Pharm Test 3 Review (STUDY PURPOSE)
1/58
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
59 Terms
Exercise-Induced Bronchospasm Treatment
Beta 2 Adrenergic Agonist: Albuterol (Proventil, Ventolin)- best
Make sure you have enough inhalers (one in car, home, job, etc)
Montelukast
Mast Cell Stablizers: Cromolyn
Beta2 Adrenergic Agonist: Albuterol (short acting)
Indication: long term asthma, exercise- induced bronchospasm, asthma exacerbation
Adverse effects: Triple T's
T: Tachycardia (and because ur heart is beating fast you will feel palpitations which could has chest pain and SOB)
* Remember Albuterol AMMPS up the body* :TACHYCARDIA
Although this med makes your heart beat fast remember ppl can handle a high HR but not low breathing so don't quickly discontinue med if patient get high HR.
T: Tremors (report these)
T: Tossing and Turning (Insomnia) which could make you restlessness and nervous
- Avoid Caffeine
Order of meds to take for Acute Asthma Attacks (ALWAYS IN THIS ORDER)
AIM:
A- Albuterol
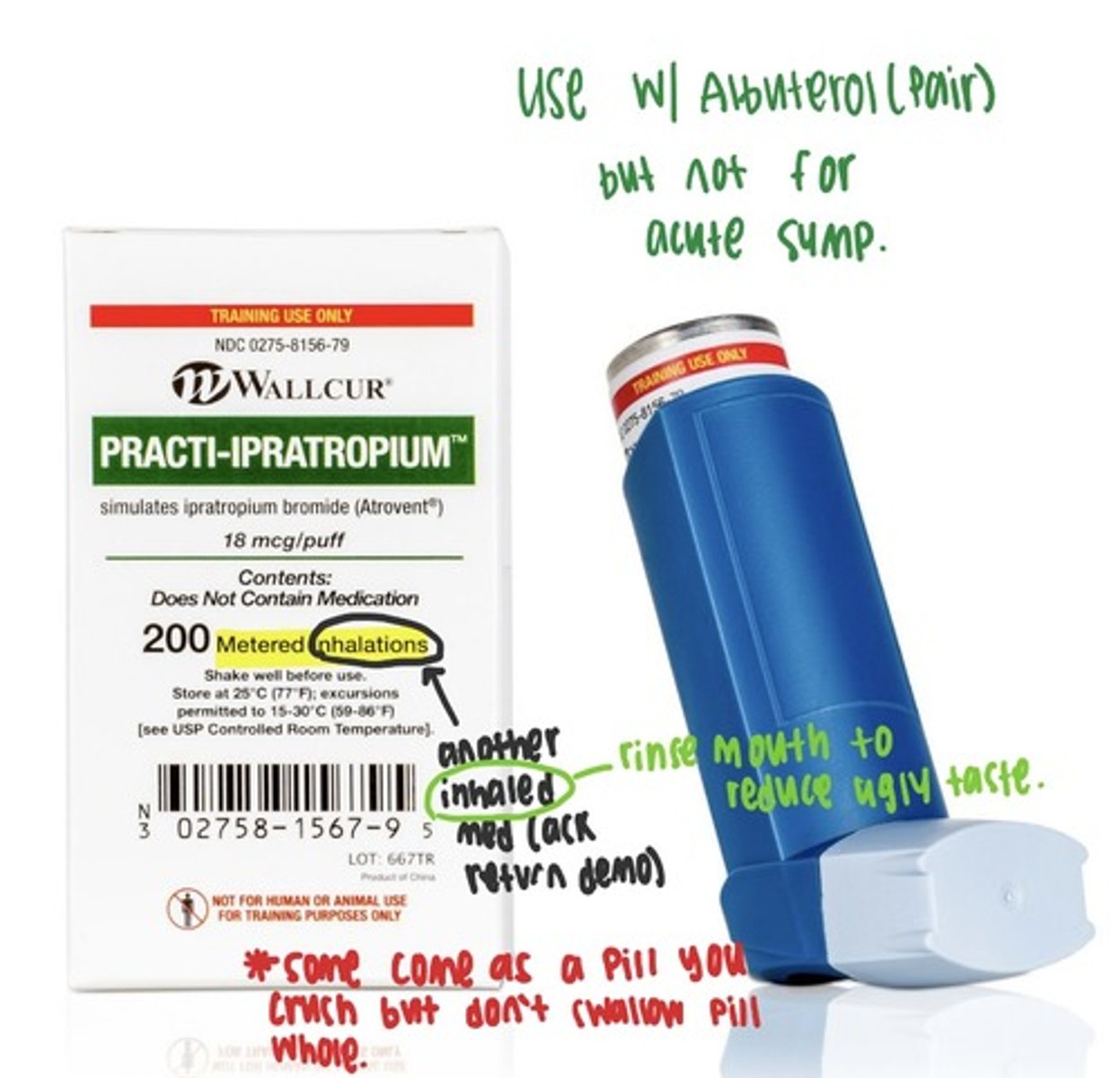
I- Ipratropium
M- Methyl-prednisolone
Inhaled Anticholinergics: Ipratropium
Tro-pium you can't pee w/ them
Indications:
Decrease secretion in COPD clients, relief broncho-constriction in COPB clients
Adverse Reactions:
ALL THOSE ANTI-CHOLINERGIC EFFECTS
Can't see (intraocular pressure), pee (urinary retention), spit (dry mouth, pharynx irritation) or sh*t
Intervention:
If they have dry mouth give water and candy, get tested for glaucoma, monitor urine
Contradictions: sensitivity to ipratropium, atropine, belladonna alkaloids or bromide
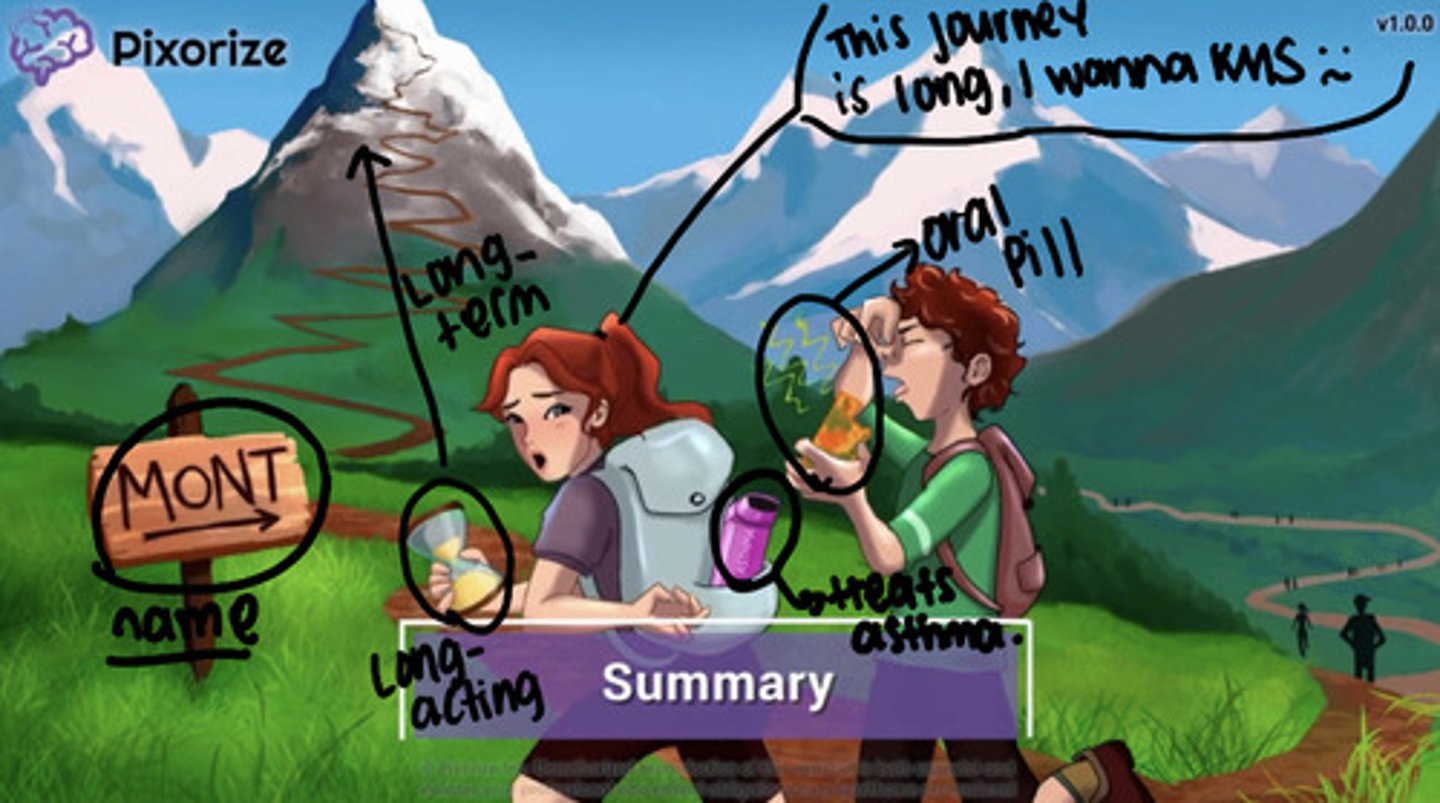
Leukotriene: Montelukast
Indication: treat allergic rhinitis, exercise induced bronchospasm
Adverse: neuropsych events such as suicidal ideations
Intervention: observe behavior change
Admin: once a day oral pill, to prevent EIB take 2 hrs before exercise
Contradiction: acute exacerbation, status asthmaticus, (no for montelukast but for zafirlukast liver dysfunction)
3 Ls
Luke likes to sing (open airways)
Long Term, use
Long onset (1 to 2 weeks to reach therapeutic range)
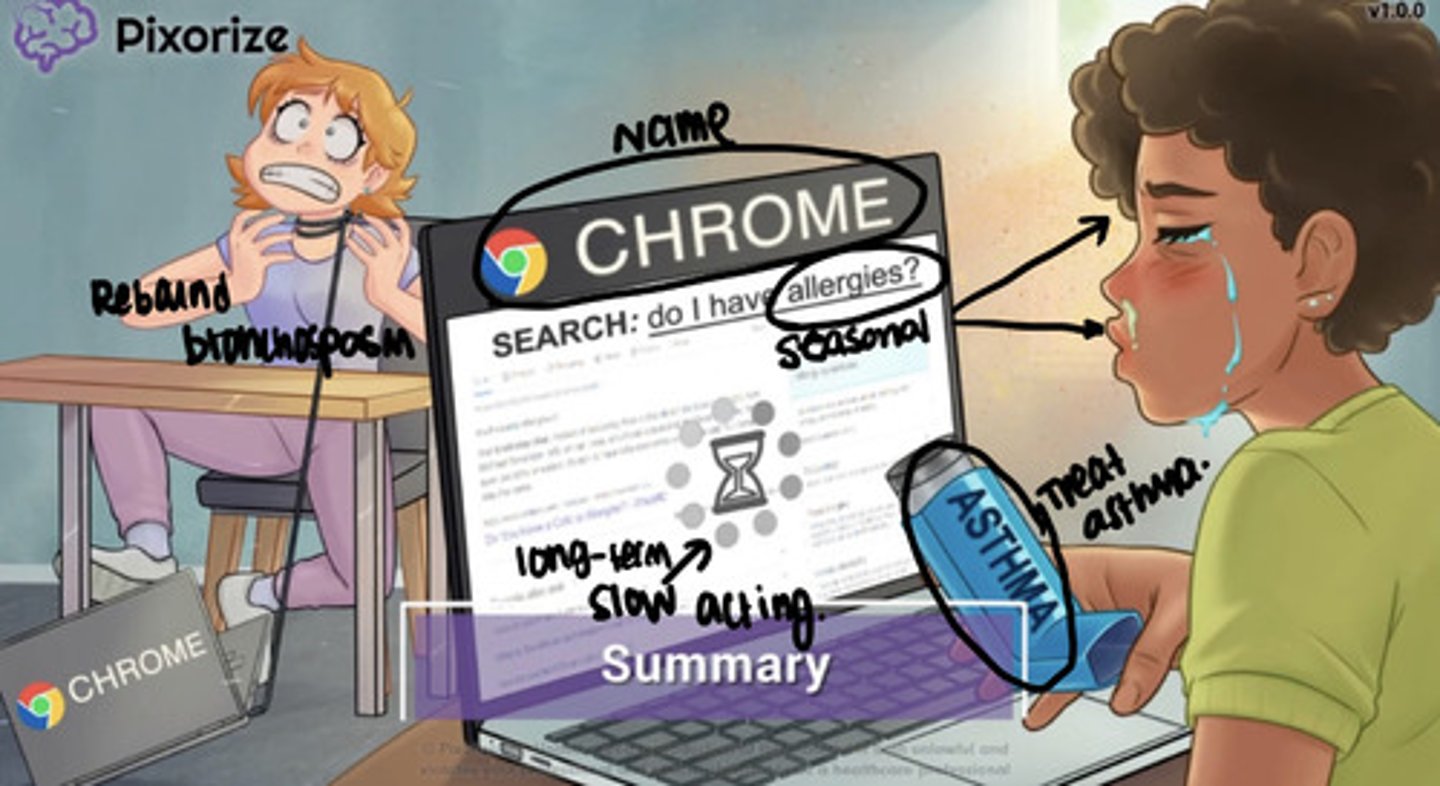
Inhaled Corticosteroids
beclomethasone, fluticasone (Flovent)
beclomethasone, fluticasone (Flovent)
MOA: reduce inflammation cause corticosteroids act on glucocorticoids receptors and less inflammation equals more open airways and reduce secretion
Indication: long term chronic asthma (first line)
Route of Admin: inhaled but risk for candidiasis (risk for thrush, so rush to brush)
Adverse: candidiasis (oral), adrenal gland sad= infection, muscle & bone weakness, high sugar, peptic ulcer, fluid imbalance, headache
THISES ARE SLOW- NEVER USE 1ST FOR ACUTE ASTHMA TAKE UP TO 2-3 WEEKS
Systemic Glucocorticoids: Prednisone, Methylprednisolone
MOA: reduce inflammation, which open more airways and reduce secretion
Indication: acute exacerbation of asthma, long term manage chronic asthma
Route of Admin: These are oral
Adverse: alot...
suppress adrenal function (so immune suppression), weight gain (fluid retention) , headache, hyperglycemia, bone & muscle wasting, peptic ulcer disease, hypokalemia
TAPER THIS DRUG OFF & NO NSAIDS
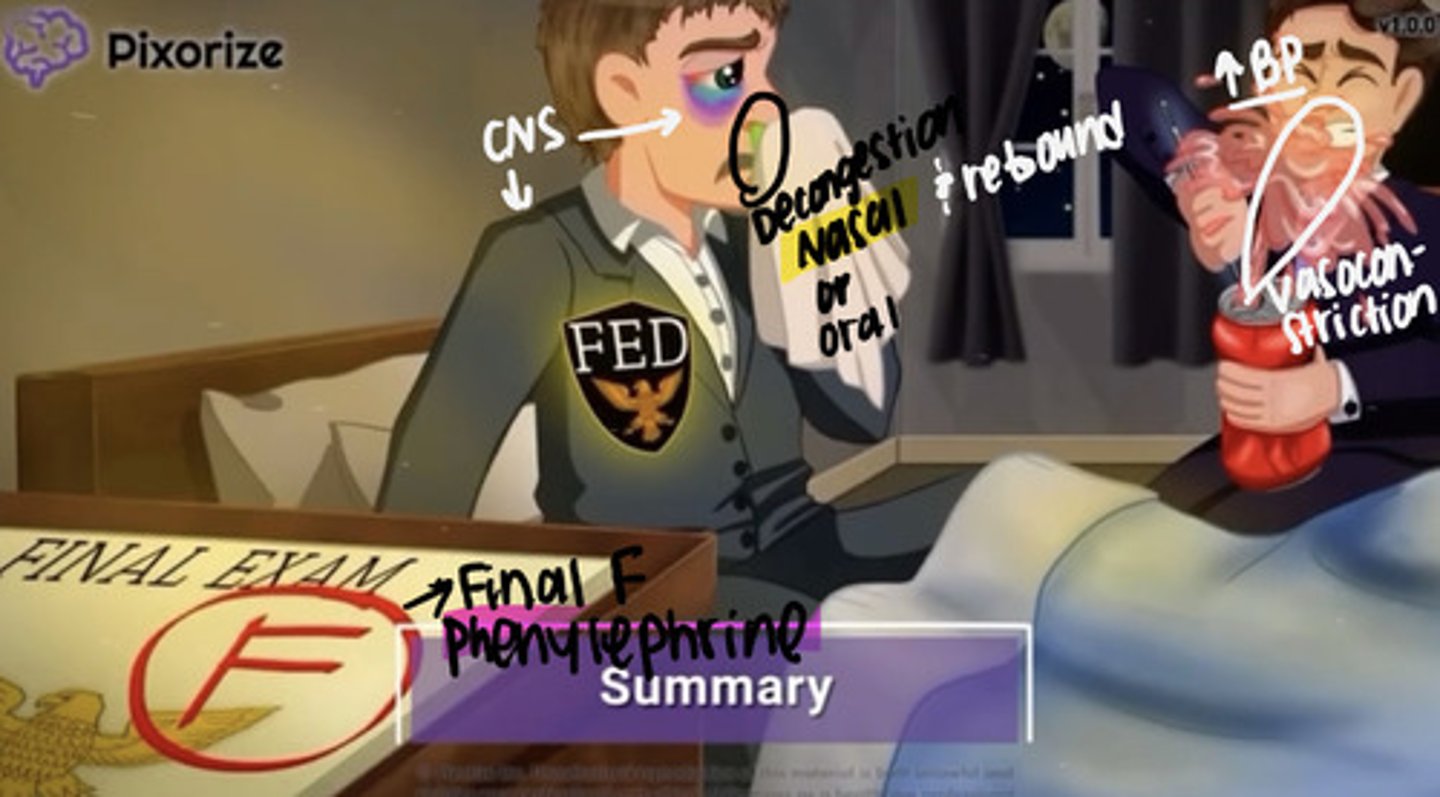
Nasal Decongestants: Phenylephrine (Neo-Synephrine)
MOA: vasoconstriction nasal
Indication: allergic rhinitis, sinusitis, and common cold
Adverse Effects:
Increase BP, tachycardia/ palpitation, insomnia with can cause restlessness, overdose or systemic absorb (hypertension, tachycardia, palpitation), rebound congestion with prolonged use (so basically only take for 3-5 days if you take for more days it will be hard to come off from and when you stop symptoms will return (rebound) becuz body got use to it)
Interventions:
basically if insomnia offer sleep aid, if high bp monitor bp, if high HR monitor HR, only administer when needed
Recommend glucocorticoid to minimize symptoms while discontinue this med after prolong use
Common Cold
Acute, self-limiting, and highly contagious viral infection of the upper respiratory tract.
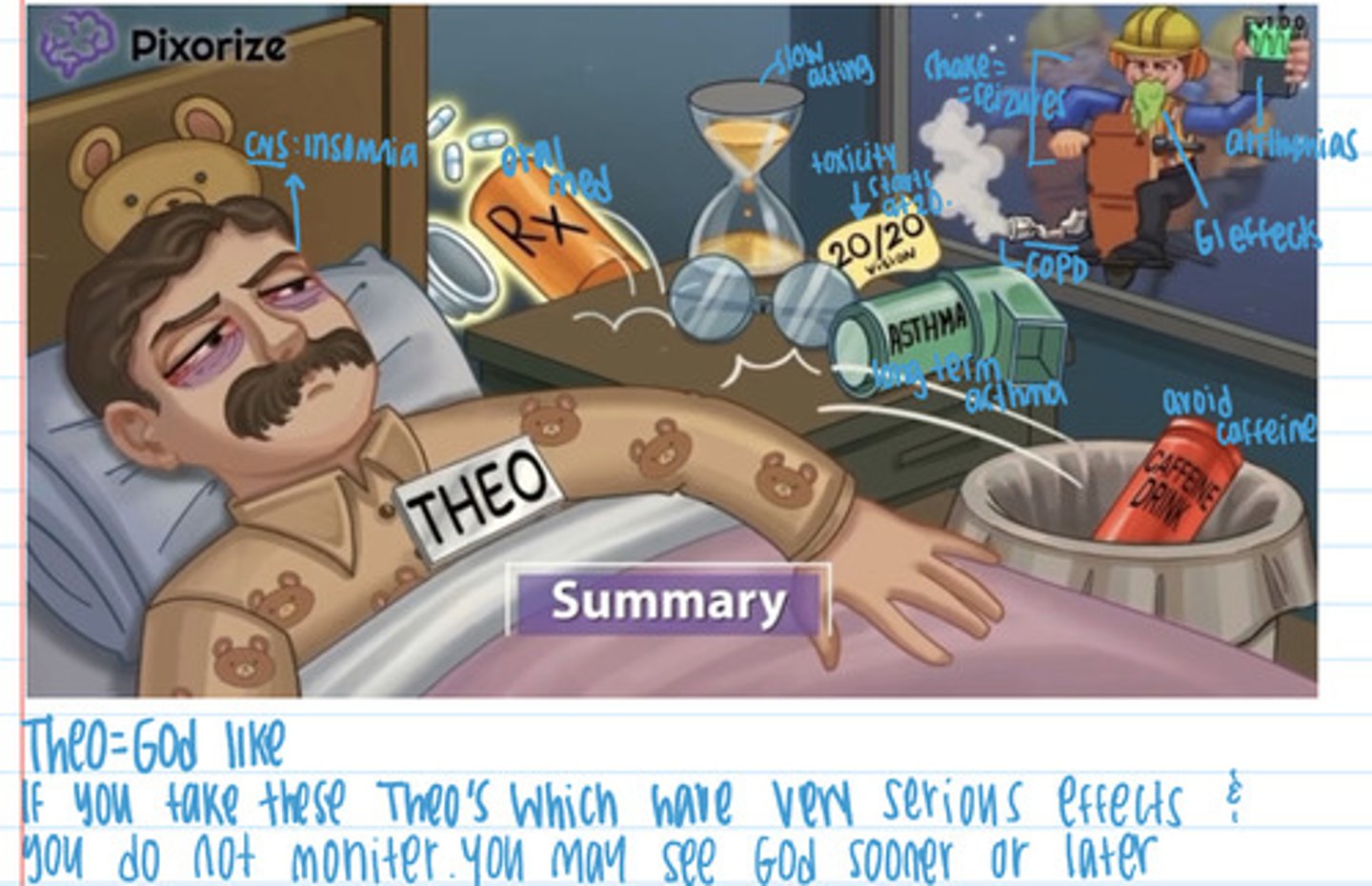
Methylxanthines: Theophylline
Indication: long- term management of chronic asthma
Adverse effects: rare at therapeutic levels, GI effects, dysrhythmias (blackbox), restlessness & insomnia (over therapeutic), seizure (toxic levels), tachycardia
Intervention: monitor plasma, discontinue is toxic symptoms, seizure precaution, monitor hr, give antidysrhythmics (if dysrhythmias)
Client: avoid caffeine, drugs, and don't give to patients with impaired metabolism (oral pill)
Dextromethorphan (Non-opiods)
MOA: decrease sensitivity cough receptors
Indications: to reduce cough
Route of Admin: oral
Adverse: large amounts cause CNS depression, GI effects, dizzy/ lightheadedness, potential for abuse
Intervention: slow position change, drug w/ food or milk
Antitussives: Codeine (Opioid)
Indication: suppress chronic cough & non-productive cough
Adverse Drug Reaction: CNS depress, dizzy, lightheadedness, GI effects, constipation, respiratory depress, potential for abuse (black box)
Client instruction:
get up slowly cause CNS depress, drink with food cause GI, avoid activities of mental awareness, increase fluid & fiber, remove cough triggers
Don't take with alcohol, opioids, CNS depressants
Contradiction: known allergy, htx of abuse, caution w/ children, reduced respiratory reserve- asthma, emphysema, prostatic hypertrophy, MAOIS or SSRIS
Brain & Breathing
Brain exhales when notices there is too much CO2 in body but some have a hypoxic drive (drive to breath in only when O2 level are low, so increase of CO2)
Cromolyn
Indication: Long term treatment of asthma, prophylaxsis for exercise induced bronchospasm, prophylaxsis of seasonal allergies
Adverse: allergic reaction if allergic to med
Intervention: administer epinephrine and/ or antihistamines to reverse allergic effect
Admin: nebulizer or meter does inhaler, several weeks to take effect, four times daily on fixed schedule (low patient compliance), use 15 minutes before exercise, does not relieve acute asthma
Expectorant: Guaifenesin
MOA: helps you cough up gunk (increase expectorant idk increase cough)
Indication: cough related viral upper respiratory tract infection, loosen phlegm to reduce secretion
Adverse: GI, dizzy, drowsy, headache, rash
Intervention: slow position chang , drink with food or 8 oz water, encourage 1500-2000 ml daily
Admin:
Don't take with cough meds that already have guaifenesin
Hypertension (high bp) Importance to treat
Underlying danger (importance of why htn should be managed)
- Body organ damage
- Increased risk of atherosclerotic vascular disease, thick heart
(difficult to diagnosis becuz must patients asymptomatic and hard treat because of compliance but is a silent killer)
Non- pharmacological/ life style management for HTN
First thing pt must do.
- reduce salt (dash diet)
- watch for high in potassium foods like bananas, potatoes (risk of hyperkalemia)
- increase exercise (150 min)
- increase fiber
- decrease weight (for every 1kg down, systolic goes down one)
- quit smoking
- reduce alcohol
- reduce caffeine
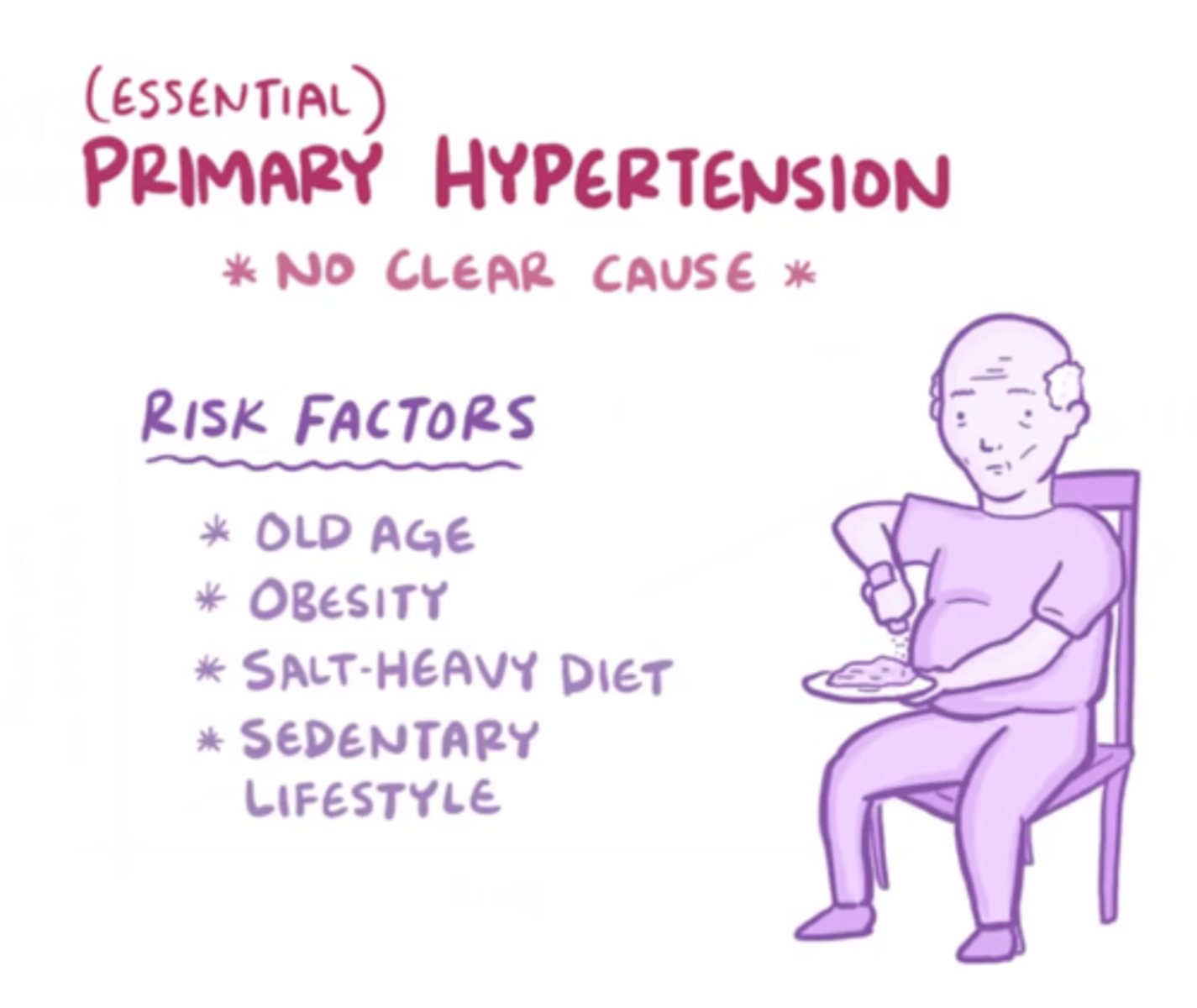
Risk Factors for HTN
increased age, cigarette smoking, high salt diet, high intake of alcohol, low physical fitness, obesity, insulin resistance, psychological stress, sleep apnea, and family htx
Why do we use combination medication when treating HTN?
multiple low dose preferred vs high dose of a single agent, monotherapy limited to how much it can decrease bp (roughly 10-20 systolic decrease per med at standard dose)
What is resistance hypertension ?
when the target goal for your BP is not met with 3 appropriate dose medication.
How to prevent:
- ensure compliance
- consider white coat syndrome
- pt referred to specalist
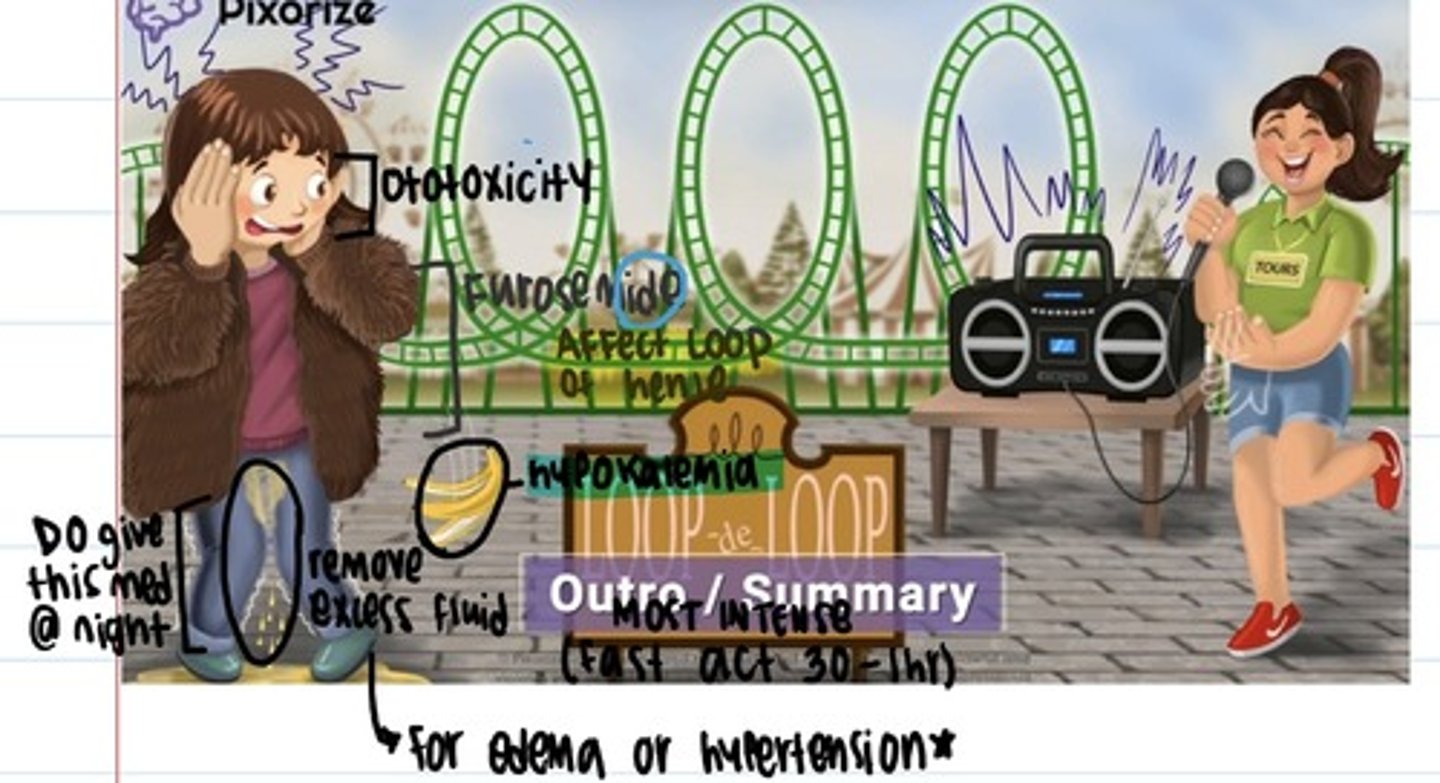
Loop Diuretics (Furosemide)
Block the chloride pump in the ascending loop of henle (decrease reabsorption of sodium and chloride)
Indication: pulmonary edema in HF, treats renal, cardiac, and hepatic edema, treats htn
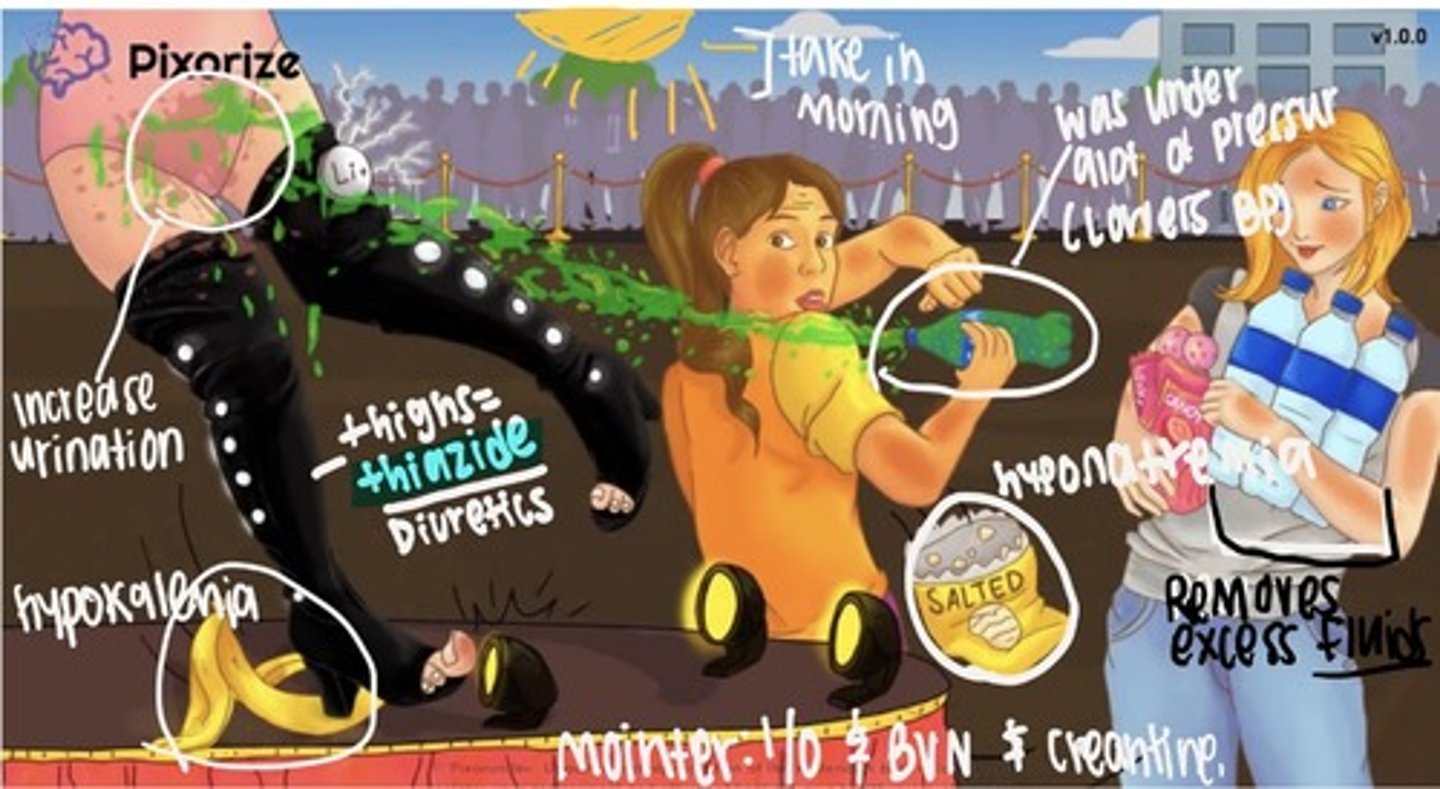
Adverse Effects: * electrolyte depletion (hyponatremia, hypochloremia, hypokalemia, ototoxicity, hyperglycemia, increase uric acid, kidney toxic
Pt education/ intervention: report all sym, eat more potassium, monitor weight and intervention monitor Bun and creatinine, monitor for dysthymia caused by hypokalemia
Give med in morning to avoid nocturia (none past 2pm)
- Oral, IV, IM
Thiazide diuretics (ends w/ thazide)
Chlorothiazide & Hydrochlorothiazide (HCTC)
MOA: blocks reabsorb of sodium and chloride in the early distal convoluted tubule (basically keeps Na and Cl in tubes to be excreted so it stops it from being reabsorbed back in body)
Indications: HTN & edema (most prescribed/ first line)
Adverse: electrolyte imbalance (hyponatremia, hypochloremia), dehydration, hypokalemia, hypotension, hyperglycemia, chance of gout, photosensitivity, don't give past 2pm
Nursing Consideration: monitor pt input and output, (REPORT IF LESS THAN 30 ml/ hr) BUN and creatinine
Every time there is an adverse effect for hypokalemia monitor for
dysrhythmias
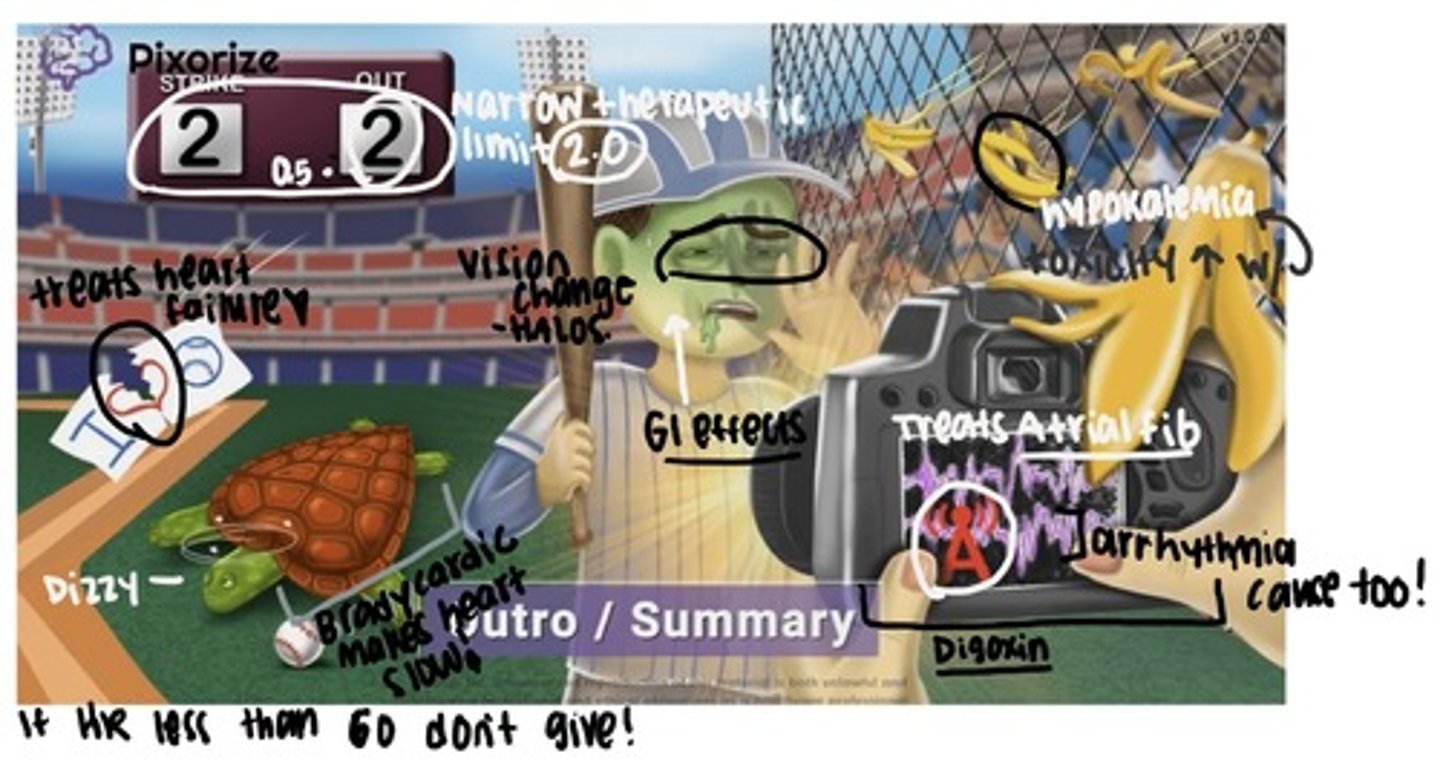
Importance of potassium with digoxin
- You need K+ for digoxin to work.
- Also you need potassium for your muscles to work. If there is no potassium your heart (a muscle) can start beating weird (arrhythmia- sign of toxicity)
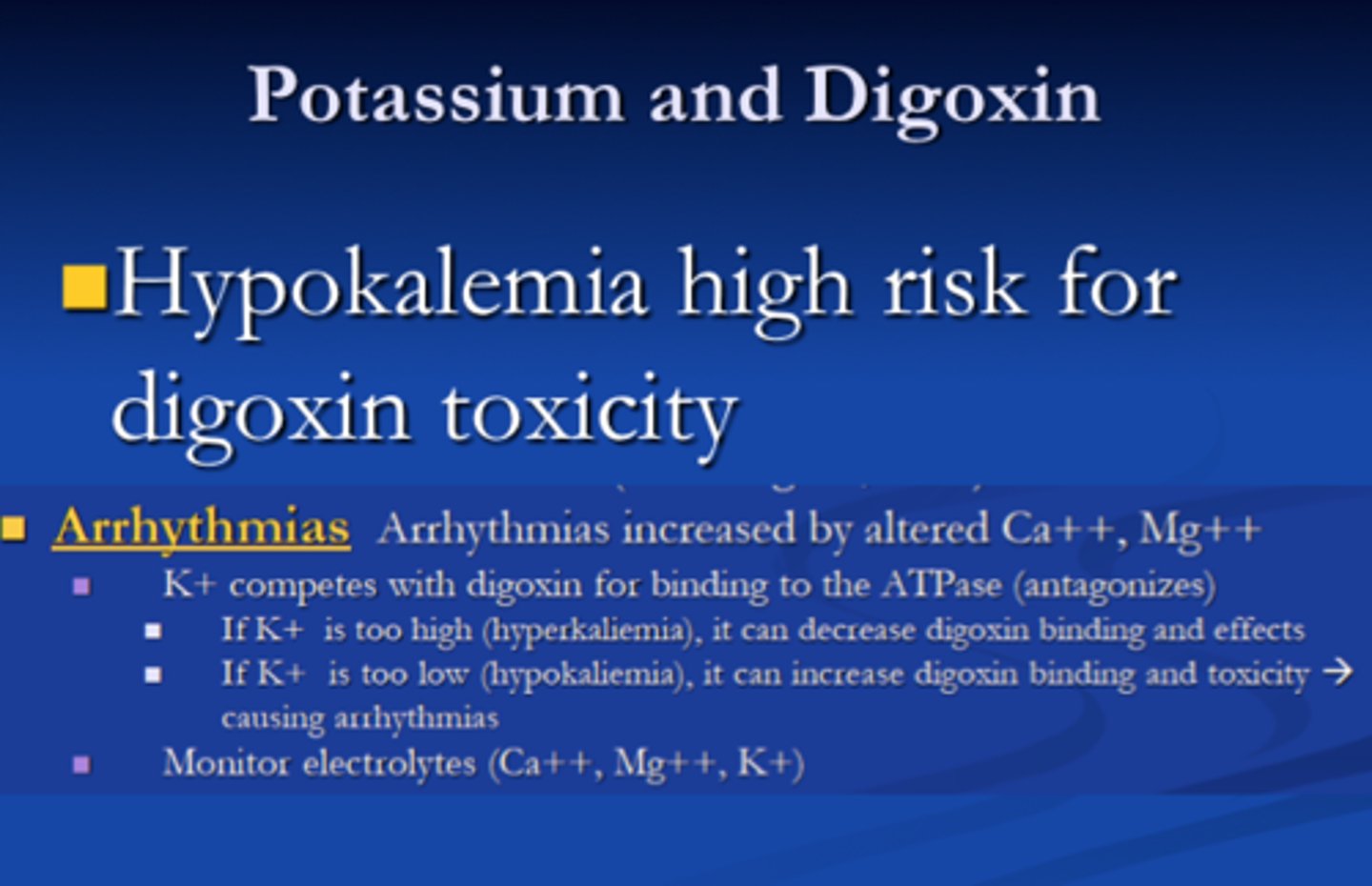
Adverse effects when taking digoxin and furosemide in combination
Many diuretics can cause potassium loss. A low level of potassium in the body can increase the risk of digitalis (digoxin) toxicity.
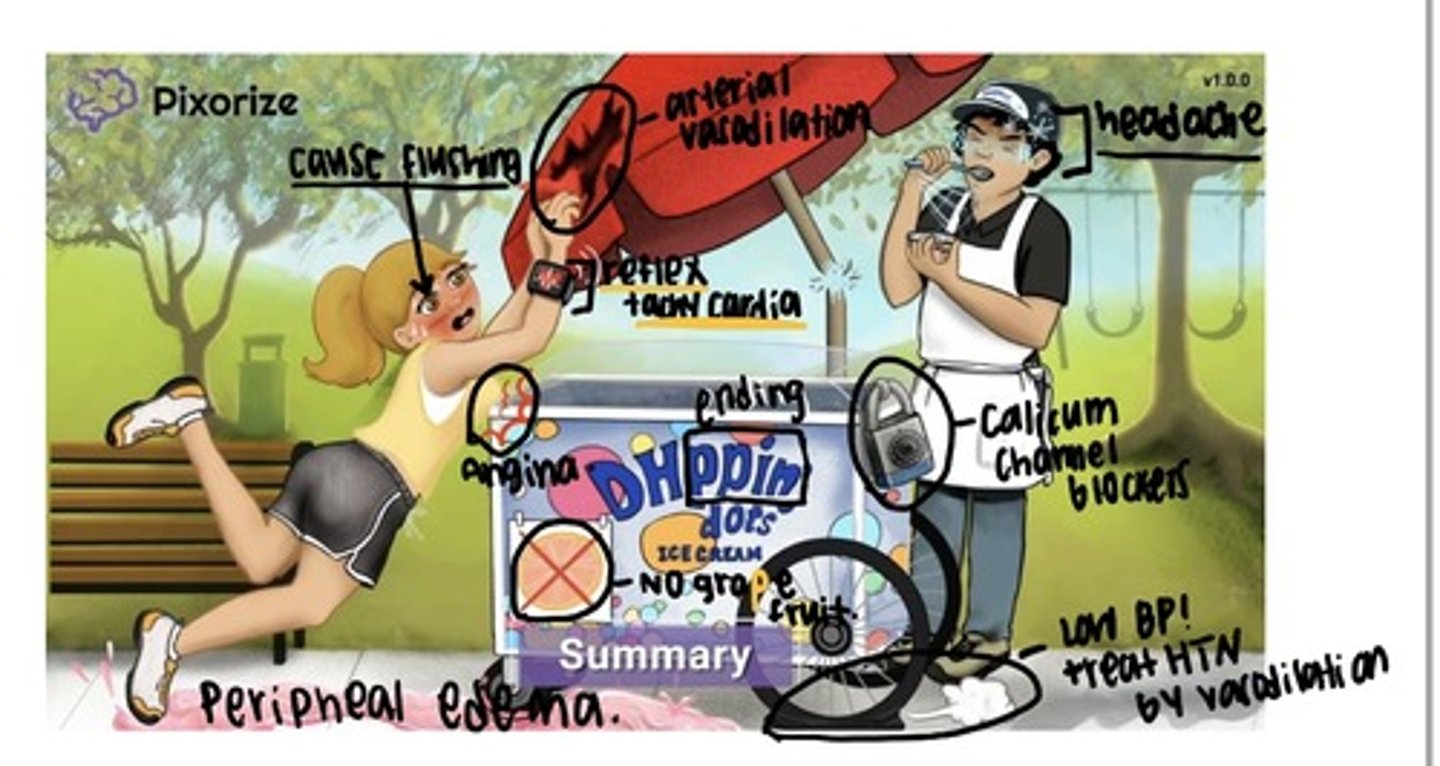
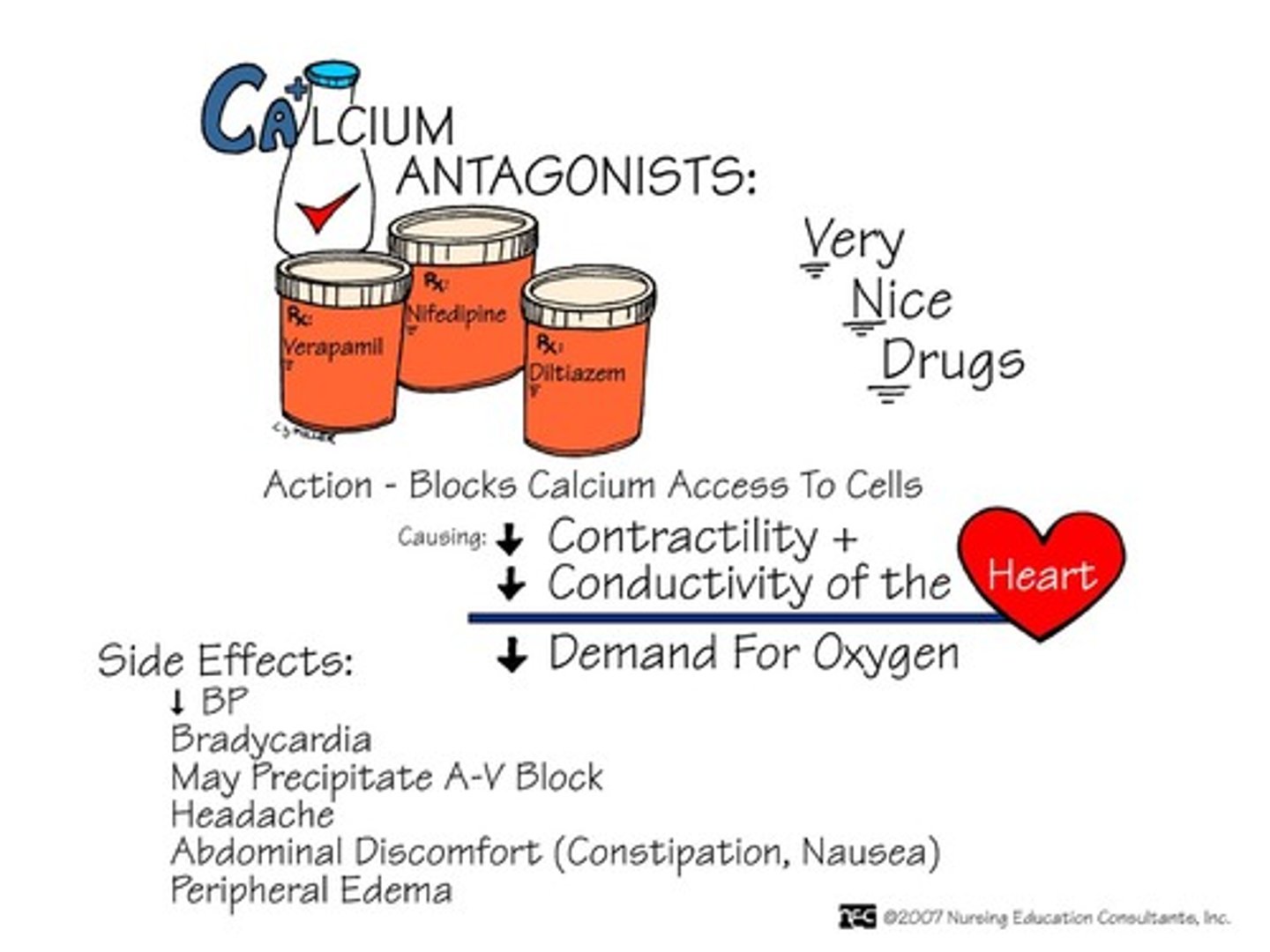
CCB
Everything that ends with dippine but DON'T FORGET verapamil and diltiazem
Indication: decrease bp (cardiac workload), angina (O2 consumption)
Adverse: reflex tachycardia, headaches, lightheadedness, dizzy (basically CNS effects), face flushing, peripheral edema, arrhythmia, gingival hyperplasia (rare), constipation
Pt teaching: XR and SR must be swallowed whole
Food and Drug Interaction: Grapefruit, St. John's wort, beta blockers, other stuff like rifampin, phenobarbital, etc
Cardiac Glyxoside/ inotropic: Digoxin
Indication: treat HR symptoms, artial fib and flutter, and atrial tachycardia
Adverse: cardiac dysrhythmias, digoxin toxicity
Early sign of toxicity: GI symptoms (n/v, anorexia), CNS symptoms (fatigue, visual disturbance, yellow vision and blurred vision), increase mortality in women
Toxic above 2.0
Intervention:
- Take apical pulse for 1 min before administering digoxin, withhold drug if pulse falls below 60/ min in adults
- For severe digoxin toxicity, digoxin immune FAB (Digibind) admin IV as an antidote to neutralize digoxin
- Monitor serum potassium levels
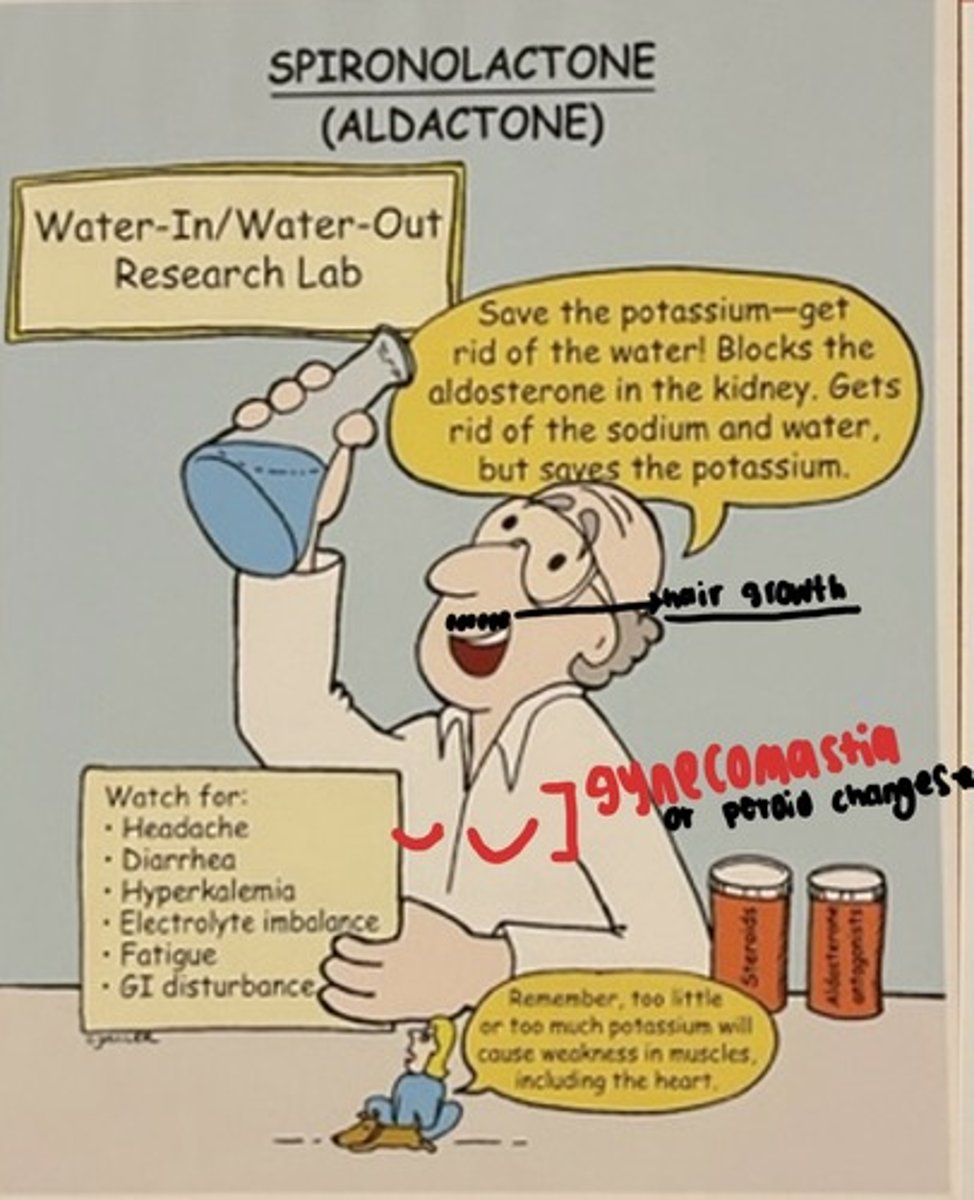
Potassium Sparing Diuretics: Spironolactone
Indications: HF, hypertension
MOA: Blocks aldosterone, promoting excretion of Na+ & water, but retention of K+
Adverse: Hyperkalemia, amenorrhea, gynecomastia
Interventions: Monitor K+ levels, teach pts to AVOID salt substitutes containing K+, monitor BUN & creatinine, monitor for dysrhythmias
SPIRonoLACtone will improve your SPIRits bc you won't LACk potassium.
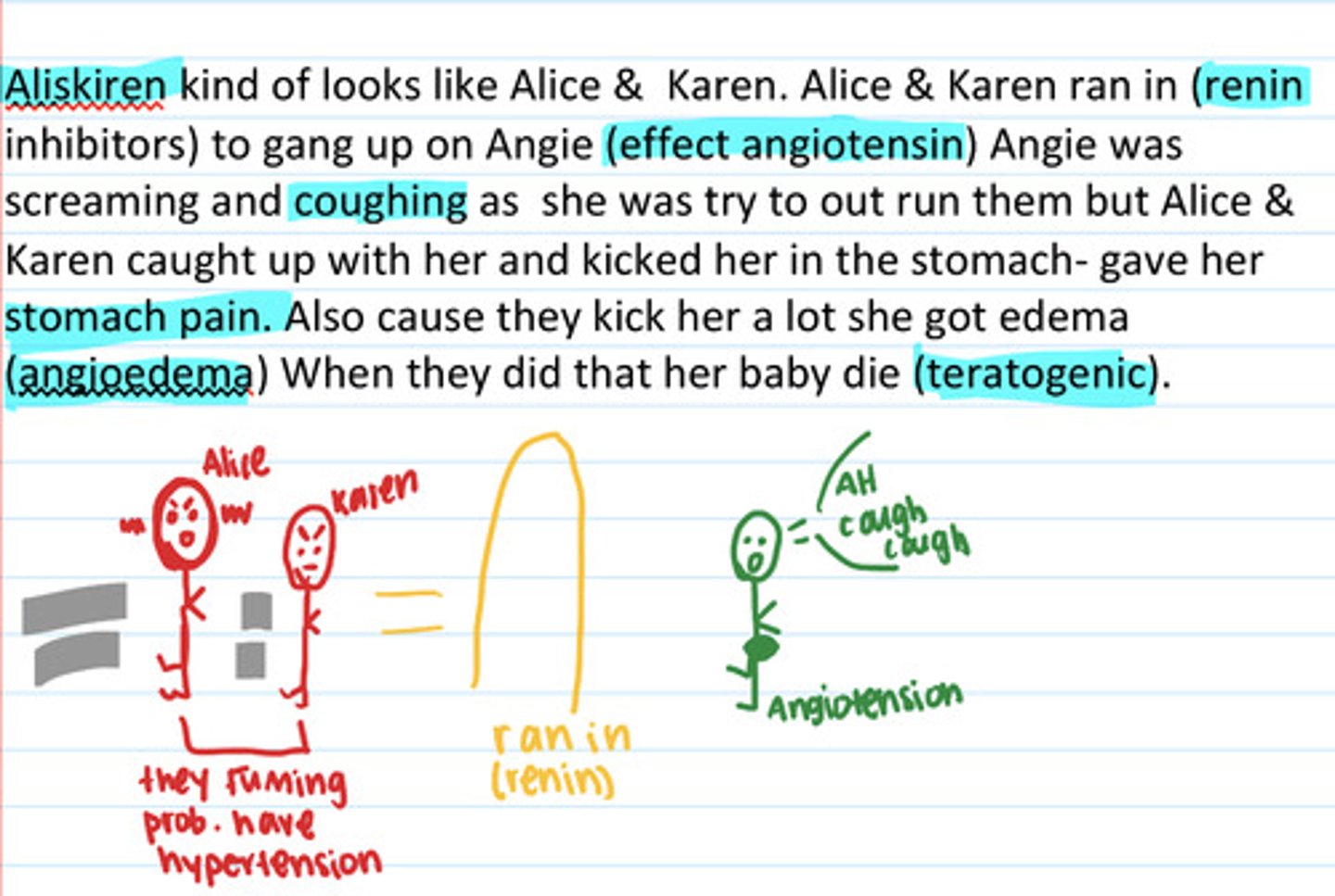
ACE inhibitors (ending -pril)
Angiotensin converting enzymes (effects angiotensin 1)
Indication: hypertension, HF, diabetic nephropathy, left ventricular dysfunction
Adverse: hypotension, dry cough, angioedema (too much can stop airway), hyperkalemia (so no more potassium supplements or potassium sparing diuretic), captopril can cause neutropenia
Nursing Consideration: Don't give if pt BP lower then 90 and HR lower then 60, if have renal problem no
- teach client to rise slowly (orthostatic pressure), notify provider or cough or angioedema, not a lot of potassium eating
Treat severe angioedema with IV epinephrine

Renin Inhibitors: Aliskiren
ONLY Renin inhibitor on market
directly inhibits renin so inhibits conversion of angiotensinogen to angiotensin
Indication: HTN
Adverse: cough, angioedema, abdominal pain, diarrhea, hyperkalemia, fetal toxicity
Drug interaction: potassium sparing
ARBS: Losartans
Indication: used alone or in combo to treat hypertension, HF and after MI, slow progression of renal disease , stroke
Adverse: headache, dizzy, syncope, weakness, GI problems, dry mouth, rash, dry skin, alopecia, angioedema (less likely then ACE but still)
Contraindications: allergy, pregnancy, children under 6, or children more than 6 with low creatinine
Treat severe angioedema with IV epinephrine

Therapeutic response to medication treatment of HCTZ and ARBs (losartan)
HCTZ (causes hypokalemia) often used in combination with ARBs to reduce risk of hyperkalemia
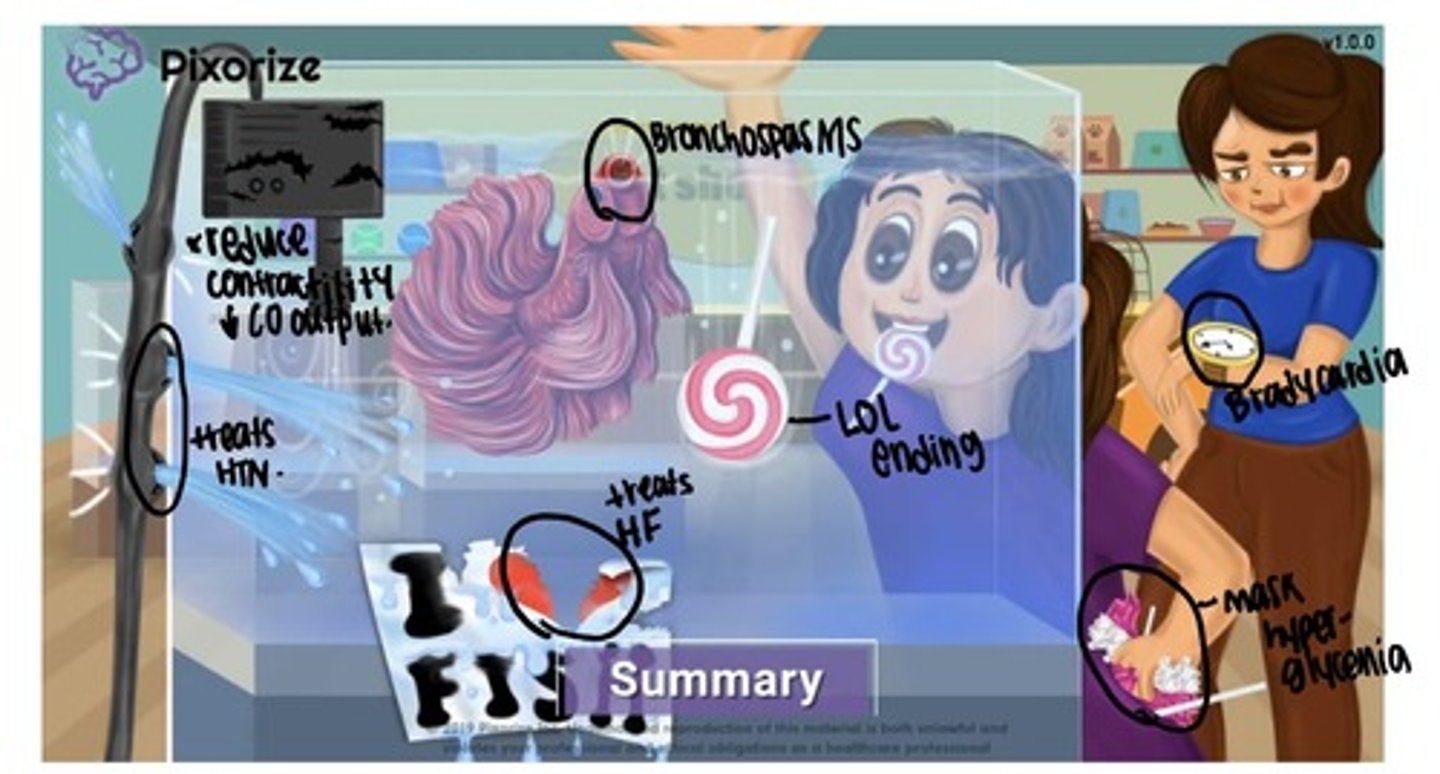
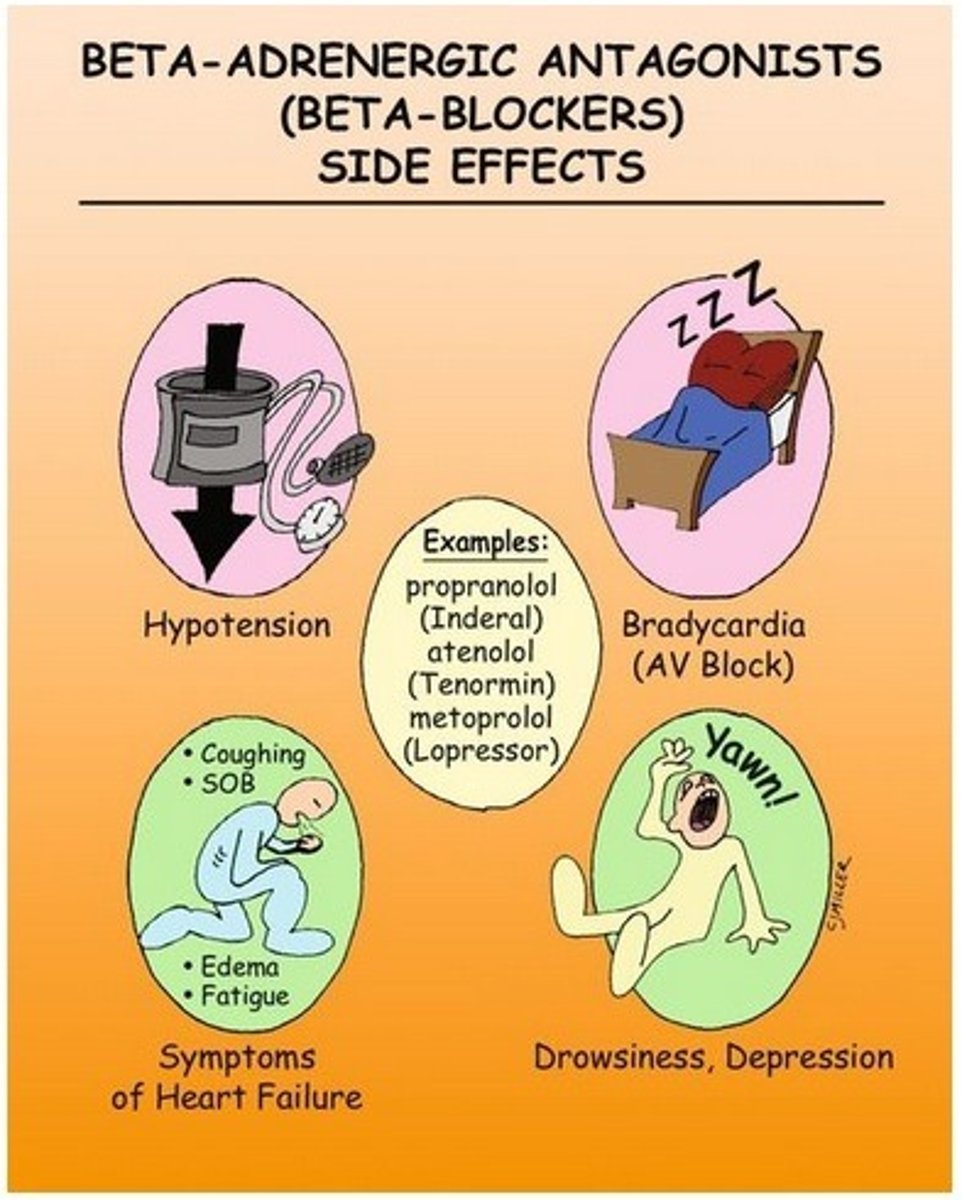
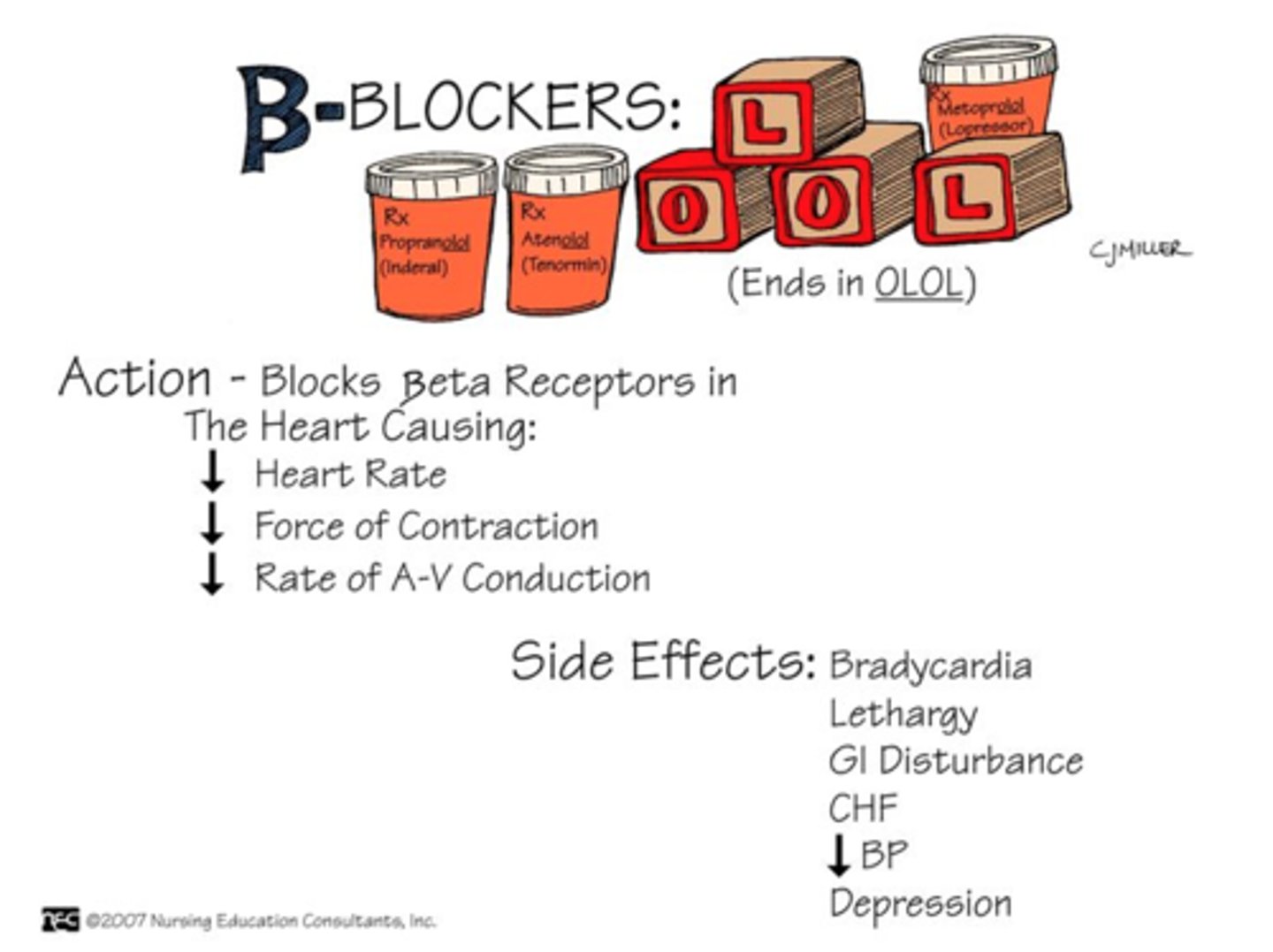
Beta Blockers
Indication: treats htn, treats hf, prolonged chance of survival following MI, angina, migraines prevention
Adverse: GI effects, CV effects (bad for heart failure pt w/ cracks in chest, no edema, rapid weight gain) , respiratory effects (wheezing), blood sugar masking, bradycardia (if HR less the 60, hold), hold if low bp too
HOLD CAFFEINE
Contraindications: severe unstable HF, asthma or other bronchospastic disorders, heart block or bradycardia, preg/ lactation, cardiogenic shock
First action for first sign of chest pain
Person should stop all activities and sit or lie down
Nitrates: Nitroglycerin
MOA: vasodilation
Indication: Acute angina, HF
S/S: headaches, orthostatic hypotension, reflex tachycardia
Routes: IV, sublingual, transdermal (handle with gloves)
ALl bypass liver and first-pass effect
Contradiction: head injury, hypotension, anemia, allergy, erectile dysfunction meds (all the -fils that fill a d*ck)

Angina when to call 911
If chest pain is not relied in 5 minutes after one does, the patient should call 911. Pt can take one more tablet while awaiting for emergency care and third tablet 5 minutes later (NO MORE THAN THREE, angina pain that does not react to nitrates might be MI)
Short Term treatment of angina
sublingual, translingual, iv nitrates
Long term treatment of angina
used to prevent anginal episode, sr oral capsules, transdermal nitrates
Also organic nitrates (Isosorbide dinitrate) oral
How to prevent nitroglycerin tolerance
regular nitrate- free period to allow enzyme pathways to replenish (transdermal form removed patch at bedtime for 8 hour)
Ranolazine
MOA: decrease O2 demand
Indication: angina prevention
S/s: QT prolongation
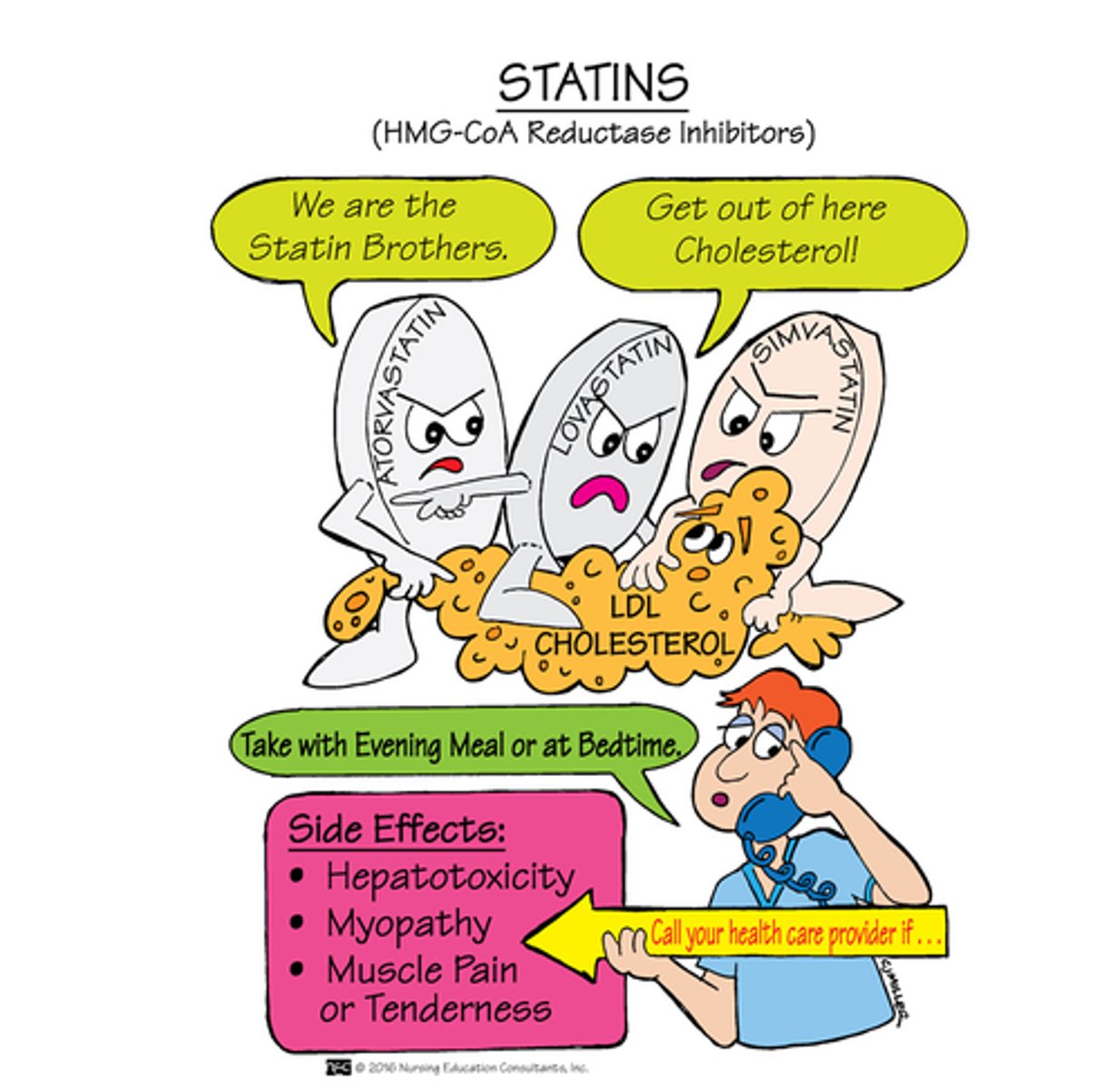
HMG-CoA Reductase Inhibitors: THE STATINS
MOA: inhibit HMG- CoA result in reduced LDL (keep the L's low) and increase of HDL
Indication: hyperlipidemia (first line) and prevention of cardiac disease
S- Sore muscle that progress to rhabdomyolysis (adverse effect)
T- Toxic liver (monitor ALT & AST)
A- Avoid grapefruit and St. Wort
T- Take at night (cholesterol synthesis at night)
Administration: Oral, Take in evening for greatest effect, don't give to children under 8 cause their liver not mature
Other Antilipemic Medications (QUICK summary)
Bile acid sequestrants (cholestyramine & colesevelam)
MOA: increase loss of ldl through feces
S/S: GI effect- constipation
Fibrates (Fenofibrates & Gemfibrozil)
MOA: lowers triglycerides
S/S: increase risk gallstone, GI problems, and Myopathy, liver
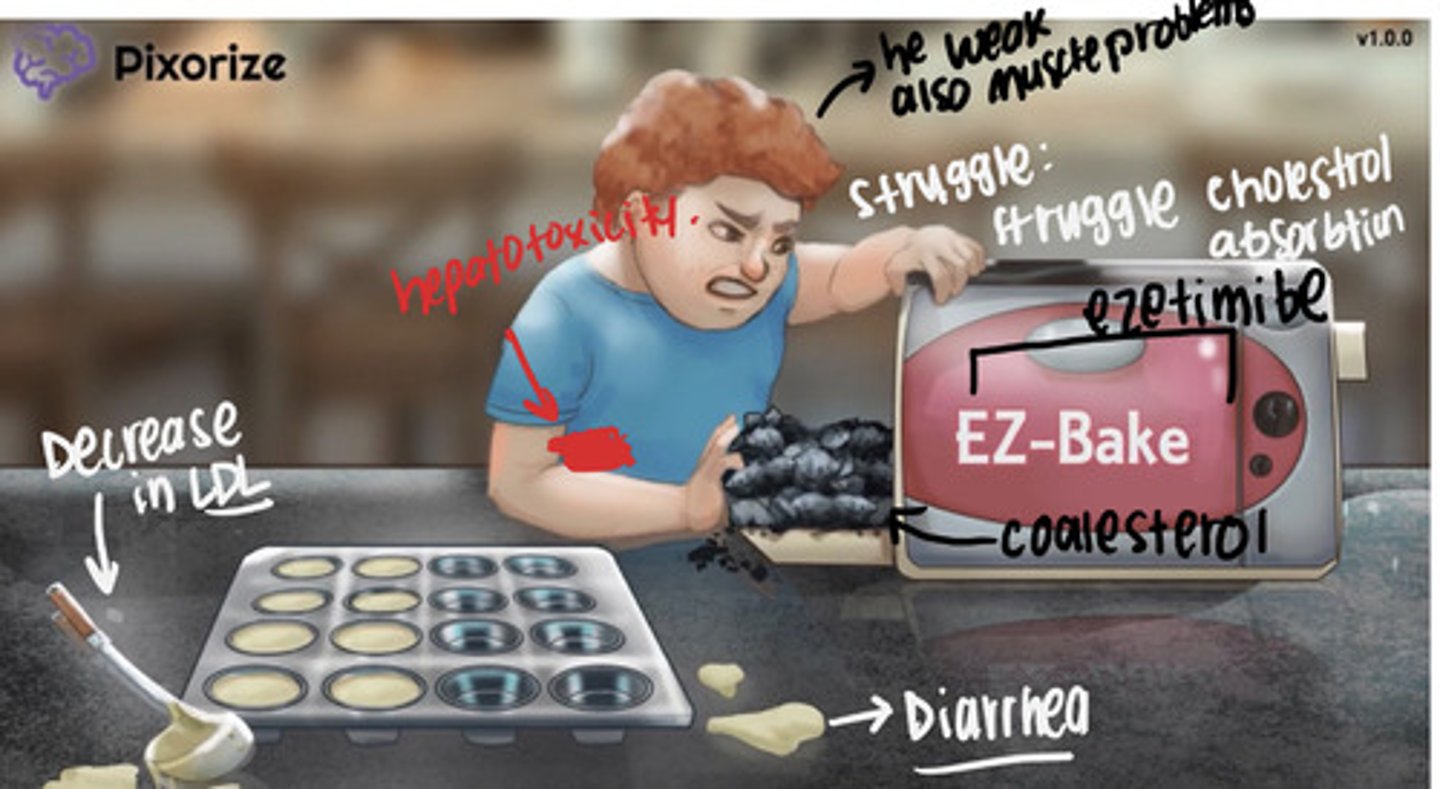
Cholesterol absorption (ezetimibe)
inhibits absorption of cholesterol
add on to statins
s/s: hepatitis, myopathy
PCSK9 (Alirocumab & Evolocumab) - For ppl who can't tolerate statins
sub q every two or more weeks (monotherapy)
Prevents breakdown of LDL receptors so more LDL receptors work and reduce LDL
s/s: hypersensitivity (rash, etc)
Adenosine
MOA: Slows conduction through AV nodes
Indication: supraventricular tachycardia (fast beat)
Uses: Short half-life (less then 10 seconds), only administered as fast IV push followed by saline
MAY BE ASYSTOLE FOR A FEW SECONDS (nurse should continue to monitor)
Class 1 Medication- Sodium Channel Blocker
slow cardiac conduction velocity
sodium blockers- divided into four groups (1 a, 1 b, 1 c)
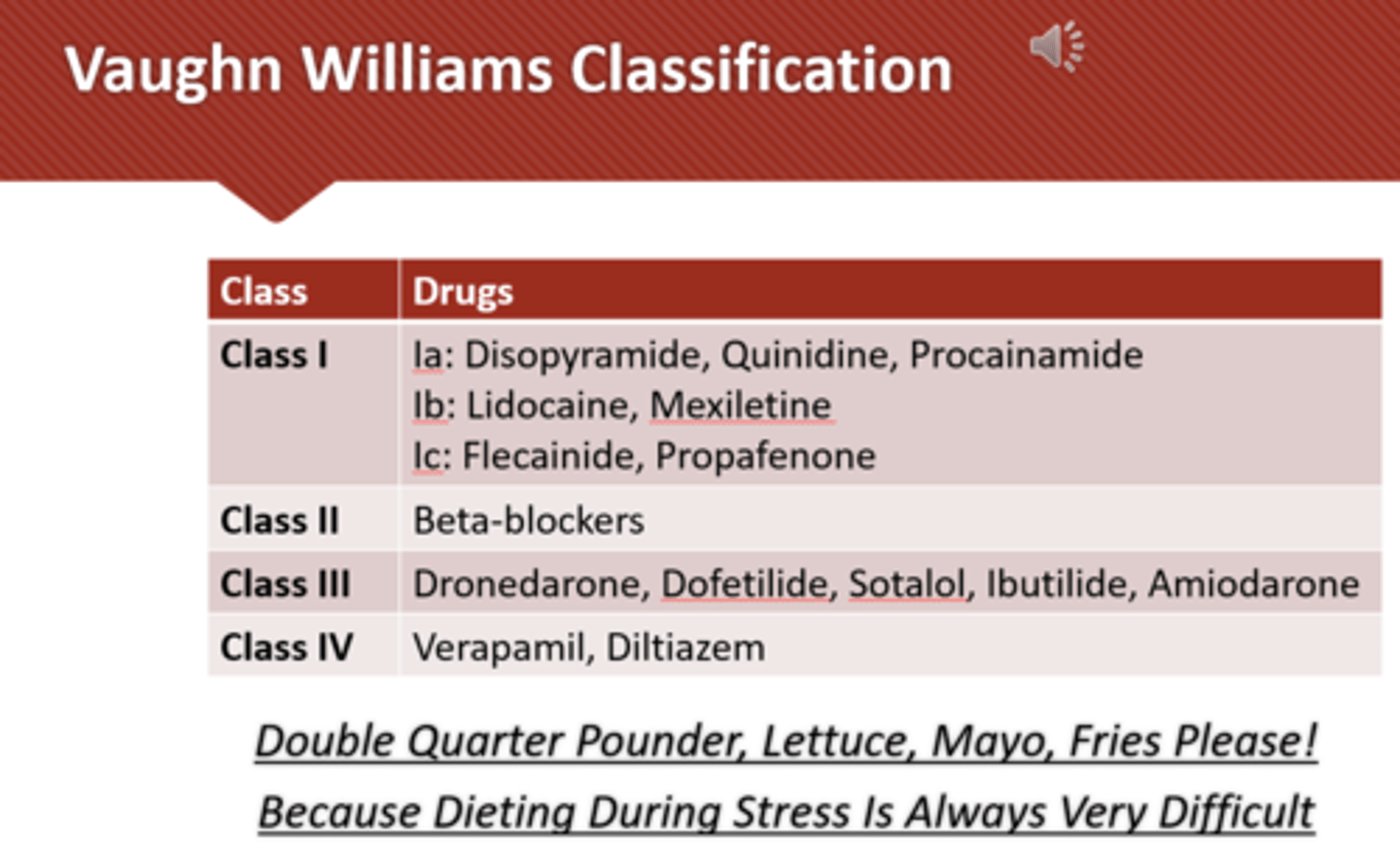
Antiarrhythmic Class 1A: disopyramide, quinidine, procainamide
MOA: block sodium (fast) channels,
slow impulse conduction, thus refractory (rest) lengthen
Indication: arrhythmias
S/S: diarrhea, cinchonism (n/v, tinnitus and stuff) ventricular dysrhythmias occur due to toxicity (proarrhythmic effect), hypotension, cardiotoxicity, black box for systemic lupus, blood dyscrasias
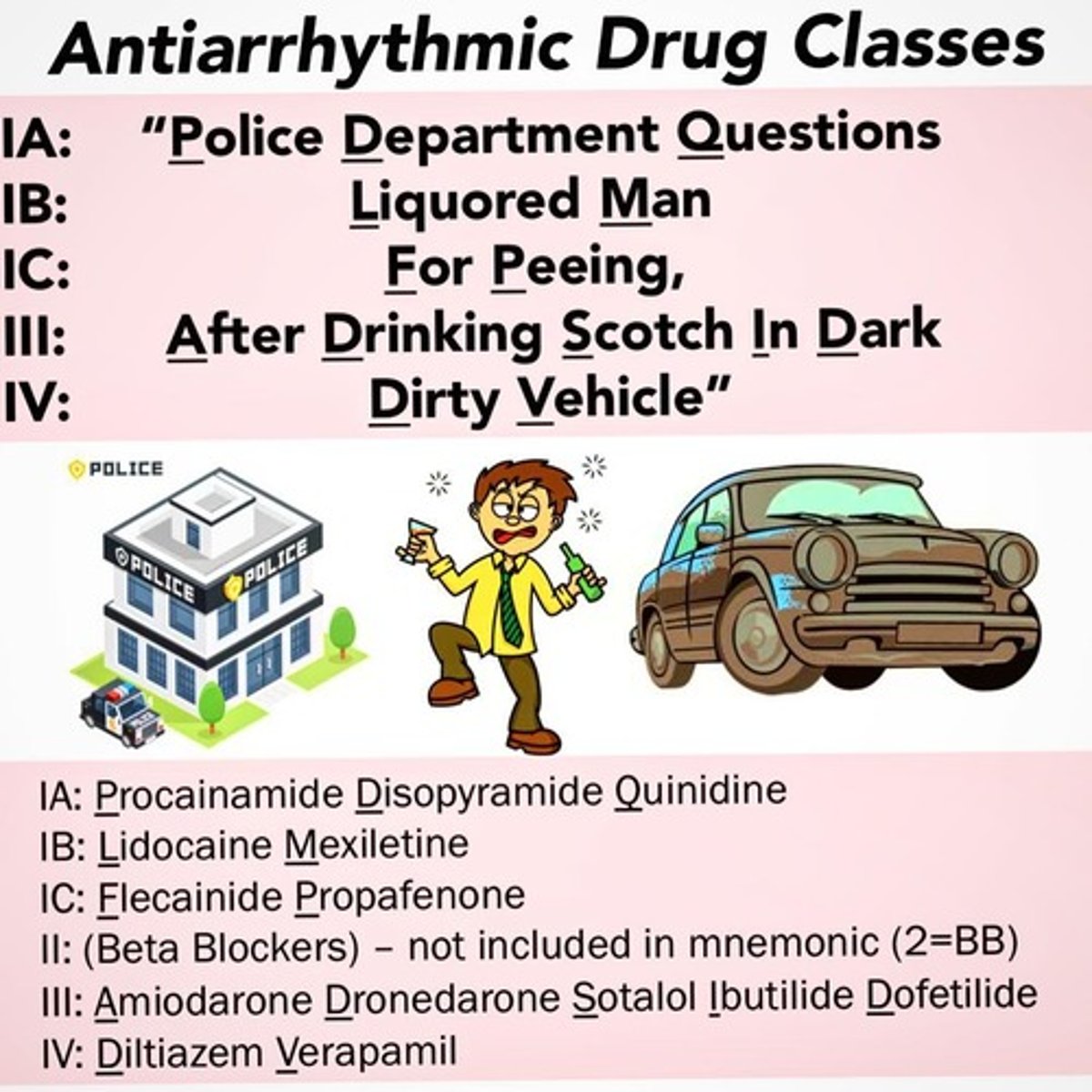
Antiarrhythmic Class 1B: phenytoin, lidocaine
MOA: Excrets small blockage of sodium channel, cell is then unables to respond to another stimulus (slows cardiac conduction)
IV or Local
Indication: Lidocaine is used for ventricular dysrhythmias only.
Phenytoin is used for atrial and ventricular tachydysrhythmias caused by digitalis toxicity or OT syndrome
These are both anesthetic
Adverse: CNS effect (toxicity), hypotension, bradycardia, heart block w/ high dose (respiratory arrest)
Antiarrhythmic Class 1C: flecainide, propafenone
MOA: block sodium channels (more pronounced effect), slows cardiac effect
Uses: severe ventricular dysrhythmias, may be used in atrial flutter, wolff- parkinson- white syndrome , SVT
Adverse: bradycardia, HF, dizzy, weak, hypotension, bronchospasms, multiple dysrhythmia (black box proarrhythmia consideration for increased mortality)
Class II: Beta-Adrenergic Blockers: labetalol
MOA: prevent sympathetic NS stimulation of the heart
Uses: angina, htn, arrhythmia, decrease mortality following MI, prophylaxis for headaches
Adverse: double low for the double LL (low hr and low bp), hf, av block, sinus arrest, fatigue, bronchospasm for clients with asthma
Beta- blockers and angina
By slowing the heart rate, beta blockers reduce the oxygen demand of the heart and reduce the frequency of angina attacks.
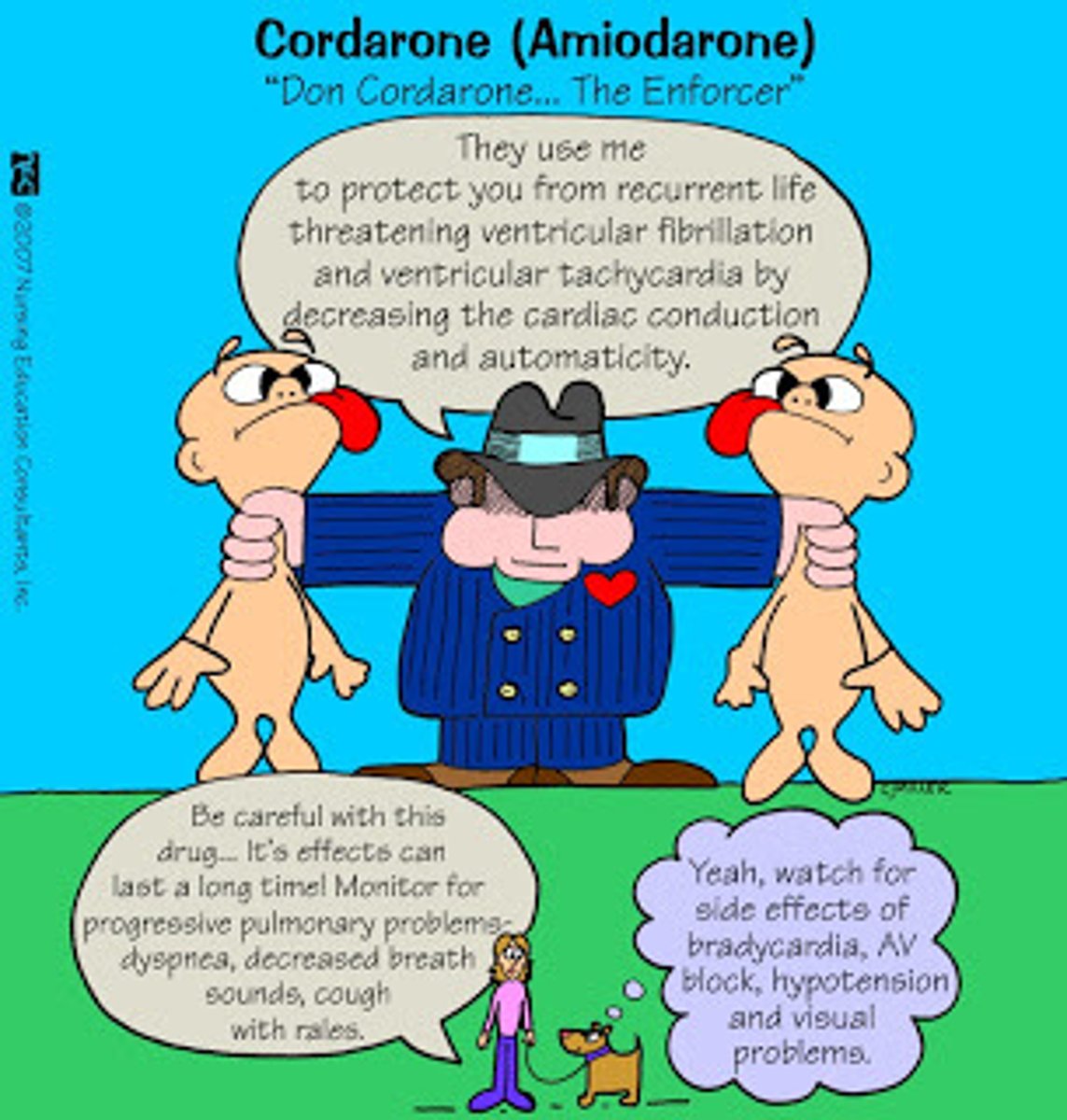
Class III Potassium Channel Blockers (Amiodarone, dronedarone, dofetilide, ibutilide)
MOA: increase APD, prolong repolarization in phase 3
Indication: life threatening ventricular fib, some atrial dysrhythmias
S/S: bradycardia, hypotension, arrhythmia, hepatotoxicity, pulmonary toxicity, skin sensitive to light, blue gray discoloration of skin
Blackbox: proarrhythmic effect, pulmonary toxicity, hepatotoxicity, phletitis w/ iv, hypotension, visual problems
NO GRAPEFRUIT JUICE, ASSESS both bp and hr and last for months
Class IV: Calcium Channel Blockers: Verapamil & Diltiazem
MOA: prolong cardiac conduction depress depolarization and decrease O2 demands of heart
Used: arrhythmias, HTN, angina
s/s: dysrhythmias, peripheral edema, HF, hypotension, av block
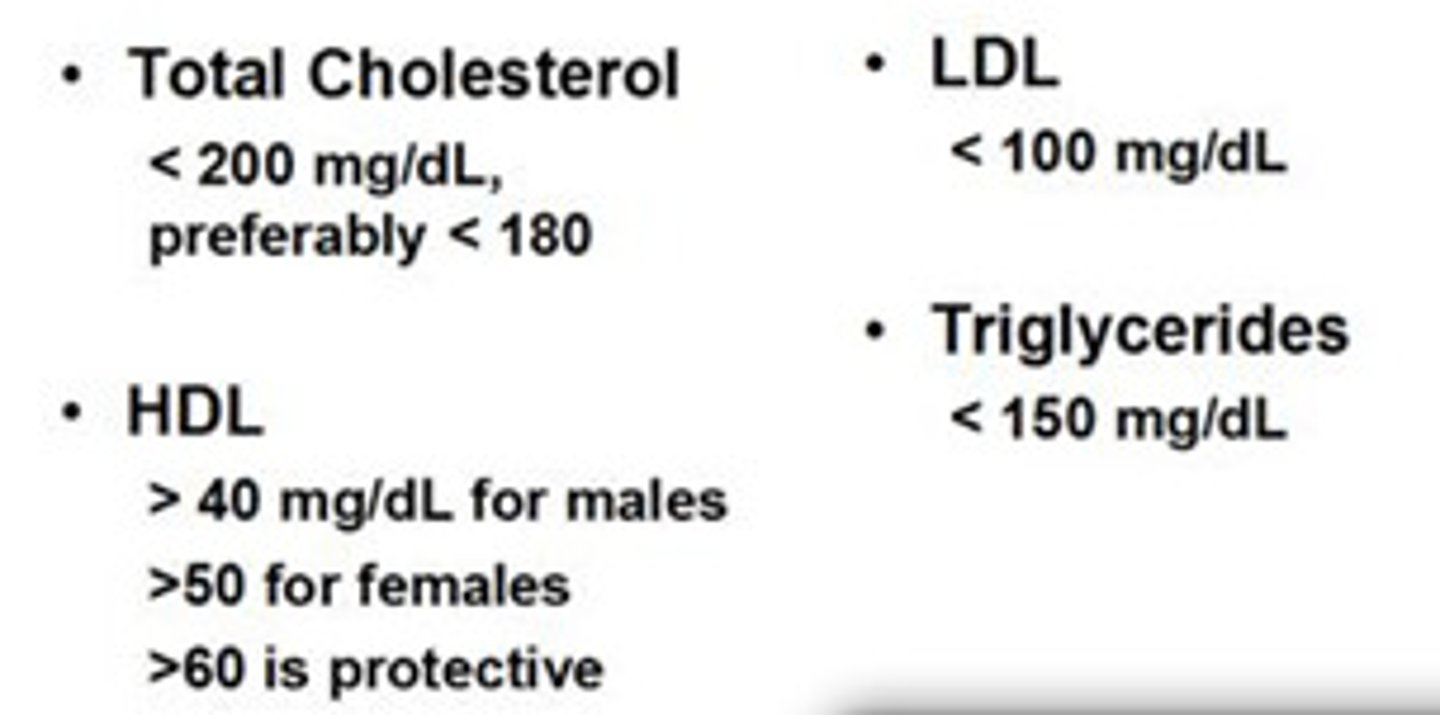
LDL cholesterol
bad cholesterol, "L" must keep low. should be under 100

HDL
Good cholesterol (High-density lipoprotein) "H" must keep high and happy
50 for females, 40 for males

Triglycerides
<150 mg/dL
Total Cholesterol
<200 mg/dL
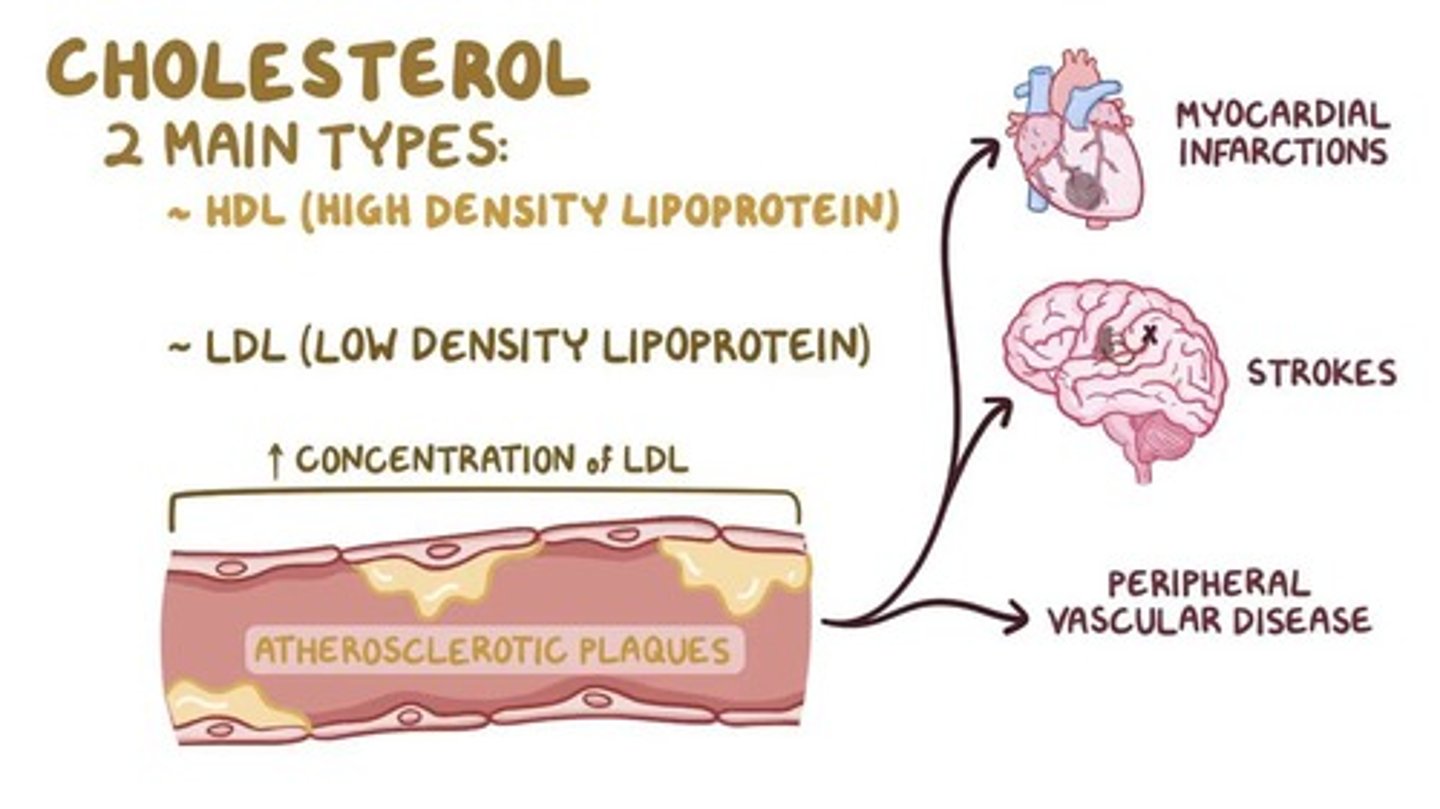
MI
Myocardial infarction (heart attack)
Caused by decreased or complete cessation of blood flow to a portion of the myocardium. (sometimes because atherosclerosis- build up of fat which can be caused by cholesterol)
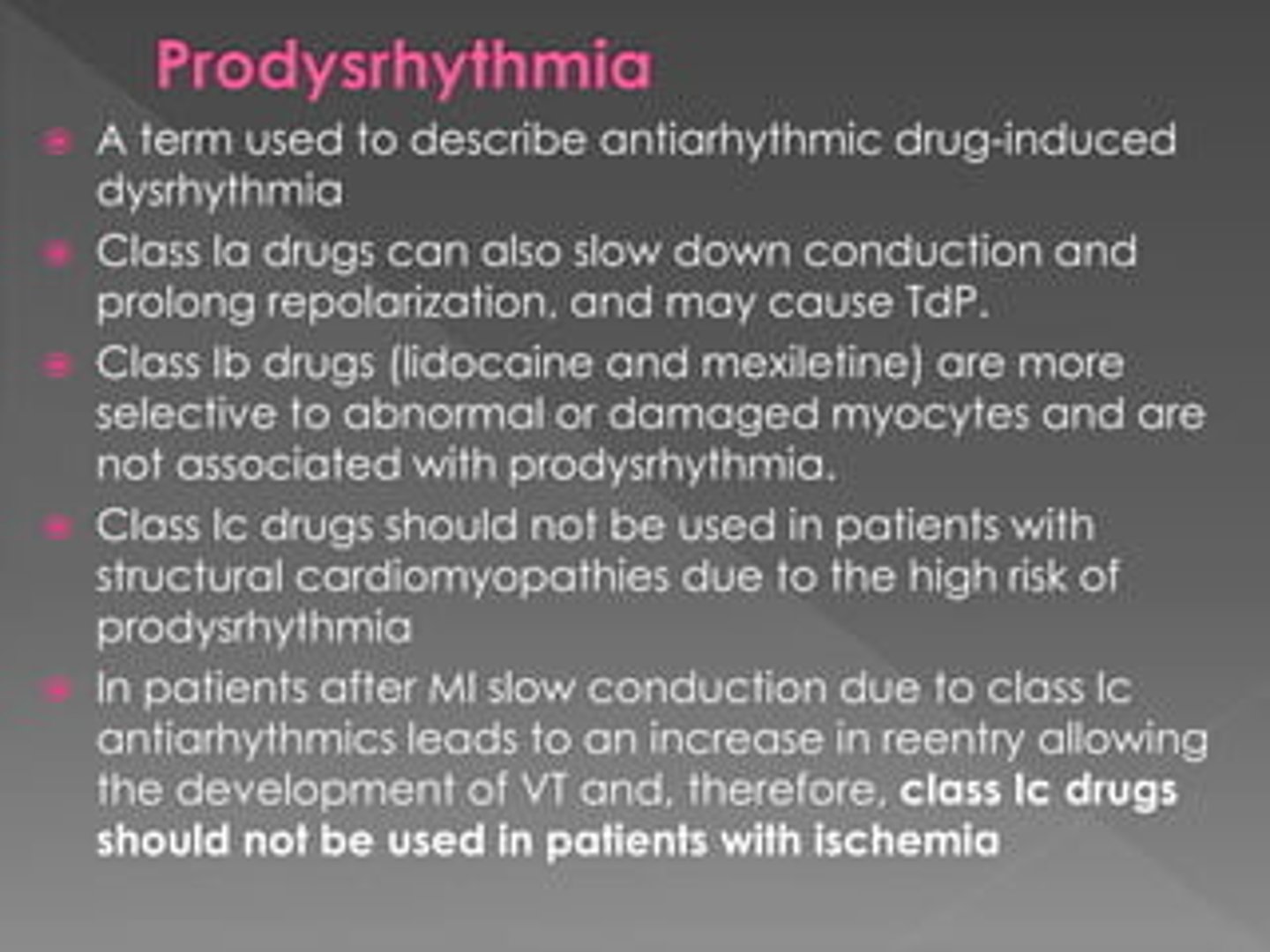
Prodysrhythmic Effects of Antidysrhythmic Drugs Toxicity
•Can worsen existing dysrhythmias and generate new ones
•Antidysrhythmic drugs should only be used when dysrhythmias are symptomatically significant
•Risks vs benefits should be considered
Which Medication causes cyanide toxicity ?
Nitroprusside