Y1 Dev
1/89
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
90 Terms
importance of dev psychology
children aren’t just smaller versions of adults (their knowledge/abilities are qualitatively different from adults)
psychological explanations need to be developmentally plausible
we need evidence supporting the best strategies for education and social support
competence
true underlying ability/knowledge
performance
what we demonstrate
always limited by other factors, so can never get pure measures of competence (eg. cognition, social/cultural context)
Piaget
most influential developmental psychologist
argued that children lack certain competencies at particular ages
conservation - can’t understand that water poured from small glass into big glass will be the same amount, even when it looks different
criticism - kids might expect something to have changed if an adult does something, then asks what has changed
Vygotsky
developed the sociocultural approach to understand how social and cultural influences affect children’s development
the unity of child and context
human evolution
we are born long before brain development is complete, so need intensive, proximal care during early childhood
we have a long childhood period (12 years, then puberty)
continuing brain development even at 25 years
several cultures do ‘cooperative breeding’ of a child by many adults
as brain/body proportion increases, so does the time taken until sexual maturity
biological parents and other family members have cared for a growing infant
institutionalisation of non-parental care in nurseries and schools created a need for the infant to bond with adults who are in a position to care for them
need for attachment to primary carer
motivation to be ‘likeable’ to all potential carers
attachment
the bond that an infant forms with their primary caregiver, characterised by proximity and feelings of being comforted and content
Bowlby’s attachment theory
revolutionary
influenced by empirical findings that there is an evolutionarily urge to bond with a caregiver (not simply because the infants need feeding)
contrasts to the psychoanalytic views of the time, that based mother-child relationship on mothers fulfilling the child’s primary needs
but follows Freud’s idea that early childhood experiences determine future
has 5 phases of attachment development
lifelong significance of attachment
initial attachment creates an internal working model - a cognitive prototype influencing a person’s perception of our reactions to other relationships)
the views on attachment stability follows from Freud’s psychoanalytic ideas on how early childhood experiences determine their future
5 phases of attachment development (Bowlby)
first few months - orienting towards people indiscriminately
5-7 months - orienting and preferentially engaging with the caregiver
7-9 months - crawling to the caregiver and expressing distress when separated from them (onset of attachment)
2-3 years - goal-corrected partnership where the child also accommodates the caregiver’s needs (waits for their return)
4+ years - switch from physical proximity to more abstract emotional closeness
internal working model
a cognitive prototype influencing a person’s perception of other relationships, and our reactions to them
lifelong significance of secure attachment at infancy
associated with:
more curiosity and problem solving at 2, social confidence at 3 and empathy at 5 (Oppenheim et al)
fewer internalising and externalising behaviours at 3 (McCartney et al)
social competence (Groh et al)
Ainsworth’s attachment styles - strange situation
longitudinal observations of mother-infant interactions
children presented with a separation scenario and asked how they would feel in that situation
high validity and reliability
avoidant, secure or anxious
type D (disorganised) has no obvious behaviour pattern
type A attachment
dismissive/avoidant
when separated, infant is not distressed
at reunion, infant ignores adult, turns away and averts gaze
type B attachment
secure
when separated, infant may be distressed but recovers fairly quickly
actively seeks proximity at reunion, interacts with adult
type C attachment
anxious/ambivalent
when separated, infant may be distressed/oblivious to being alone
at reunion, seeks proximity, but then resists interaction
universality hypothesis
when given an opportunity, most infants become attached to at least 1 specific caregiver
true in all examined cultures
normativity hypothesis
most infants are securely attachment in contexts that are not inherently threatening to health and survival
true in most cultures
sensitivity hypothesis
attachment security depends on sensitive and prompt responses to the infants signals
varied among cultures
competence hypothesis
secure attachment leads to positive child outcomes
varied among cultures
more powerful when it goes beyond mother-infant attachment
origins of attachment
parental factors
child factors
cultural factors
origins of attachment - parental factors
meta-analysis of 66 studies
self-evident behaviour groups based on Ainsworth’s original scale
sensitivity - mother’s ability to perceive infant’s signals, and response promptly and appropriately
contiguity - frequency of mother’s responding to infant’s signals (reciprocity)
physical contact
cooperation - whether mother intrudes/interferes with infant
other behaviour groups defined by experts
synchrony
mutuality (sharing of a feeling/relationship)
these 2 are as important as sensitivity
emotional support (words, hugging)
positive attitude
stimulation
supports the orthodox view that maternal sensitivity is key for a secure attachment
effect size not as high as original Ainsworth study
origins of attachment - child factors
attachment style was assessed using SS procedure in toddlers with autism, development disorders and mental retardation, against a non-clinical comparison group:
those with development disorders are less likely to have a secure attachment, than the comparison group
suggests there are child-related factors that affect attachment styles
not just emphasis on the parent’s behaviour
origins of attachment - cultural factors
western middle-class assumption of a healthy maturity is individual autonomy
differences in socialisation goals in different cultures eg. society’s approach to strangers and stranger anxiety
wide variety in caregiving arrangements across cultures
cross-cultural evidence in scarce
maternal responsivity …
to infant’s signals is a key indicator of secure attachment
the optimally sensitive mother is able to see things from her baby’s PoV
she is alert to perceive baby’s signals, interprets them accurately and responds appropriately and promptly
nature
innate factors
genes - hereditary material, that is unchanging over life
nuture
the environment
life experiences
social interactions
parenting styles
anything not genetic
includes stress hormones, vitamins, things from outside world eg, smoke and pesticides
development
interactions of genes and environment (not nature vs nurture)
these change over development,
some genes interact with other genes and multiple environmental factors
romanian orphans
in the early 1990s, almost all children had severe learning disabilities at the time of their adoption
most of them ended up with typical learning ability once grown, but with a higher incidence of psychological illness
an environment-environment interaction
PKU - phenylketonuria
rare, inherited condition
learning disability caused by diet - reduced ability to metabolise an amino acid
treated by avoiding foods that are sources of phenylalanine
with a strict diet, there are no symptoms of PKU
genetically-defined (nature), but can be fully treated by diet (nurture)
dyslexia
word reading significantly below expected, given a child’s age, intelligence and education
3-6% prevalence
has a biological basis
manifests itself differently across language:
transparent languages
where word-sound correspondences are invariant, fluency is affected
speed of reading eg. Italian
opaque languages
many word-sound mappings, accuracy and fluency are affected
eg. English
impact of dyslexia varies depending on the language
has a genetic basis, but manifests differently across language (nature and nurture)
genetic predispositions
where an individual may not be born with something, but may be at high risk of acquiring it (WHO)
autism, ADHD, depression, bipolar and SZ have common genetic predispositions
certain genes are associated with increased risk of some disorders
probabilistic causes
causes are only probabilistically related to effects
eg. smoking and lung cancer
cases of lung cancer without smoking, or smokers living to old age, do not undermine the confidence in the causal relation
the idea that psychological disorders are caused by a accumulation of risk factors, each of small effect
like physical diseases
environmental modifiers (triggers)
determine whether people with a genetic predisposition to a disease/disorder, actually end up with it
eg. someone may have a predisposition to being very tall, but only end up tall with the environmental modifier of a balanced diet
eg. someone with a predisposition to lung cancer might end up with it, if they smoke
positive modifiers
positively change the effect of a gene
eg. vitamins protecting against a genetic predisposition to cancer
psychology-based interventions can improve behavioural, cognitive and academic outcomes
psychology can be used to change the course of development
all education is an intervention
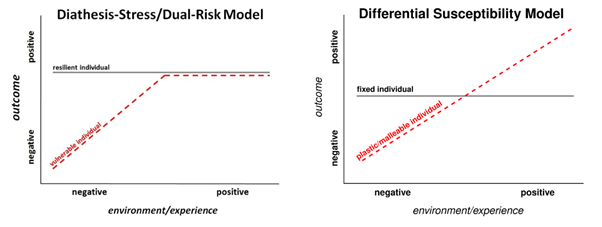
differential susceptibility
individuals vary in their sensitivity to environmental influences, both positive and negative
Belsky - some people are more ‘plastic’/susceptible, and affected by their environment
orchid vs dandelion analogy
orchids - highly sensitive, flourish in supportive environments, but struggle in adverse ones
dandelions - less sensitive, capable of adapting to a wider range of environments
Pluess and Belsky - does children’s temperament moderate their response to different childcare environments?
large longitudinal sample involving children exposed to different types of childcare settings
measures:
child’s temperament assessed early in development to identify negative emotionality
childcare quality was evaluated based on responsiveness of caregivers, richness of learning environment and caregiver-child ratio
child behaviour outcomes assessed in later childhood
low-quality childcare - difficult children displayed more behaviour problems compared to those with low negative emotionality
high-quality childcare - difficult children showed fewer behaviour problems, compared to those with low negative emotionality
interpretations:
environmental sensitivity - responsiveness
same heightened physiological reactivity may cause them to struggle in adverse environments
makes them particularly receptive to the benefits of nurturing and enriched environments
higher levels of arousal - self-direction
seeks out more interactions with caregivers
results in richer developmental experiences that ultimately foster more social learning
male gender differences in different susceptibilities
show a broader variability in outcomes, influenced more significantly by environmental conditions
more likely to be affected by negative influences, but also to benefit more profoundly from positive conditions
higher rates of behavioural and emotional problems under adversity
boys exposed to harsh parenting/high levels of family stress exhibit more externalising problems (eg. aggression and conduct issues, compared to girls)
explanations:
slower maturation of prefrontal cortex, involved in emotional regulation
higher cortisol responses during stress-inducing tasks indicates their hypothalamic pituitary adrenal axis (HPA) is more sensitive in social stress contexts
more pronounced gains in supportive environments
boys with high physiological reactivity are more sensitive to positive environments (measured through indicators like cortisol responses)
in supportive settings - tend to show significant improvements in socioemotional development, self-regulation and social competence
in nurturing, structured and positive environments, this sensitivity translates into better developmental outcomes
female gender differences in different susceptibilities
tend to show greater resilience and less extreme variability in outcomes
more consistent responses to environments, often less reactive to both negative and positive extremes - compared to males
social learning
learning through cues provided by other social agents
enables cumulative culture - changes are incorporated into the repertoire and transferred across generations
advanced social learning creates social transmission of information = traditions and cultures
especially important for learning about social conventions, which vary across time and cultures
babies learn passively, and through being taught by others
their social learning is influenced by cognitive-motor development and social-cultural context
critical for learning about physical (instrumental) and social (conventional) aspects of the world
learning can be about:
properties of individual things
relations between things, and actions (cause and effect)
social conventions
psychological theories of social learning
from Piaget, Vygotsky and Bandura
Piaget’s theory of social learning
children’s behavioural and mental capacities expand as their cognitive skills develop with age
child is an individual scientist exploring the world
cognitive skills are individual characteristics
infants use others as a source of information
predicts infants can’t learn from others until 18-24 months (when imitation begins - key mechanism of social learning)
children can’t put themselves in other people’s shoes until pre-operational stage
egocentrism first (2-7 years)
learnt behaviours can’t be easily transferred to other domains until formal operations stage (11+ years)
stages of Piaget’s theory
1 - sensorimotor (0-2 years)
coordination of senses with motor response
sensory curiosity about the world
language used for demands and cataloguing
object permanence developed (understanding that objects exist even when not being perceived)
egocentrism
2 - preoperational (2-7 years)
symbolic thinking
use of proper syntax and grammar to express full concepts
imagination and intuition are strong, but complex abstract thought is still difficult
conservation developed
3 - concrete operational (7-11 years)
concepts attached to concrete situations
time, space and quantity are understand and applied, but not as independent concepts
4 - formal operations (11+ years)
theoretical, hypothetical and counterfactual thinking
abstract logic and reasoning
strategy and planning possible
concepts learned in one context can be applied to another
conservation
developed in preoperational stage
the ability to understand that properties of an object (quantity, volume etc) remain the same, even when appearance changes
Vygotsky’s theory of social learning
children’s behavioural and mental capacities develop through social interaction, giving them the ‘tools’ of learning and thinking
set of activities the child can currently do = things they can do with aid (zone of proximal development) + things they can’t do
every skill we require is a cooperation of social interaction
social learning is the primary form of knowledge production
language is an important tool for developing mental capacities
a piece of knowledge, behavioural pattern or an idea is first constructed within a social interaction, then is internalised by the individual
Bandura’s theory of social learning
emphasis on WHO children learn from
identification processes on basis of:
adopting behaviours
symbolic representations
similar meaning systems
claims gender related behaviours are socially learnt
parents, teachers and peers reinforce sex-appropriate behaviour = child’s behaviour < - > child observes and imitates others, usually of same sex
Bobo doll experiment
children imitated aggressive behaviour (especially boys)
later empirical studies partially supported his theory
children are influenced by what they observe and imitate
however, they also act in line with their social identity and gender schemas
mechanisms of social learning
learning through observation, and imitation
learning through observation
happens while being actively taught, or passively while watching
relies on associative learning mechanisms
X and Y tend to co-occur
evolutionary ancient mechanism
useful in early development before children develop the motor skills necessary to execute the actions themselves
can be examined using methods of habituation, looking time, and predictive gaze (how well infants can predict what will happen)
in experiments, need to make sure the target behaviour is something the child can’t do yet, otherwise can’t know if learning is through observation or trial and error
learning to feed through social observation study
54 6 month olds, 54 10 month olds, 32 adults
infants predictive eye gaze tracked as they watch videos of an adult
prediction = fixation at the area of interest before the action occurs
experiment 1 - feeding action (manual vs self-propelled)
infants watched videos of an adult feeding herself, either by moving the spoon with hand, or with the spoon ‘flying’ into her mouth
experiment 2 - combing action (unfamiliar compared to feeding)
infants watched videos of an adult either feeding herself or combing her hair
results:
6 and 10 month olds predicted the outcome of a manual feeding action
only 10 month olds predicted the outcome of a self-propelled feeding action
neither predicted the outcome of combining action
the more infants observe an action, the better they learn its outcome
learning through imitation
first observing another person, then copying their actions
relies on the ability to perceive others actions, and map them onto one’s own body
emulation - copying the end goal of an action, without necessarily doing it the exact way as the model
can be assessed by looking at how much children copy the style vs the end goal of an action
would expect more faithful imitation when learning about social conventions (not emulation)
over-imitation - copying seemingly unnecessary/irrational actions of another person
can help faithful transmission of information across generations
can signal one’s group membership
rational imitation in preverbal infants
27 14 month olds
infants first watched an adult switch on a lightbox by touching the lamp with her head, then given the lightbox to turn on themselves
results:
when adult was free to move her hands, infants used their head (imitated)
when adult wasn’t free to move her hands, infants used their hands (emulated)
infants understand others action goals, at as young as 14 months
infants imitation takes action rationality into account
may not be mature enough to learn social conventions yet
imitation for learning instruments vs conventions
57 6-8 year olds from Vanuatu, 85 from USA
children watched an adult make a necklace, then made on themselves
2 conditions:
instrumental - i am going to make a necklace (individual preference)
conventional - everyone makes a necklace like this (social pressure/norm)
used seemingly unnecessary actions in both conditions
results:
children imitated more faithfully in conventional than instrumental
those from Vanuatu imitated more than US children in instrumental
US children only faithfully imitated when learning about conventional actions, not instrumental preferences
for conventional learning, both countries imitated faithfully
cultures values (autonomy in US vs conformity in Vanuatu) guide children’s imitations
DSM-V for autism
part 1
social and communication characteristics are considered as one clinical aspect
autism spectrum disorder - clinically significant persistent deficits in social communication and interactions, as manifest by deficits in all of the following:
social-emotional reciprocity
non-verbal communication
developing, maintaining and understanding relationships
part 2
restricted, repetitive patterns of behaviour, interests and activities as manifested by at least 2 of the following:
stereotyped motor/verbal behaviours, unusual sensory behaviours
excessive adherence to routines and ritualised patterns of behaviour
restricted, fixed interests
abnormal responses to sensory stimuli
symptoms must be presented in early childhood, but may not become fully manifested until social demands exceed limited capacities
definition - deficits in social functioning and communication, and in repetitive behaviours/restricted interests
how many people are autistic
1-2% in England - 2023
a 787% exponential increase in prevalence of autism diagnosis between 1998 and 2018 in the UK
incidence - true rate
prevalence - recorded rate
incidence is constant, but prevalence increases
better/more available diagnosis? change in diagnosis? broader diagnostic criteria?
60-70% of UK autistic people may have a learning disability
29% of people with learning disabilities are autistic
disability - physical/mental impairment that has substantial and long-term negative effects in the ability to do normal daily activities
disorder - a group of systems involving abnormal behaviours or physiological conditions, persistent/intense distress, or a disruption of physiological functioning
no meaningful, obvious distinction here
downsides to autism
some feel alienated and misunderstood, can feel frustrated by the barrier that their condition puts between themselves and neurotypicals
bullying of ASD children is very common, because bullies single out those who are different
upset when routines are broken or expectations are not met
medical model – things are going wrong because the autistic person is behaving/feeling differently
social model – things are going wrong because the people around the autistic person are behaving in a way that is not well-matched to the needs of them
improving communication in autism
the Lancet published an encouraging study of 152 children with ASD aged 2 -4 years
2x a month for 6 months, parents watched videos of their interactions with their children
a therapist paused the video periodically to discuss methods that parents could use to better engage their children and bolster their communication skills
6 years later, 46% were considered to have severe autism in the intervention group, it was 63% in a control group
there is a scope for improving social and language functioning in a world full of neurotypicals
peer-mediated programs for autism - Watkins et al
reviewed various peer-mediated interventions in fostering social interactions between autistic and non-autistic students in inclusive settings
key findings:
improved social skills – non-autistic peers who received training demonstrated improved communication and social engagement with autistic classmates
increased social inclusion – autistic students reported reduced isolation and a greater sense of belonging in classrooms where peer interventions were implemented
long-term impact – positive social interactions continued beyond the intervention period, with changes in peer dynamics sustained over time
limited research on academic outcomes
while social benefits were clear, the study did not extensively measure the impact of peer training on academic performance
leaving a gap in understanding the full scope of the interventions impact
there is the need for ongoing support
peer-sensitivity training for autism - Roberts & Simpson
reviewed peer awareness interventions and their effectiveness in increasing understanding and acceptance of autistic students in schools
findings:
positive impact on social inclusion – programs that involved interactive learning showed greater success in fostering positive peer relationships and improving social inclusion of autistic students
eg. role playing, empathy building and direct discussions about autism
reduced stigma – increased the likelihood of autistic students being included in group activities and social interactions
varied program effectiveness – ongoing programs have a greater long term impact
neurodiversity perspective of autism
increasing recognition of autism as a difference, rather than a disorder
promoting a social model of disability (but this can gloss over serious difficulties that are not obviously social in nature)
AuDHD
autism and ADHD
85% of people with autism exhibit ADHD symptoms
co-occurrence requires careful assessment and tailored interventions
ADHD
attention deficit/hyperactivity disorder
defined by combination of symptoms of inattention and hyperactivity/impulsivity
3 types:
predominantly inattentive
hyperactivity/impulsivity
combined
subtypes of ADHD
ADHD with hyperactivity is ADD, separate from ADHD
has different neuropsychological profiles:
ADD - working memory and processing speed
ADHD - inhibitory control
different neurobiological basis (dopamine vs norepinephrine)
different patterns of comorbidity and social impairment
Kaplan et al - are different diagnoses distinct
sample of 179 children, recruited from clinics and special schools
all had dyslexia and/or ADHD
comprehensive assessment for ADHD, dyslexia, DCD
comorbidity is the norm, not the exception
only 20% have just ADHD
Dyck et al - do measures discriminate
608 children aged 3-14 years
449 typically developing
30 autism
53 ADHD
30 specific language impairment
assessments of IQ, language, motor, attention, cognition, executive function
lots of overlap in results
same profile of person but with different diagnoses eg. ADHD and SLI overlap
disorders do not dissociate using these statistical methods
SLI - specific language impairment
language does not follow typical development course
not due to hearing loss, physical abnormality or acquired brain damage
normal development in other areas
problems with language structure (phonology and syntax)
common particular problem with non-word repetition
autism and SLI
prediction of independence - children with ASD and SLI together should be very rare
ASD prevalence - 1%
SLI prevalence - 7%
predicts comorbidity 7 per 10,000
many children with ASD have language problems similar to SLI
poor nonword repetition and use of verb inflections (76% ASD with SLI)
impaired performance on a language battery (57% ASD with SLI)
they can be dissociated, yet they co-occur far more often than by chance
conventional idea of independent disorders seems wrong
there are risk factors, not a single cause, as this is too simple to account for the clinical reality (nature vs nurture)
different diagnoses
norm is meeting criteria for multiple diagnoses, not the exception
with a single diagnosis, likely to be some needs not formally recognised
different diagnoses do not neatly group according to their scores on tests, but overlap considerably
those with different diagnoses may score the same on a range of tests (same pattern of difficulties), but receive very6 different educational interventions, based on their diagnostic category
it’s objectively possible to distinguish people with learning difficulties from those without
masking/camouflaging
involves hiding/modifying one’s natural behaviour to conform to social norms/reduce stigma
people mask to fit into social environments, avoid negative judgements or manage expectations
can hinder accurate diagnosis and lead to underdiagnosis/misdiagnosis
especially in girls and all adults with ADHD who may present atypically
common behaviours
suppressing impulsive actions
imitating neurotypical peers
actively monitoring body language and speech patterns to appear more socially acceptable
gender differences
studies indicate that females with ADHD are more likely to mask due to higher societal expectations for social conformity
prevalence
up to 60% of adults with ADHD report frequent camouflaging behaviours
may explain high rates of late ADHD diagnoses in adults
can lead to diagnostic overshadowing, mental health issues, burnout, imposter syndrome and social/identity impacts
diagnostic overshadowing
can occur from masking
where an individual’s symptoms are minimised/misinterpreted as other conditions
eg. anxiety is under/misdiagnosed
Kooij et al
adults who mask ADHD symptoms experience a delay in diagnosis of 10+ years, compared do those who don’t
females with ADHD are more often diagnosed with anxiety or depression due to masking
50% more likelihood of a delayed ADHD diagnosis, compared to males
mental health consequences of masking
increased anxiety and depression
those masking have a 1.5x higher risk of developing these, compared to those who don’t
self-criticism and low self-esteem
correlated with long term masking
chronic stress
reported from 70% of ADHD masking adults, compared to 45% of non-maskers
there is a mental health toll of sustained masking behaviour
ADHD burnout
ADHD women who mask regularly are vulnerable to emotional and cognitive fatigue
imposter syndrome
adults who mask experience imposter-like feelings
as if they are ‘faking’ their way through social and professional settings
can exacerbate mental health issues
adults with autism and mask report feeling more disconnected from their own identity - feeling like they are ‘living a lie’
social and identity impacts from masking
report of a higher avoidance of social situations, leading to isolation and loneliness
identity confusion, struggles of separating authentic self from the masked behaviours
prolonged struggles contribute to a cycle of mental health challenges
masking intensifies isolation and internal conflict, leading to further issues - developmental cascade
implications of masking awareness
clinicians ask targeted questions about coping strategies and social interactions, to uncover potential masking
improved diagnostic tools
utilising more holistic assessments, that consider gender differences and masking behaviours, may improve diagnostic accuracy
awareness of masking in teacher training
helps educators identify neurodivergent traits in pupils who might otherwise go unnoticed
theory of mind (ToM)
attributing mental states to self and others (beliefs, desires, knowledge, emotions, perceptions, sensations)
our guesses/theories about other people’s minds, what they’re thinking and believing
essential for social interactions, and predicting/understanding behaviour
the foundation of empathy, communication, deception and morality
involves false and true beliefs
false - inaccurate, don’t reflect reality
true - accurate, current representation of reality
children develop true belief before false
initial studies showed it develops after 4 years, but this view is changing
acts as a mediator of reality
tells us what’s real/not real
deals with thoughts as if they are real
orders
what do you think
what do you think i think
what do you think that i think you think
history of ToM
research with chimpanzees in 1978 (Premack & Woodruff)
they consistently chose the photo that showed the correct solution to a problem presented to them
concluded they can read other people’s minds
criticisms
social learning through observations - are the chimps just drawing associations between actions they see occur frequently together, rather than attributing mental states to others
don’t necessarily understand false beliefs
they can understand others’ goals and intentions, but can’t represent others having false beliefs
chimpanzees = goal psychology (perception)
adults = desire psychology (belief)
children are in between these
methods for assessing ToM
different methods based on age and executive function requirements eg. memory and meta-thinking
explicit methods (infants express thoughts using language)
false-belief tasks
smarties task
sally-anne task
implicit methods (researchers infer infants’ understanding from their behaviour eg. eye-tracking)
violation of expectation
anticipatory looking
false-belief tasks
explicit method of assessing ToM
includes smarties and sally-anne task
based on idea that as ToM abilities advance, children appreciate that own thoughts/beliefs may differ from other peoples’, and they may hold beliefs that do not reflect reality
smarties task
measures ToM about others false beliefs, and their own previous false beliefs
researcher asks what they think is in the box
they reply smarties, as it’s a smarties box
they open it and see it’s pencils
researcher asks what one of their friends would guess what’s in the box
children younger than 4 will say pencils
they can’t appreciate the other person will have a false belief about the box
children older than 4 will say smarties
sally-anne task
assess true belief as a control condition
sally puts her marble in her basket, then leaves the room
anne takes it out the basket, and puts it into her box
sally comes back
where will she look for her marble?
anne has a true belief about the marble being, now, in the box
sally has a false belief about the marble being in the basket
children younger than 4 will say the box
children older than 4 will say the basket
can be adapted to implicit tasks, by replacing verbal responding with eye-gaze tracking, and measuring children’s behavioural response/interaction
violation of expectation
non-verbal (implicit) measure of ToM
used primarily with infants
example: shown video of sally’s end goal
sometimes she acts in accordance with infant’s belief (expected)
sometimes she acts oppositely (unexpected)
infants with ToM will form predictions about how an agent will act next
if the prediction doesn’t happen, will infant will react with surprise
suprise reaction is assessed using habituation and pupil dilation
looking longer at a stimulus/pupils dilating, means they find the stimulus surprising/unexpected, so can infer what their expectations were
infants without ToM will be oblivious to the event that should have violated their expectation
anticipatory looking
non-verbal (implicit) measure of ToM
used primarily with infants
infants with ToM form predictions about how an agent will act next, and divert their eye-gaze to where they predict the agent will go, before it happens
predictive eye-gaze can be measured using eye-tracking
development of ToM
early studies showed distinct shift in abilities at 4 years old
meta-analysis of 178 ToM development studies
regardless of how ToM questions are asked, those under 3 don’t respond correctly above chance
children of all ages showed improved performance with implicit tasks
no evidence for ToM development before 3
recent studies show capacities begin to emerge in younger ages, but not consistently
2 major changes/revolutions of ToM
9 months
basic ToM
perception-goal psychology
4 years
fully-fledged meta-representation ToM
belief-desire psychology
into adulthood
refinement of meta-representation (representing how other people represent the world)
recursive, higher order ToM
precursors of ToM
children need to have a fundamental understanding of:
self-other distinction
other people’s goals and intention (even when action goals are not met)
in order to formulate theories about other people’s minds
these 2 social-cognitive skills/precursors are in place by age 2, in at least rudimentary form
they continue developing throughout childhood
both undergo a revolution at 9 months, in line with 2 stage view of ToM development
precursors of ToM - understanding of self-other distinction
24 hour newborns – similarity between self and others
infants look longer at social agents synchronously stroked with them
3-5 months – self-initiated actions
infants look longer at live displays that are not contingent with their own leg motion
15-24 months – prosocial engagement
toddlers share resources, help and comfort others in need, indicating they can identify other people’s thoughts/beliefs
precursors of ToM - understanding of others goals and intentions
6 months – goal understanding
infants predict the outcome of others’ actions if these actions are familiar to them eg. feeding
9 months – intention understanding, even when action goals are not met
infants patiently wait if an adult is unwilling to give them a toy vs when the adult is trying but unable to do so
interventions
any treatment undertaken to halt, manage or alter the course of the pathological process of a disease/disorder
action from psychotherapist to deal with the client’s issues
usually takes place when a child is experiencing difficulties
aim is to arise a change in feelings, beliefs, thoughts and behaviour
based on thorough assessment and formulation, not just diagnosis
has potential to do harm however
goals of interventions - medical model
most common
the ‘disorder’ is within the individual
identifies cluster of symptoms and biomedical origin of the client’s condition
focuses on reducing symptoms and improving ‘normalcy’
medical view for autism:
autism is a disorder
social-communicative deficits are within the individual
goals of intervention - social model
society is the heart of the problems and challenges faced
identifies social and environmental contribution to the client’s difficulties
focuses on quality of life, skills, goals and accommodation
social view for autism:
autistic people have differences
society is to blame for the social-communicative deficits
efficacy of interventions