Other Extraoral Views
1/17
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
18 Terms
lateral cephalometric
-ortho use for treatment planning
-need soft tissue shadow for orthognathic measurement analysis^
-an aluminum wedge filter is set up at the tube head and absorbs some of the radiation to allow visualization of facial soft tissues
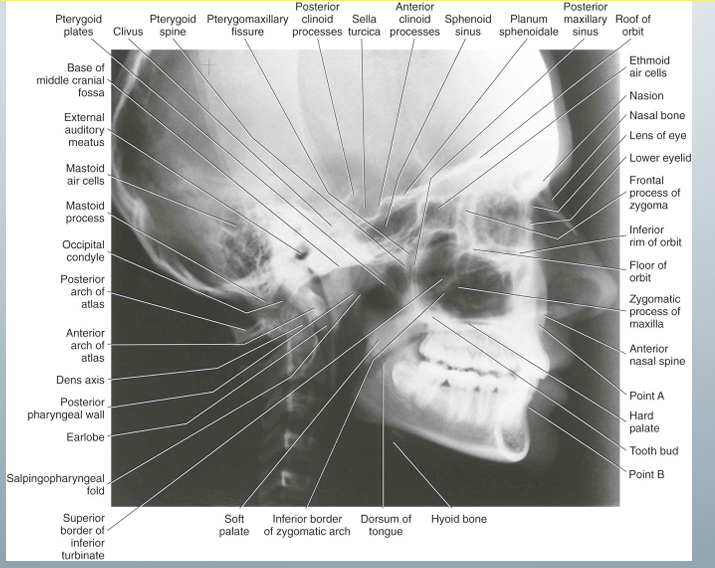
most common skull view in dentistry
-lateral ceph
-lateral ceph v. lateral skull: ceph has the cephalostat to maintain a constant relationship among skull, image detector, x-ray beam
-exact superimposition of the right and left sides would not be possible because of projection geometry
-structures near the image receptor will be less magnified than the same structures on the side away from the image receptor
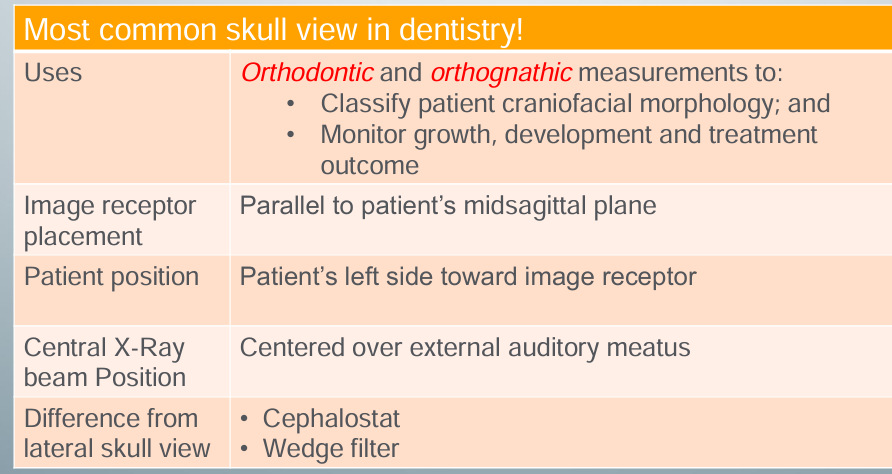
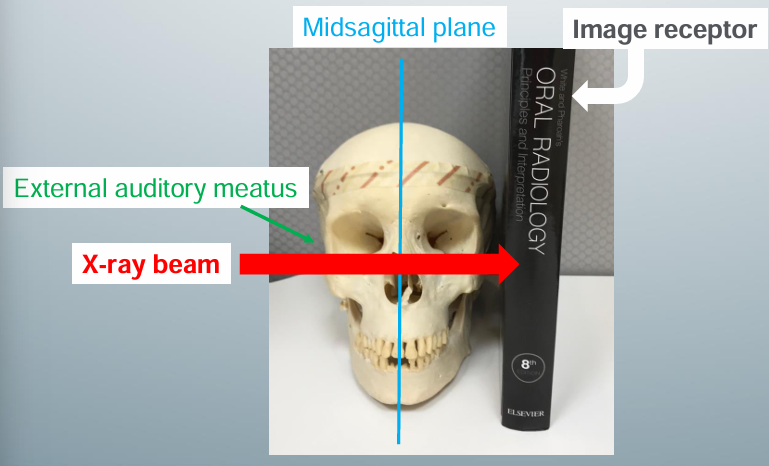
how to take lateral ceph
-image receptor parallels the patient’s midsagittal plane
-central x-ray beam centered over the external auditory meatus
posteroanterior cephalometric
-”PA ceph”
-ortho uses to evaluate facial asymmetry
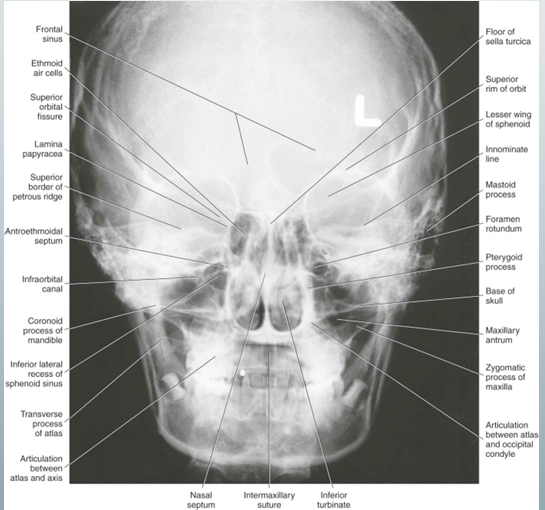
PA ceph uses, image receptor placement, pt position, central x-ray beam position, difference from PA skull view
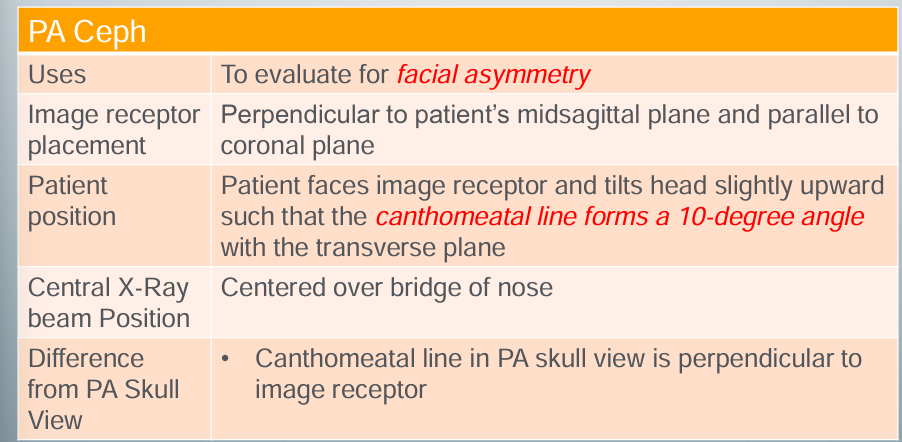
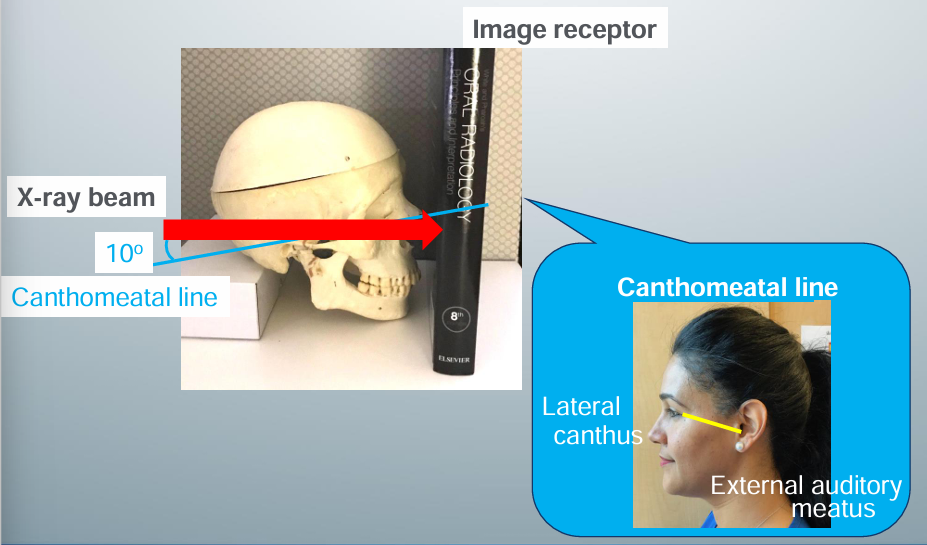
how to take PA ceph
-image receptor perpendicular to pt’s midsagittal plane and parallel to coronal plane
-pt faces image receptor and tilts head slightly upward so the canthomeatal line forms a 10 degree angle with the transverse plane
-central x-ray beam positioned centered over the bridge of the nose
-canthomeatal line: line between the lateral canthus and the external auditory meatus
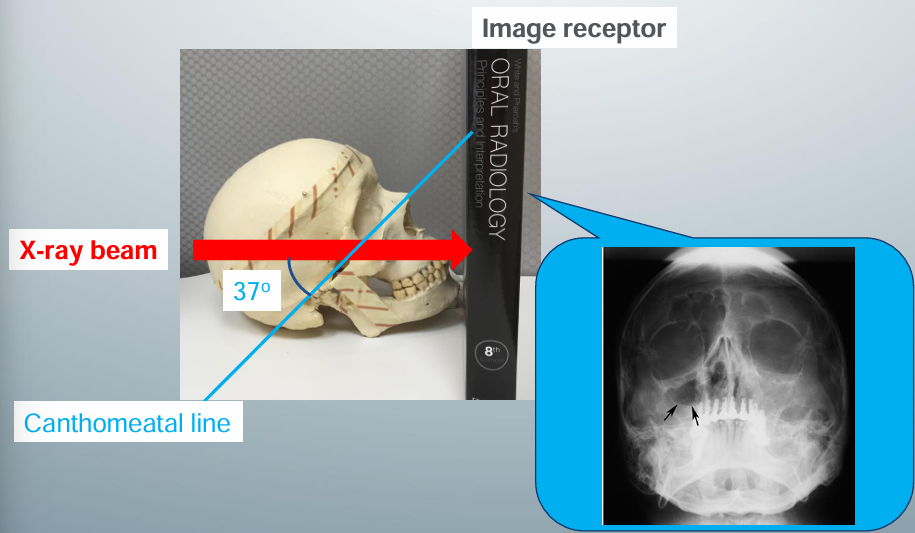
Waters view
-used to evaluate maxillary sinuses (can see without obstruction)
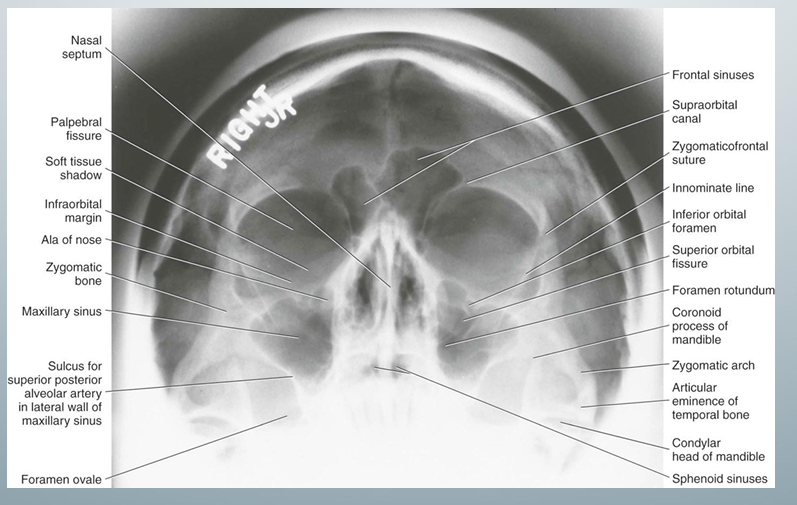
Waters view- uses, image receptor placement, pt position, central x-ray position, notes
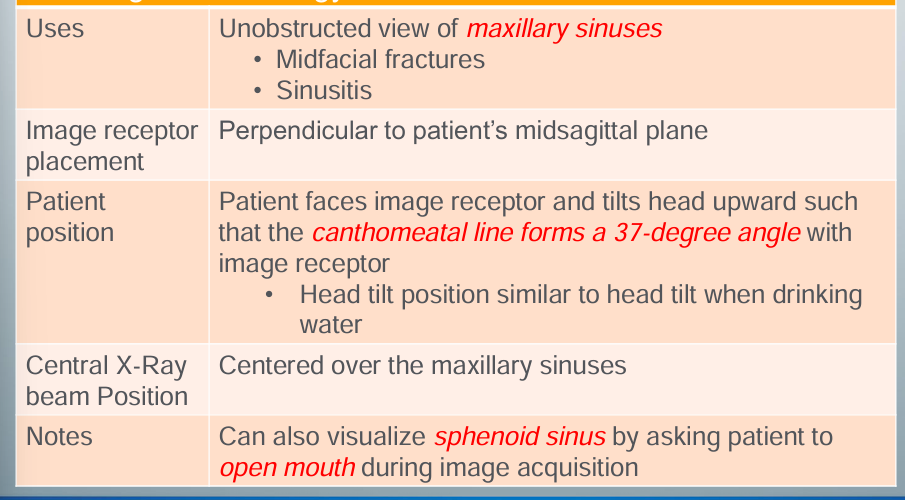
how to take waters view
-image receptor perpendicular to pt’s midsagittal plane
-pt faces image receptor and tilts head upward so the canthomeatal line forms a 37 degree angle with the image receptor
-head tilt position similar to head tilt when drinking water
-central x-ray beam positioned centered over the maxillary sinuses
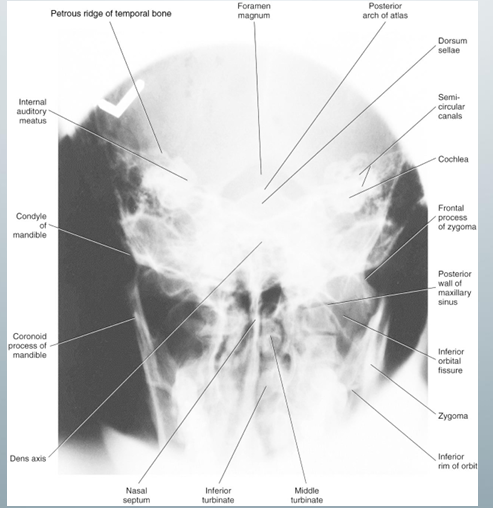
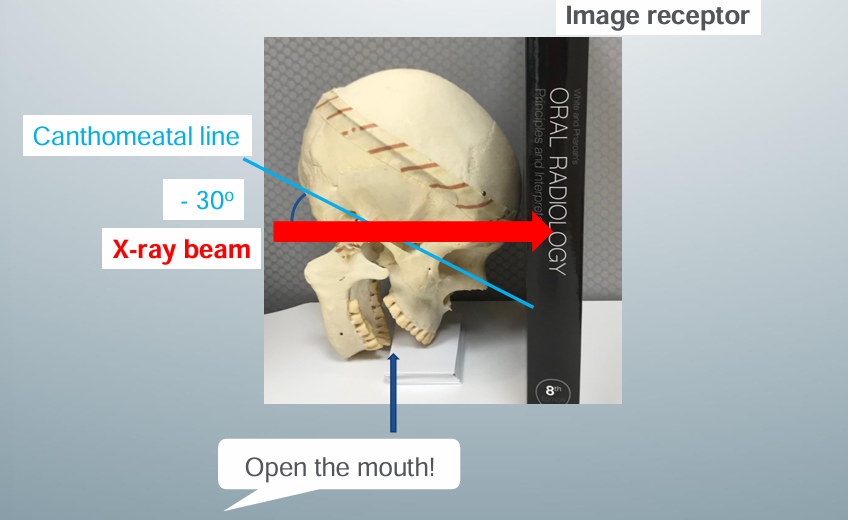
Reverse-Towne view
-used to investigate mandibular condyles
-always ask t to open the mouth because a closed mouth would not be useful for condylar assessment (would get occiput and/or skull base view)
Reverse-Towne view- uses, image receptor placement, pt position, central x-ray beam position, notes
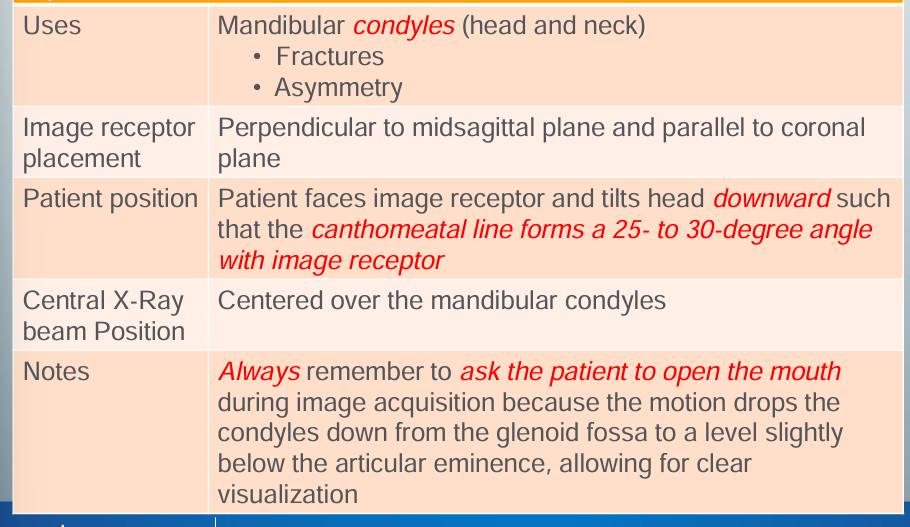
how to take Reverse-Towne view
-image receptor perpendicular to midsagittal plane and parallel to coronal plane
-pt faces the image receptor and tilts head downward so the canthomeatal line forms a 25 to 30 degree angle with the image receptor
-central x-ray beam positions centered over the mandibular condyles
-always ask pt to open mouth because the motion drops the condyles down from the glenoid fossa to a level slightly below the articular eminence, allowing for clear visualization
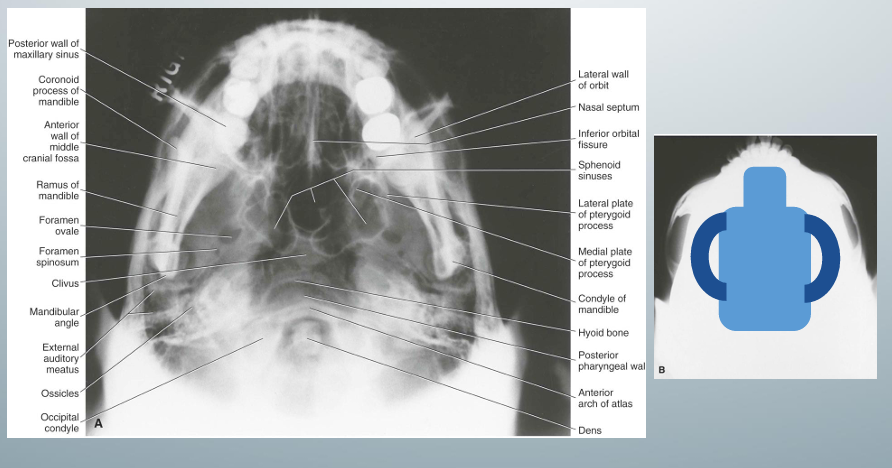
submentovertex view
-”jug handle view” because zygomatic arches stand out like the handles of a jug handle
-used for zygomatic arch fracture evaluation
-underexposure recommended to visualize zygomatic arches well
submentovertex view- uses, image receptor placement, pt position, central x-ray beam position, notes
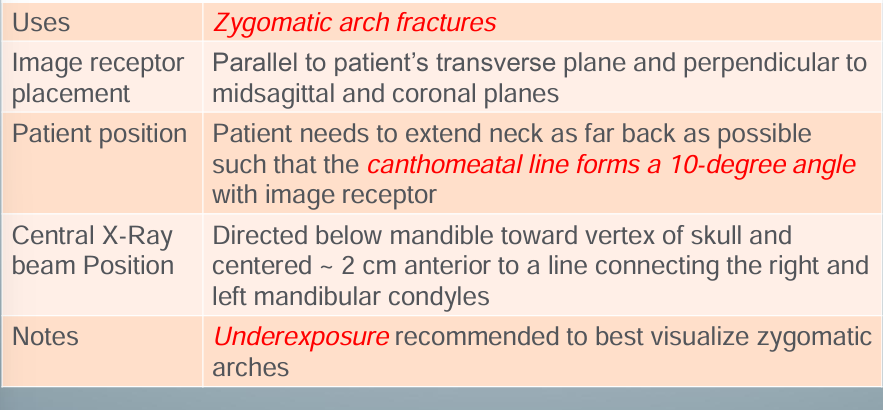
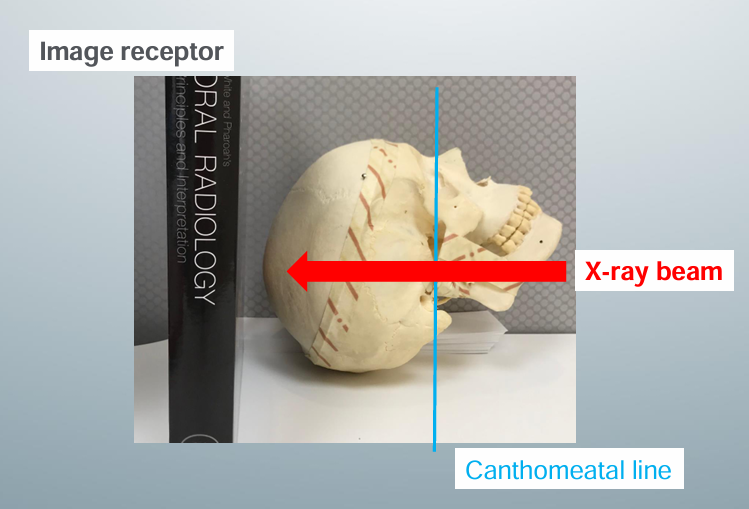
how to take submentovertex view
-image receptor placed parallel to pt’s transverse plane and perpendicular to the midsagittal and coronal planes
-pt needs to extend neck as far back as possible such that the canthomeatal line could form a 10 degree angle with image receptor
-central x-ray beam position directed below the mandible toward the vertex of the skull and centered to 2cm anterior to a line connecting the right and left mandibular condyles
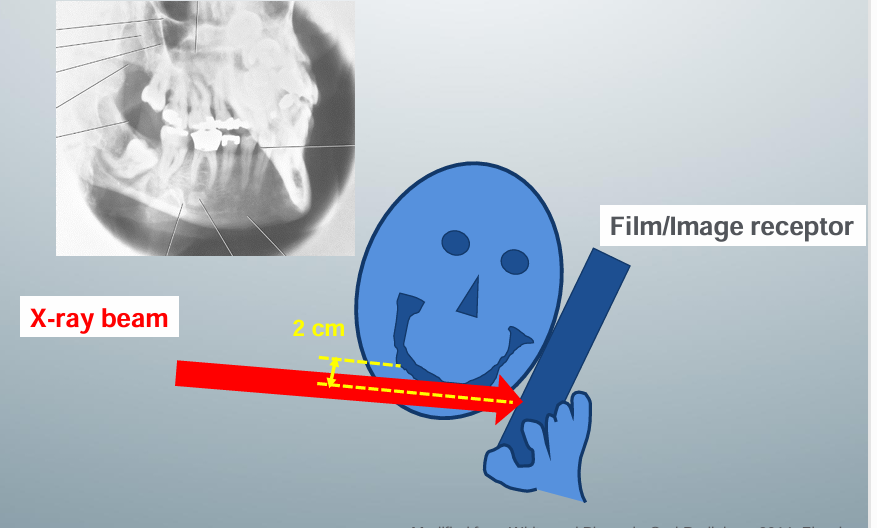
mandibular oblique lateral views
-used to evaluate mandibular body and ramus
-inferior border of the image receptor parallel and at least 2 cm below the inferior border of the mandible so that the image receptor can cover the entire mandibular body and ramus
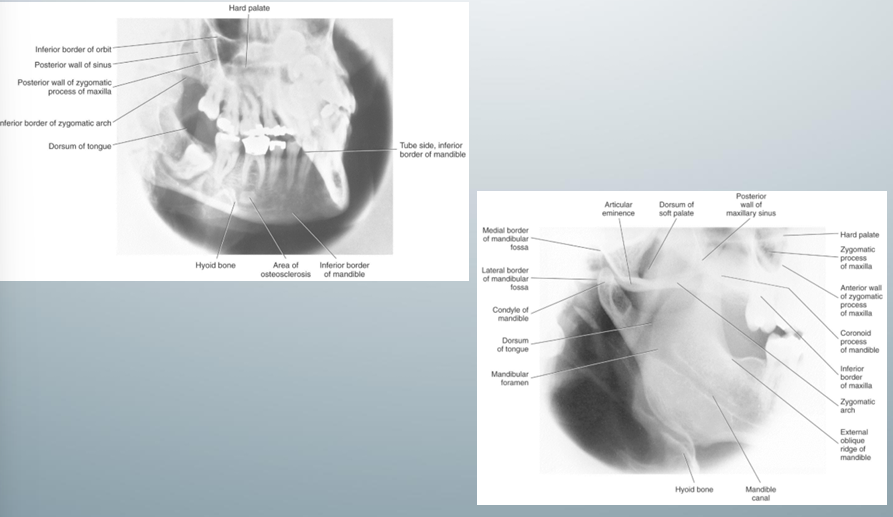
mandibular oblique lateral views- uses, image receptor placement, pt position, central x-ray beam position
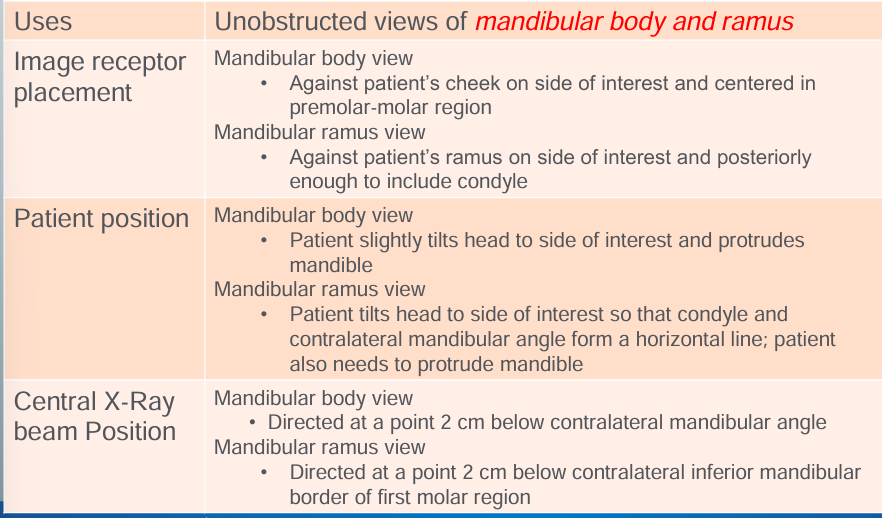
how to take mandibular oblique lateral views
-image receptor placed against the pt’s cheek on the side of interest and centered in the premolar-molar region
-pt slightly tilts head to the side of interest and protrudes mandible
-central x-ray beam positions are directed at 2cm below the contralateral mandibular angle