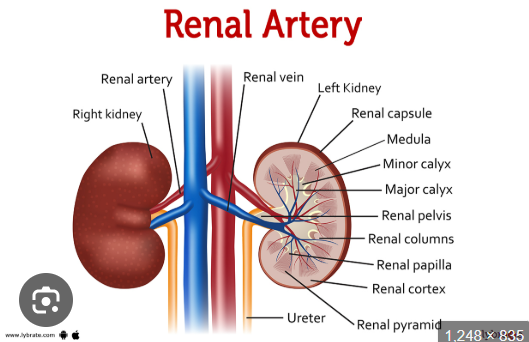
US ASSESSMENT OF THE RENAL ARTERIES
1/70
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
71 Terms
What is the normal kidney length?
What is the normal kidney width at the hilum?
What is the normal AP thickness of the kidney?
What is the normal kidney length?
→ 9–12 cm (relative to pt size)*
What is the normal kidney width at the hilum?
→ 4–5 cm
What is the normal AP thickness of the kidney?
→ 2.5–3.0 cm
Hilum means the “entry/exit doorway” of an organ.
For the kidney, the renal hilum is the area where important structures go in and out of the
Do both kidneys normally have approximately the same size?
What vertebral levels do the kidneys lie between?
Which kidney sits more caudal?
Do both kidneys normally have approximately the same size?
→ Yes
What vertebral levels do the kidneys lie between?
→ T12–L3
Which kidney sits more caudal?
→ Right kidney
How much lower is the right kidney compared to the left?
Why is the right kidney lower than the left kidney?
How much can the kidneys move during respiration?
How much lower is the right kidney compared to the left?
→ About 1–2 cm
Why is the right kidney lower than the left kidney?
→ Due to the liver
How much can the kidneys move during respiration? respiration = breathing.
→ 3–8 cm
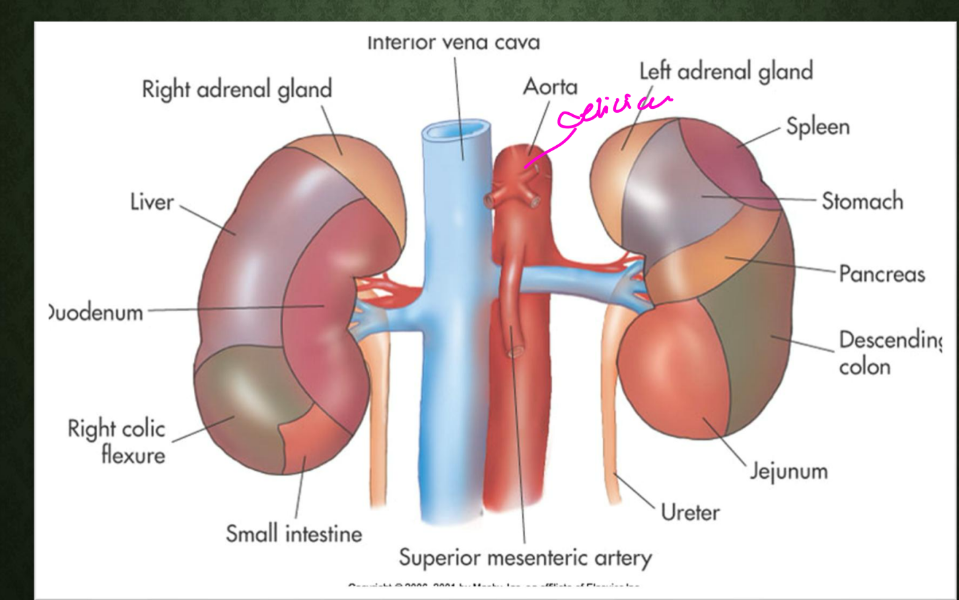
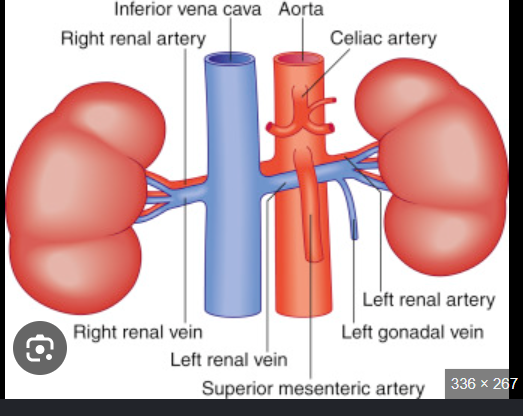
What major vessel lies posterior to the right renal vein?
The right renal artery passes posterior to what vessel?
What artery lies slightly above the renal arteries?
What major vessel lies posterior to the right renal vein?
→ Right renal artery
The right renal artery passes posterior to what vessel?
→ IVC
What artery lies slightly above the renal arteries?
→ SMA
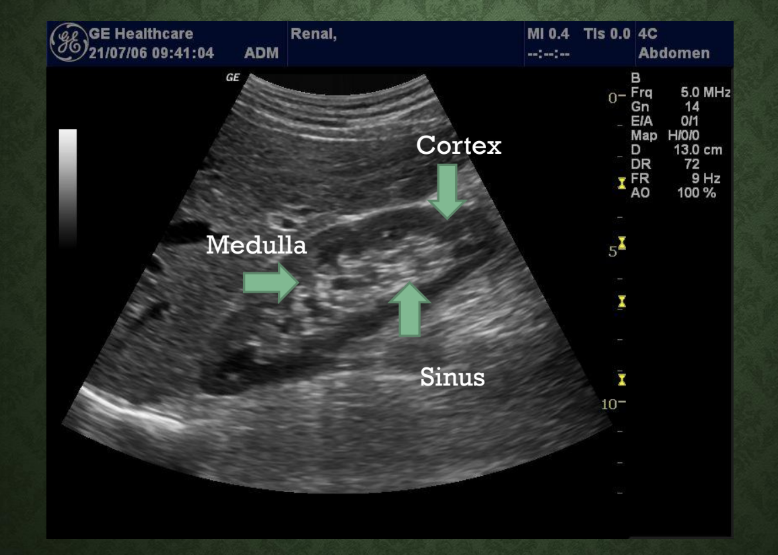
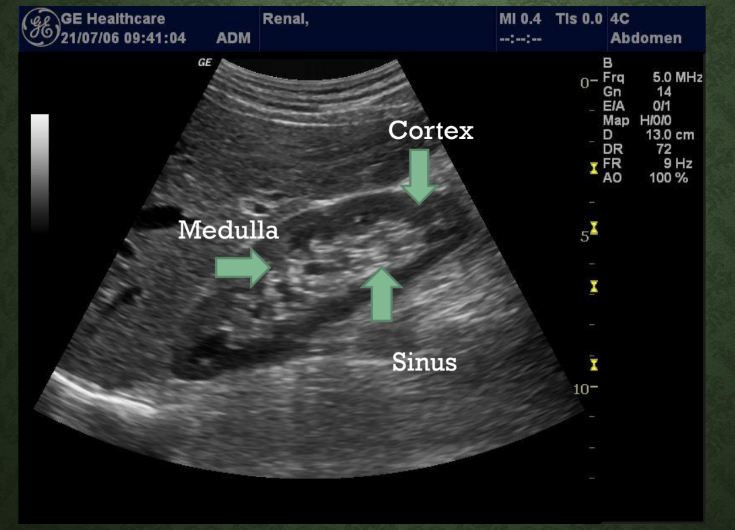
Name the 3 layers of the kidney.
Name the 3 layers of the kidney.
→ Cortex, medulla, renal pelvis
What is the cortex? which zone is it of the kidney?
What does the cortex contain?
Is the cortex hypoechoic or hyperechoic?
What type of echoes are seen in the cortex?
What is the cortex?
→ Outermost zone of the kidney
What does the cortex contain?
→ carries Convoluted tubules
Is the cortex hypoechoic or hyperechoic?
→ Hypoechoic
What type of echoes are seen in the cortex?
→ Low-level grey echoes
Convoluted tubules = tiny twisted kidney tubes that help filter blood and make urine.
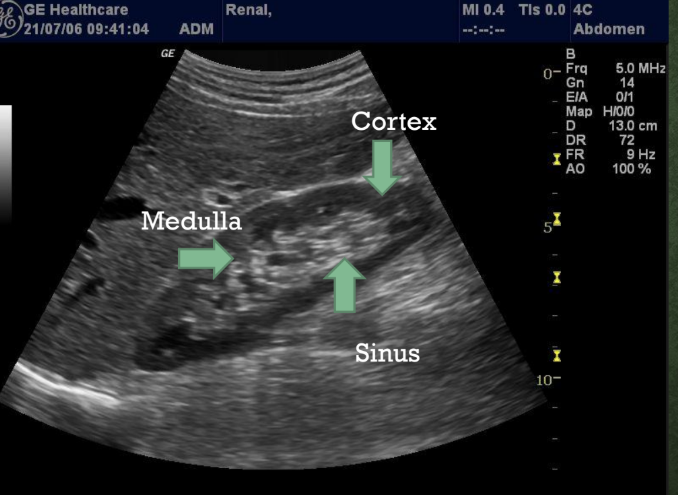
What is the medulla? what zone
How many renal pyramids are normally in the medulla?
Is the medulla hypoechoic or hyperechoic?
What is the medulla?
→ Middle zone of the kidney
How many renal pyramids are normally in the medulla?
→ 8–18 pyramids
Is the medulla hypoechoic or hyperechoic?
→ Hypoechoic
What is the renal pelvis? which zone ?
What shape is the renal pelvis?
Where is the renal pelvis located?
What is the renal pelvis continuous with?
How many minor calyces are normally present?
What is the renal pelvis?
→ Innermost zone of the kidney
What shape is the renal pelvis?
→ Triangular structure
Where is the renal pelvis located?
→ Within the renal sinus
What is the renal pelvis continuous with?
→ large cavity at Upper expanded end of ureters
How many minor calyces are normally present?
→ 8–18
The renal sinus is a central, fat-filled cavity inside the kidney. It acts as a protective hub or "lobby" for the structures that manage fluid and blood, securely housing the renal pelvis (which collects urine), blood vessels, nerves, and lymphatic channels as they enter and exit the organ.
Calyces (singular: calyx) are the cup-shaped, funnel-like structures in the kidney that act as the first stage of the urinary drainage system. They collect urine from the kidney's filtering units and channel it directly into the renal pelvis to be carried to the bladder.
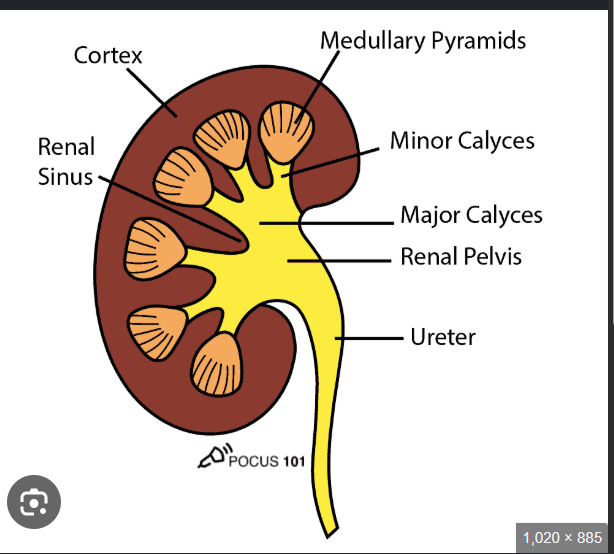
What do minor calyces receive?
How many major calyces are normally present?
What do major calyces receive?
What does the renal sinus contain?
What do minor calyces receive?
→ Fluid from pyramids
How many major calyces are normally present?
→ 3
What do major calyces receive?
→ Fluid from minor calyces
What does the renal sinus contain?
→ Major and minor calyces
Renal pyramids are cone-shaped tissues found inside the inner region of your kidneys. Their main job is to act as a plumbing system, transporting urine that has been filtered by the outer part of the kidney down to the tubes that carry it to your bladder
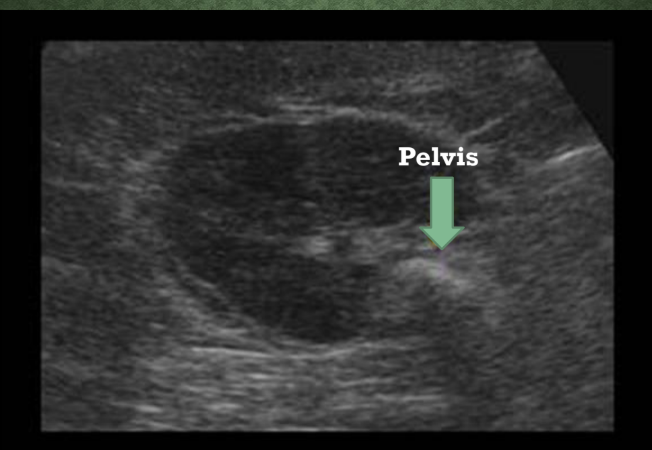
What structure is identified in the center of the kidney on this image?
What structure is identified in the center of the kidney on this image?
→ Renal pelvis
Name 3 major kidney functions.
removal of what
regulate what content - name 2
regulate what else
• Removal of wastes
• Regulate fluid and electrolyte content
• Regulate blood pressure
LAB TESTS******
What does BUN stand for?
What lab value evaluates kidney function?
What does UA stand for?
What does BUN stand for?
→ Blood urea nitrogen
What lab value evaluates kidney function?
→ Creatinine
What does UA stand for?
→ Uric acid
What does RBC stand for?
What does WBC stand for?
What test evaluates the urine?
What does RBC stand for?
→ Red blood cell count
What does WBC stand for?
→ White blood cell count
What test evaluates the urine?
→ Urinary analysis
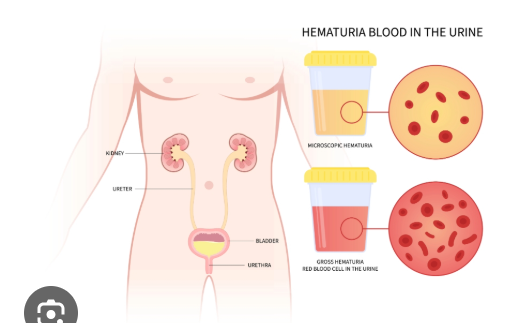
What does hematuria mean?
Name the 2 types of hematuria.
What does hematuria mean?
→ Blood in urine
Name the 2 types of hematuria.
→ Gross and microscopic hematuria
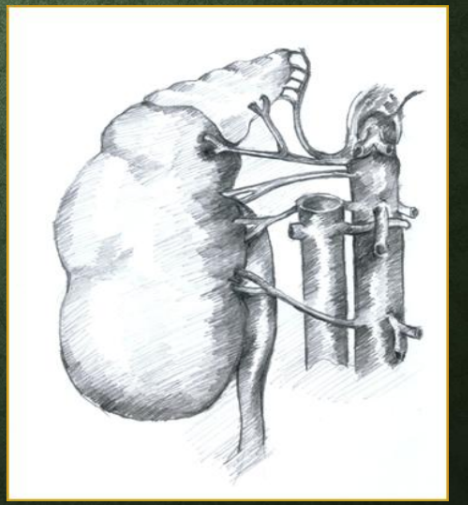
Where do the renal arteries arise from?
From what aspect does the right renal artery arise?
The right renal artery passes posterior to what structure?
Where do the renal arteries arise from?
→ Aorta slightly below the SMA
From what aspect does the right renal artery arise?
→ Anterolateral aspect of aorta
The right renal artery passes posterior to what structure?
→ IVC
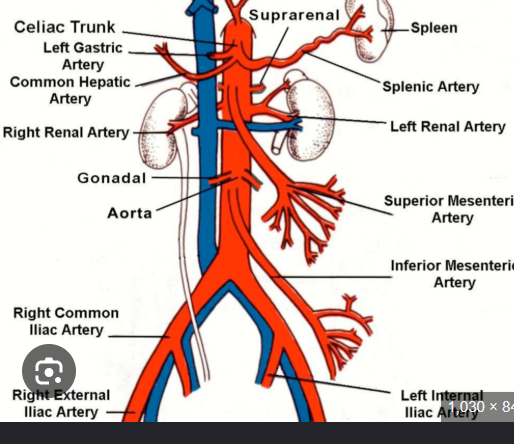
Where does the right renal artery course toward?
From what aspect does the left renal artery arise?
Where does the left renal artery course toward?
Where does the right renal artery course toward?
→ Right renal hilum
From what aspect does the left renal artery arise?
→ Lateral or posterolateral aspect
Where does the left renal artery course toward?
→ Left renal hilum
Approximately how many kidneys are supplied by multiple arteries?
What is main renal artery duplication?
What are accessory renal arteries?
Approximately how many kidneys are supplied by multiple arteries?
→ 1/3
What is main renal artery duplication?
→ Two main renal arteries supplying the kidney
What are accessory renal arteries?
→ Additional arteries supplying the kidney
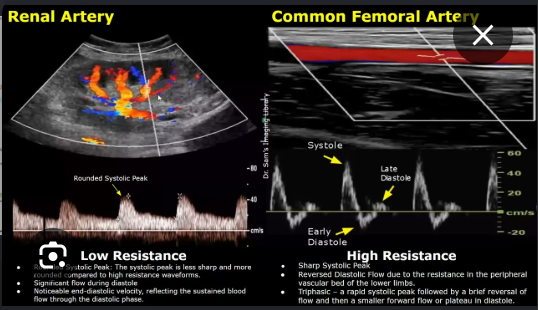
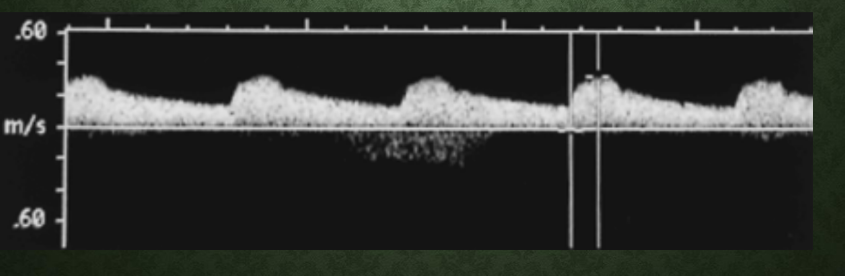
What type of Doppler waveform do renal arteries normally have?
Why are renal artery waveforms ^ resistance?
What type of Doppler waveform do renal arteries normally have?
→ Low resistance waveform
Why are renal artery waveforms low resistance?
→ Kidneys require constant perfusion
MAIN RENAL ARTERIES
What scan plane can image renal artery origins from the front? (anterior approach)
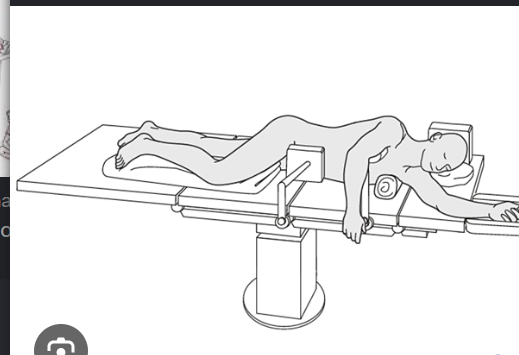
What patient position is used for coronal renal artery imaging?
What transducer approach may be used in decubitus imaging?
What acts as the acoustic window for renal artery imaging?
What scan plane can image renal artery origins from the front?
→ Transverse midline anterior approach
What patient position is used for coronal renal artery imaging?
→ Decubitus position
What transducer approach may be used in decubitus imaging?
→ Posterolateral approach
What acts as the acoustic window for renal artery imaging?
→ Kidney
What waveform characteristic is normally seen in renal arteries?
Why do renal arteries normally have continuous diastolic flow?
What waveform characteristic is normally seen in renal arteries?
→ Low resistance flow
Why do renal arteries normally have continuous diastolic flow?
→ Kidneys require continuous perfusion
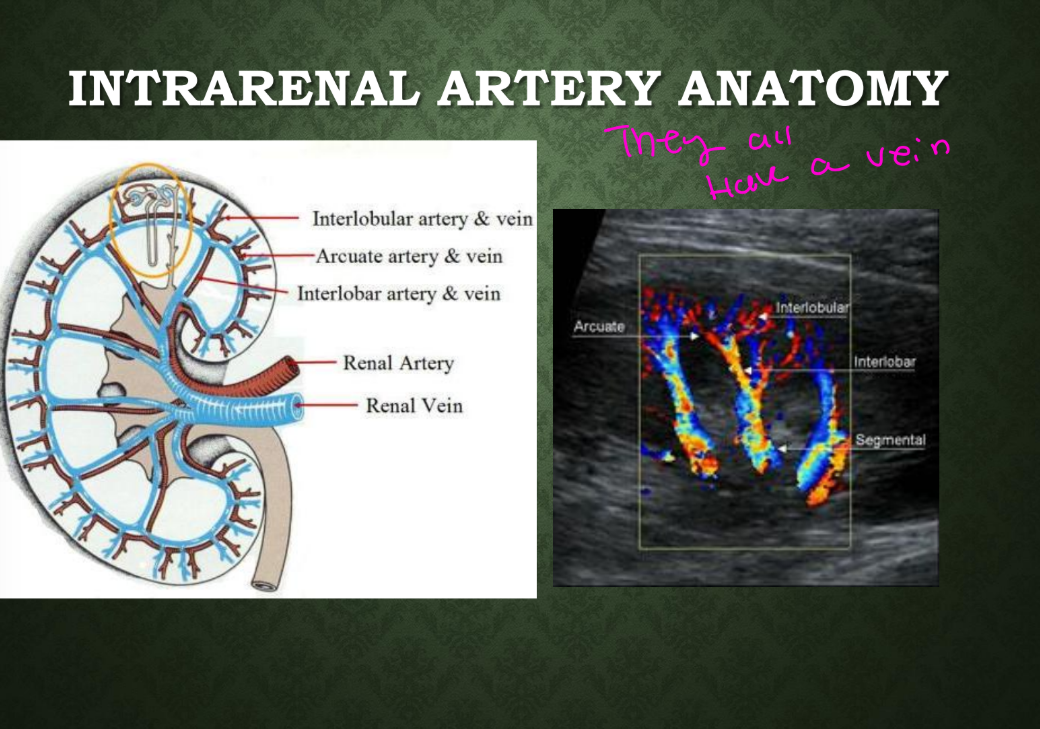
INTRARENAL ARTERY ANATOMY
What are the first branches of the main renal artery? and where do they course?
What arteries arise from the segmental arteries?
Where do interlobar arteries lie?
What do interlobar arteries penetrate?
What are the first branches of the main renal artery?
→ Segmental renal arteries
Where do segmental arteries course?
→ Through the hilum
What arteries arise from the segmental arteries?
→ Interlobar arteries
Where do interlobar arteries lie?
→ Between the pyramids
What do interlobar arteries penetrate?
→ Renal parenchyma
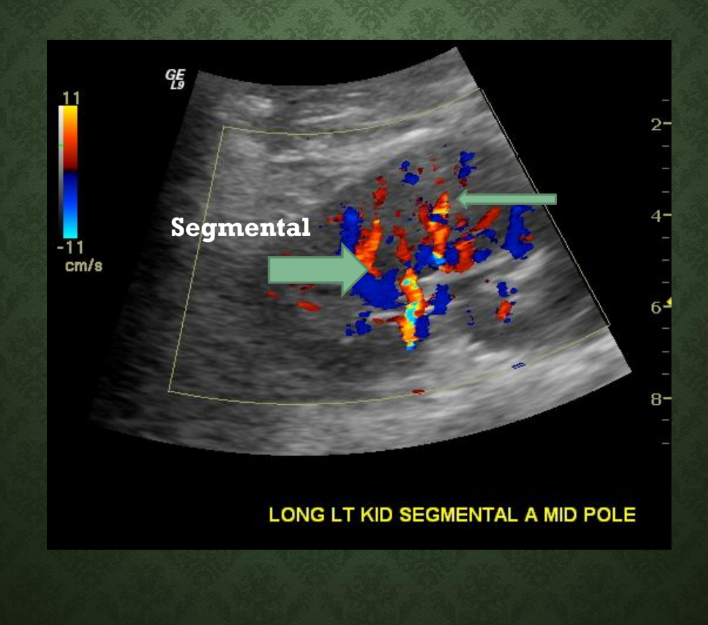
What 2 intrarenal arteries are labeled in this image?
What 2 intrarenal arteries are labeled in this image?
→ Segmental and interlobar arteries
INTRARENAL ARTERY ANATOMY
What arteries arise from interlobar arteries?
How do arcuate arteries course?
What arteries arise from arcuate arteries?
Where do interlobular arteries extend?
What arteries arise from interlobar arteries?
→ Arcuate arteries
How do arcuate arteries course?
→ Parallel to cortical surface
What arteries arise from arcuate arteries?
→ Interlobular arteries
Where do interlobular arteries extend?
→ Cortex
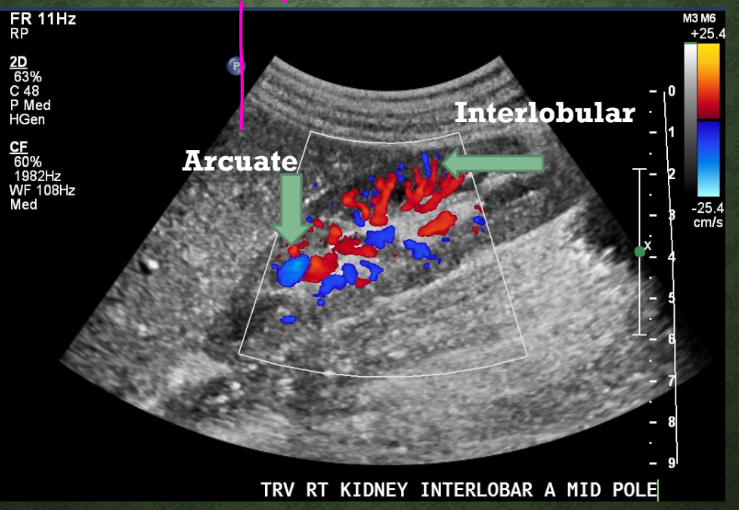
Which renal artery runs parallel to the cortical surface?
Which renal artery runs parallel to the cortical surface?
→ Arcuate artery
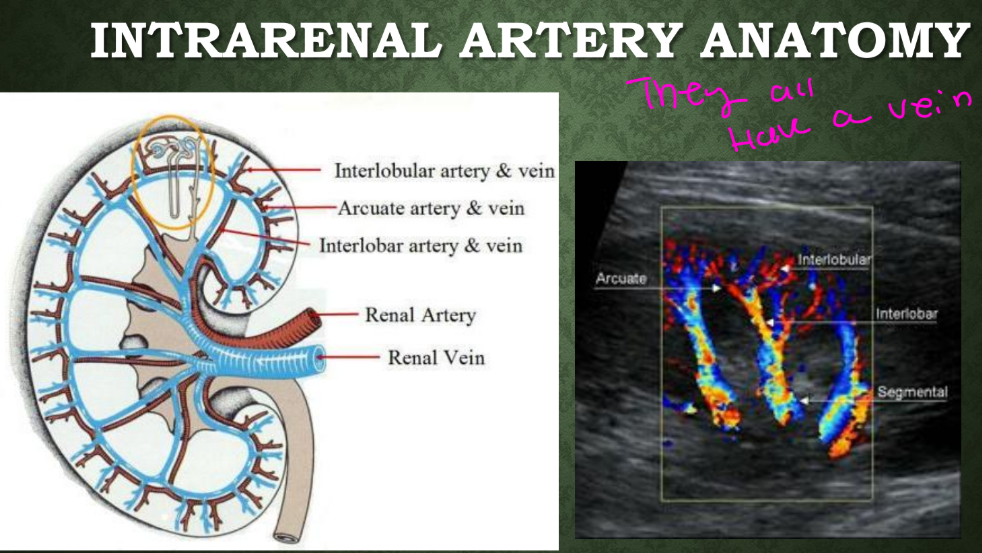
What vessels usually accompany the renal arteries?
What vessels usually accompany the renal arteries?
→ Renal veins
How many branches unite to form the main renal veins?
At what vertebral level do renal veins arise?
Are the renal veins anterior or posterior to the renal arteries?
Why does the IVC enlarge above the renal veins?
What type of waveform do renal veins normally have?
How many branches unite to form the main renal veins?
→ 5–6 branches
At what vertebral level do renal veins arise?
→ L2
Are the renal veins anterior or posterior to the renal arteries?
→ Anterior
Why does the IVC enlarge above the renal veins?
→ Increased blood volume from kidneys
What type of waveform do renal veins normally have?
→ Phasic and pulsatile waveform
Where does the left renal vein course from?
The left renal vein passes posterior to what artery?
The left renal vein passes anterior to what vessel?
How does the left renal vein appear on longitudinal imaging?
How does the left renal vein appear on transverse imaging?
Where does the left renal vein enter?
Which renal vein is larger?
Where does the left renal vein course from?
→ Left kidney
The left renal vein passes posterior to what artery?
→ SMA
The left renal vein passes anterior to what vessel?
→ Aorta
How does the left renal vein appear on longitudinal imaging?
→ Circular structure
How does the left renal vein appear on transverse imaging?
→ Tubular structure
Where does the left renal vein enter?
→ Lateral aspect of IVC
Which renal vein is larger?
→ Left renal vein
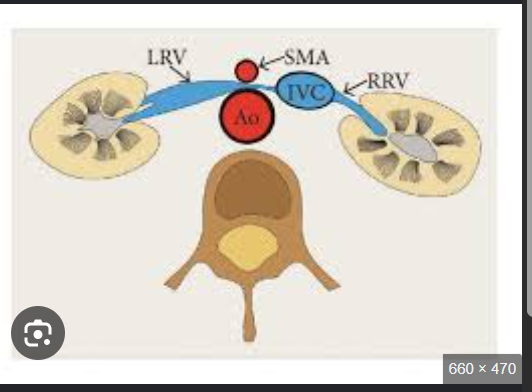
The left renal vein lies between what 2 vessels?
The left renal vein lies between what 2 vessels?
→ SMA and aorta
Where does the right renal vein course from?
Where does the right renal vein enter the IVC?
Which renal vein is shorter?
What scan plane best visualizes the right renal vein?
Where does the right renal vein course from?
→ Right kidney
Where does the right renal vein enter the IVC?
→ Posterolateral aspect
Which renal vein is shorter?
→ Right renal vein
What scan plane best visualizes the right renal vein?
→ Transverse plane
What Doppler waveform is expected in renal veins?
What Doppler waveform is expected in renal veins?
→ Phasic venous waveform
SONOGRAPHIC TECHNIQUE
What transducer is typically used for renal duplex?
Name 4 patient approaches used in renal sonography. (Utilize all available acoustic windows)
What approach may help evaluate renal artery origins in large patients?
What does decubitus mean?
What does oblique position mean?
What transducer is typically used for renal duplex?
→ Curvilinear 2–5 MHz transducer
Name 4 patient approaches used in renal sonography.
→ Anterior, flank, oblique, decubitus
What approach may help evaluate renal artery origins in large patients?
→ Flank approach
What does decubitus mean?
→ Patient lying on their side
What does oblique position mean?
→ Patient partly on their side
(Patient in variable positions)
SONOGRAPHIC TECHNIQUE
What patient preparation is recommended before renal duplex?
Are clear liquids and medications allowed before exam?
Is anti-gas medication optional?
What time of day is preferred for renal duplex?
Should the patient be dehydrated?
What patient preparation is recommended before renal duplex?
→ Overnight fast
Are clear liquids and medications allowed before exam?
→ Yes
Is anti-gas medication optional?
→ Yes
What time of day is preferred for renal duplex?
→ Morning
Should the patient be dehydrated?
→ No
RENAL AND RENAL DUPLEX EXAM PROTOCOL - SEQUENCE, whats the protocol for the renal arteries for rt side and ao
RT Kidney _____ scale in LONG name 4 steps
RT kidney_____ scale TRANS name 4 steps
SAG of Right kidney : (what are you using name 5/6)
RT ______-Artery name 3 steps
RT Renal ____ name 1 what dopplers name 2 and what is not required?
RT _____ ______ artery name name the dopplers you would use 3, and the 4 steps you evluate
Aorta at the level of the_______ _______
name 4 steps you do
Rt Kidney Grey Scale
• Long
• Lateral, Mid – with and without color Doppler, Mid – with length and AP measurement, Medial
• Trans, Superior, Mid, Mid – with width measurement, Inferior
SAG Segmental Arteries of right kidney: color and spectral Doppler (PSV, EDV, RI; w/o angle correction)
Rt Segmental Artery, Superior pole , Mid pole , inferior pole
• SAG Rt Renal Vein, Hilum only (color and spectral Doppler (velocity measuremnet not required)
• SAG right main renal artery (color and spectral Doppler (PSV with angle correction) Distal, Mid, Proximal, Origin / Ostia
SAG Aorta at the level of the renal arteries, • Grey scale, Color Doppler, & Spectral Doppler, PSV with angle correction)
Renal vein at hilum only: Use color and spectral Doppler to confirm the vein is patent and has flow. Velocity measurement is not required because renal duplex diagnosis focuses on arterial velocities and resistance patterns.
In renal duplex, the important velocity measurements are mainly for the renal arteries, especially PSV, EDV, RAR, RI, and signs like tardus parvus. Your slide specifically says for the renal vein: no velocity measurement needed.
The ostium (opening) of the right main renal artery is located on the anterolateral wall of the abdominal aorta, just below the superior mesenteric artery
A hilum (or renal hilum) is simply the indented, "doorway" area on the inner side of the bean-shaped kidney. It is the specific spot where blood vessels, nerves, and the urine tube (ureter) enter and exit the organ. [1, 2, 3]
RENAL AND RENAL DUPLEX
EXAM PROTOCOL - SEQUENCE for left side & LIST WHAT WE DIDNT DISSCUSS!
same as RT
Lt Kidney Grey Scale
• Long, Lateral, Mid – with and without color Doppler, Mid – with length and AP measurement, Medial
• Trans, Superior, Mid, Mid – with width measurement, Inferior
Lt Segmental Artery, Superior, Mid, inferior
Lt Renal Vein, Hilum only
• Lt Main Renal Artery, Distal, Mid, Proximal, Origin / Ostia
Intraparenchymal arteries, No angle correction, RI ratio
• Accessory renal artery / arteries:
• Distal
• Mid
• Proximal
• Origin / Ostia
RENAL DUPLEX ONLY
EXAM PROTOCOL - SEQUENCE
for rt side and ao
Sag Rt Kidney GS with
• Length measurement only
•
Sag Rt Segmental Arterys of RT kidney : CD, SD PSV, EDV, RI; w/o angle correction)
• Superior pole
• Mid pole
• Inferior pole
•
Sag Rt Renal Vein
• At hilum only with CD and SD (velocity measurement not required)
•
Sag Rt Main Renal Artery, CD, SD PSV with angle correction
• Distal
• Mid
• Proximal
• Origin / Ostia
• SAG Aorta at the level of the renal arteries
• Grey scale
• Color Doppler
• Spectral Doppler
(PSV with angle correction)
RENAL DUPLEX ONLY
EXAM PROTOCOL - SEQUENCE left side and the rest
Sag Lt Kidney
• Length measurement only
•
Sag Lt Segmental Artery
• Superior
• Mid
• Inferior
•
Sag Lt Renal Vein
• At hilum only
•
Sag Lt Renal Artery
• Distal
• Mid
• Proximal
• Origin / Ostia
Intraparenchymal arteries
• No angle correction
• RI ratio
•
Renal vein
• No velocity measurement needed
•
Accessory renal artery / arteries
• Distal
• Mid
• Proximal
• Origin / Ostia
TECHNICAL TIPS
When using spectral Doppler on small vessels, what should be done?
What Doppler angle should be used in renal duplex?
How much of the spectral display PRF should the waveform occupy?
When using spectral Doppler on small vessels, what should be increased?
→ increase Sample volume size for smaller vessels
What Doppler angle should be used in renal duplex?
→ ≤60°
How much of the spectral display should the waveform occupy?
→ About 2/3 of display
TECHNICAL TIPS
Why is lower (slower) sweep speed used?to improve visualization of what?
When should optimization be performed during the exam?
Should deep inspirations be minimized or exaggerated?
Can adjustments be made using a frozen image?
Name 2 adjustments that may be changed on frozen spectral Doppler.
Why is slower sweep speed used?
→ Improve visualization of systolic acceleration (breathing holdings issues from pt)
When should optimization be performed during the exam?
→ Before patient suspends respiration (temporaly stop breathing)
Should deep inspirations be minimized or exaggerated?
→ Minimized
Can adjustments be made using a frozen image?
→ yes, Minor adjustments may be made from frozen image
Name 2 adjustments that may be changed on frozen spectral Doppler.
→ Scale/PRF and spectral gain, sweep speed
That is why your renal duplex slide says to use a lower/slower sweep speed to improve visualization of systolic acceleration. This helps you evaluate things like acceleration time and tardus parvus, where you need to see if the waveform is slow to rise.
Simple card:
Slower sweep speed = stretches the waveform horizontally and shows fewer beats, making systolic acceleration easier to see.
What renal arteries should show similar Doppler waveform patterns?
What type of flow is normal in renal arteries?
What happens to spectral broadening deeper into the renal parenchyma?
What does absent or reduced end diastolic flow indicate?
Name 3 causes of absent/reduced end diastole.
What renal arteries should show similar Doppler waveform patterns?
→ All of the renal arteries (from main to arcuate) should show similar Doppler waveform patterns
What type of flow is normal in renal arteries?
→ Low resistance antegrade flow
What happens to spectral broadening deeper into the renal parenchyma?
→ Increases
What does absent or reduced end diastolic flow indicate?
→ Increased distal resistance (Indicates resistance to flow distally)
Name 3 causes of absent/reduced end diastole.
→ Obstructed renal artery, medical renal disease, renal vein thrombosis
Because as you sample deeper into the kidney tissue, the arteries get smaller and more branched, so the blood flow becomes a little less uniform.
Spectral broadening means the Doppler waveform looks more “filled in” instead of having a clean empty window under the peak. It happens when the sample volume is picking up blood cells moving at different speeds and directions.
In the renal arteries:
Main renal artery = larger vessel, more organized flow → cleaner waveform
Segmental/interlobar/arcuate arteries inside parenchyma = smaller branching vessels → more mixed velocities → more spectral broadening
That is why your slide says increase in spectral broadening is seen as sampling is made further into the parenchyma. It can be a normal finding as you move farther into the small intrarenal vessels.
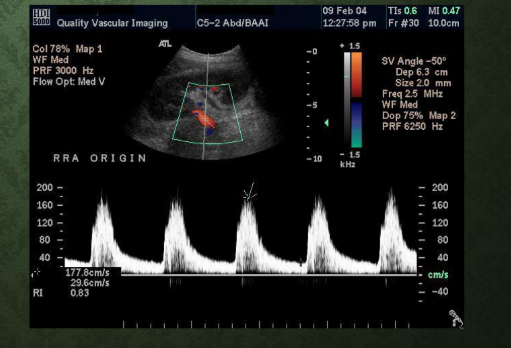
What is the normal renal artery PSV range?
What RI range is considered normal?
What type of waveform is normal in renal arteries?
What is the normal renal artery PSV range?
→ 100–150 cm/sec
What RI range is considered normal?
→ 0.5–0.7
What type of waveform is normal in renal arteries?
→ Low resistance waveform

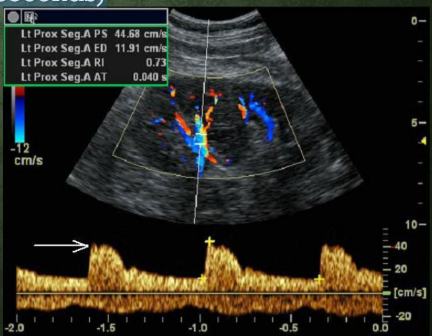
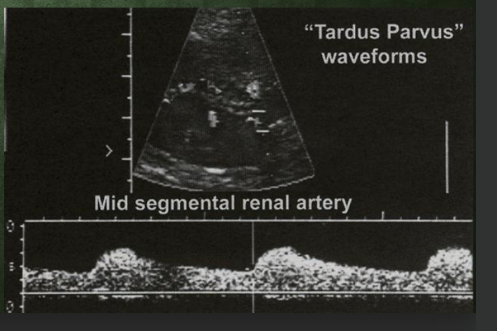
What is tardus parvus? describe the waveform….
What does tardus parvus indicate?
What happens to acceleration time in tardus parvus?
What is tardus parvus?
→ Waveform slow to rise and fall
What does tardus parvus indicate?
→ sign of Proximal obstruction
What happens to acceleration time in tardus parvus?
→ Prolonged/long acceleration time
What do renal Doppler ratios help evaluate? indication for…..
What does RI stand for?
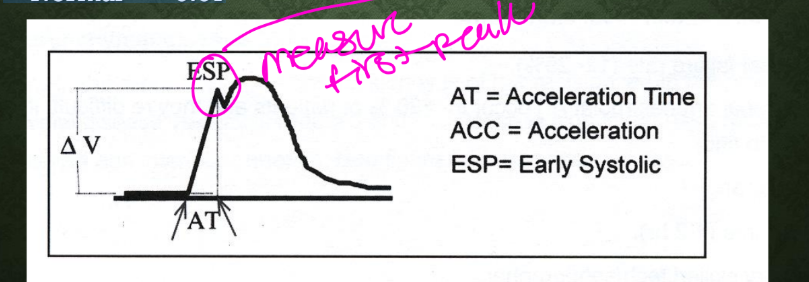
What does AT stand for?
Name 3 sonographic indicators of renal disease.****
What do renal Doppler ratios help evaluate?
→ Parenchymal resistance
What does RI stand for?
→ Resistive index
What does AT stand for?
→ Acceleration time
Name 3 sonographic indicators of renal disease.
→ Kidney length ≤9 cm, >2 cm size discrepancy, increased echogenicity
What kidney size suggests renal disease?
→ 9 cm or less
What kidney size discrepancy suggests renal disease?
→ Greater than 2 cm difference between kidneys
(example Pt who has CKD & HTN indication for US)
Name 3 findings of critical renal artery stenosis. waveform
Why should accessory renal arteries be evaluated?
What should be looked for on the aorta when evaluating accessory arteries?
What approach helps identify multiple renal arteries?
Name 3 findings of critical renal artery stenosis.
→ Flow jet, post-stenotic turbulence, tardus parvus
Why should accessory renal arteries be evaluated?
→ May contribute to renal disease/HTN
What should be looked for on the aorta when evaluating accessory arteries?
→ Look for multiple arterial take off from the aorta
What approach helps identify multiple renal arteries?
→ Use a coronal approach to look for multiple
arteries feeding the kidney
RENAL SONOGRAPHY INDICATIONS
Name 3 indications for renal sonography.
What is the purpose of renal duplex in hypertension?
Name 3 indications for renal sonography.
→ Vascular HTN evaluation, medical renal disease, elevated renal function tests
What is the purpose of renal duplex in hypertension?
→ Identify vascular etiology
ETIOLOGY RENAL HYPERTENSION
What is the most common cause of renal hypertension?
Where does ^^^^renal disease usually occur?
What does FMD stand for? ____— occurrence, and on angiogram demonstreates a what apparance of the renal arteries
Where does FMD usually occur in the renal artery?
What other pathology can cause renal hypertension besides atherosclerosis and FMD?
How many patients in the USA are affected by renal hypertension?
What is the most common cause of renal hypertension?
→ Atherosclerosis
Where does atherosclerotic renal disease usually occur?
→ Proximal renal artery b/c of the Bifurcation)
because plaque commonly forms near vessel origins/branch points where there is more turbulent flow and wall stress
What does FMD stand for?
→ Fibromuscular dysplasia, Common occurrence,
on angiogram demonstreates a beaded apparance of the renal arteries
Where does FMD usually occur in the renal artery?
→ Mid to distal segment
What other pathology can cause renal hypertension besides atherosclerosis and FMD?
→ Aortic dissection extension/dissection
How many patients in the USA are affected by renal hypertension?
→ About 20 million
Name the 2 renal sonography methods.
Name the 2 renal sonography methods.
→ Direct and indirect methods
DIRECT METHOD
What does the direct renal duplex method evaluate? name 3
Limitations;
Undetected WHAT renal artery is a potential cause of what?****
List 4 Limitations of the direct method…
What does the direct renal duplex method evaluate?
→ Renal arteries/accessory arteries and renal veins
Undetected WHAT renal artery is a potential cause of what?****
Undetected accessory renal artery is a potential cause of
renovascular hypertension
List 4 Limitations of the direct method…
Inability to image entire length of both renal arteries
• Obesity
• Bowel gas
• Patient inability to hold breath
Reno = kidney
Vascular = blood vessels
HTN = high blood pressure
So renovascular HTN means high blood pressure caused by a problem with the blood vessels going to the kidneys, usually renal artery narrowing/stenosis.
Simple idea:
If the renal artery is narrowed, the kidney thinks, “I’m not getting enough blood.”
So the kidney releases renin, which starts the RAAS system and raises BP.
Name 2/ 3 kidney characteristics evaluated in the direct method.
Why is the aorta evaluated during direct renal duplex?
What aortic Doppler value is obtained?
^why do we do that what ratio are we trying to get?
Name 2 kidney characteristics evaluated in the direct method.
→ Size and morphology/echogenicity
Why is the aorta evaluated during direct renal duplex?
→ Evaluate for aortic disease
What aortic Doppler value is obtained?
→ Mid-aortic PSV
^why do we do that what ratio are we trying to get?
→ Used for renal artery – aorta ration (RAR)

What approach is used to identify renal artery origins?
What velocities are measured in renal duplex?
Name the 3 renal artery segments evaluated with velocities.
What index is determined during renal duplex?
What additional arteries should always be noted?
What approach is used to identify renal artery origins?
→ Transverse HH approach
HH most likely stands for “heel-toe” approach/maneuver.
What velocities are measured in renal duplex?
→ PS and ED velocities
Name the 3 renal artery segments evaluated with velocities.
→ Proximal, mid, distal
What index is determined during renal duplex?
→ Resistive index
What additional arteries should always be noted?
→ Secondary/accessory renal arteries

Name 3 diagnostic parameters used in the direct method.
Name 3 diagnostic parameters used in the direct method.
→ PSV, renal-to-aorta ratio, resistive index
DIRECT METHOD
What is the principal ultrasound criterion for renal artery stenosis?
Why is a careful Doppler survey important?
What does aliasing commonly suggest in renal arteries?
What is the principal ultrasound criterion for renal artery stenosis?
→ Velocity flow jets/elevated PSV
Why is a careful Doppler survey important?
→ Identify maximum flow velocity
What does aliasing commonly suggest in renal arteries?
→ High velocity stenotic flow
DIRECT METHOD
What does RAR stand for?
What does the RAR help diagnose?
How is RAR calculated?
Why is the RAR useful? Compensates for what variability between patients
What is the normal RAR?
What does RAR stand for?
→ Renal-to-aortic ratio
What does the RAR help diagnose?
→ Renal vascular disease
How is RAR calculated?
→ Highest renal artery PSV ÷ aortic PSV
Why is the RAR useful?
→ Compensates for hemodynamic variability between patients
What is the normal RAR?
→ Less than 3.5
DIRECT METHOD
younger patients have what in where and can (say the velocity) without ______?
elderly patients with what disease or poor _____demonstrate?- even in regions of ?
When determining renal artery stenosis, should you rely on only one criterion?
(name 5)
What can younger patients have without stenosis?
→ Younger patients have higher normal PSV flow in the
aorta and branch vessels, can exceed 180 cm/sec without
stenosis
What can elderly patients with cardiac disease or poor output demonstrate?
→ Elderly patients (cardiac dz/poor output) demonstrate lower
PSV even in regions of stenosis
When determining renal artery stenosis, should you rely on only one criterion?
→ No, Use all of the criteria when determining a stenosis – PSV, RI, RAR, Post-stenotic turbulence, Tardus parvus
DIRECT METHOD
What does the RI evaluate?
What can it also be called?
Parameter not used for diagnosis what?
How is RI calculated?
what is the normal RI value?
What RI value is considered abnormal?
What does an elevated RI suggest?
What does the RI evaluate?
→ Resistance within renal parenchyma
What can it also be called?
→ Also called Pourcelot’s ratio
Parameter not used for diagnosis what?
→ Parameter not used for diagnosis of renal artery stenosis
How is RI calculated?
→ PSV − EDV ÷ PSV
what is the normal RI value?
→ Normal <0.75
What RI value is considered abnormal?
→ Greater than 0.75
What does an elevated RI suggest?
→ Increased renal parenchymal resistance/disease
An "elevated" value in parenchymal renal disease typically refers to blood markers like creatinine or blood urea nitrogen (BUN), or the presence of protein (albuminuria) in your urine. These indicate that the functional kidney tissue (parenchyma) is damaged and unable to properly filter waste from the blood.
Because "parenchymal renal disease" is a broad term encompassing conditions like chronic kidney disease (CKD), diabetic nephropathy, or glomerulonephritis, an elevated lab result points to specific functional issues:
DIRECT METHOD INTERPRETATION
Renal artery occlusion
what cannot be visualized well in renal artery?
whats the amplitude of the spectral Doppler within where?
whats the kidney size?
decribe the apparnce on US?
No flow detectable in well visualized renal artery
Low amplitude spectral Doppler within renal parenchyma
Small kidney size (<9cm) (b/c no flow is going to the Renal artery b/c its occluded)
Increase echogenicity in kidney(s)
DIRECT METHOD INTERPRETATION
Stenosis technique:
what regions should be mapped with spectral dopper?
record what velocity and what should the angle be?
what should you calculate ?
Stenosis criteria
Flow velocity elevation in stenotic portion of vessel
• Post stenotic turbulence
Evidence of ______distal to stenosis or within _______
arteries (________or ________)*
Stenosis technique
• All regions mapped with spectral Doppler
• Record PSV – < / = 60°
• Calculate RAR
Stenosis criteria
Evidence of damping distal to stenosis or within intrarenal
arteries (segmental or interlobar)
DIRECT METHOD INTERPRETATION GIVE ME THE VALUES
what is the criteria for stenosis % and the following are criteria for the stenosis
RAR
PSV
you will see what post to a stenosis
color _____
Damping of what arteries
AI
AT
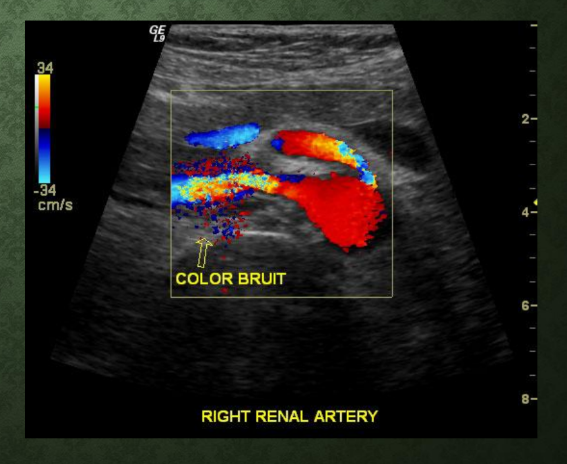
Criteria for > 50% - 60% stenosis
• RAR > 3.5
• PSV > 180-200 cm/s
• Post stenotic turbulence
• Color bruit
• Damping of intrarenal
arteries
• AI < 300 cm/sec
• AT > 0.07 sec
These numbers are looking for damping/tardus-parvus changes in the intrarenal arteries, which can suggest a proximal renal artery stenosis.
AI < 300 cm/sec
AI = Acceleration Index
It tells you how fast the waveform rises upward in systole.
Normal: sharp, quick systolic upstroke
Abnormal AI < 300: the upstroke is slower/weaker than expected
So AI < 300 means the blood is not accelerating quickly when it reaches the kidney, which can happen if there is a narrowing before it.
AT > 0.07 sec
AT = Acceleration Time
It tells you how long it takes the waveform to reach the systolic peak.
Normal AT: less than 0.07 sec
Abnormal AT > 0.07 sec: it takes too long to reach the peak
Your slides say normal intrarenal arteries have an acceleration time less than 0.07 seconds, and tardus parvus is a waveform that is slow to rise and fall with a long acceleration time.
Simple way to understand both
If the renal artery before the kidney is narrowed, blood has trouble getting through. By the time it reaches the small intrarenal arteries, the waveform looks delayed and dampened.
So:
AI < 300 = waveform rises too slowly
AT > 0.07 sec = waveform takes too long to peak
Together, they support damping of intrarenal arteries, which your slide lists as a criterion with renal artery stenosis findings
Color bruit means an area on color Doppler that looks noisy/multicolored because blood flow is very fast and disturbed.
A bruit normally means a “whooshing sound” from turbulent blood flow.
On ultrasound, a color bruit is like the visual version of that bruit.
Accessory renal arteries:
Extra arteries that also feed the kidney
This is where you measure things like PSV and calculate RAR to look for renal artery stenosis. Your slide says the direct method includes Doppler interrogation of the renal arteries/accessory renal arteries and renal veins.
Intrarenal arteries
These are the smaller arteries inside the kidney tissue. They include:
Segmental arteries → first branch of the main renal artery, course through the hilum
Interlobar arteries → run between the renal pyramids
Arcuate arteries → run along the border near the cortex/medulla
Interlobular arteries → extend into the cortex
Your slides list these as the intrarenal artery anatomy.
Easy difference
Direct method = main renal artery/accessory renal artery outside or entering the kidney.
Intrarenal/indirect evaluation = smaller arteries inside the kidney tissue used to assess RI, acceleration time, and tardus-parvus patterns.
^^^^^similar to the last slide CAN SKIP
DIRECT METHOD INTERPRETATION IDK WHAT I DID
What does the indirect renal duplex method evaluate?
Name 3 indirect Doppler parameters evaluated in renal duplex.
What waveform abnormality is associated with proximal stenosis in the indirect method?
What does the indirect renal duplex method evaluate?
→ Intrarenal arteries only
Name 3 indirect Doppler parameters evaluated in renal duplex.
→ Acceleration time, acceleration index, resistive index
What waveform abnormality is associated with proximal stenosis in the indirect method?
→ Tardus parvus waveform
INDIRECT METHOD
Interrogates what arteries name 2 ?
________ waveform characteristics evaluated for abnormality associated with what?
How long is this exam time with what success rate?
why^ most likely can ______be performed, especially when there is what visualization of the _____ arteries
Interrogates segmental and/or interlobar arteries
• Intrarenal waveform characteristics evaluated for abnormality
associated with main renal artery stenosis or occlusion
• Short exam time / high success rate
• Most likely can always be performed, especially when there is
limited visualization of the renal arteries
INDIRECT METHOD LIMITATIONS
Limited to detecting what stenosis?
Shape of intrarenal waveform affected by multiple factors list 3
^This means the waveform inside the kidney does not only depend on renal artery stenosis. Other things can change the waveform too, like:
what with arteries
resistance of what?
____phenomena meaning ?
This ^ may do what to the damping effects
Positive /Equivocal results – perform in what method?
Limited to detecting severe (>70%) stenosis
(This means the indirect method usually only becomes clearly abnormal when the renal artery narrowing is severe.
A mild or moderate stenosis may not change the intrarenal waveform enough to notice, Indirect method is better at catching severe stenosis, not mild stenosis.)
• Shape of intrarenal waveform affected by multiple factors
• Stiffness (compliance) of arteries
(If arteries are stiff, the waveform may look different even without stenosis.)
• Resistance of microcirculation
(If the tiny vessels inside the kidney have high resistance, that can affect diastolic flow and RI.)
• Inflow phenomena (renal artery stenosis)
problems affecting blood flow before it reaches the kidney tissue, such as proximal renal artery stenosis. This can make intrarenal waveforms delayed and dampened, causing a tardus-parvus pattern.
May obliterate damping effects
phrase means some factors can hide the dampened/tardus-parvus waveform, even if stenosis is present.
Example: if the kidney has high resistance or stiff vessels, the waveform may not show the classic delayed/dampened appearance clearly.
• Positive /Equivocal results – perform direct method
This means if the intrarenal waveform looks abnormal or unclear, you should go back and directly evaluate the main renal artery.
So:
Indirect method suggests a problem.
Direct method confirms by measuring the renal artery PSV/RAR.
INDIRECT METHOD
when is this inaccurate ?
Has improved accuracy:
Obtain waveforms at name 3
use a what degree angle ?
Not able to be what to the flow state?
only obtaining ______ and not ______
Use _______Doppler frequency
Set sweep speed for how many seconds
Reduce what for large waveform
Use what sample volume size?
Inaccurate when:
• AAA (Abdominal Aortic Aneurysm) superior to or at level of renal arteries
RAR is inaccurate when an AAA is superior to or at the level of the renal arteries because the aortic PSV may be abnormal. Since RAR uses aortic PSV as the denominator, an abnormal aortic velocity can make the ratio unreliable.
Improved accuracy:
• Obtain waveforms at upper, mid, and lower poles
• Use a 0 degree angle
• Not able to be parallel to flow state
• Only obtaining ratios and not velocities
• Use highest Doppler frequency
• Set sweep speed for 2 to 3 seconds
• Reduce PRF for large waveform
• Use 5 to 7 mm (large size) sample volume
INDIRECT METHOD TECHNIQUE
name 3 doppler techniques
Color Doppler,
Minimize depth, &
Doppler waveforms
INDIRECT METHOD TECHNIQUE
Color Doppler used to locate what name 2 arteries ?
• Minimize depth you are ______ on the image
Doppler waveforms tell me where name 3
what should not be the sole determinant for disease
Color Doppler
• Locate segmental / interlobar arteries
• Minimize depth
• Zoom image
• Doppler waveforms
• Superior, mid and inferior poles
• Resistive index should not be the sole determinant for disease
INDIRECT METHOD, Diagnostic Parameters name 3
RI
• End diastolic ratio (EDR)
• Acceleration time (AT)
INDIRECT METHOD INTERPRETATION
Normal intrarenal arteries
what waveform?
Whats the RI
what systolic peak is present?
AT is what value ?
Low resistance
• RI is less than 0.75
• Early systolic peak (ESP) is present
• Acceleration time (less than 0.07seconds)
Indirect Method — EDR
What is EDR in the indirect method for renal duplex? - whats the Formula?
What does EDR determine?
How should EDR values be assessed?
What is a normal EDR?
: What is an abnormal EDR? and what does it indicate?
EDR = End Diastolic Ratio. It compares EDV to PSV in the intrarenal arteries.
Formula:
EDR = EDV / PSV
It determines if flow resistance has increased within the kidney parenchyma.
Compare the values side to side between the right and left kidneys.
Normal >0.2
Abnormal EDR < 0.2
It indicates increased resistance in the renal parenchyma, meaning there is less diastolic flow compared to systolic flow. Your slide states that EDR less than 0.2 indicates increased resistance in the parenchyma.
Simple memory:
Low EDR = low diastolic flow = higher resistance inside the kidney.
INDIRECT METHOD
INTERPRETATION
• Acceleration time (AT)
• Time interval from the onset of ______to the _______peak _____ velocity
• Calipers must be placed at the base of the systolic _____and
at peak ______
• Normal =
INDIRECT METHOD
INTERPRETATION
• Acceleration time (AT)
• Time interval from the onset of systole to the initial peak systolic
velocity
• Calipers must be placed at the base of the systolic upstroke and
at peak systole
• Normal – <0.07
INDIRECT METHOD INTERPRETATION
Abnormal - what % stenosis of what artery
• Reduced what in kidney _______(which side)
• Loss of ______– ______systolic upslope
• describe the waveform
• whats the AT
what is the waveform called
name 3 things that decribe the waveform?
whats the amplitude
whats the rise time
what shape is taken place of the waveform
Abnormal - >60% stenosis MRA
• Reduced color flow in kidney unilaterally
• Loss of ESP (early systolic peak) – flattened systolic upslope
• Dampened waveform
• Prolonged AT - >0.07
• Tardus parvus waveform
• Low amplitude, prolonged
rise time, rounding of
waveform
RENAL VEIN THROMBOSIS
Typical appearance of venous thrombosis
acute vs chronic 2 for each
Acute – dilated vein, hypoechoic
• Chronic – collapsed vein, echogenic
RENAL VEIN THROMBOSIS, what happens if it is extend into the IVC?
Tumor thrombosis
RENAL VEIN THROMBOSIS, Waveforms
what waveform, occus because the thrombus changes the what?
what is happening to the flow out of the kidney?
what arteries does it affect name 2
High resistive – occurs because the thrombus changes the resistance
• Obstructing / Restricting flow out of kidney
• MRA or intra parenchymal arteries