household toxicity, pesticides, hydrocarbons and rodenticides
1/39
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
40 Terms
compare between acids and alkalis toxicity type, mechanism and depth
acids: coagulative necrosis, forms eschae limits penetration, self limiting, located in Stomach
alkali: liquefactive necrosis, saponification of fats allowing continued penetration, deeper, located in esophagus
mention phases of lesion development of corrosives
inflammation 24-48 hrs; acute cellular necrosis
sloughing phase:4-7days: cells slough off leaving ulcers and perforations
granulation phase 2 weeks: collagen deposition, new tissue formation
cicatrization phase 2-4 weeks: dense fibrous tissue formation and potential stricture development
menyion acute complications of corrosives
upper airway obstruction larynx edema
GIT hemorrhage
esophageal or gastric perforation
shock: neurogenic or hypovolemic
delayed complications of corrosives
mediastinitis
pericarditis
esophageal stricture
tracheoesophageal fistula
mpyloric stenosis
malnutrition, dehydration and cachexia
investigations to diagnose GIT lesions in corrosives and CONTRAINDICATIONS
upper GI endoscopy
CI:
airway obstruction
clinical signs of perforation
severe hemodynamic instability
severity grading and prognosis
Grade I: mucosal erythema and edema, excellent prognosis
grade II: mucosal ulcer, hemorrhage and pseudomembranes, good with treatment
grade Iii: deep ulcers, necrosis, high complications
mention complications of corrosives and how to diagnose them
pneumomediastinum in esophageal perforation - chest X-ray
free air under diaphragm, gastric perforation - abdominal X-ray
esophageal stricture - barium swallow after 21 days
extent of injury - CT scan of chest/abdomen
anemia- CBC
acid base status - ABG
assess renal function - electrolytes and BUN, and serum creatinine
blood glucose levels
emergency treatment of corrosives
secure airway immediately
dilute carefully
areange early endoscope
monitor closely for complications
provide adequate pain relief
anti shock measures
no otal intervention
supportive treatment of corrosives
nutritional support
acid suppression
antibiotics
corticosteroids
surgical intervention and indications for corrosives
emergency: sever hemorrhage, perforation and grade Iii injury
elective: delayed,
esophageal stricture dilatation: stricture
esophageal stenting: refractory stricture
esophageal replacement: in case of severe non-dilatable strictures
long term follow up for corrosives
for grade II and III injuries:
regular follow up for 1 year
serial esophagogram to detect stricture formation
endoscopic surveillance
nutritional assessment
button batteries mechanism of injury
corrosive effects: alkaline content
pressure necrosis
heavy metal toxicity
treatment of button batteries
airway assessment
location based management: remove in trachea or esophagus and symptomatic stomach,
for asymptomatic stomach: stool examination, x ray in 4-7 days, return if symptoms develop
if battery in intestine: monitor, if battery stops moving or becomes symptomatic, remove, most batteries beyond stomach pass spontaneously
pathophysiology of phenol
general protoplasmic poison:
cell membrane disruption
protein coagulation
coagulative necrosis
systemic absorption leading to multiorgan toxicity
routes of ingestion of phenol
ingestion
inhalation
skin exposure(rapid and extensive)
eye exposure(vision loss)
characteristic symptoms of phenol
phenol odor
distinctive painless skin lesions
dark olive green urine
characteristic presentation of corrosives
spontaneous vomiting
hoarseness and stridor
dysphagia and drooling
hemetamesis and melena
investigations for phenol toxicity
urine studies
renal function
hematological: CBC, methemoglobin(cyanosis), decreased hemoglobin and RBCs(hemolysis)
liver function test
ECG for arrhythmia
chest x ray if inhalation exposure
treatment of phenol
emergency: ABCD
decontamination:
for ingestion: gastric lavage within 1 hour
inhalation: remove victim, expose to fresh air, administer oxygen and monitory respiratory complications
skin: immediate and prolonged washing, remove contaminated clothing, avoid scrubbing
eye exposure: flush and irrigate for 15-30 mins, check corneal pH, urgent opthalmology consultation
specific treatment:
for methemoglobinemia: methylene blue
acute kidney injury: hemodialysis, alkalinize urine if myoglobinuria, aggressive fluid resuscitation
kerosene toxicity mechanism
pulmonary:
direct chemical injury to repsiratory epithelium
surfactant disruption- alveolar collapse
increased capillary permeability => pulmonary edema
risk of secondary bacterial infection
CVS depression
cardiac sensitisation to catecholamines - arrhythmia
GI mucosal irritation
timeline of kerosene toxicity
0-2 hrs: GI and initial resp. symptoms(tachypnea)
2-6 hours: peak resp symptoms, distress and dyspnea
6-24 hours: chest x ray changes appear
more than 48 hrs: possible secondary bacterial infection
investigations of kerosene
pulse oximetry
chest x ray(4-6hrs)
ABG
CBC
tests for toxic additives
critical rules of management of kerosene
no vomiting
no GL or AC
no prophylacatic antibiotics
critical points of management of corrosives
no vomiting, GL, AC or neutralising agents
treatment of kerosene
emergency: ABCDE
decontamination:
remove contaminated clothes
wash skin and eye irrigation
supportive treatment:
bronchodilators
ventilatory support
antibiotics: not prophylactic, only with 2ry infection
#corticosteroids: not recommende
discharge criteria for kerosene toxicity
asymptomatic 6 hrs
normal vitals and chest exam
normal oxygen saturation
routes of exposure for organophosphates (pesticides)
dermal(slower but common in farmers) 1-4 hrs
ingestion(suicidal, fastest and most severe) 30 mins to 2 hours
inhalation(intermediate in farmers) 15 mins-1 hour
pathophysiology of OPC(pesticides)
irreversible inhibition of acetyl choline esterase by phosphorylation
accumulation of acetyl choline at netve endings
continuous overstimulation of receptors
affects true cholinesterase (RBC AChE) and pseudocholinesterase (plasma AChE)
aging occurs after 24-48 hours
most important clinical manifestations of OPCs
DUMBELS
bronchospasm, bronchorrhea
respiratory failure: most common cause of death
anxiety
fasciculations
investigations for OPC toxicity
specific: cholinesterase enzyme levels:
pseudocholinesterase: easier, better and more available
true AChE: more accurate indicator
ECG
ABG
serum electrolytes(hypokalemia)
serum glucose(hyperglycemia
Liver and kidney function tests
chest X-ray
treatment of OPCs(pesticides)
stabilisations: ABCD
decontamination:
dermal:
healthcare worker protection is essential: wear gloves, gowns and avoid contact with contamination clothing
remove all contaminants, wash skin thoroughly, pay attention to hair, nails and skin folds, cut hair if it retains odor
oral: gastric lavage(1-2 hrs and protect airways first) and AC(1-2 hrs)
antidote:
atropine comp for muscarinic only, doesn't affect nicotinic effects and doesn't reactivate AchE
oximes(before aging): reactivates AchE, reverse all effects, (obidoxime)
supportive treatment: respiratory support, seizure control(BZDs, fluid management, electrolyte balance and monitoring
atropine dosing and endpoints for OPCs
adults: 1-2mg IV every 10-20 mins, continue till atropinisation
pediatric: 0.03-0.05mg/kg IV(min 0.1 mg) every 10-20 minutes
Endpoints:
clear lung fields on auscultation
adequate oxygenation >90%
reduction in bronchial secretions
complications of OPC poisoning
intermediate syndrome: 24-96 hours after apparent initial recovery, not responsive to antidotes, after cholinergic crisis resolves, overall weakness(neck, palsy, tendon reflex and limbs and respiratory ms.
organophosphorus induced delayed neuropathy: 2-3 weeks after exposure due to neuropathy target esterase(NTE), unresponsive to antidotes, not related to AChE inhibition partial recovery(months to years), may cause permanent disability. , starts with burning in fret, progressive weakness, tendon reflexes loss and sensory loss
routes of absorption and mechanism of carbamates
dermal, ingestion, inhalation.
reversible inhibition AchE by carbamylation, hydrolyzes within hours,
carbamates vs OPCs
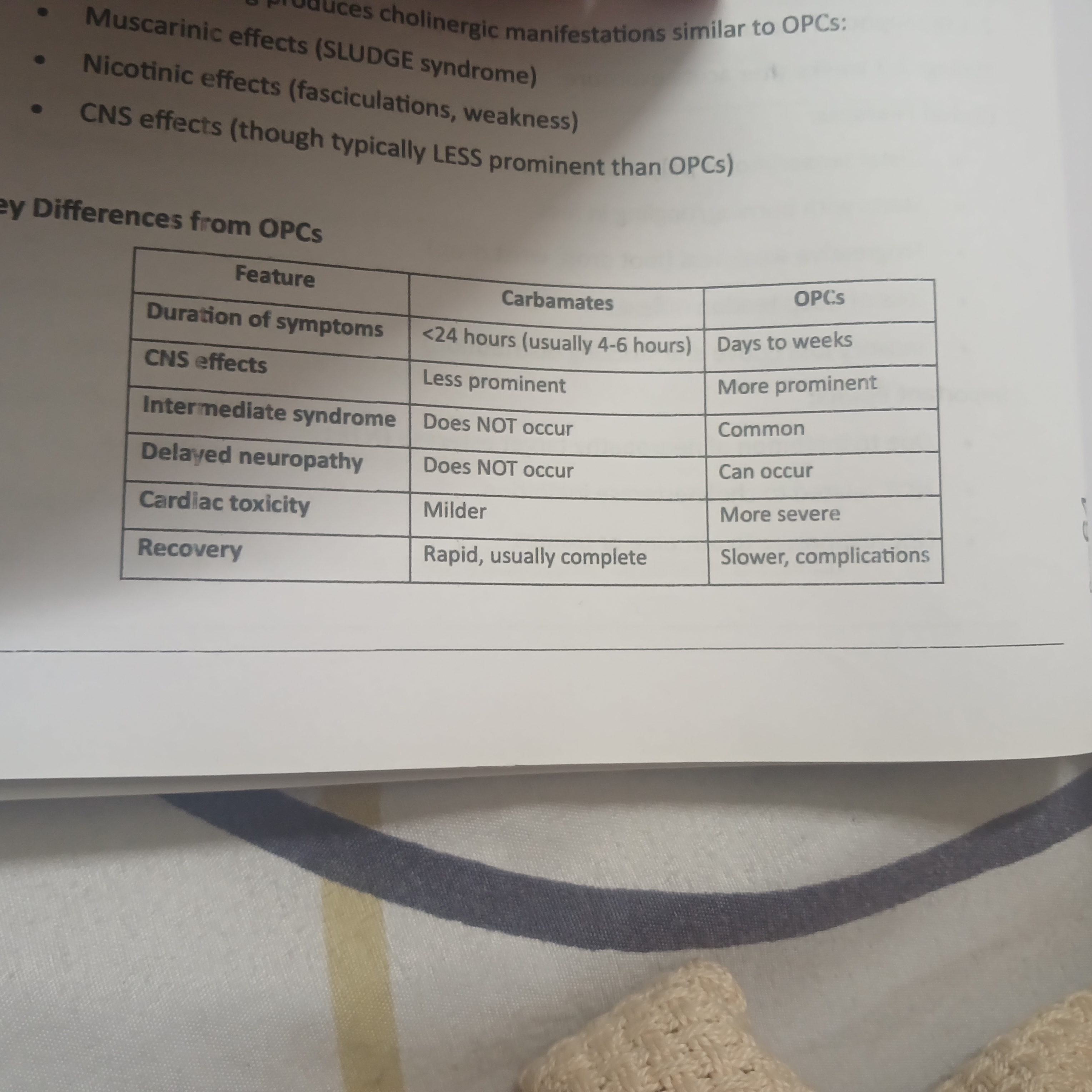
treatment of carbamates
same as OPCs
EXCEPT: no oximes but considered if OPC and carbamate congestion
phosphides modes of toxicity and mechanism
suicidal, accidental and occupational
chemical reaction: on contact with water, phosphides liberate phosphine gas
Toxic mechanism: rapidly absorbed
inhibits cytochrome c oxidase enzyme in mitochondrial ETC blocking aerobic metabolism, resulting in:
decreased ATP
lactic acid accumulation (metabolic acidosis
cellular death
mention phases of phosphides toxicity and main problems
acute phase(1-24 hrs): GIT (black vomitus with rotten fish or garlic odor) , respiratory(ARDS, dyspnea and resp failure) and cardiovascular (most serious), (arrhythmia, cardiac arrest(most common cause of early death). neurology(coma(bad prognosis)), metabolic acidosis
phase 2: apparent recovery(may be absent) 24-48 hrs)
phase 3: delayed toxicity phase 36 hrs- 7 days:
severe hepatotoxicity: prolonged PT/INR, acute liver failure, jaundice
renal toxicity
multiorgan failure: DIC, death from cardiovascular collapse of multi organ failure
investigations of rodenticides(phosphides)
ECG
ABG
serum electrolytes
cardiac markers
liver function tests(AST, ALT, PT/INR(crucial), serum billirubin)
renal function test
blood glucose
chest x ray
treatment of phosphide poisoning
ABCD,
decontamination: GL with paraffin or coconut oil to neutralise gastric acid, reduce phosphine gas liberation,
AC is contraindicated
specific:
magnesium sulfate: cardioprotective
N-acetylcysteine: antioxidant, hepatoprotective, free radical scavenger
IV sodium bicarbonate: sever metabolic acidosis pH<7.2
supportive treatment:
fluid management
correct electrolyte abnormalities
cardiovascular support
hepatic support(vit K and FFP)
hemodialysis in renal failure