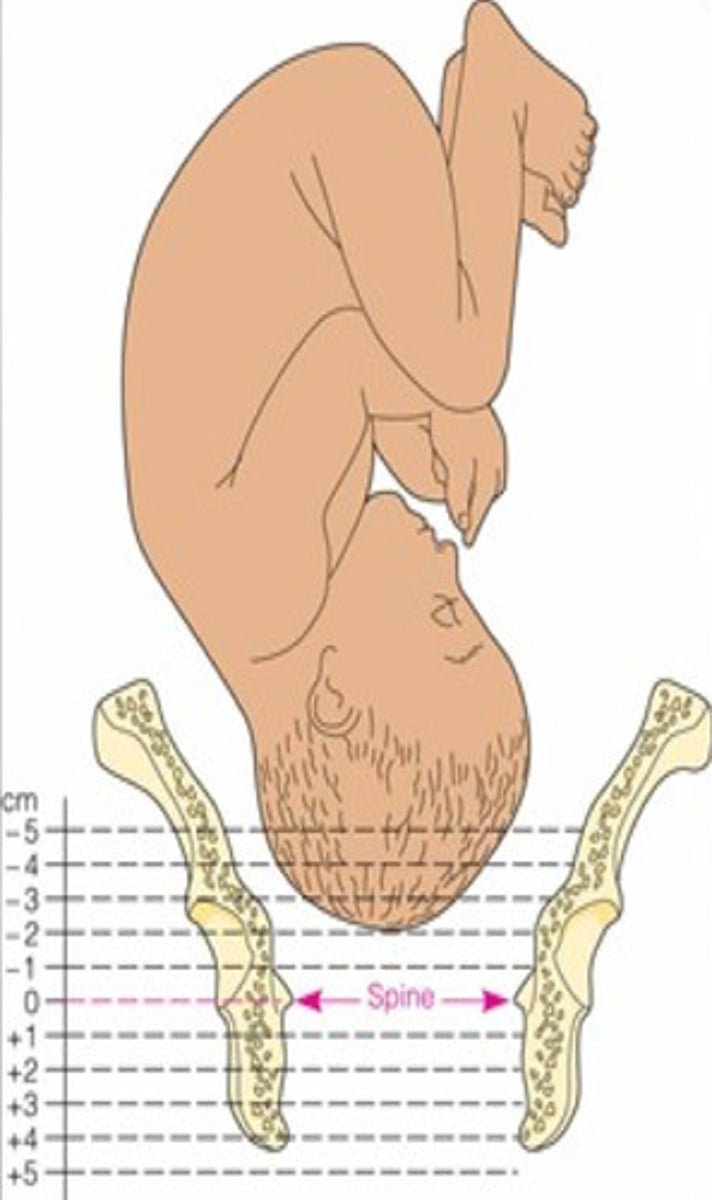
Internal Vaginal Assessment: Fetal Station
represents fetal descent into the pelvis
What is fetal station measured in relation to?
an imaginary line drawn between the ischial spines of the maternal pelvis
What is the interspinous diameter?
the narrowest part of the pelvis between the ischial spines
What does zero station indicate?
the presenting part is engaged at the level of the ischial spines
What do negative station numbers indicate?
the presenting part is above the ischial spines
What do positive station numbers indicate?
the presenting part is below the ischial spines, moving toward delivery
Simply explain the numbering system of fetal station
negative numbers mean higher up; meanwhile positive numbers mean lower down (e.g. +4 on the floor)
What allows the baby's head to mold during birth?
the flexibility of the skull bones and suture lines
What are the main components of the passageway in labor?
the pelvic inlet, pelvic cavity, and pelvic outlet