USMLE Step 1 HY Images to Know
1/479
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
480 Terms
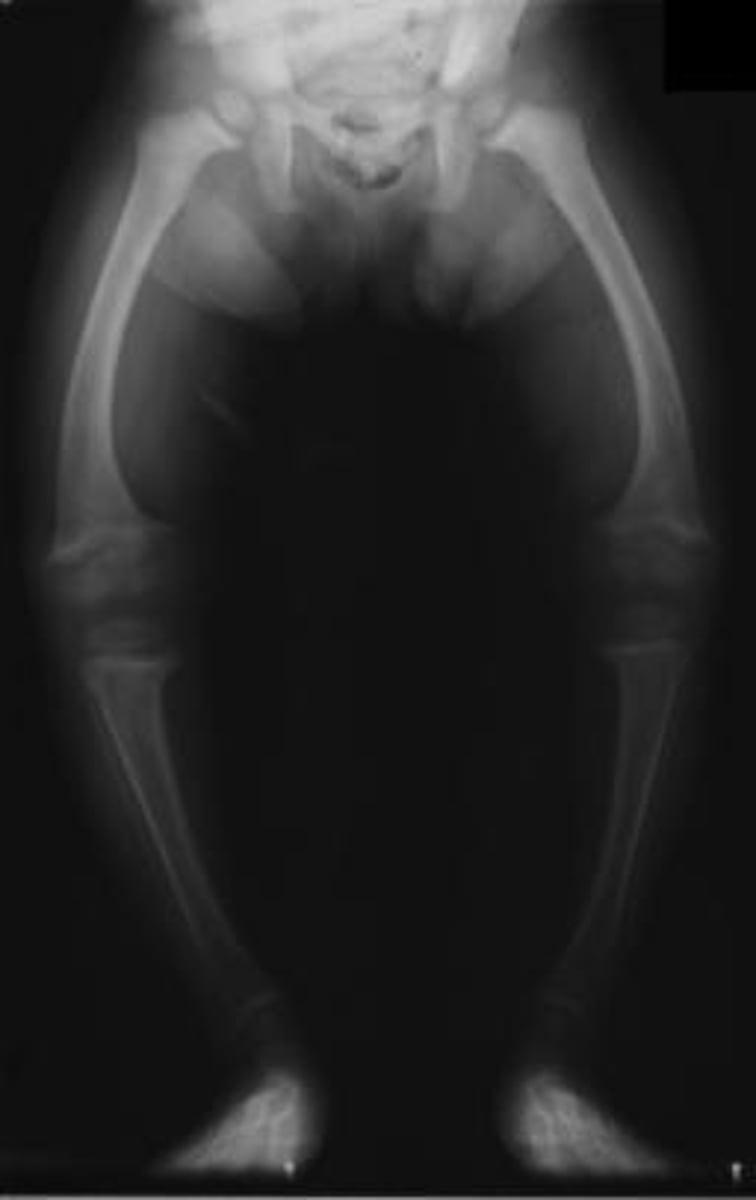
RICKETS d/t vit D def
-notice femurs bowed out (genu varum)
x-ray of legs of toddler
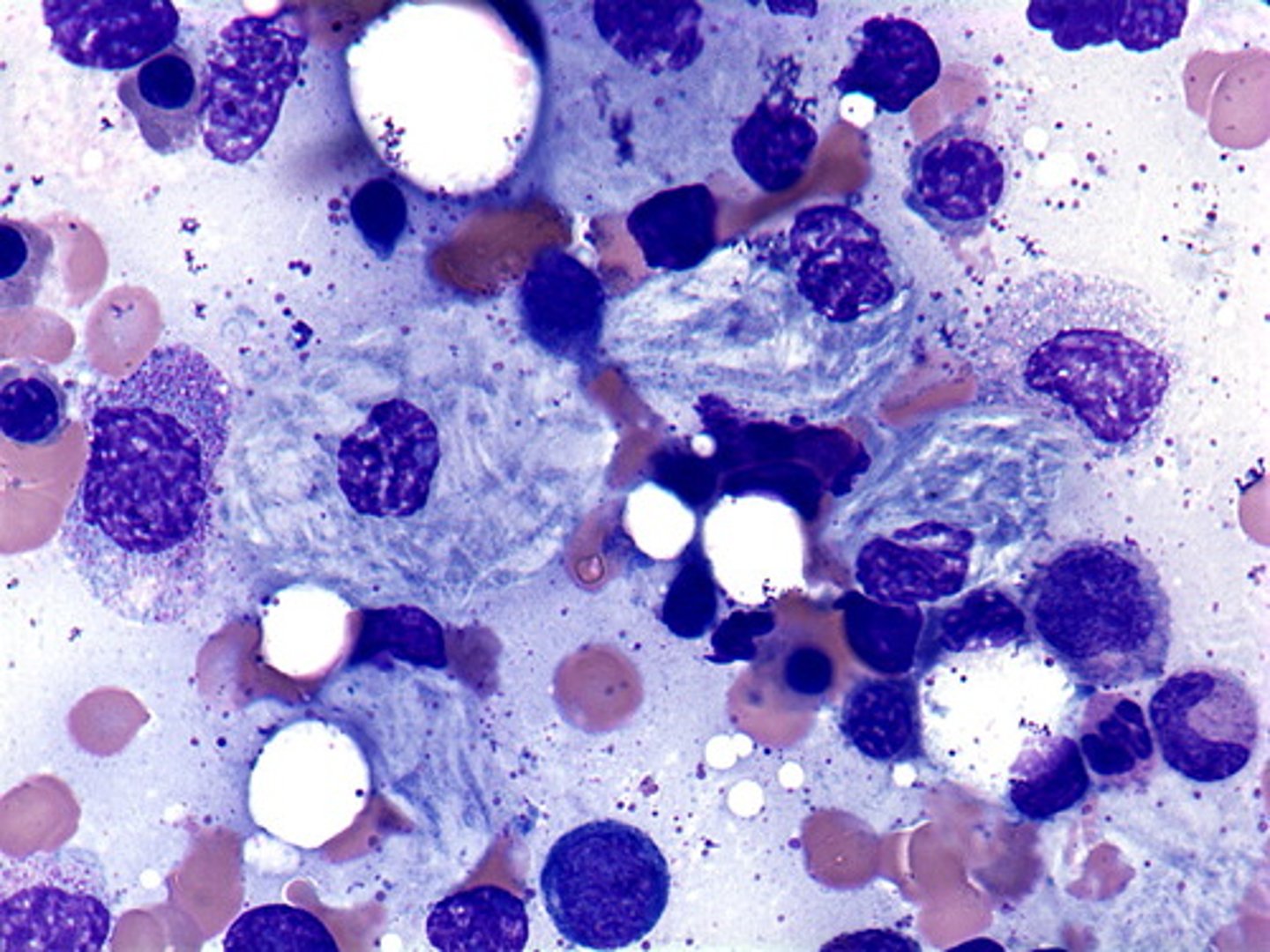
Gaucher's cells in Gaucher's Dz (lysosomal storage Dz); macrophage looks like crumpled tissue paper
histo of macrophage
foam cells (stored w/ fat) in niemann pick Dz
histo of macrophage 2
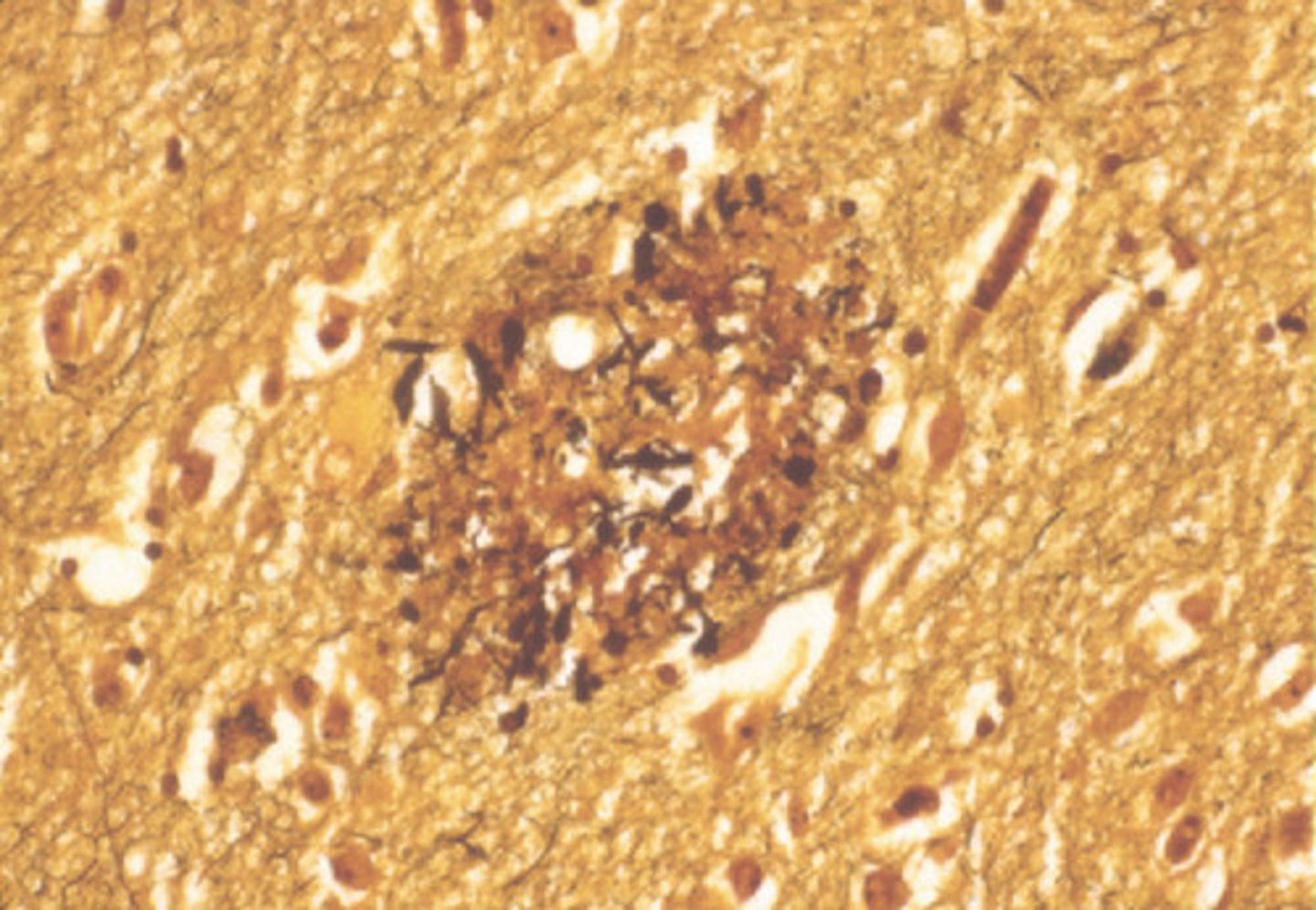
senile plaque in Alzheimer's Dz
β-amyloid protein
MS
-areas of oligodendrocyte loss + reactive gliosis
paraventricular plaques
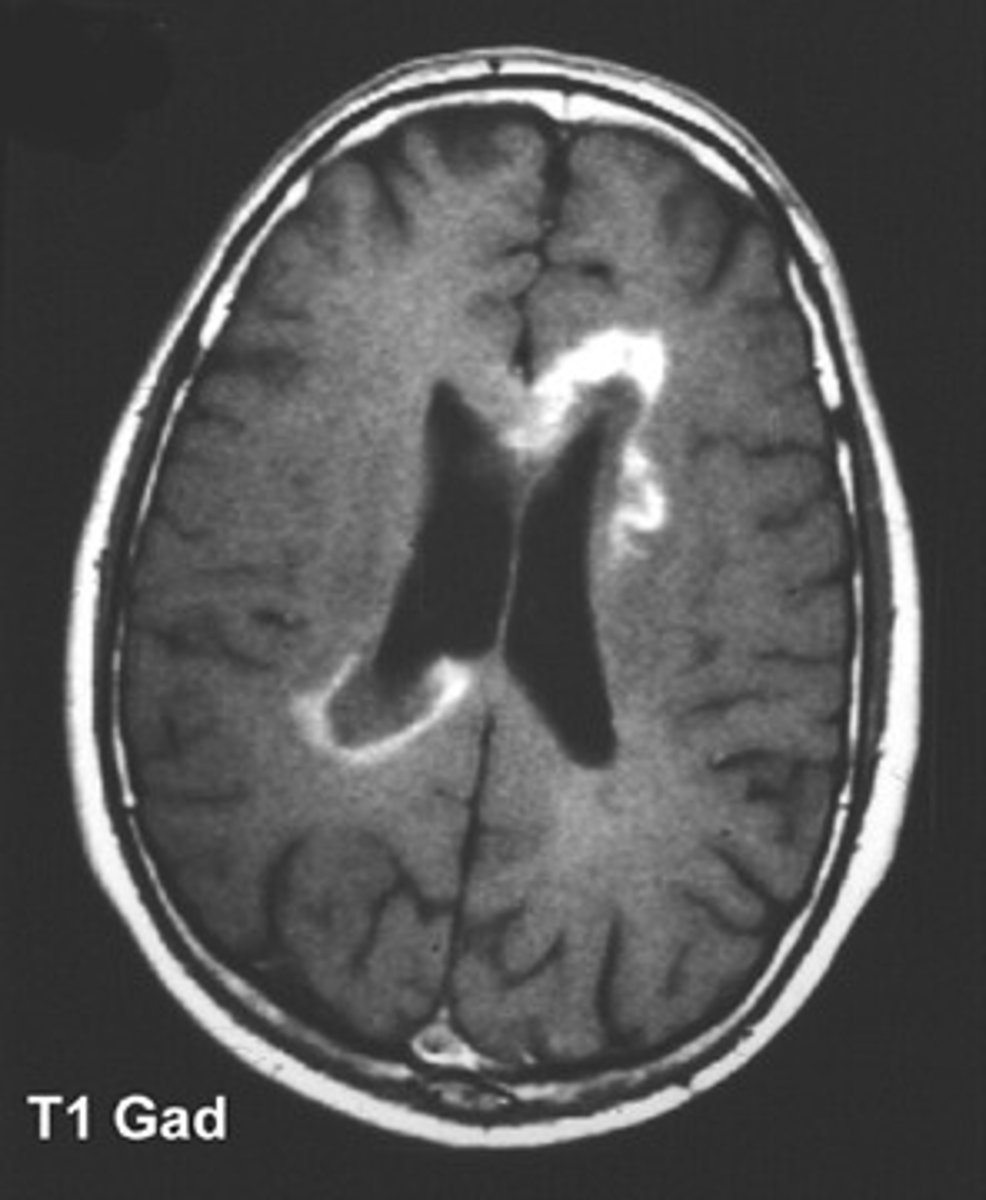
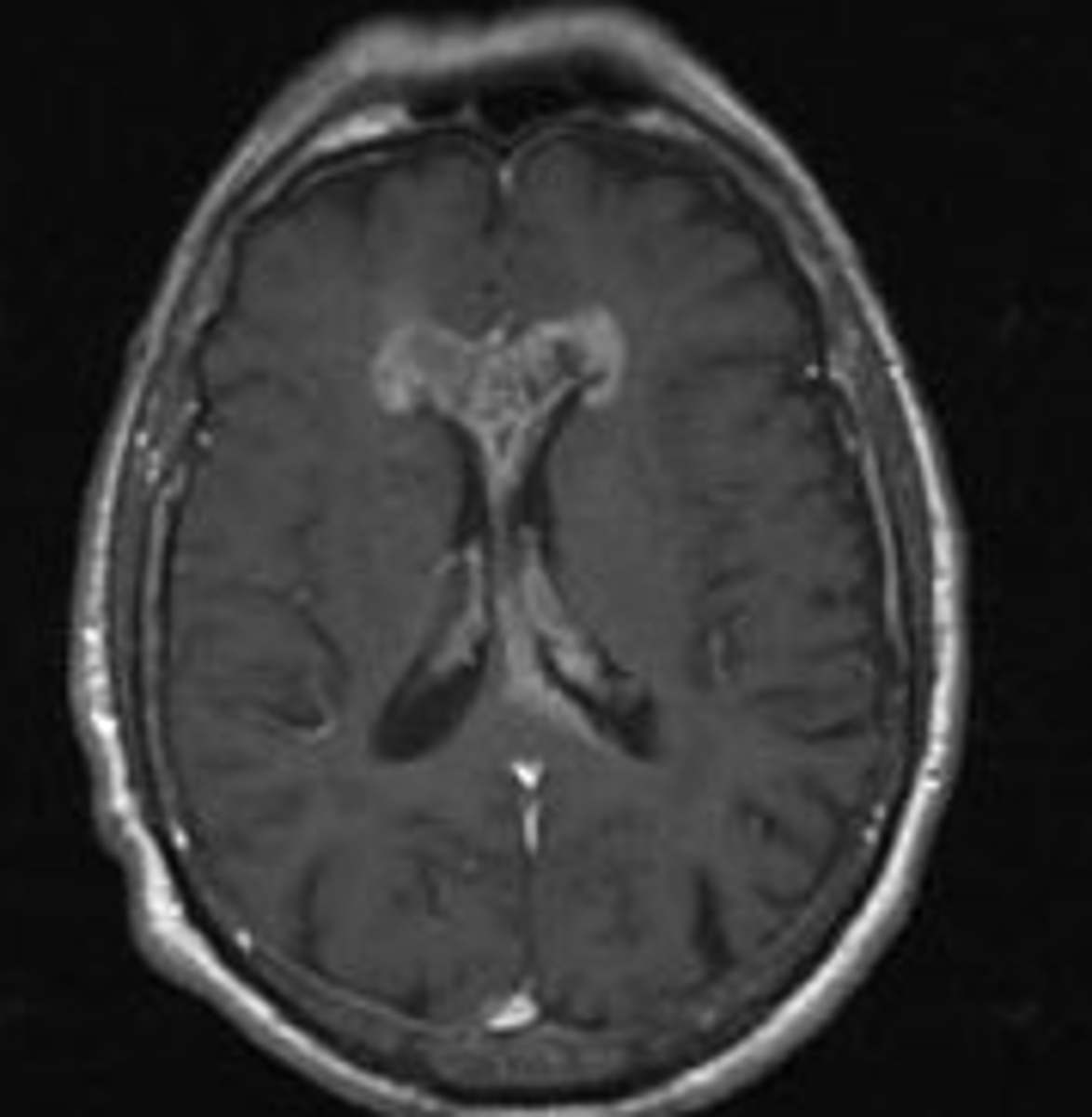
butterfly glioma in Glioblastoma multiforme
tumor crossing corpus callosum
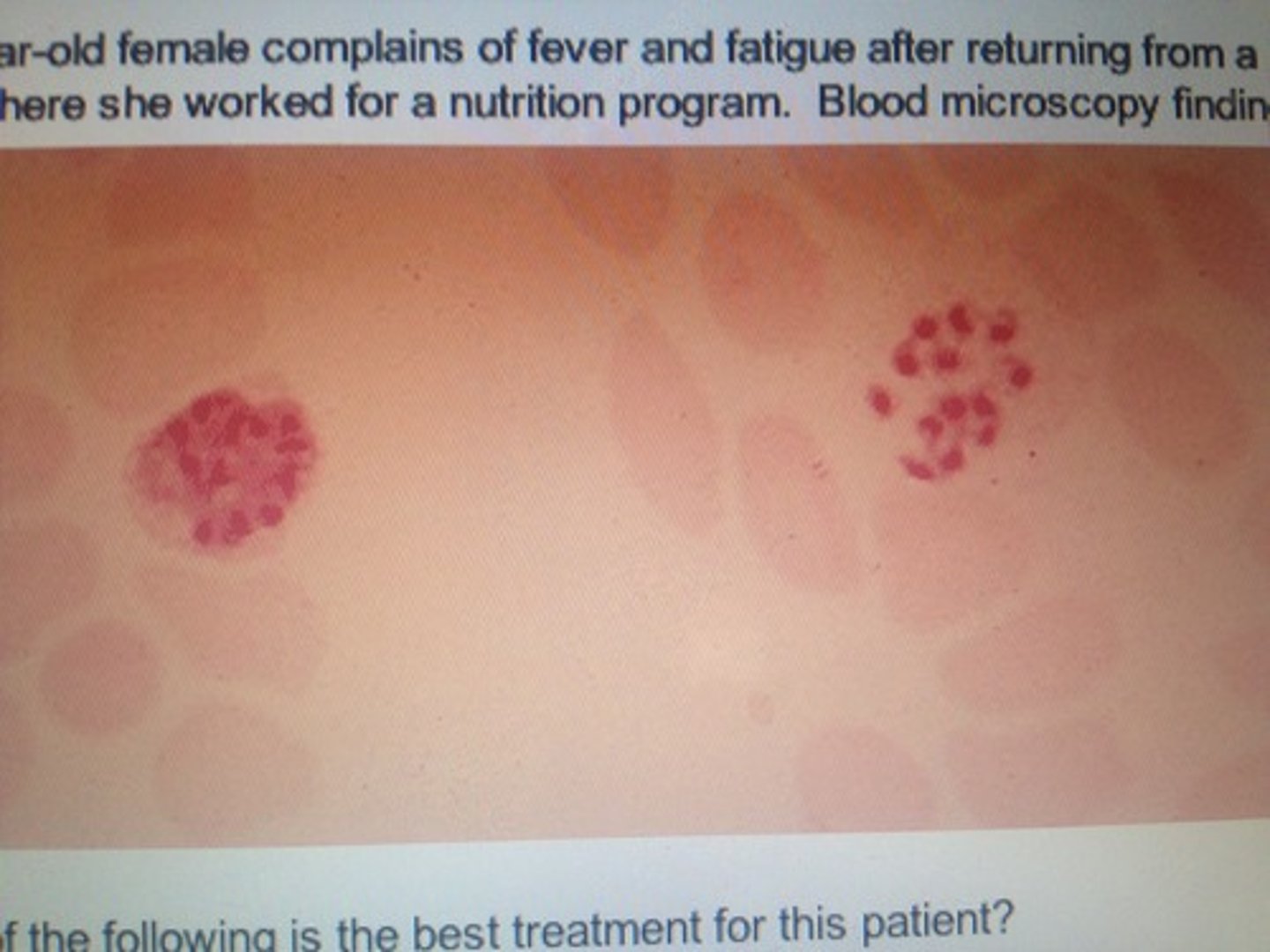
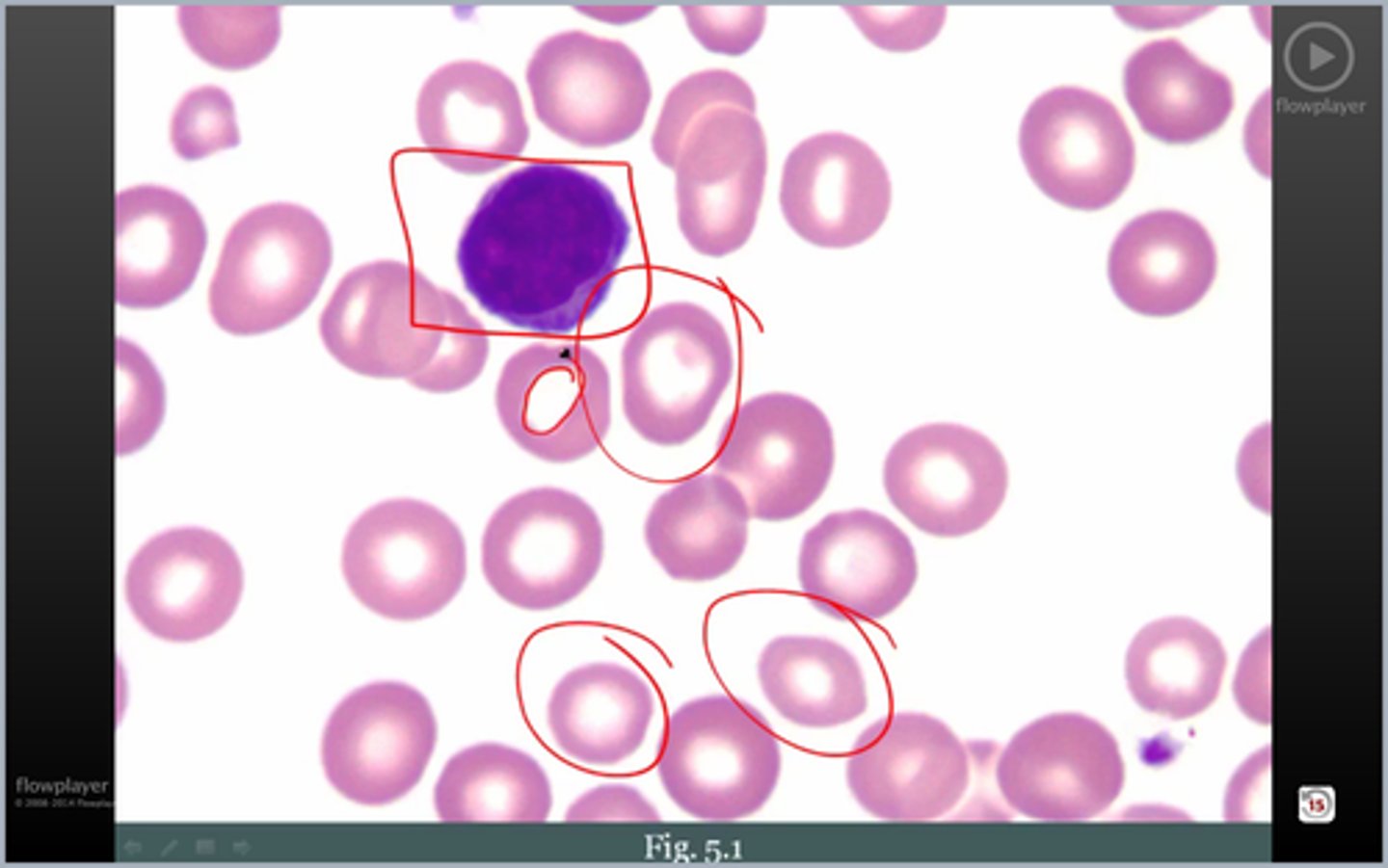
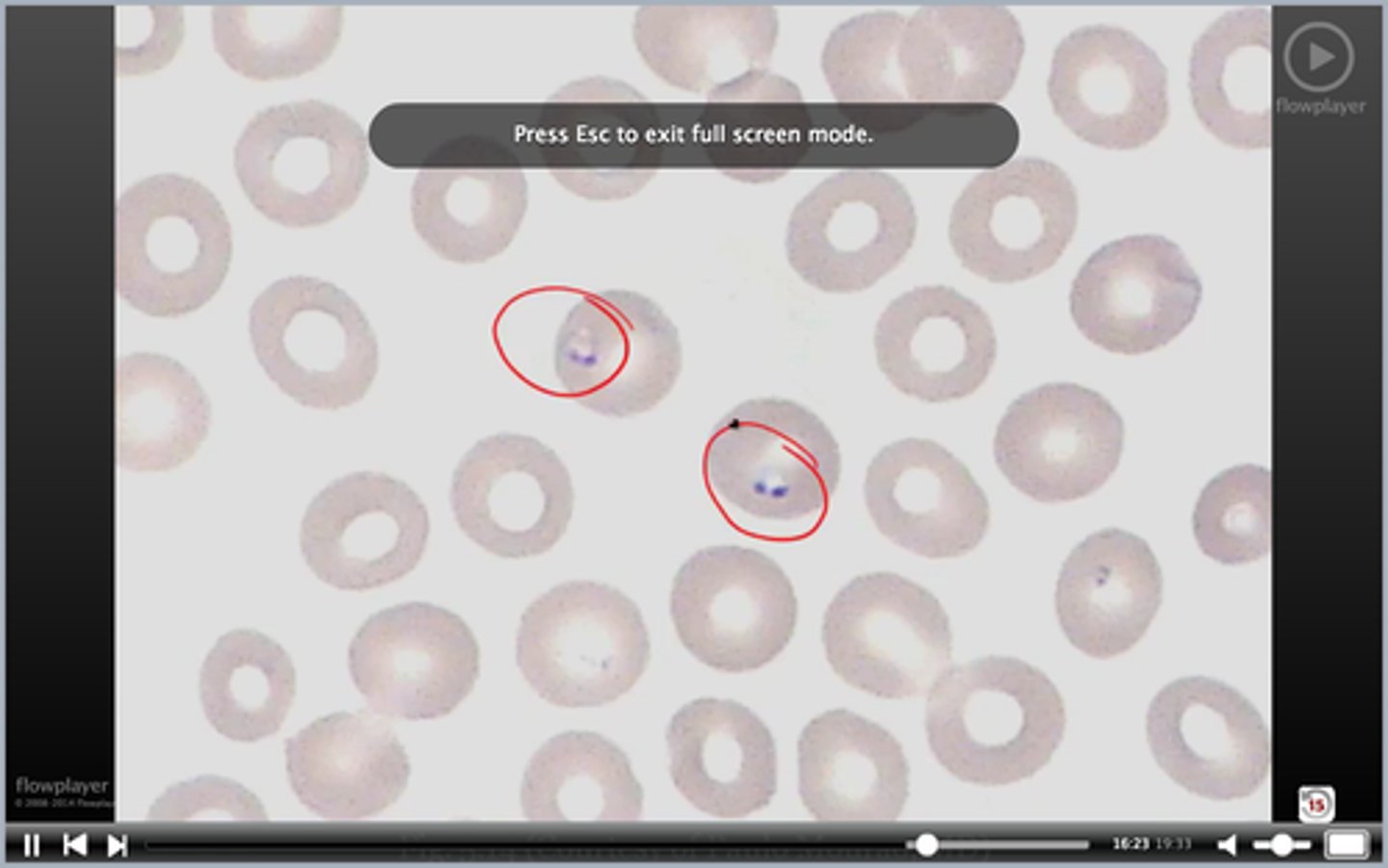
plasmodium/malaria
Tx: chloroquine/Mefloquine
blood smear. Tx?
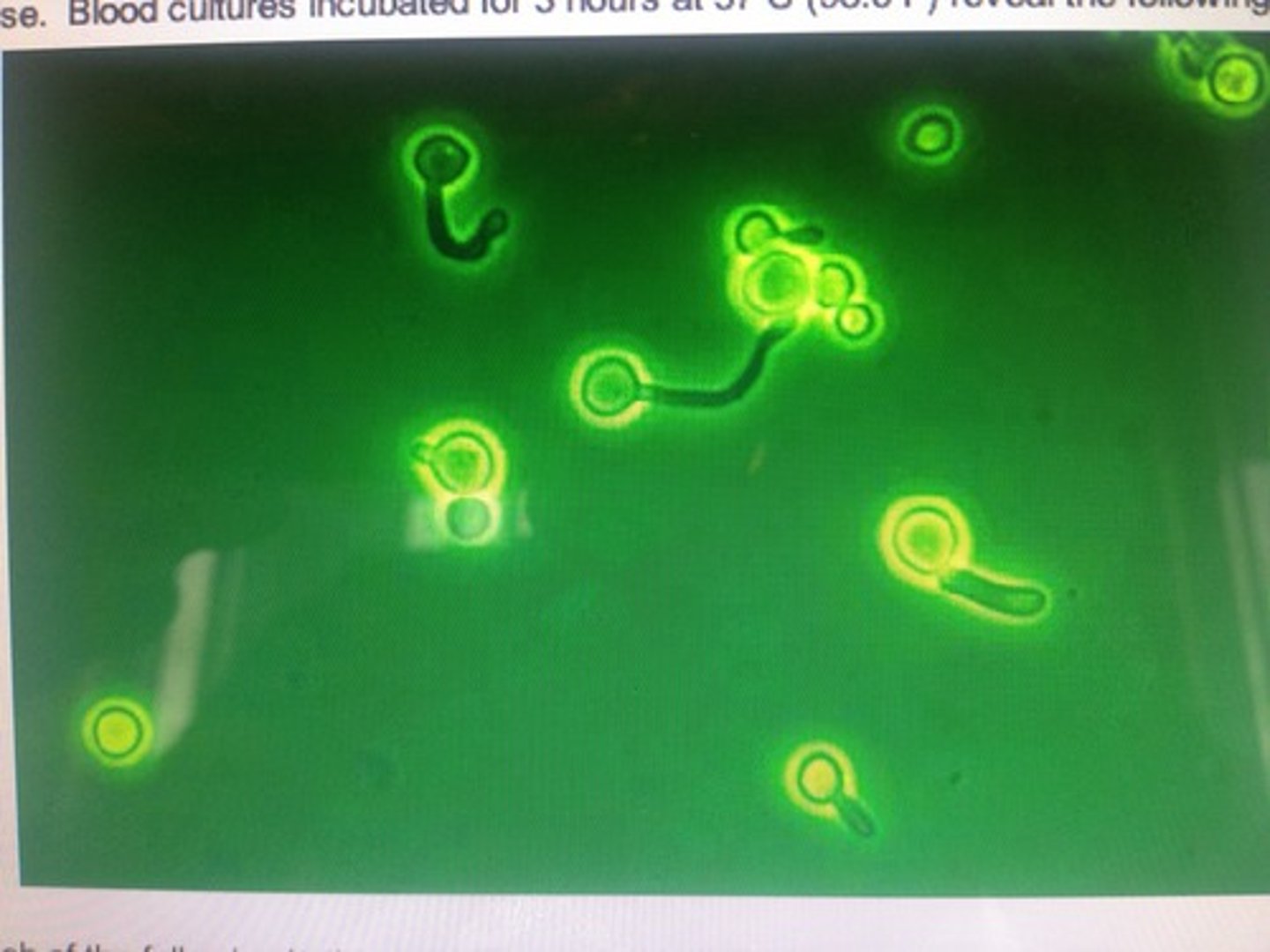
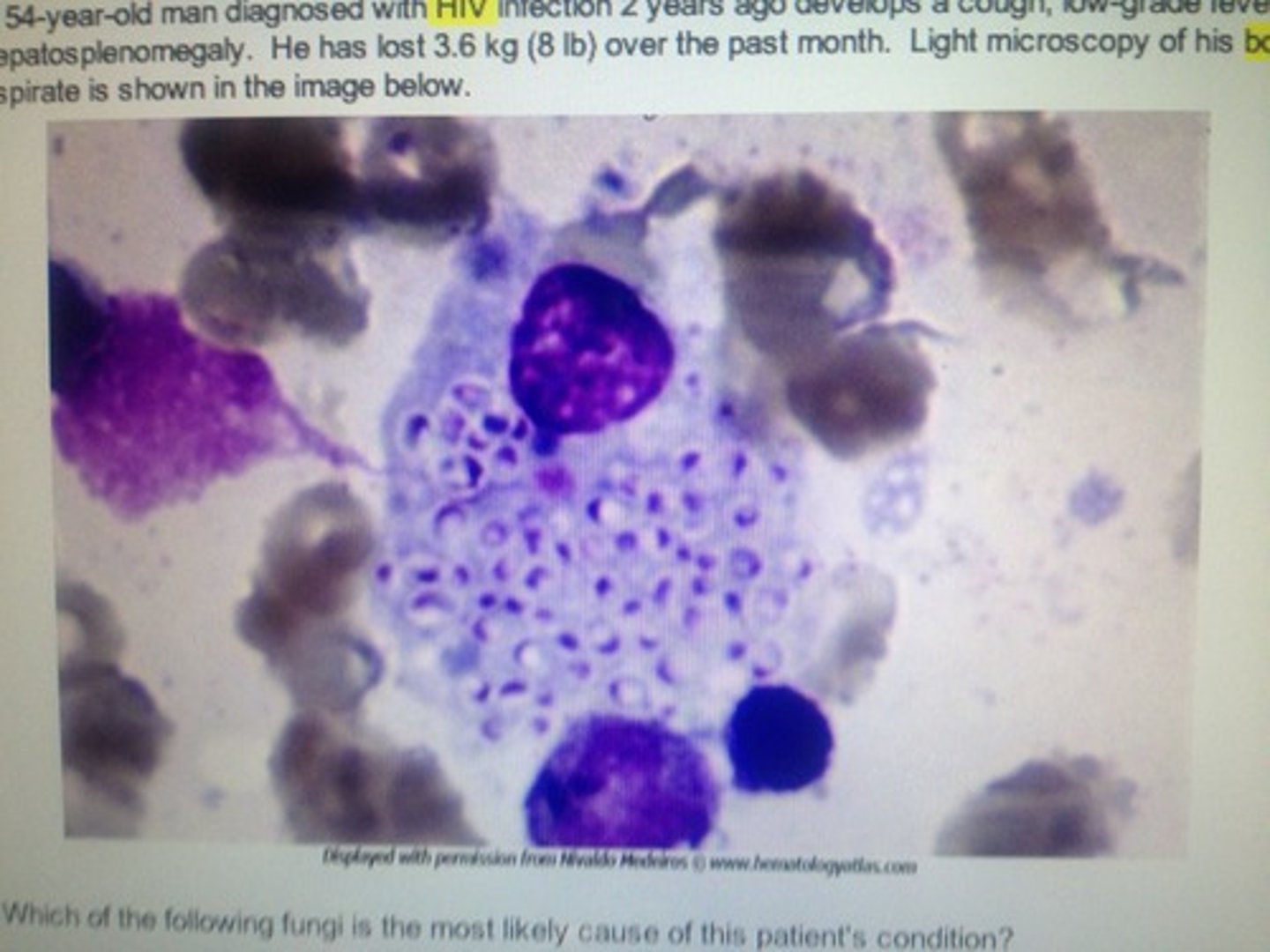
candida (know this img)
ID the opportunistic mycoses
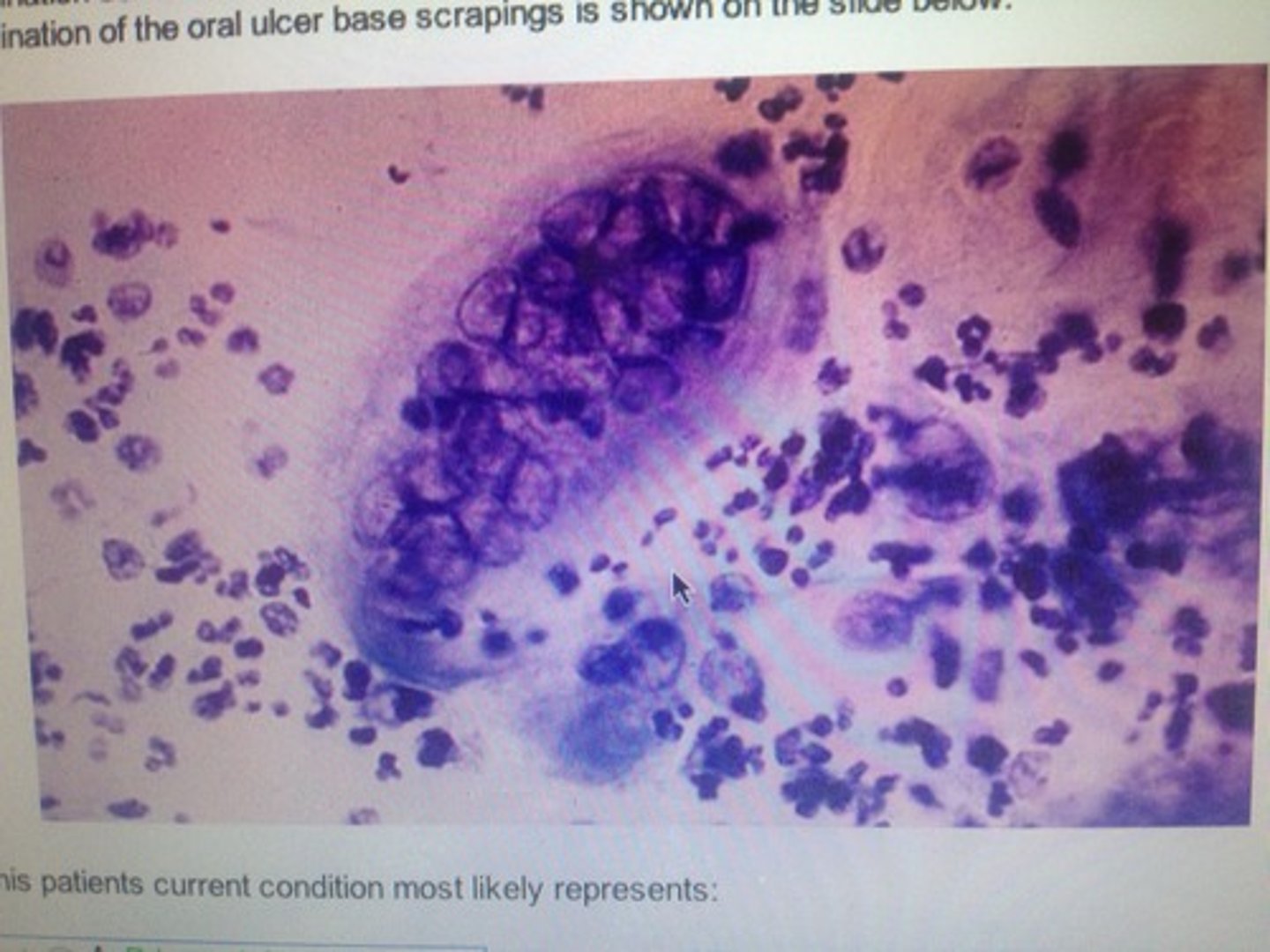
looks like a stoma (mouth)
think gingivostomatitis -> 1º HSV infxn
ID this smear
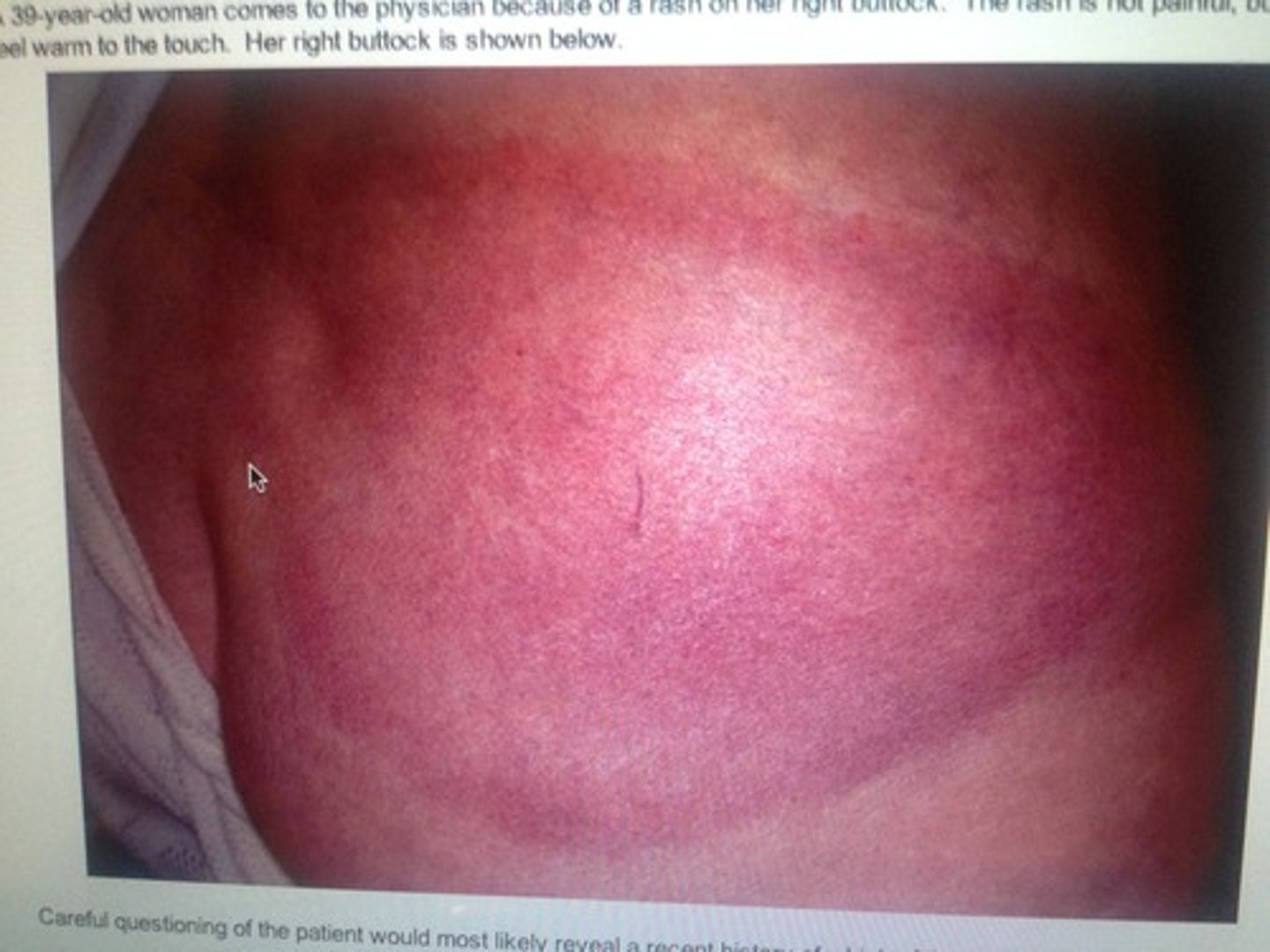
jk what cutaneous lesion?
borrelia (lyme Dz - Pt was fkn round in the woods); usu Cx lesion is erythema migrans = target sign w/ zone of central clearing but that's actually rarely seen so rmr this
ID whose ass this is
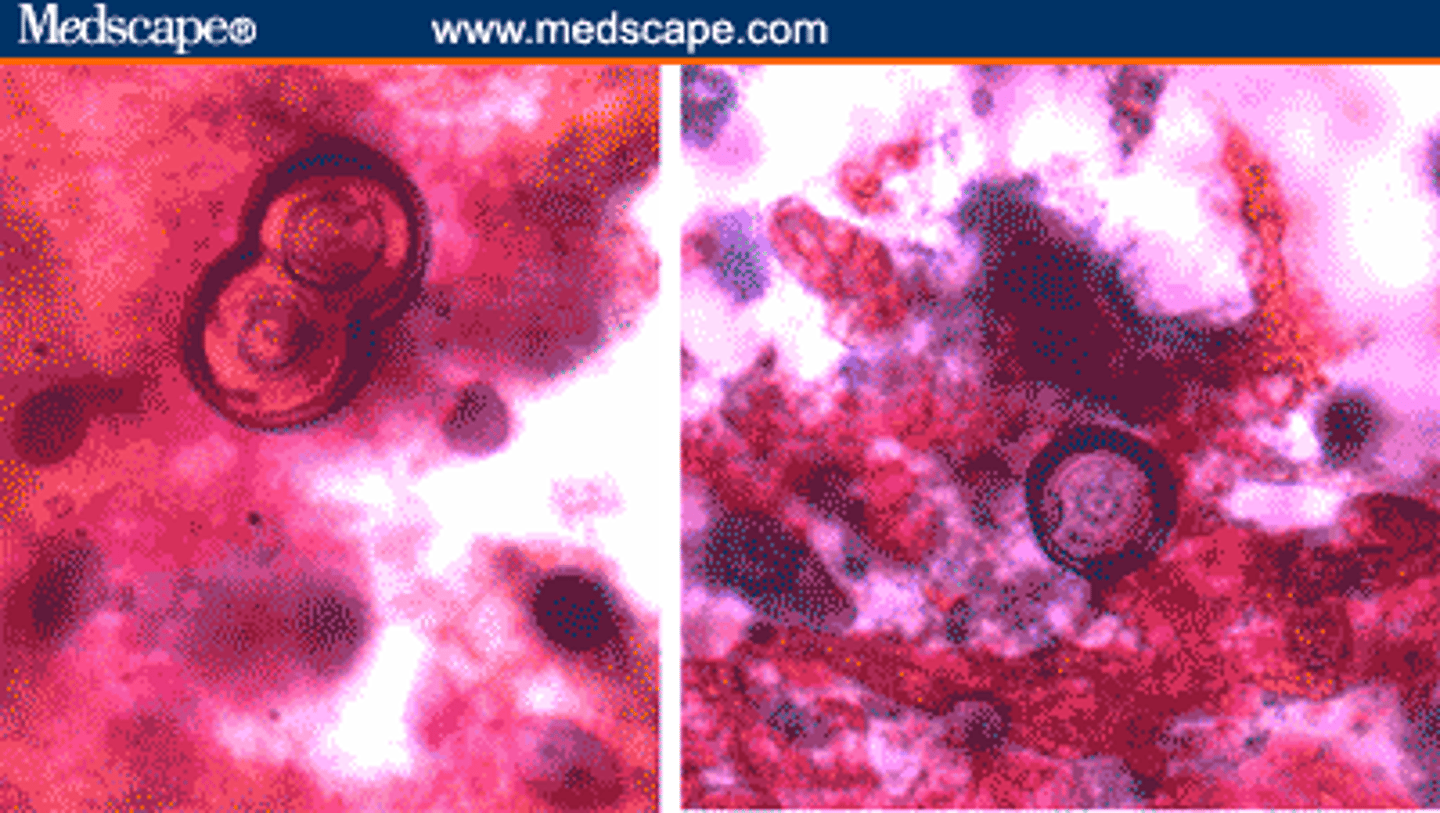
double refractive walls w/ broad based budding so think Blasto (focus on L pic); in great lakes, ohio, miss river
iD this fungi in lungs
notice how fungi is HIDING in macrophage, so Histoplasma
id this fungus in i-c Pt. (BM)
(arrow points to intranuc inclusion so u know its virus): CMV
interstitial PNA in transplant Pt.

ecythemic gangrenosum d/t Pseudomonas
necrotic patches in skin in cancer Pt. d/t

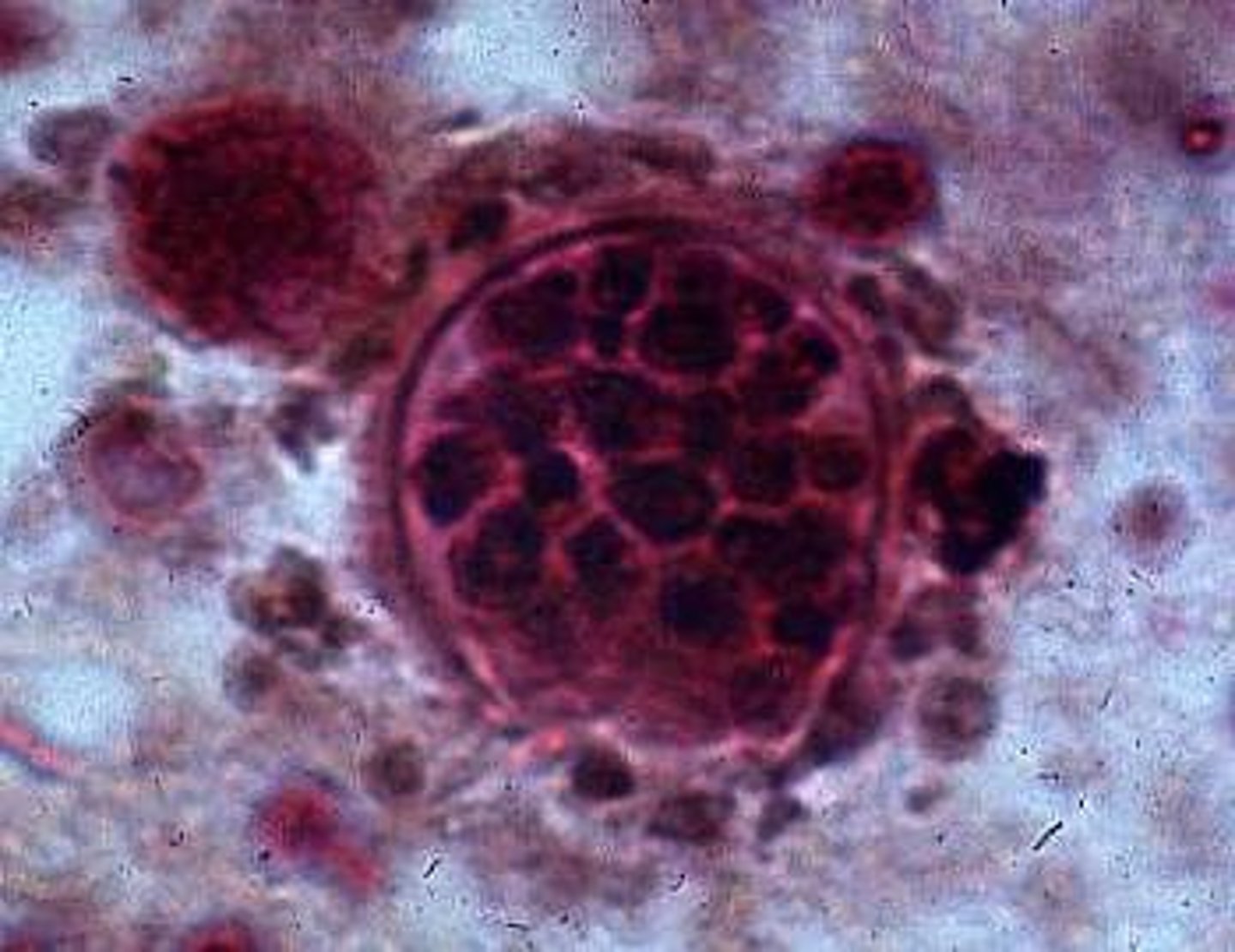
spherules containing endospores (coccidio)
fungal
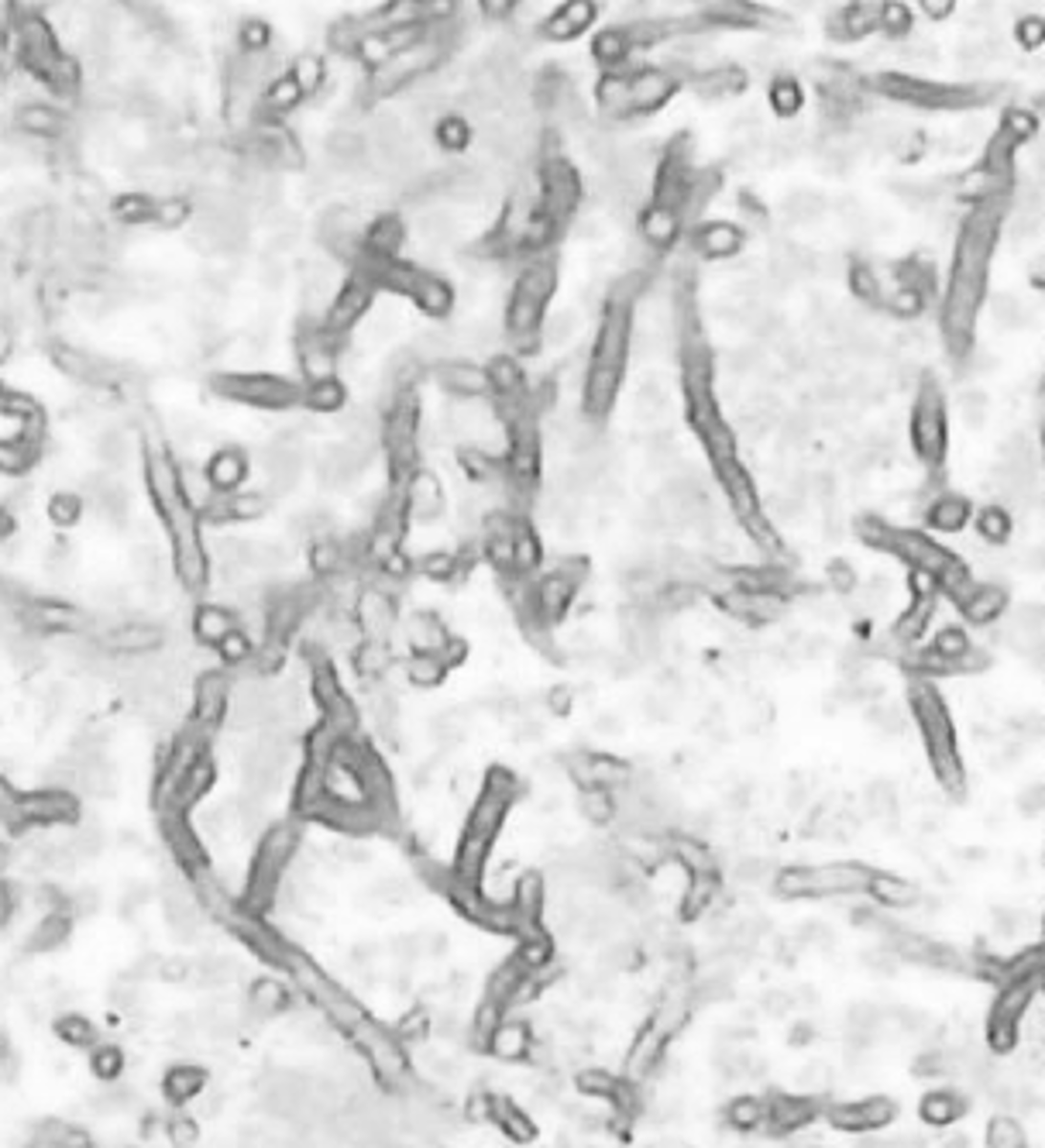
notice acute angles ("V"): aspergillus fumigatus
fungal2
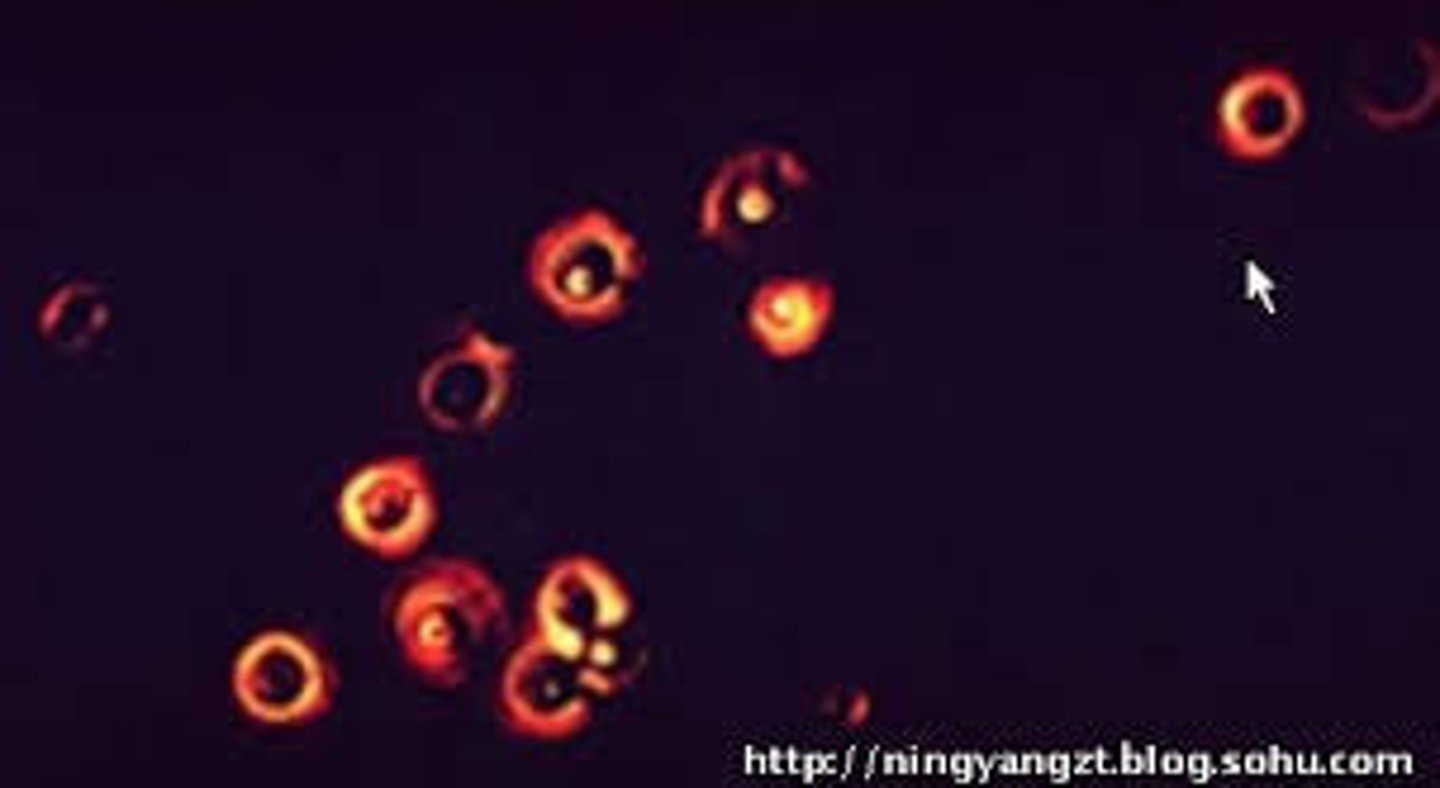
india ink stain: crypto/HIV Pt. with meningitis
ID Cx stain/bug/Pt/Dx
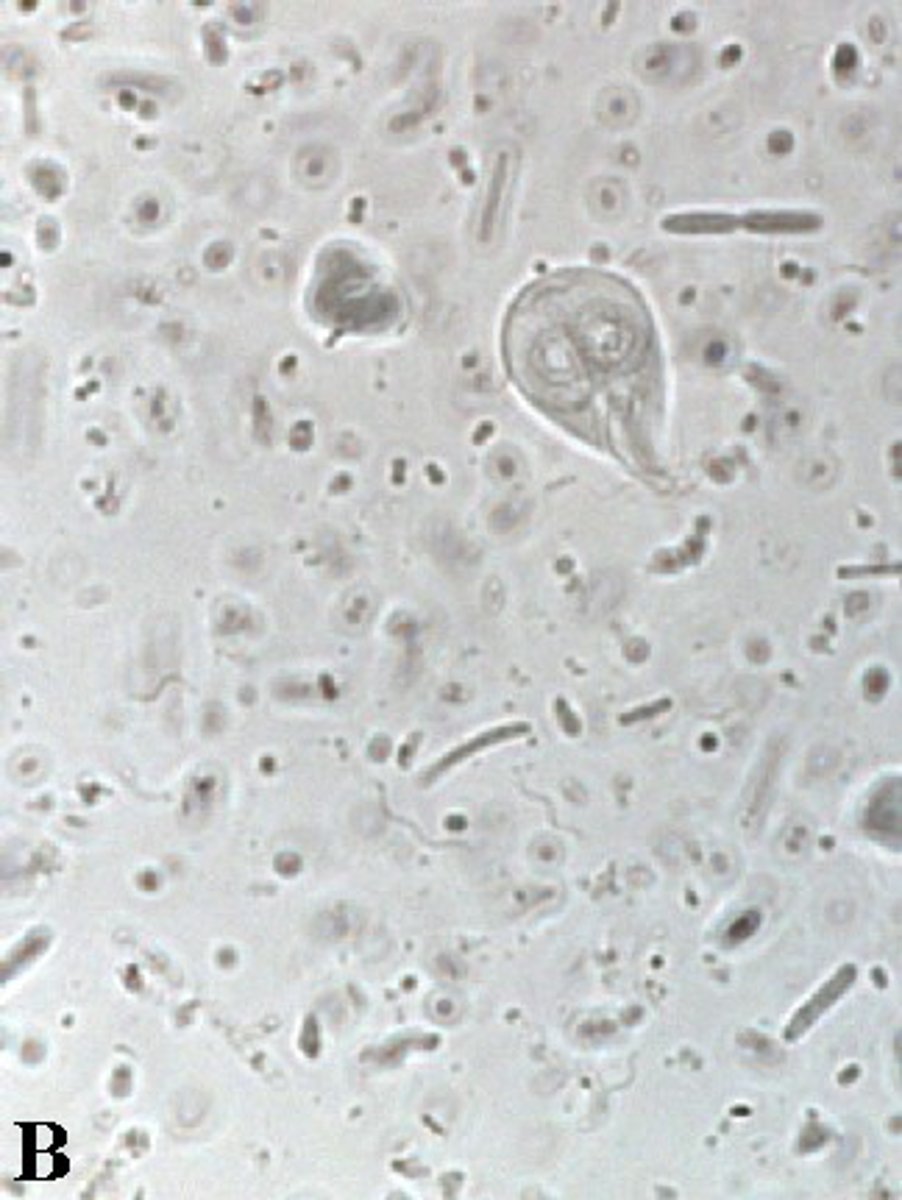
tear drop w/ owl-like face
GIARDIA
recurrent diarrhea d/t protozoan
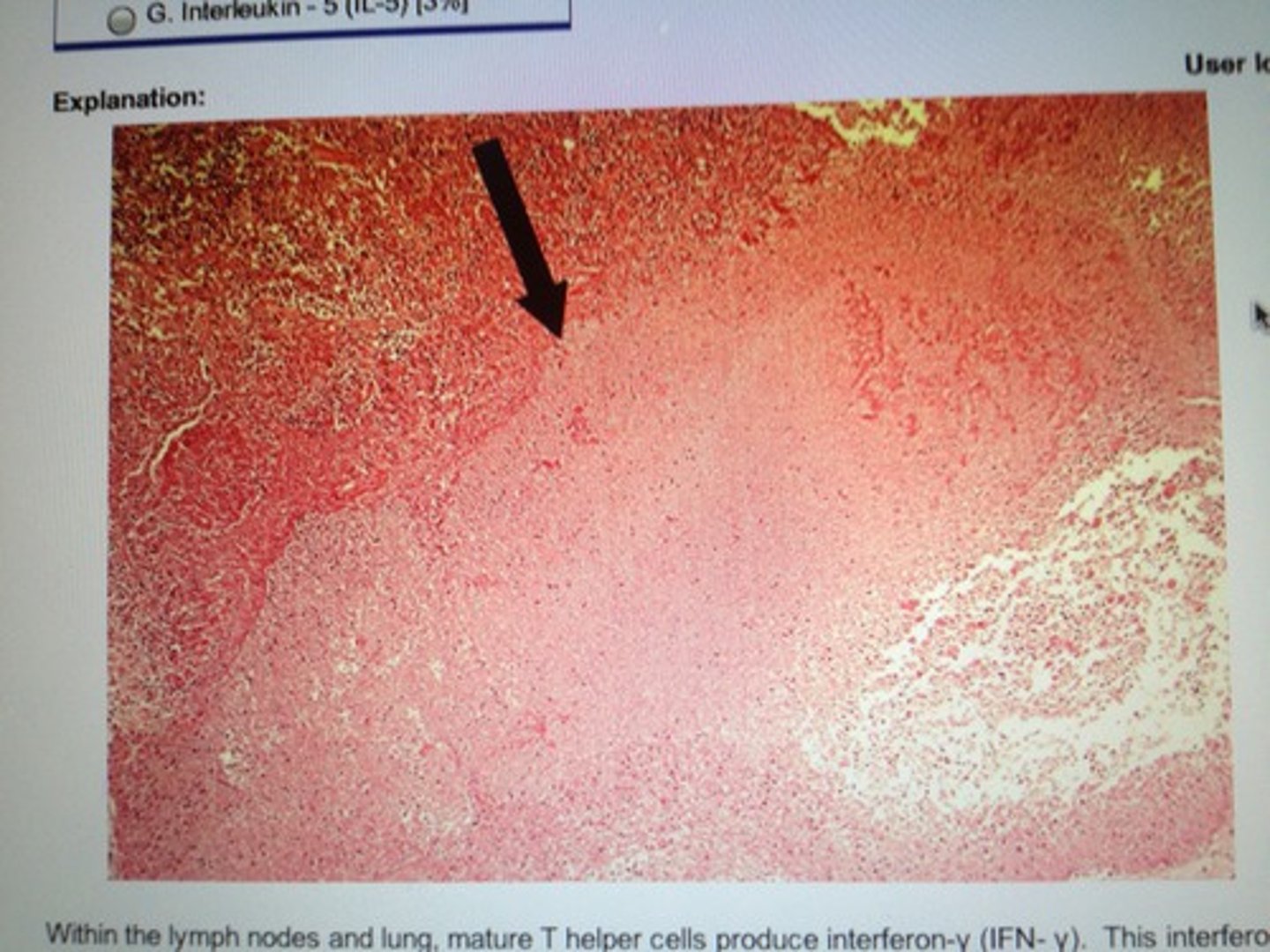
granuloma (Tb)
-IFN-y
the hell is you lookin at; also what cell responsible for this?
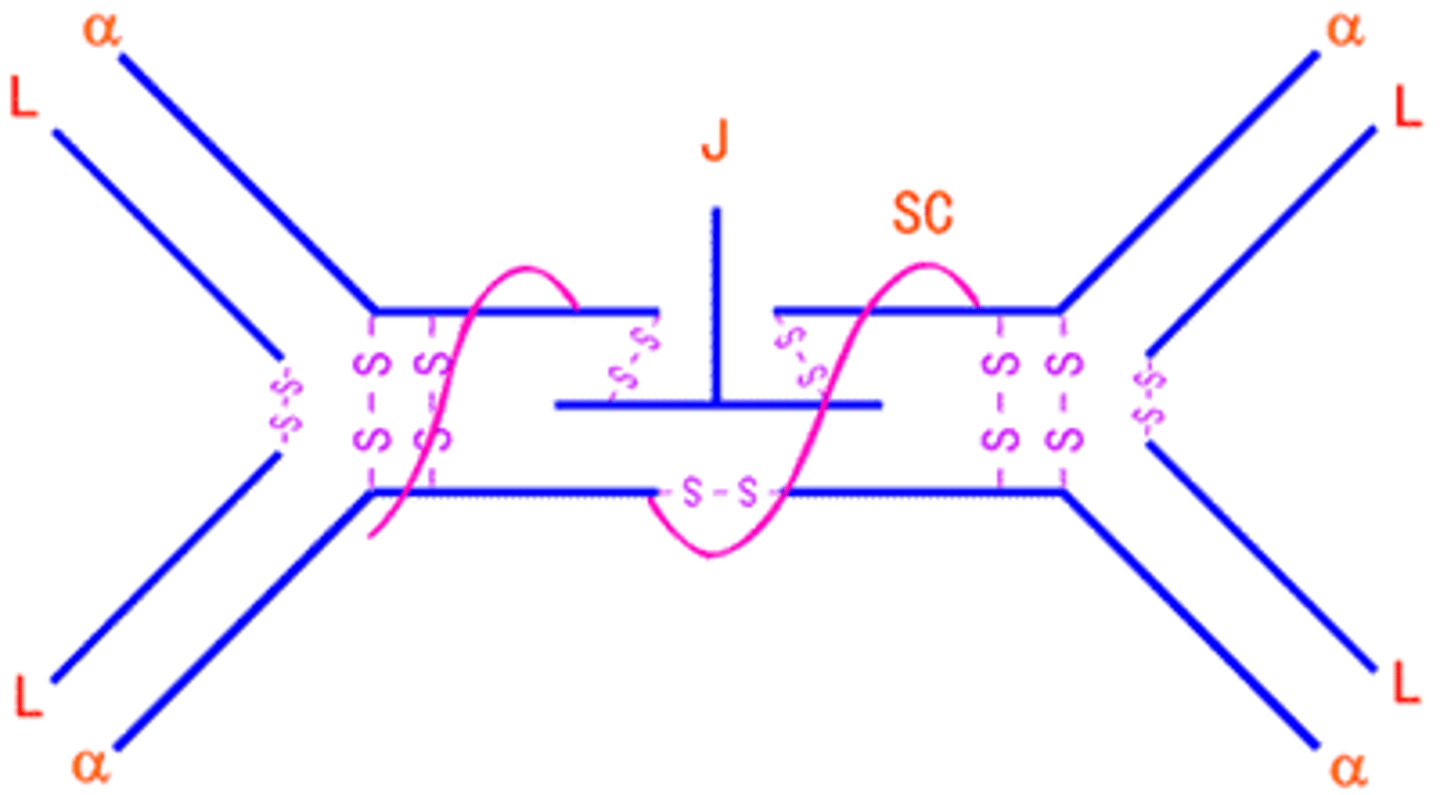
2 Ig monomers:
J in middle = J chain; SC = secretory component
secretory IgA: found in colostrum (also tears, saliva, mucus)
name the Ig; primarily found in
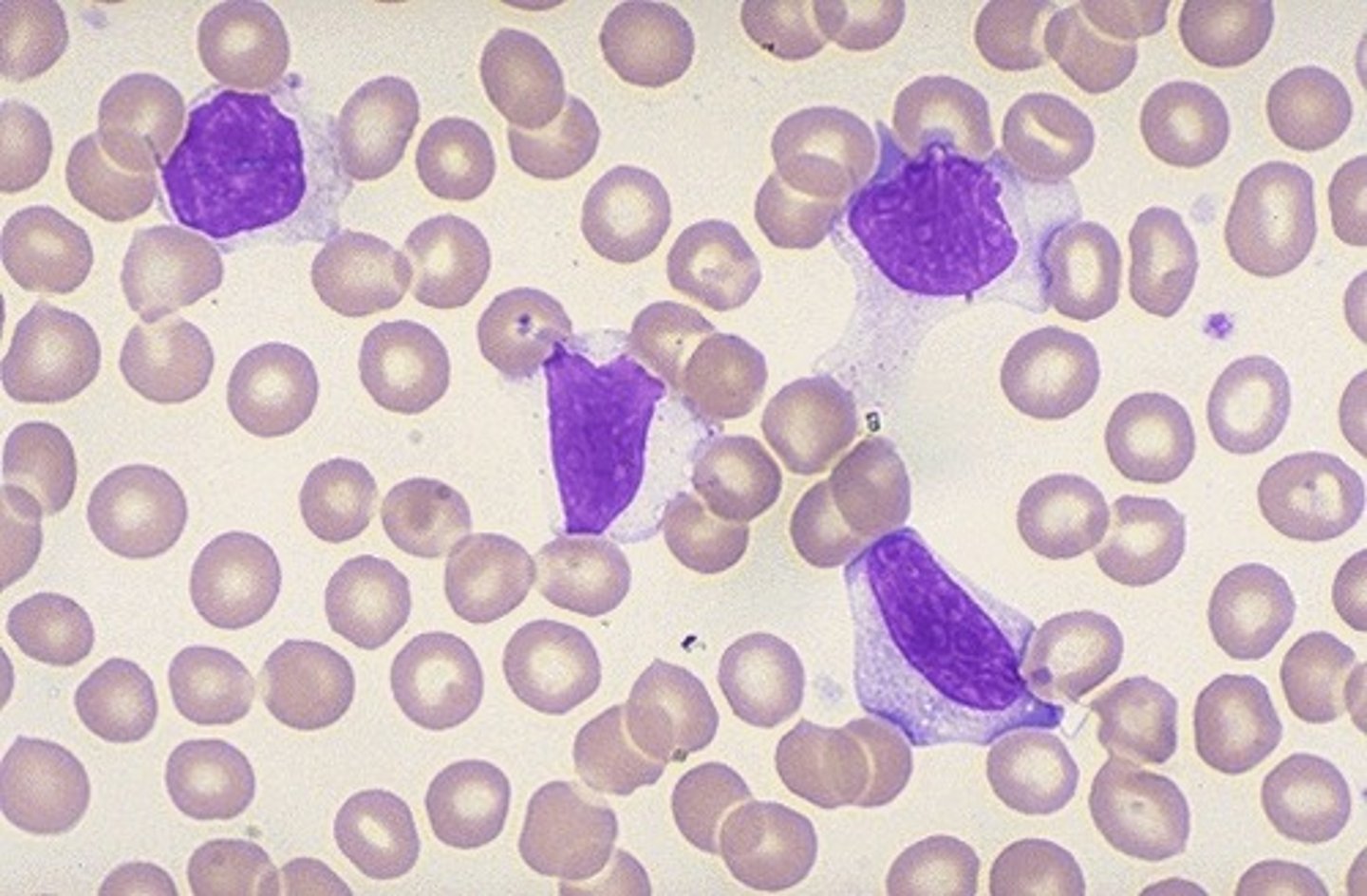
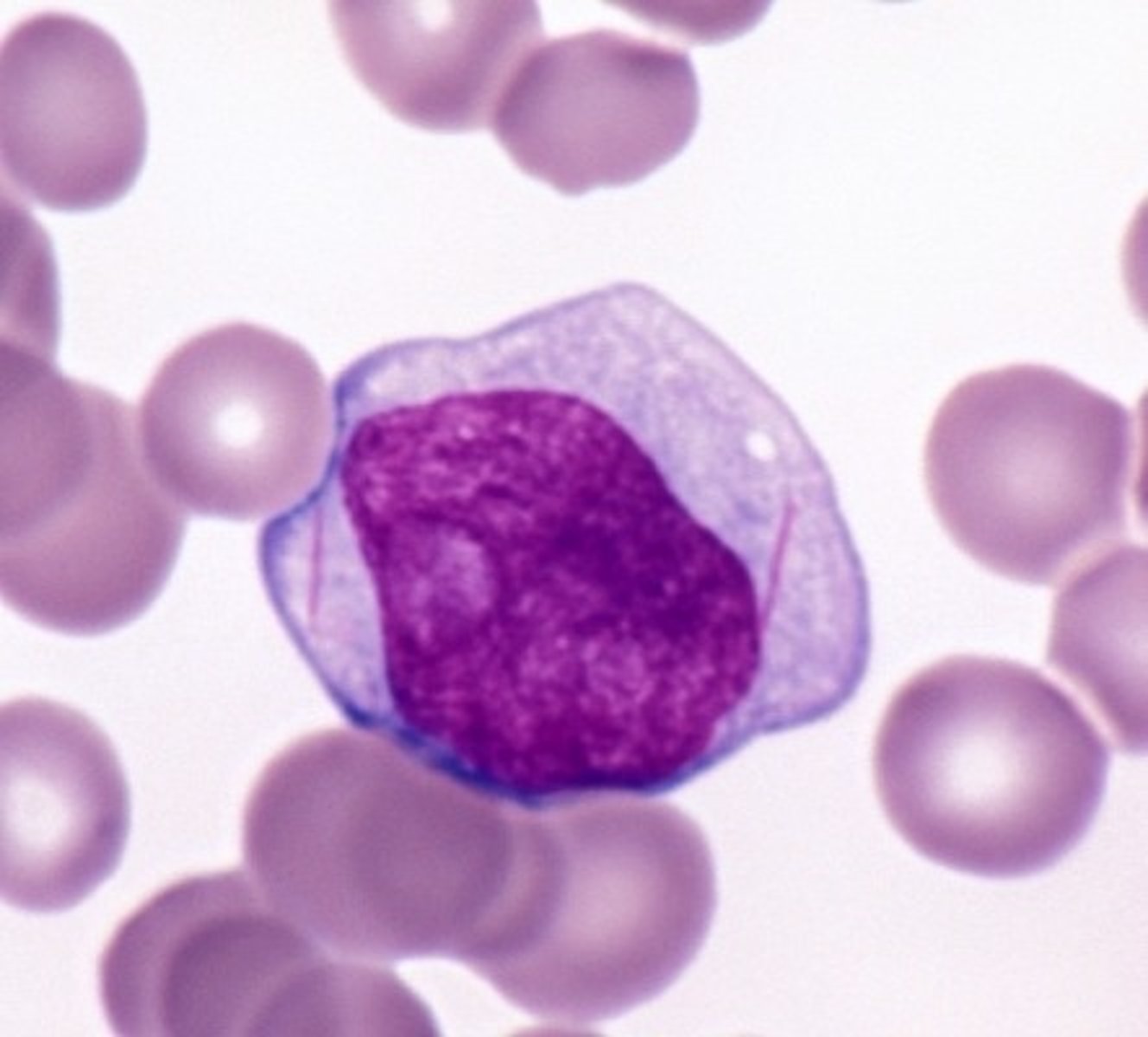
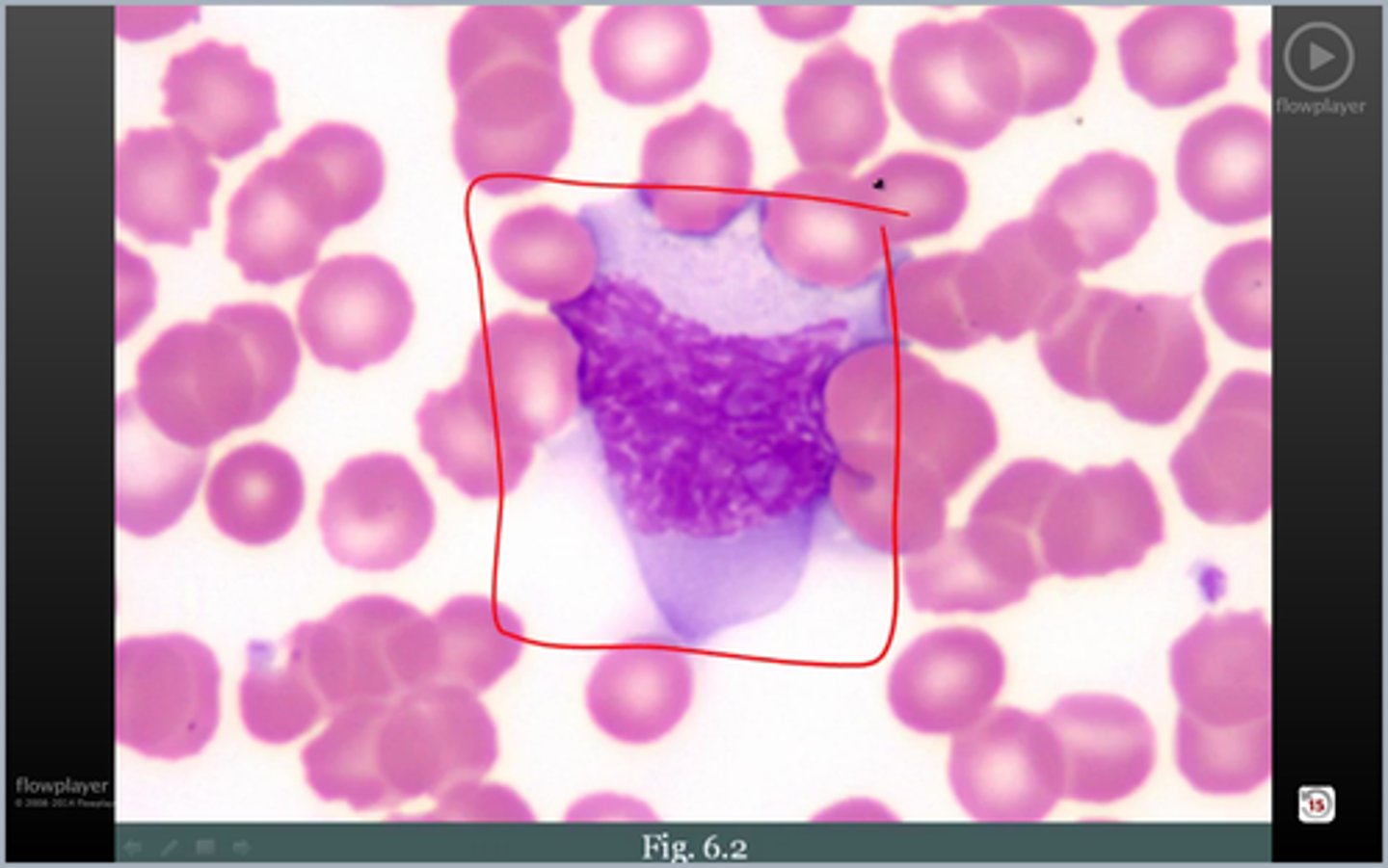
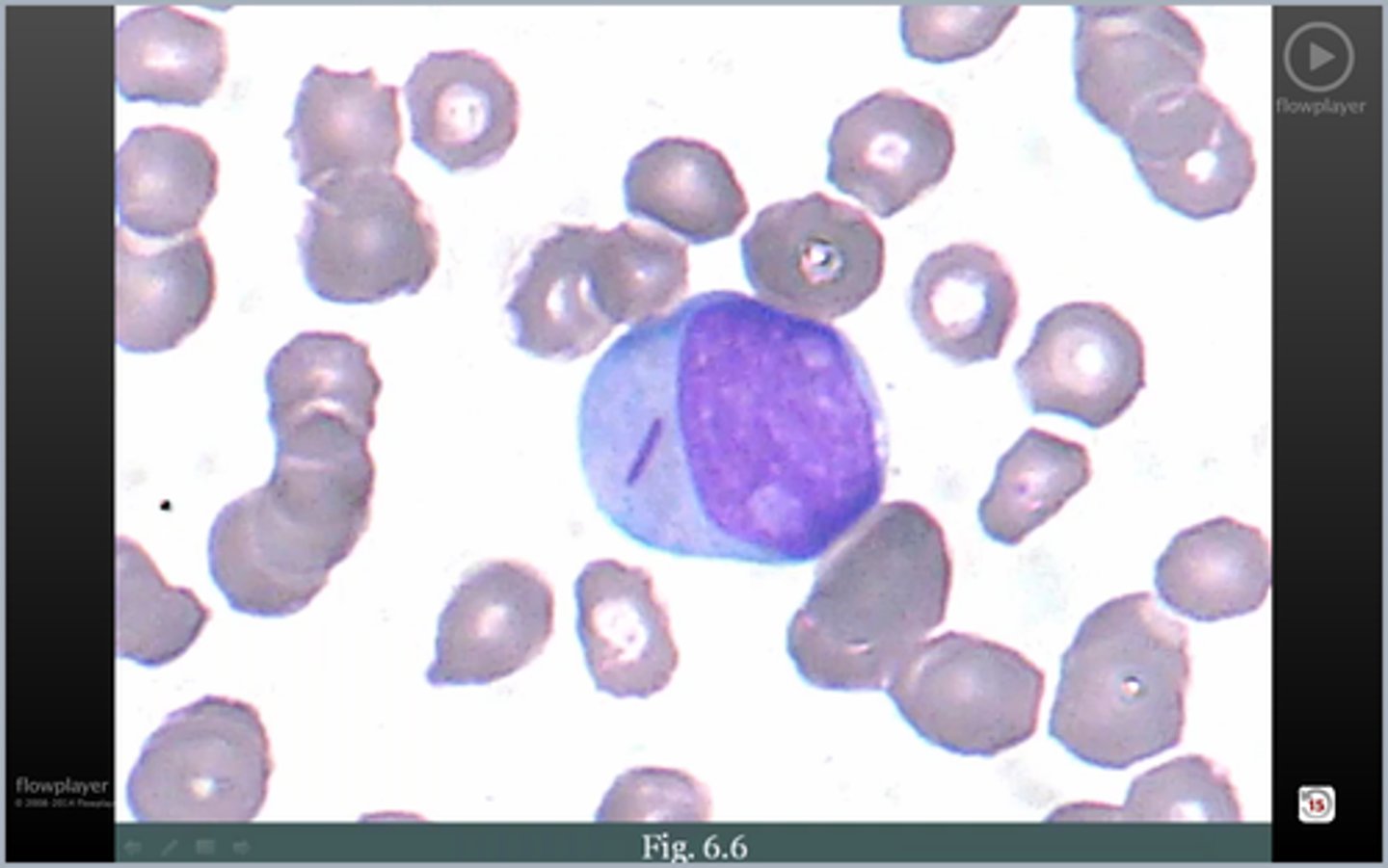
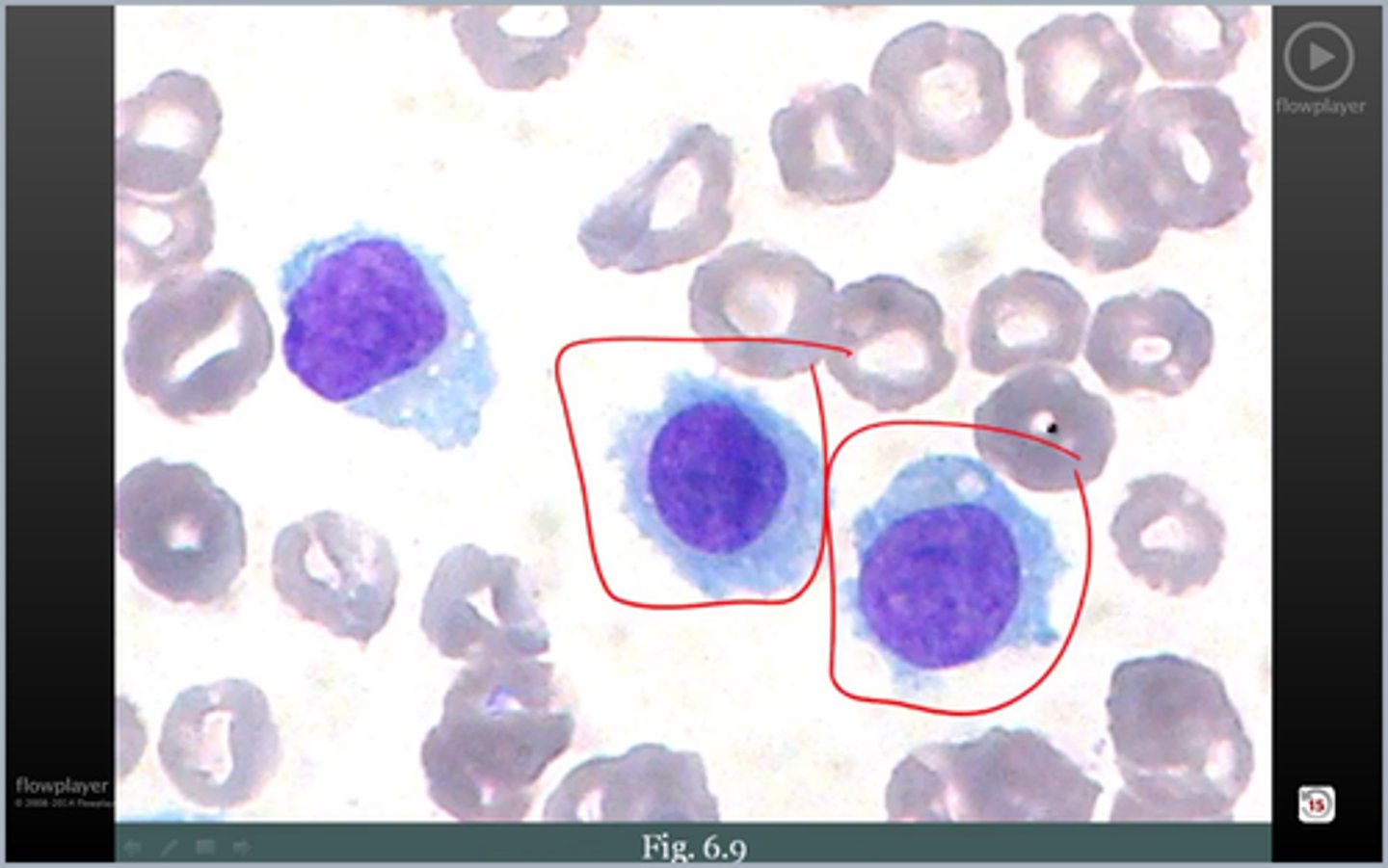
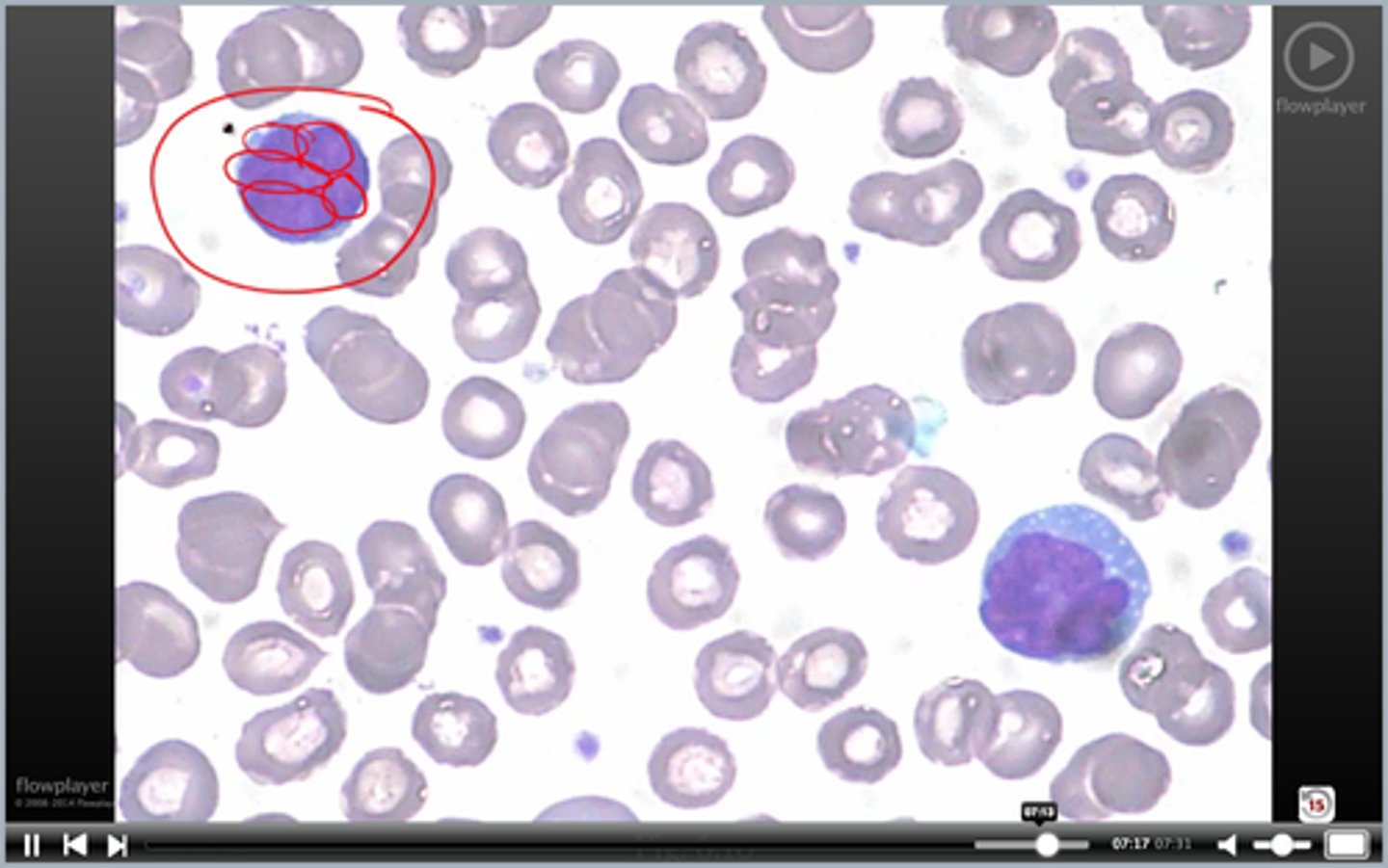
atypical lymphocytes (activated CD8 T cells);
seen in infectious mono (d/t CMV or EBV)
what are these?
Dx?
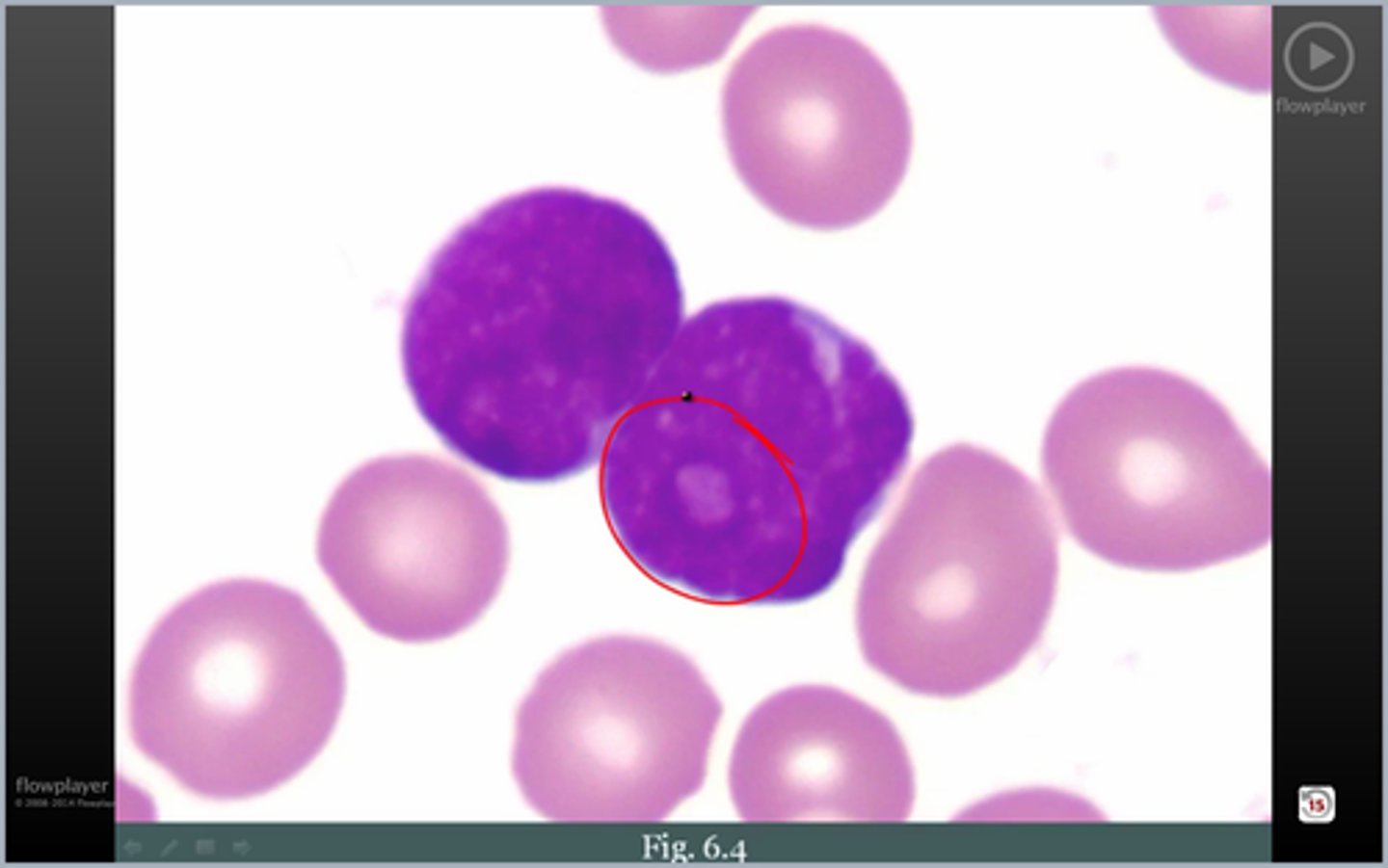
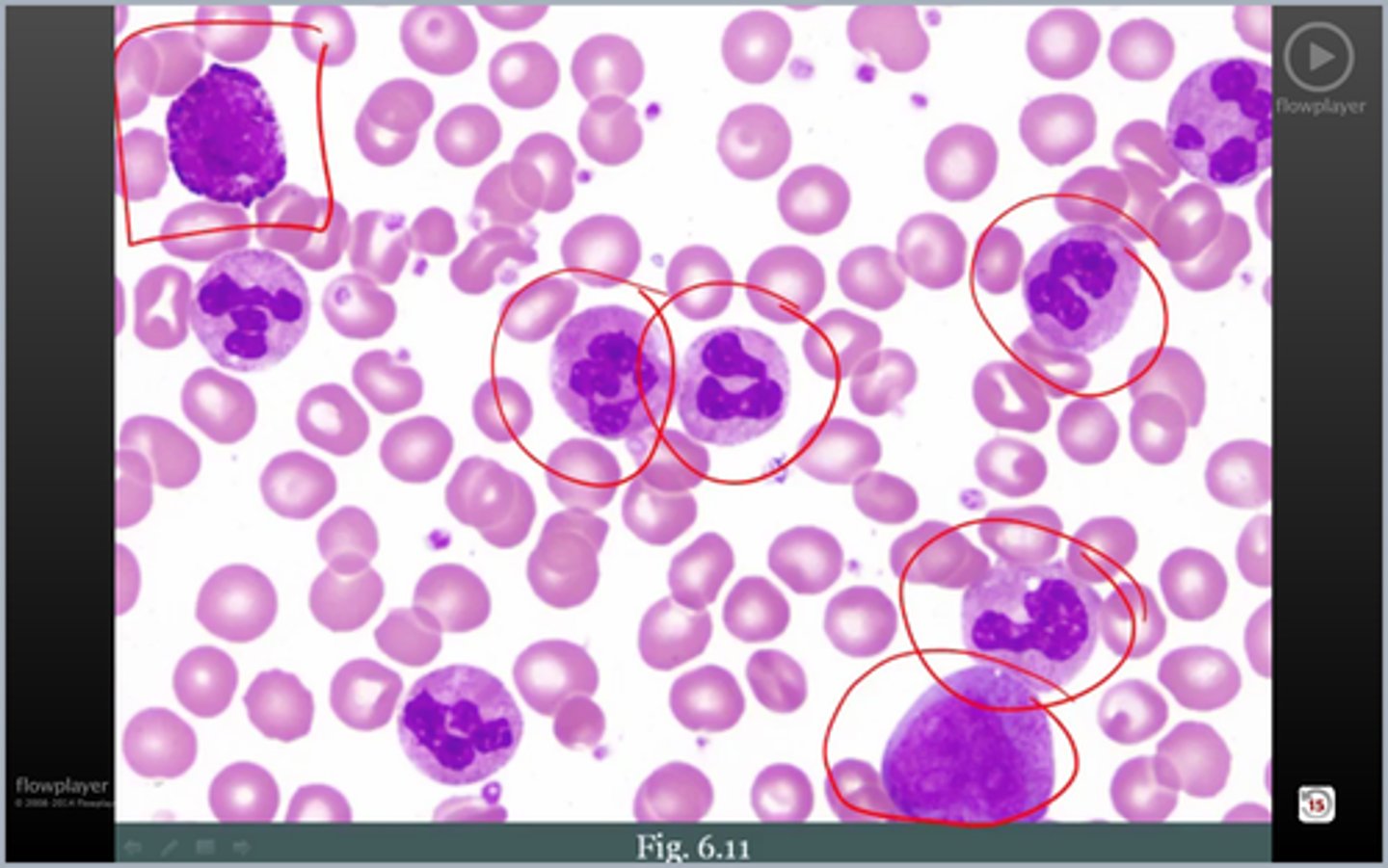
myeloblasts w/ coarse rod-shaped intra-cytoplasmic granules aka auer rods; think AML
seen in blood smear
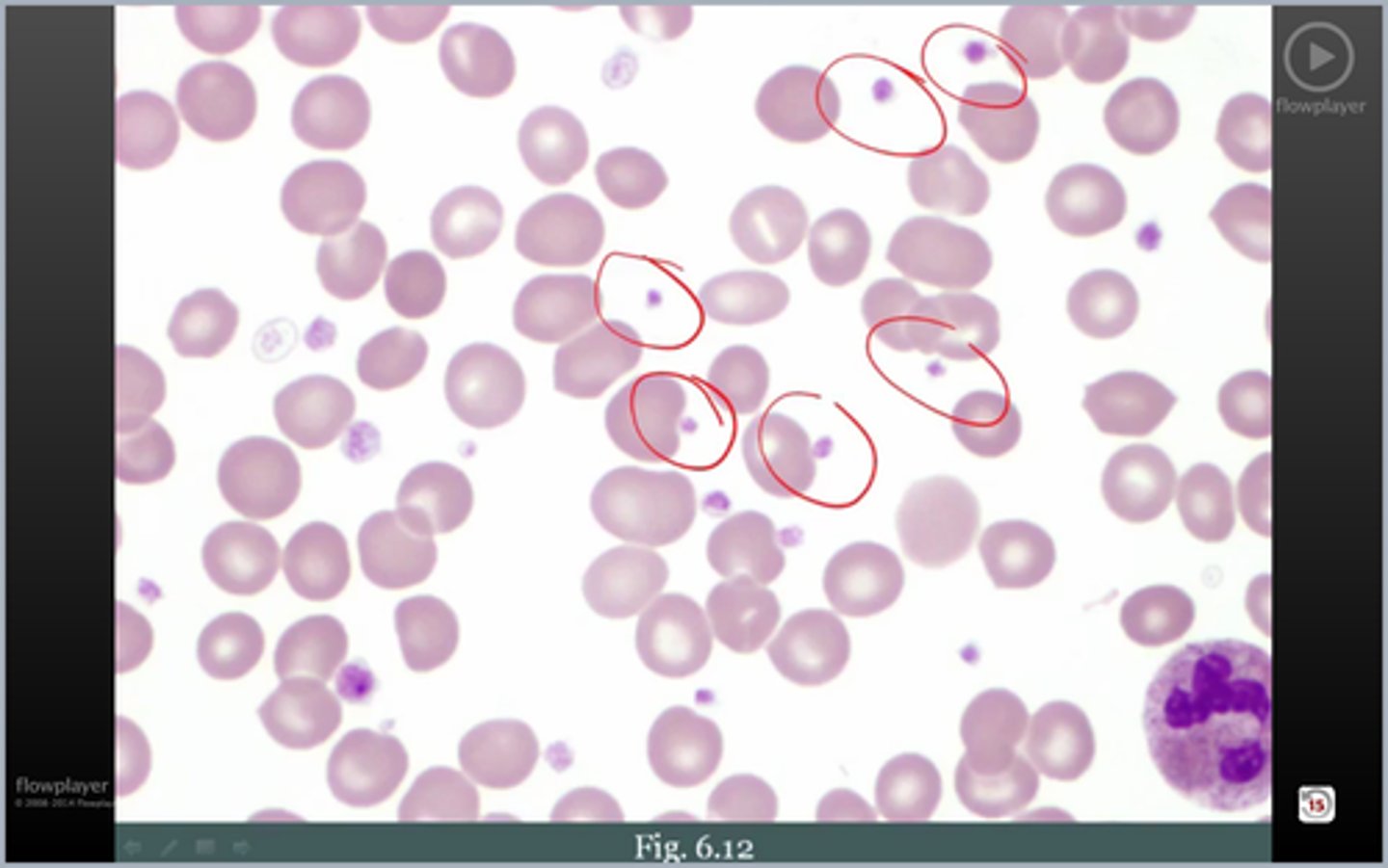
neurofibromas, so think NFT1
cuatenous lesions are?

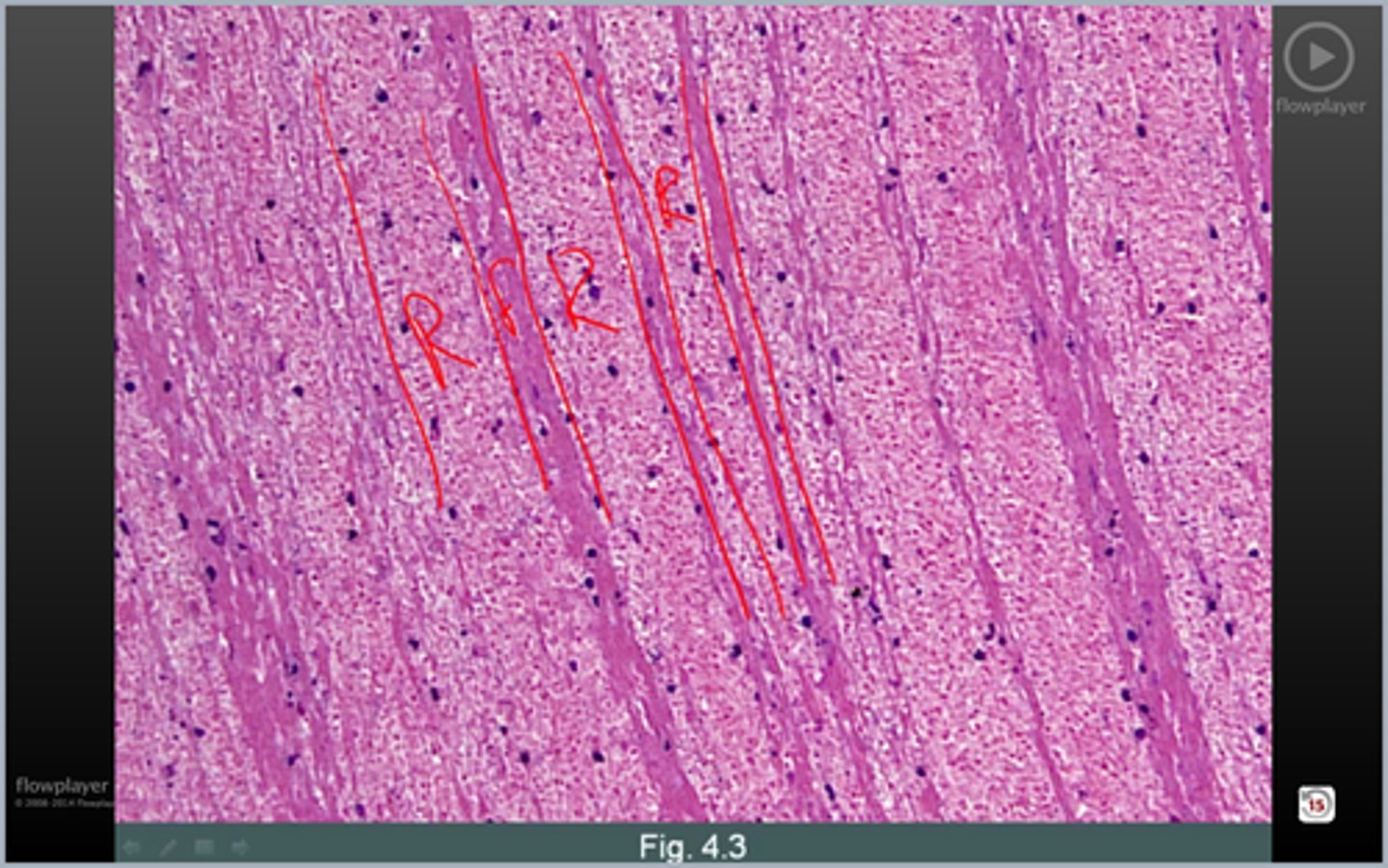
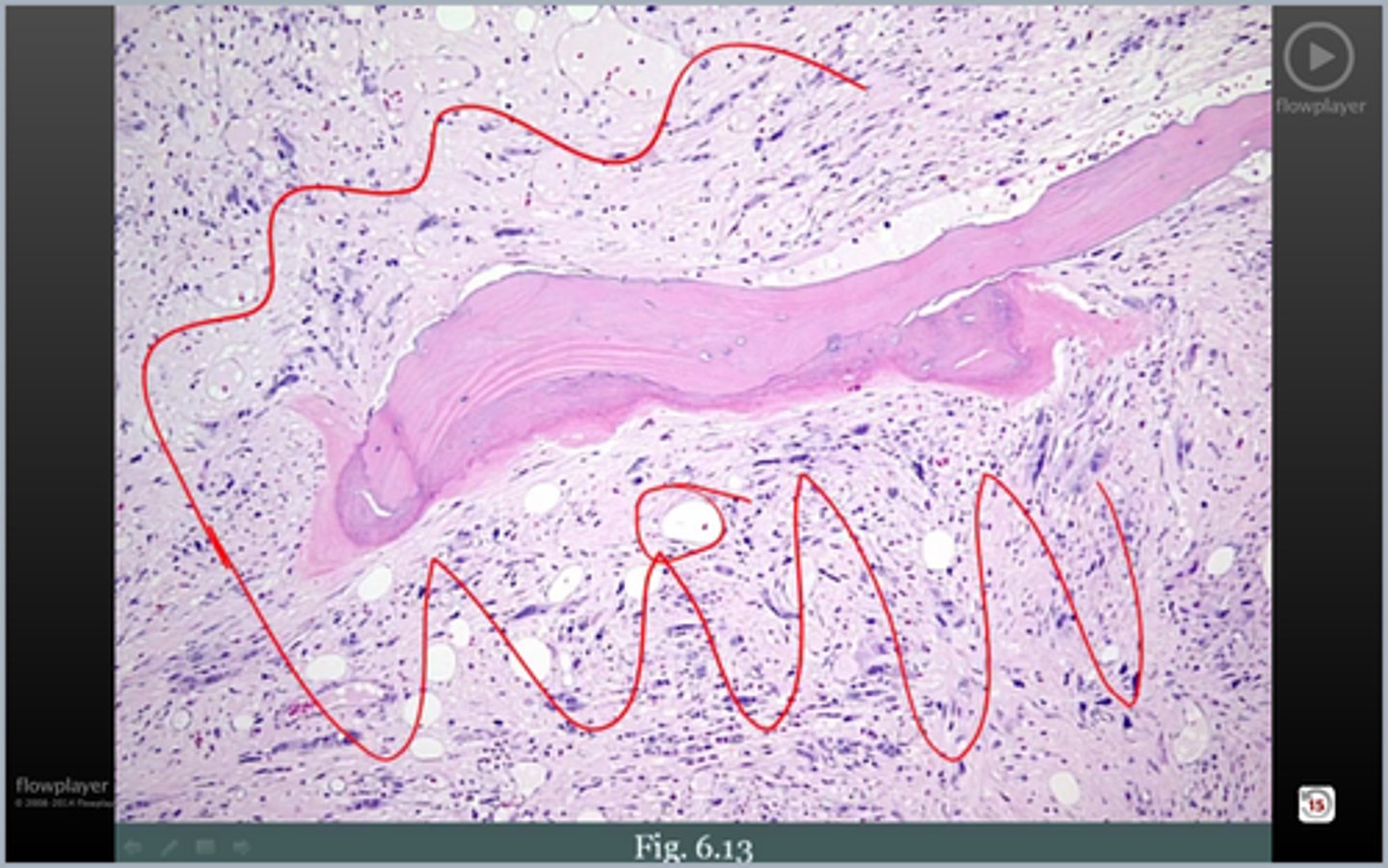
LVHT
hypertrophy bc cardiac myocytes have no stem cells to undergo hyperplasia, like sk. mm., can only undergo hypertrophy. notice L (HT) vs R (normal)
pathologic process involved

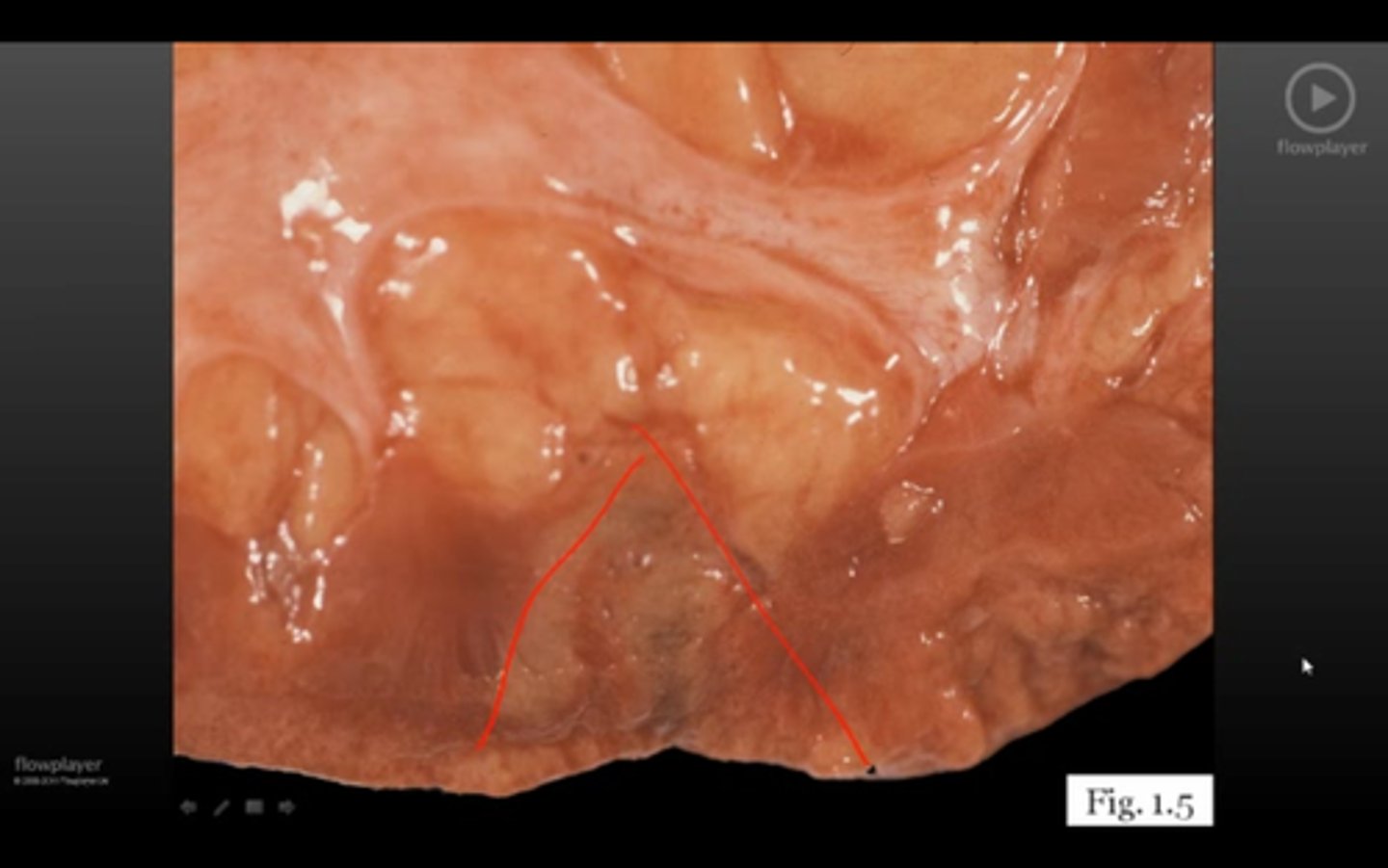
GERD -> barret's esophagus (non-K StrSq replaced by non-ciliated columnar epith w/ goblet cells) -> esoph ADCA
mucinous columnar epith on surface (asterisk) w/ underlying mixed mucous glands (arrows)
Id Dz (pathophys)

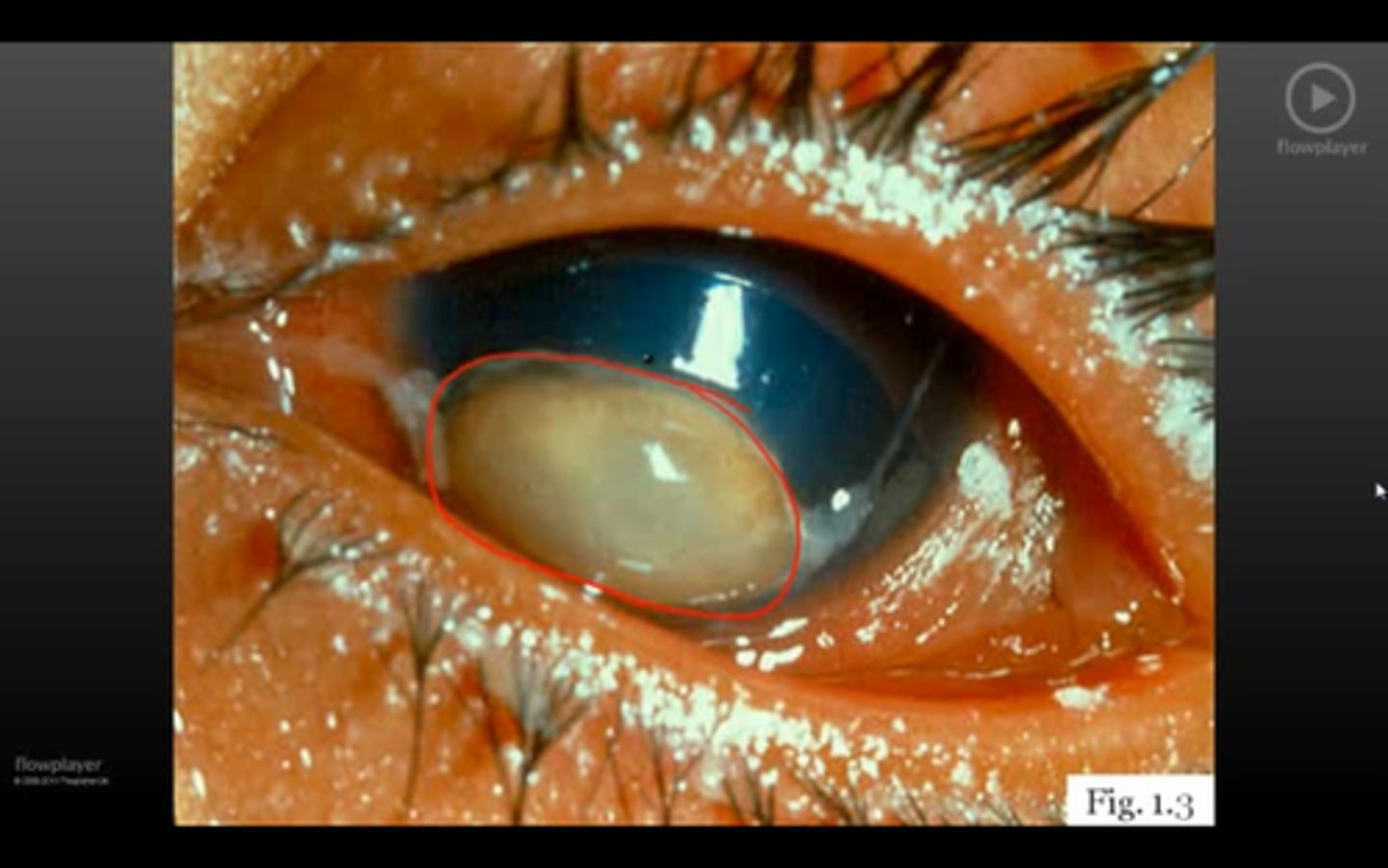
keratomalacia (notice thickened/white cells @ bottom) d/t vit A def -> metaplasia in conjunctiva
ocular path; cause
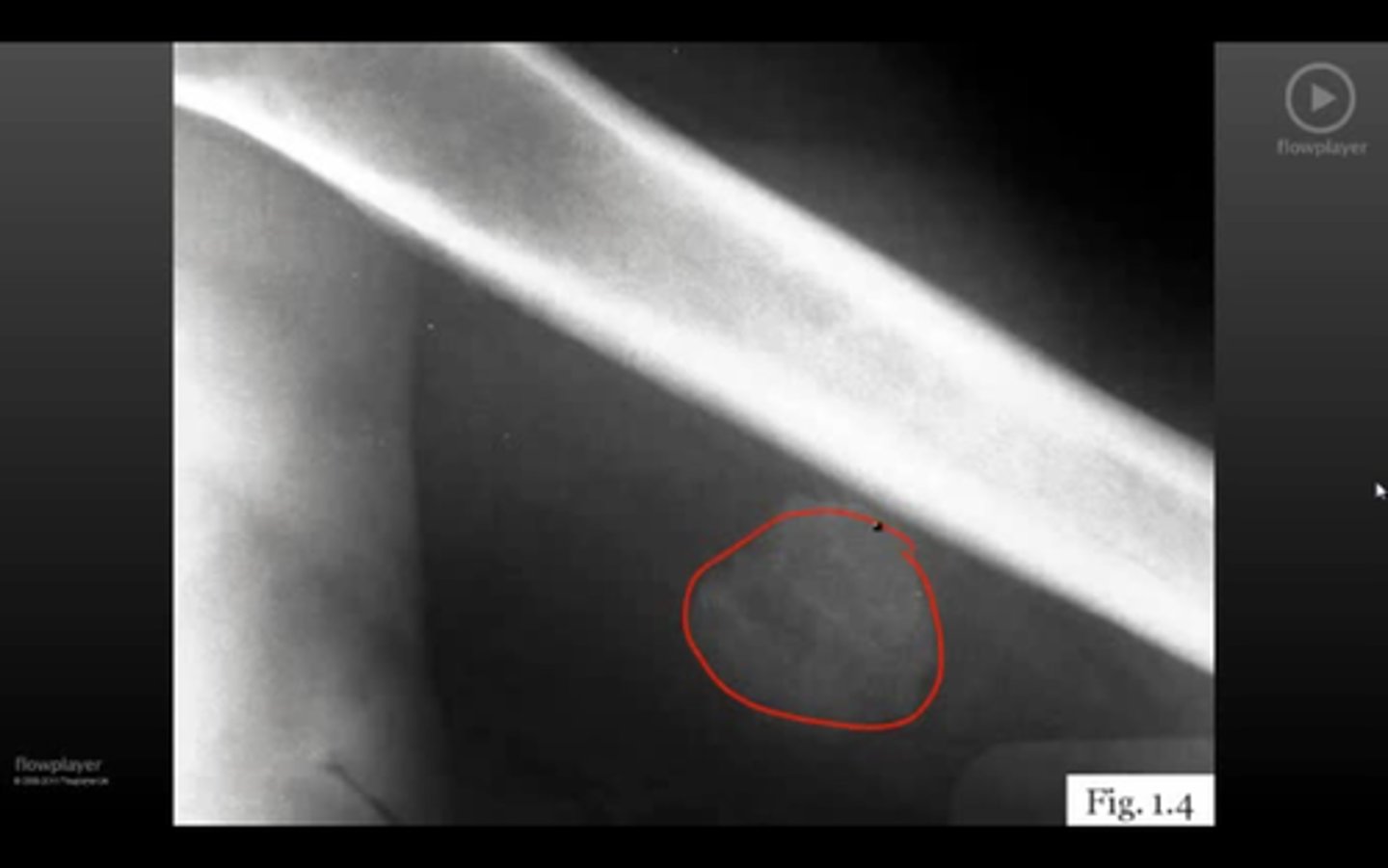
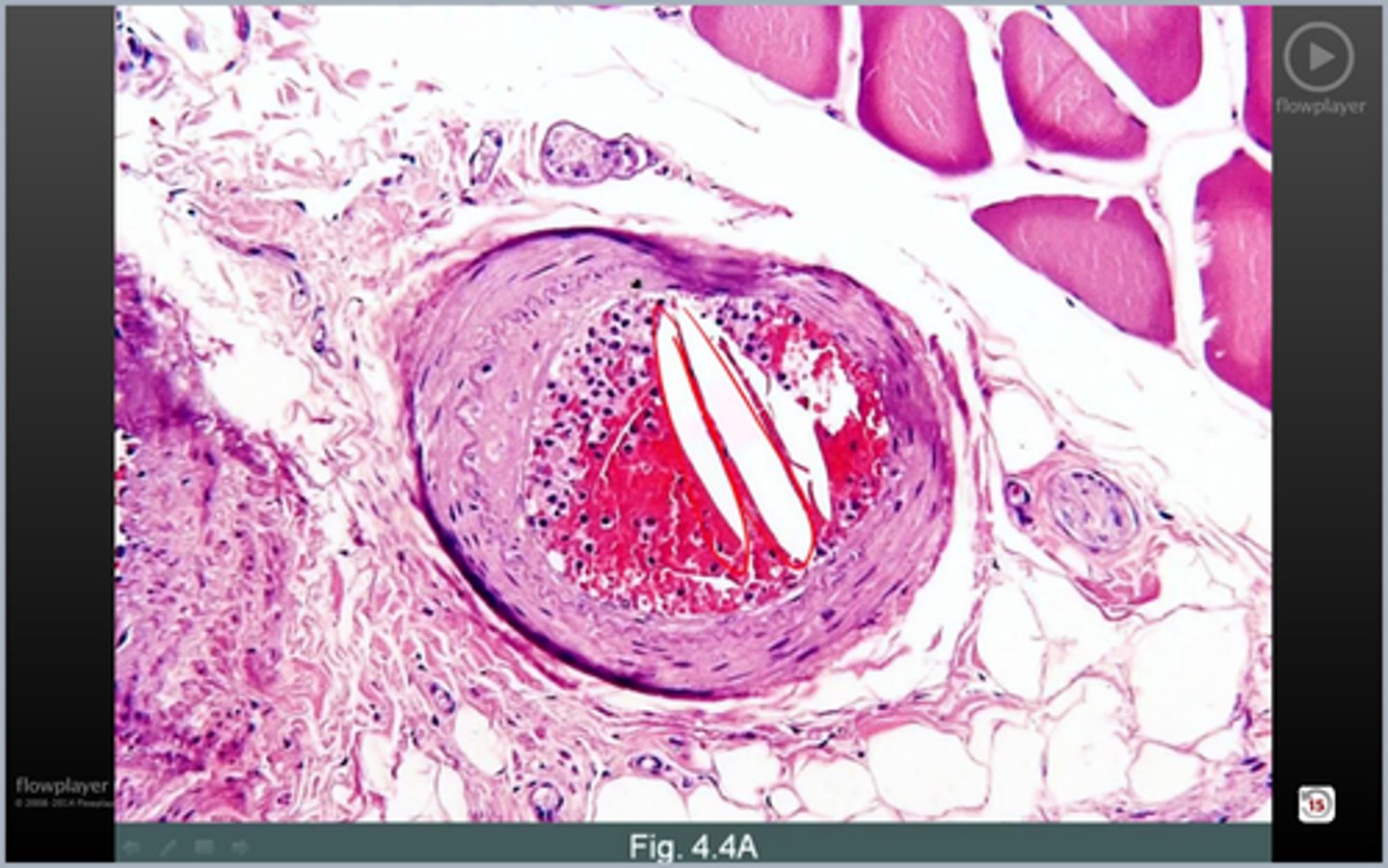
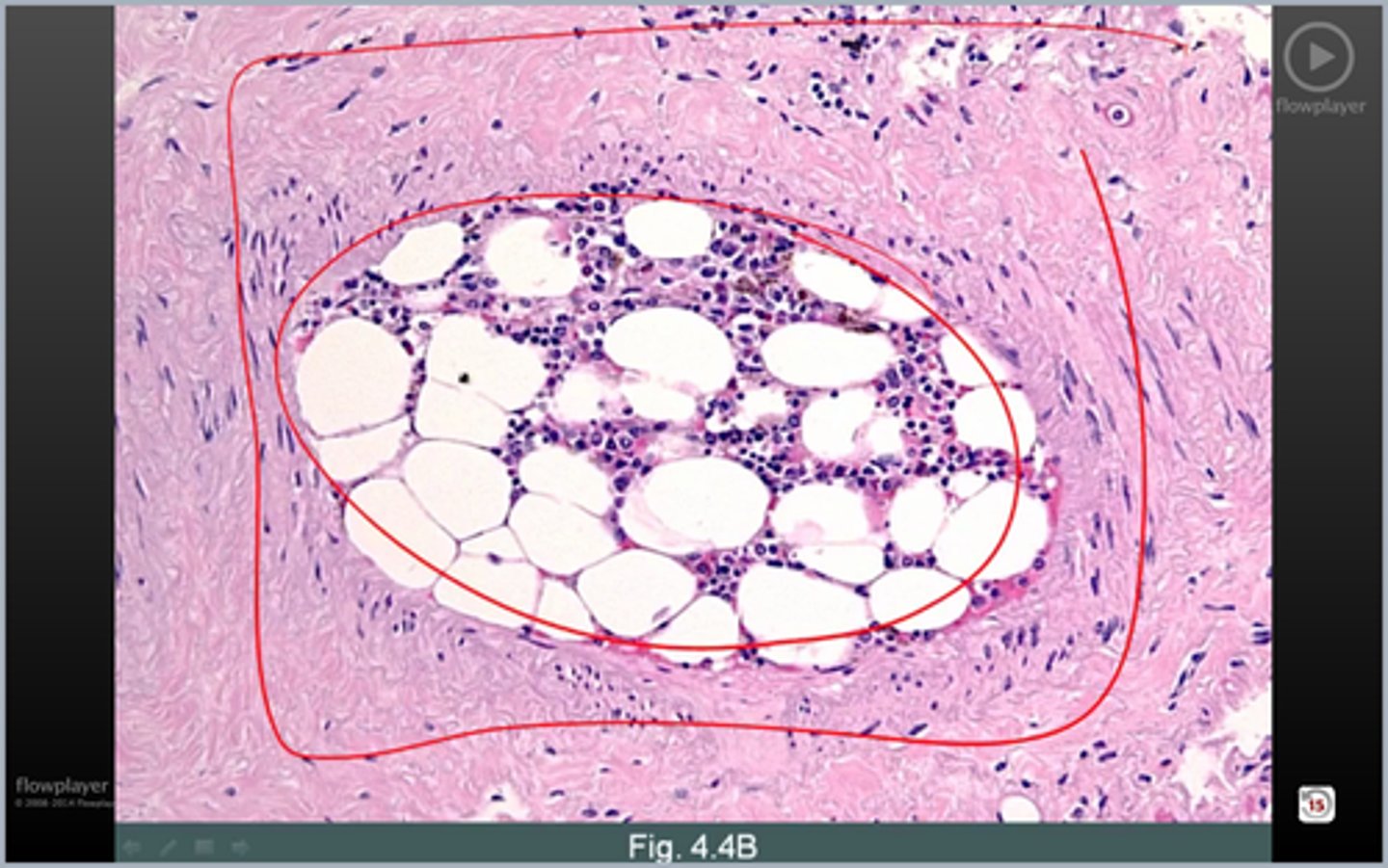
circle = bone in sk. mm. = myositis ossificans (portion of sk. mm. becomes bone d/t inflm via trauma)
confused for osteosarcoma but notice how adjacent bone is normal and is distinct from circular lesion so you know new bony mass is not growing off of long bone but rather sk. mm.
notice circle in sk. mm.
-confused for?
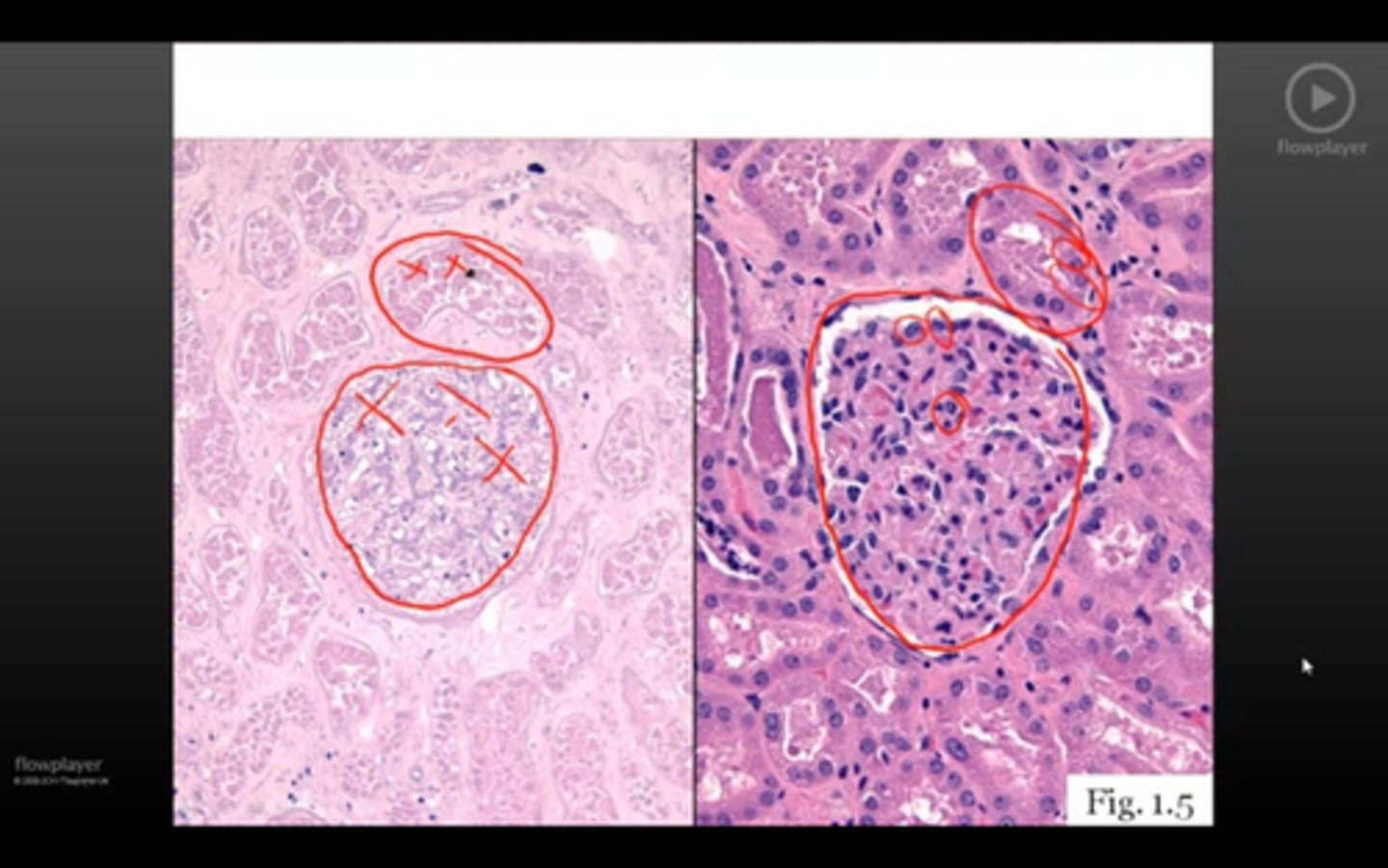
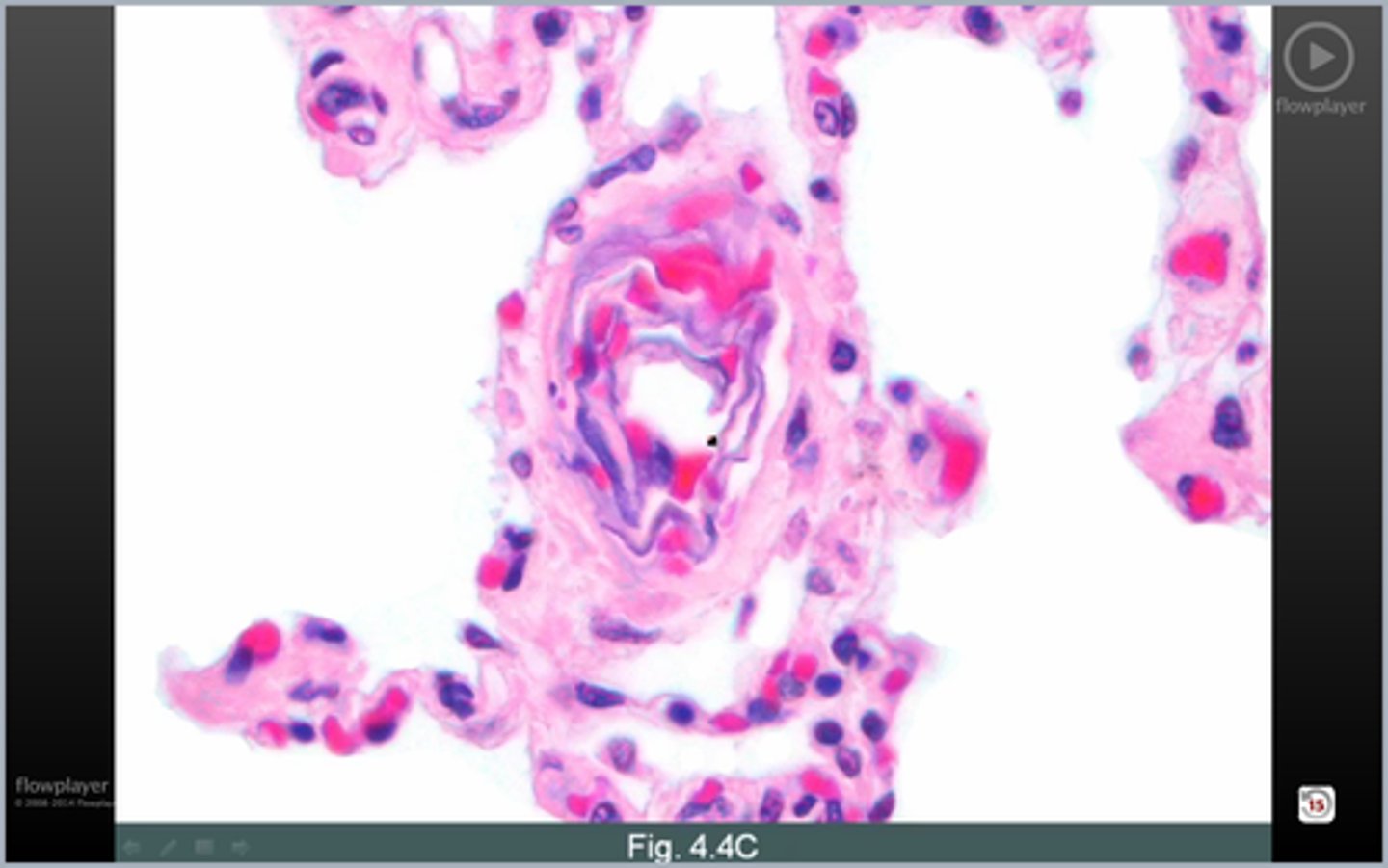
L = coagulative necrosis of kidney glomeruli
notice on R you see blue nuc, but not on L; also gen shape of L histo is preserved even w/o nuc d/t coag of cellular proteins
necrosis type
pale, wedge shaped infarct of kidney -> coag necrosis
ID what's seen; indicates what
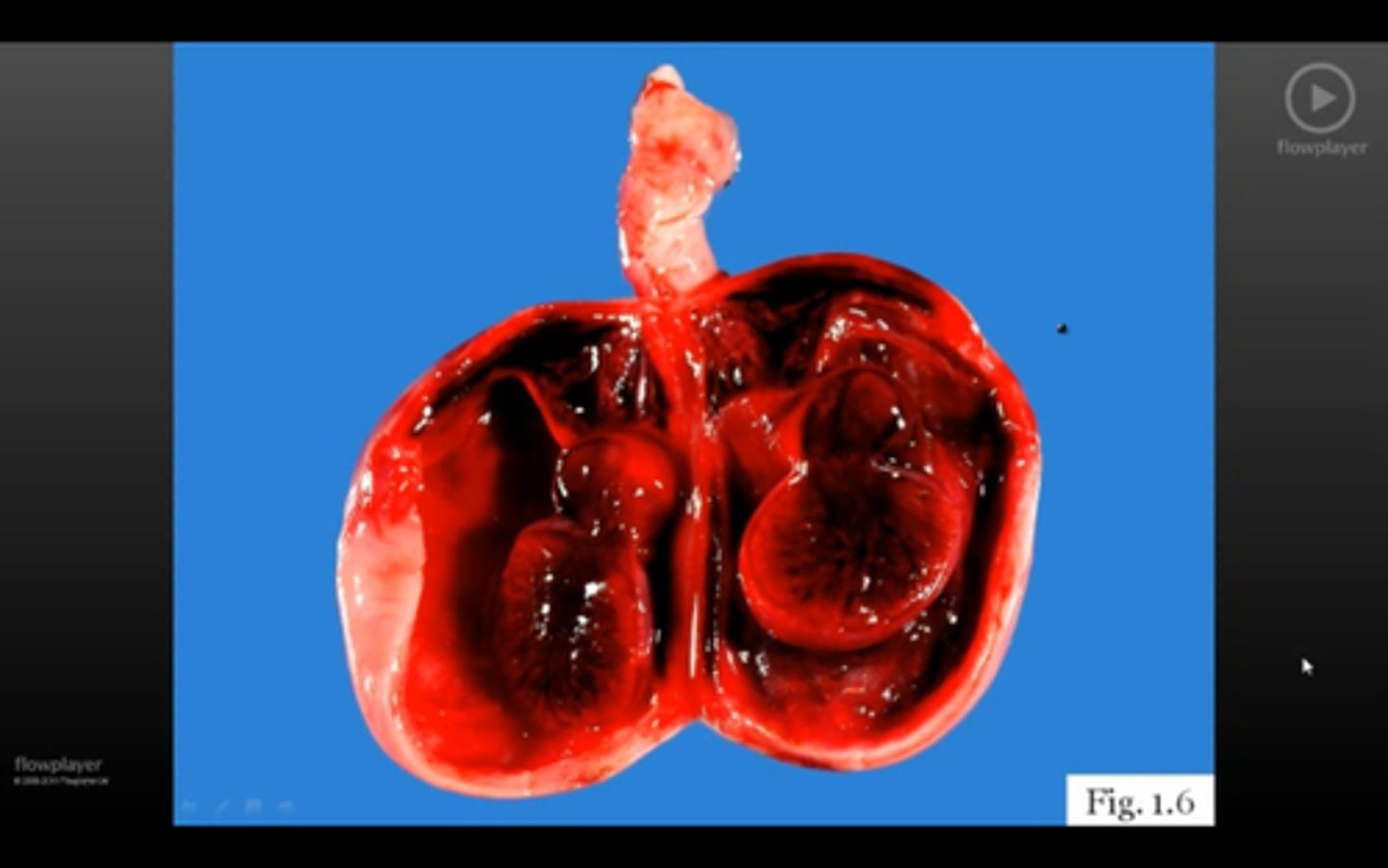
red (hmrg-ic) infarct of testicle
-d/t re-perfusion & fact tissue is loosely org (allows tissue to hold re-entered blood)
-cause: spermatic cord houses thick walled a. and thin v. when cord twists, a. is ok d/t thick wall but v. ruptures easily and the blood from their (that was supposed to exits) instead spills into scrotum
ID again; d/t what 2 things; cause
gangrenous necrosis of L/E in DM Pt.
ID gross path

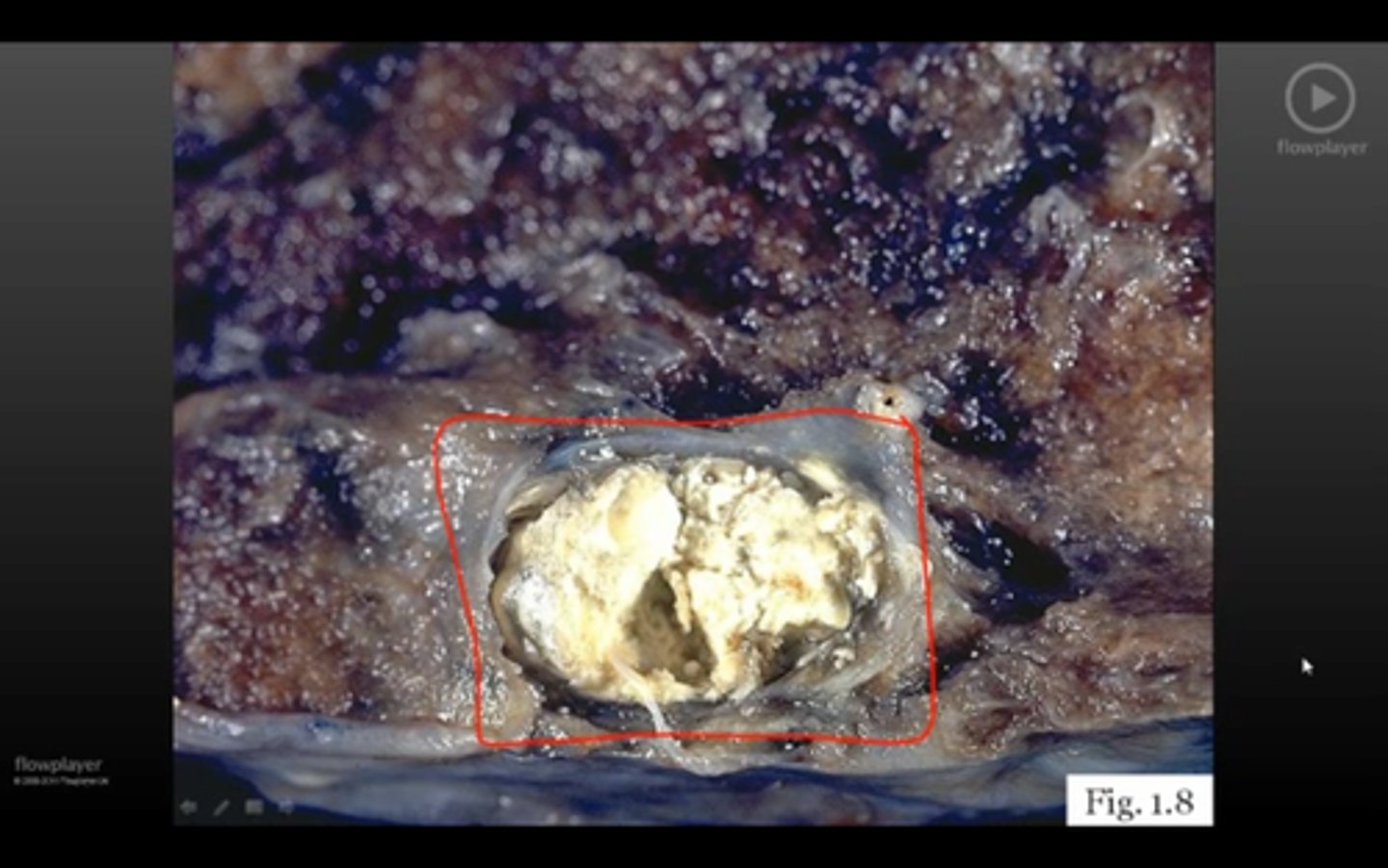
caseous necrosis (notice white, cottage cheese-like appearance) d/t Tb
ID gross path again
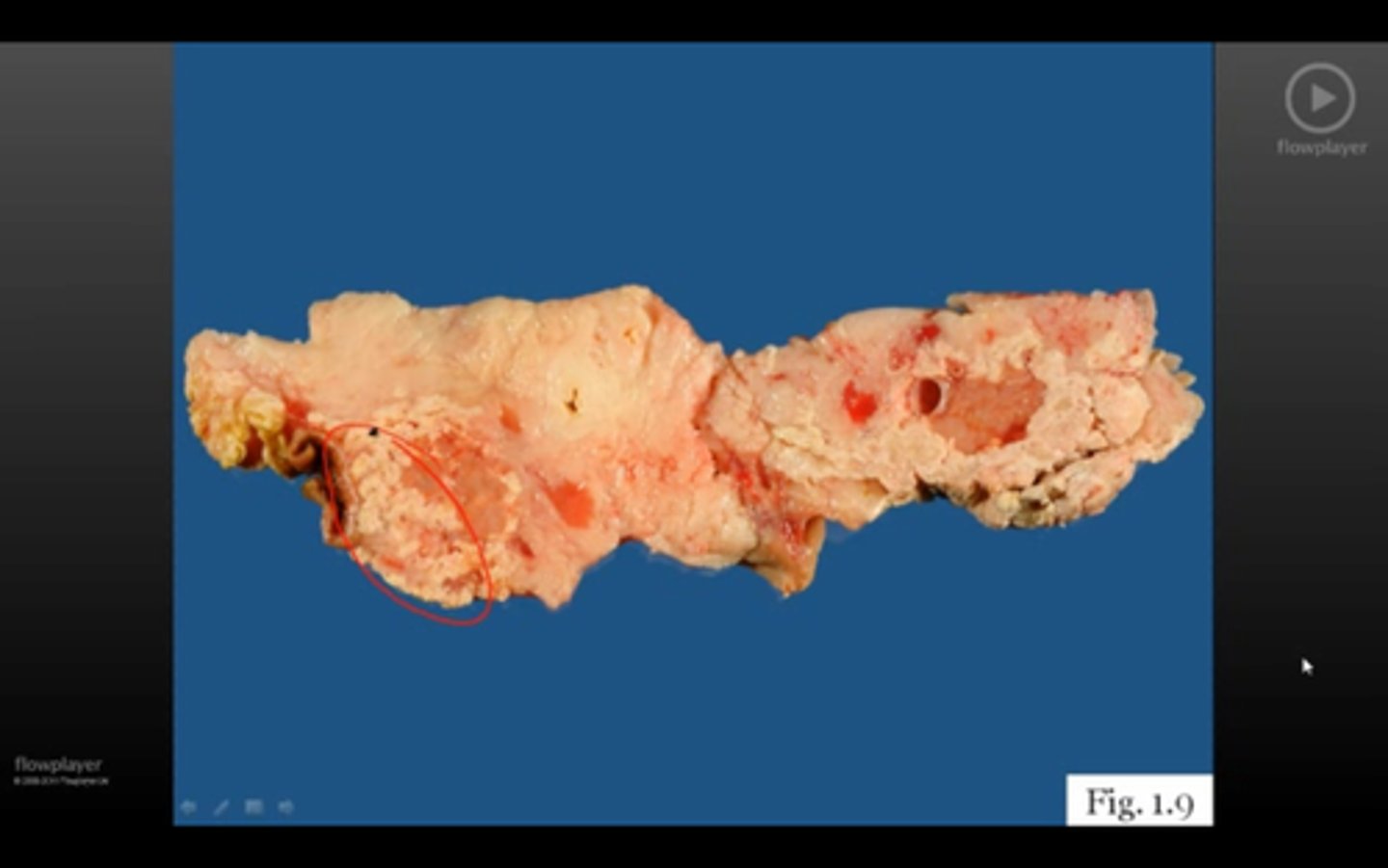
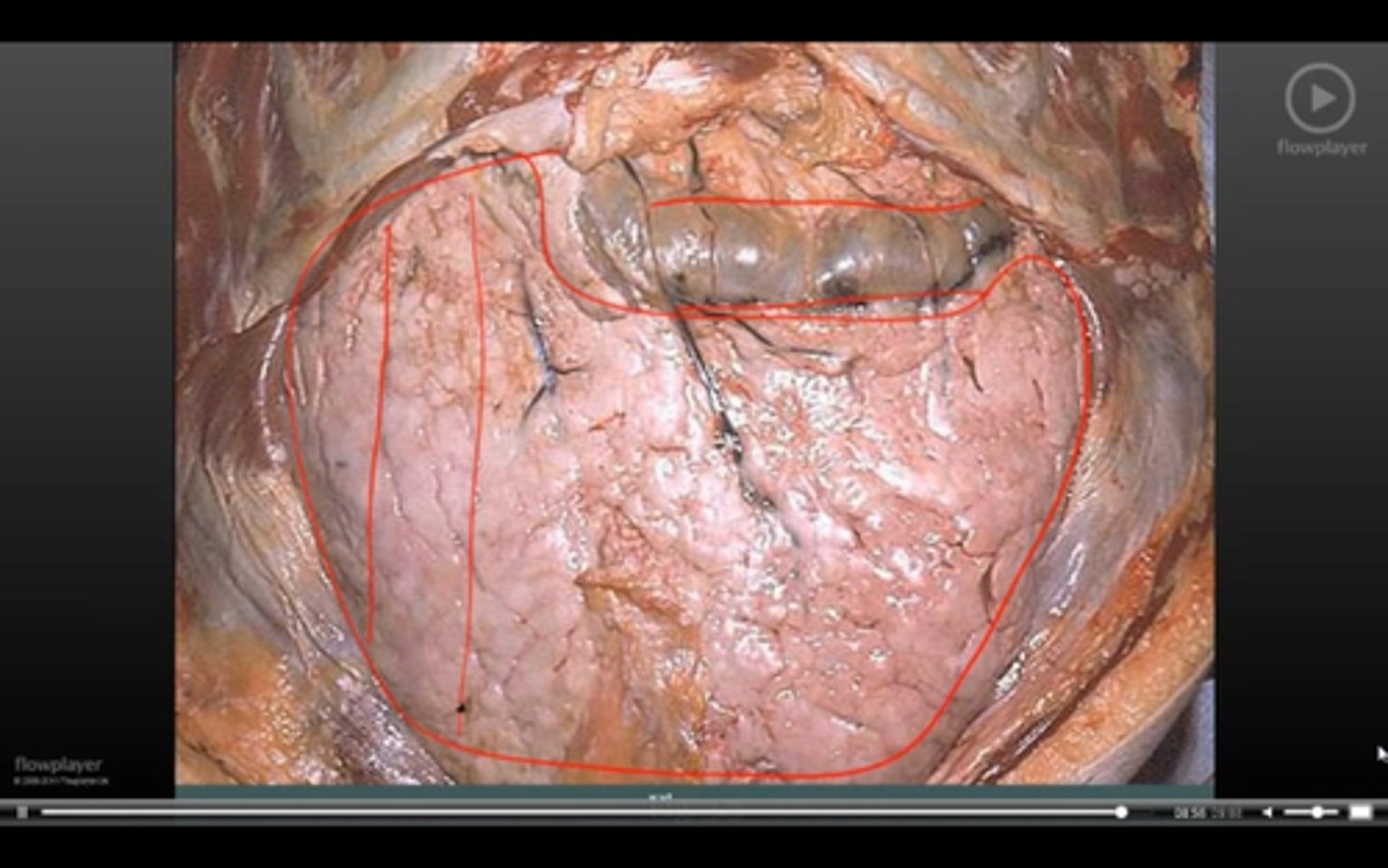
white chalky deposits encircled = peri-pancreatic fat that's undergone fatty necrosis via saponification (deposition of Ca++, which gives it chalky white look)
ID gross path again1
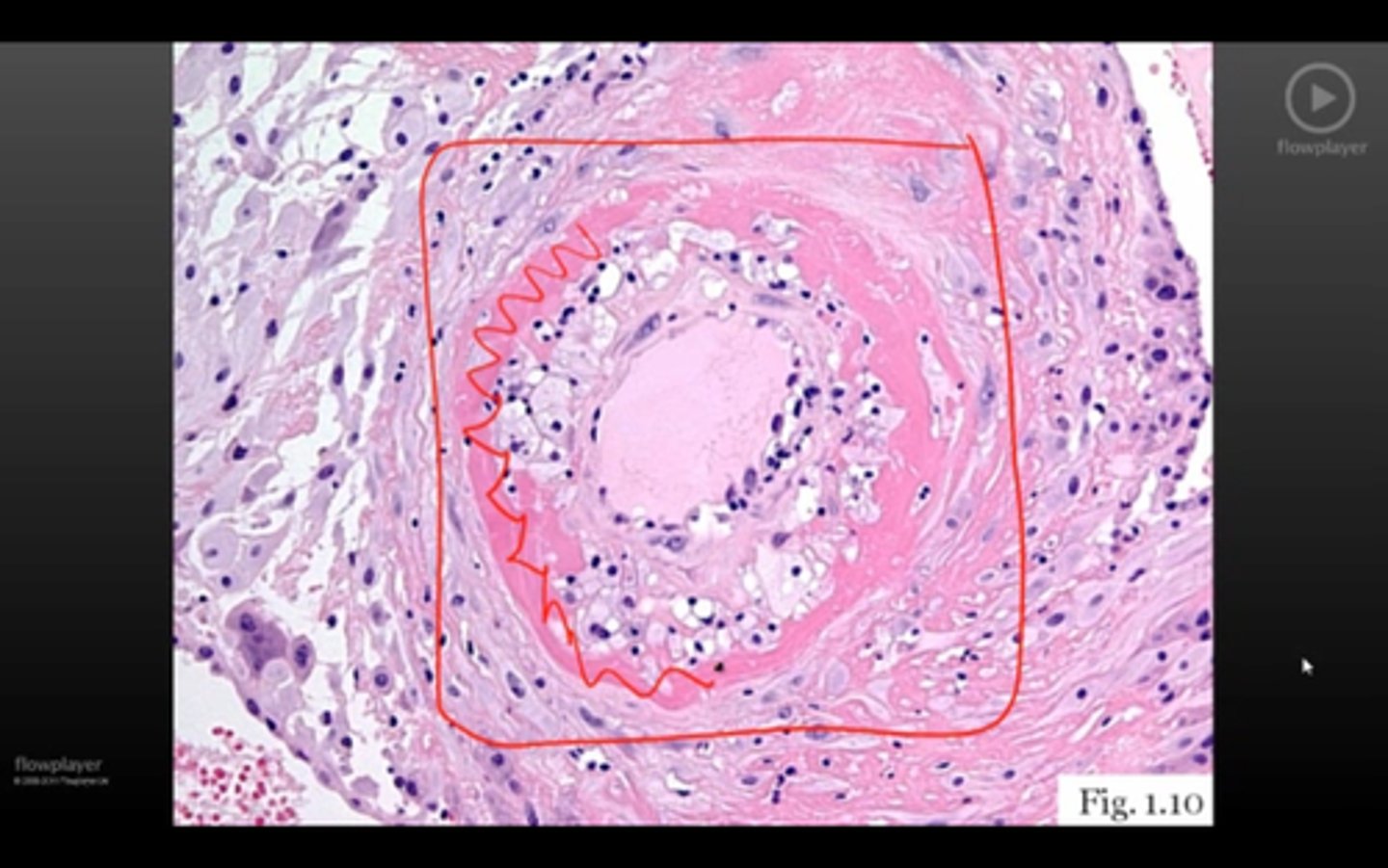
bright pink stain in wall of blood vessel = fibrinoid necrosis
notice pink stain
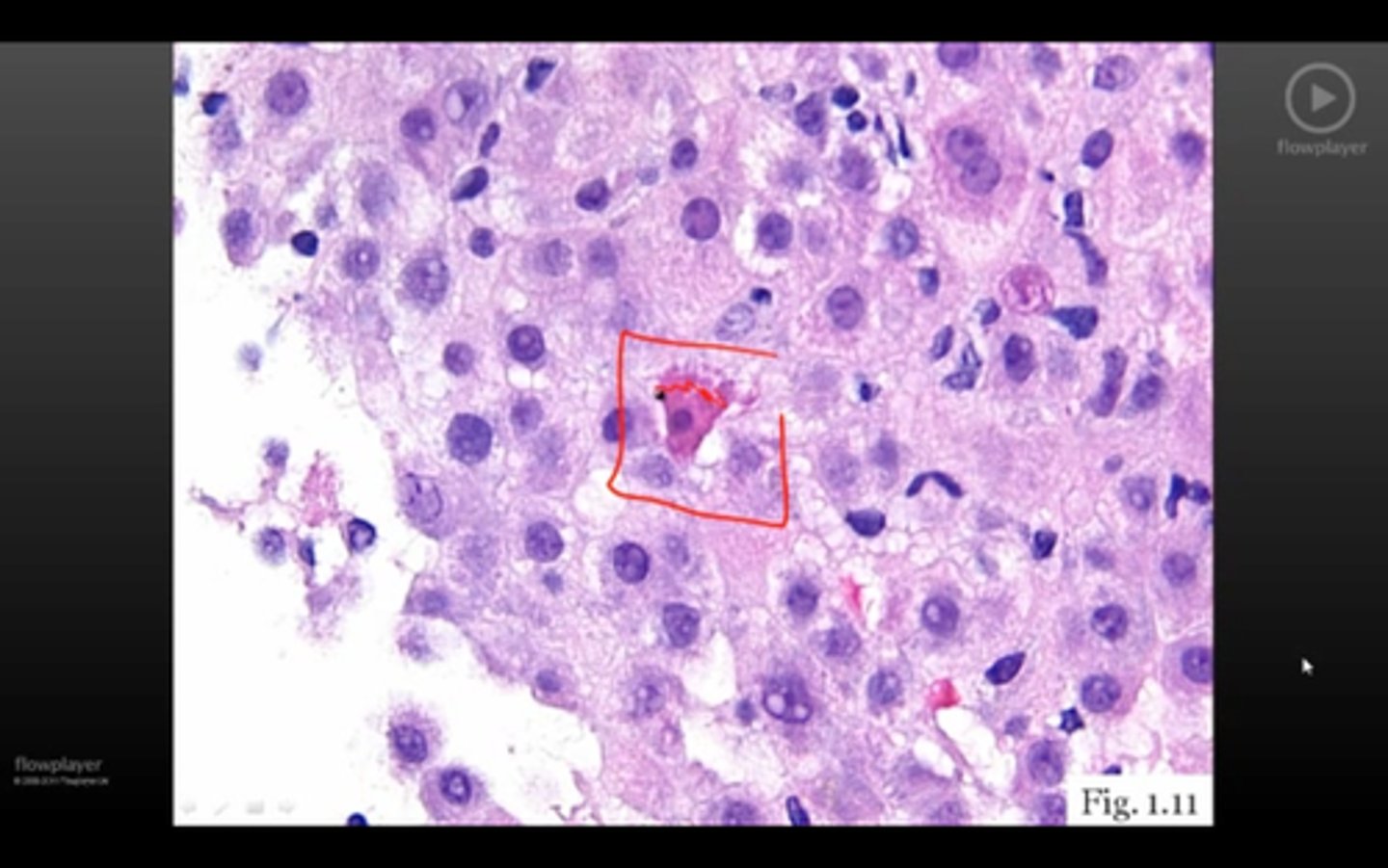
apoptotic body (pink Eos cytoplasm (bc it's getting concentrated as cell shrinks) & nuc is smaller)
what's the cell
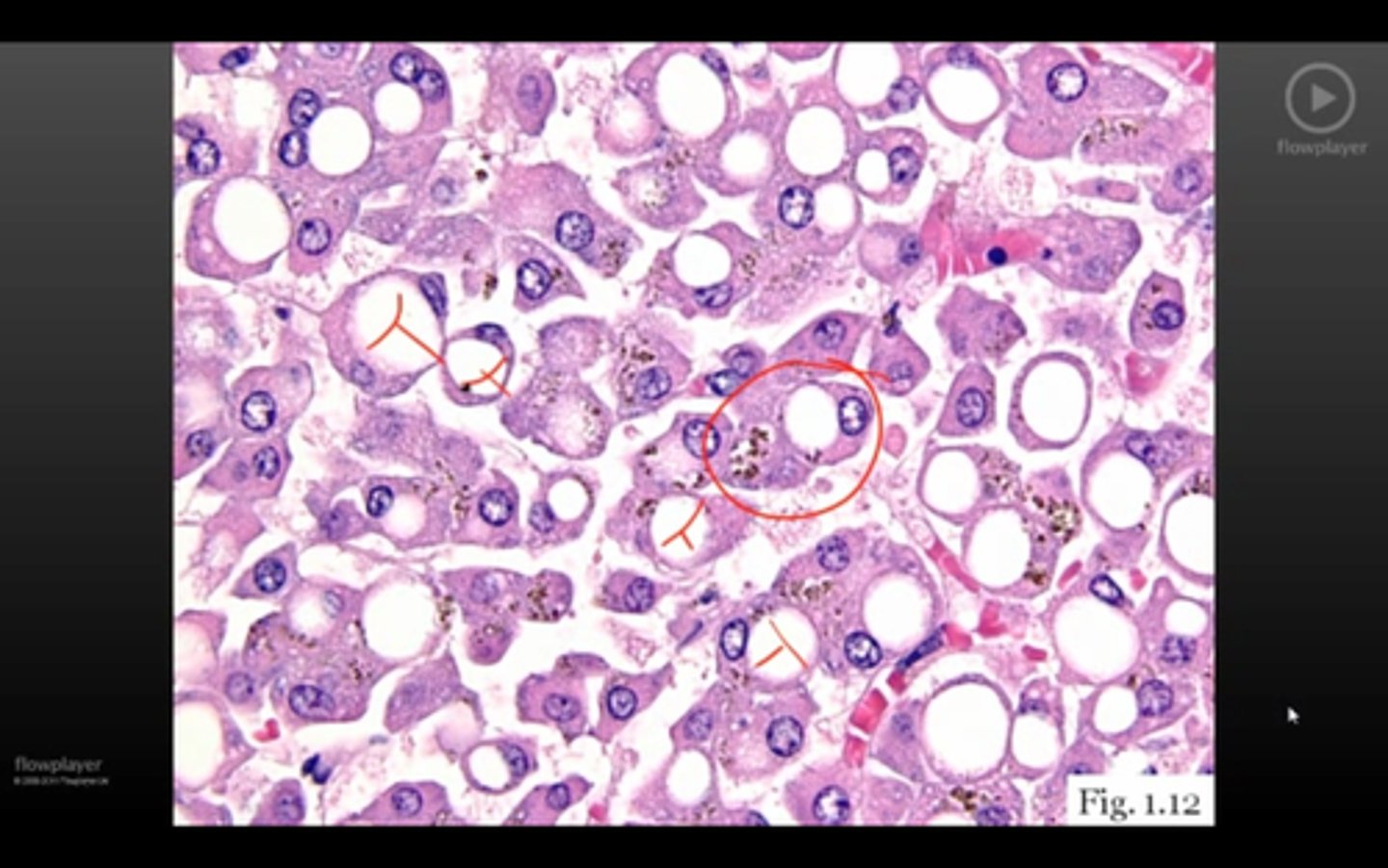
circled = hepatocytes
big white cells = adipocytes d/t fatty change in liver
liver histo
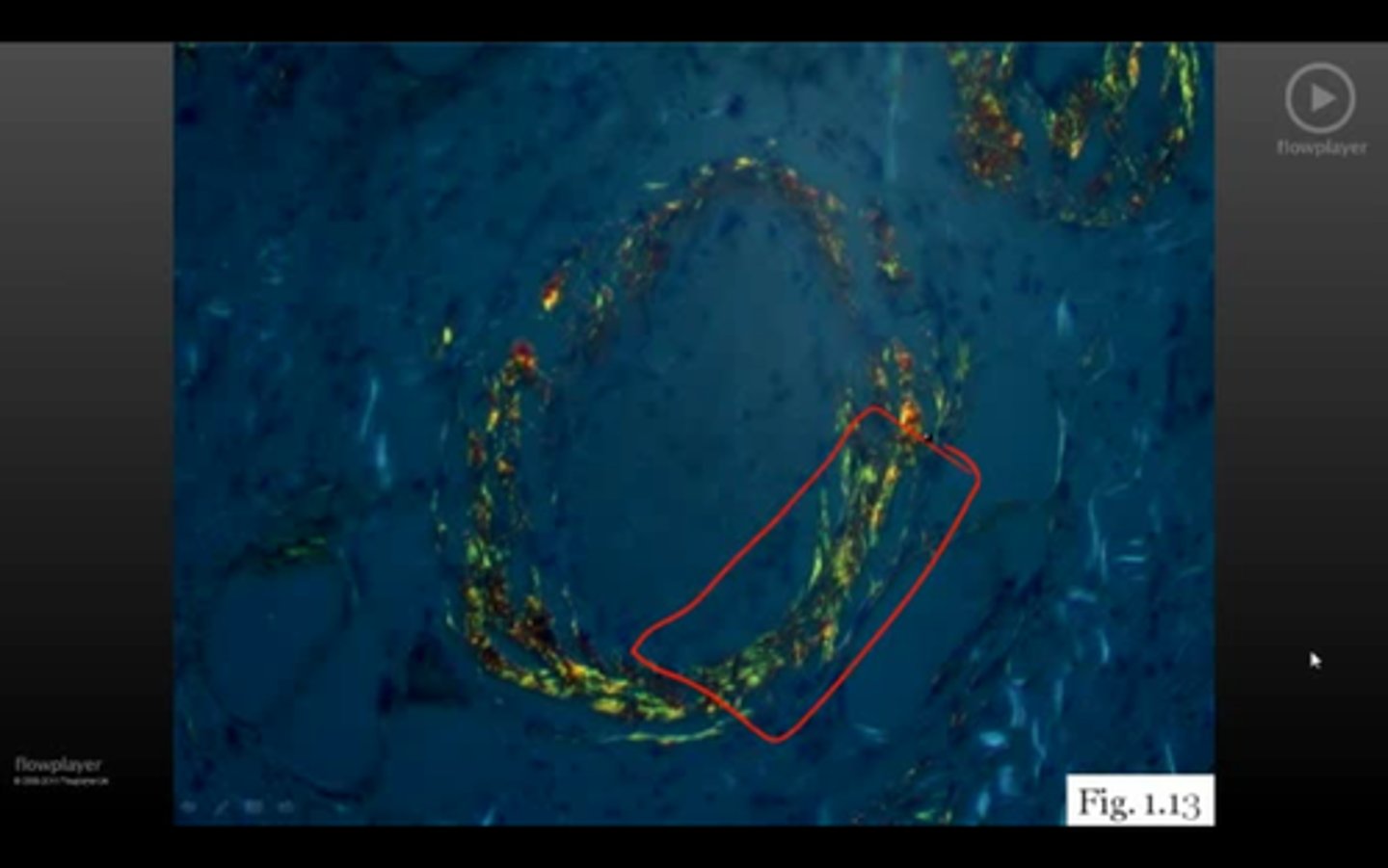
congo red stain identifying amyloid deposition around blood vessel in extra-cellular space (small red dot in middle of box)
-Alz
identify what's around blood vessel
-classic Dz
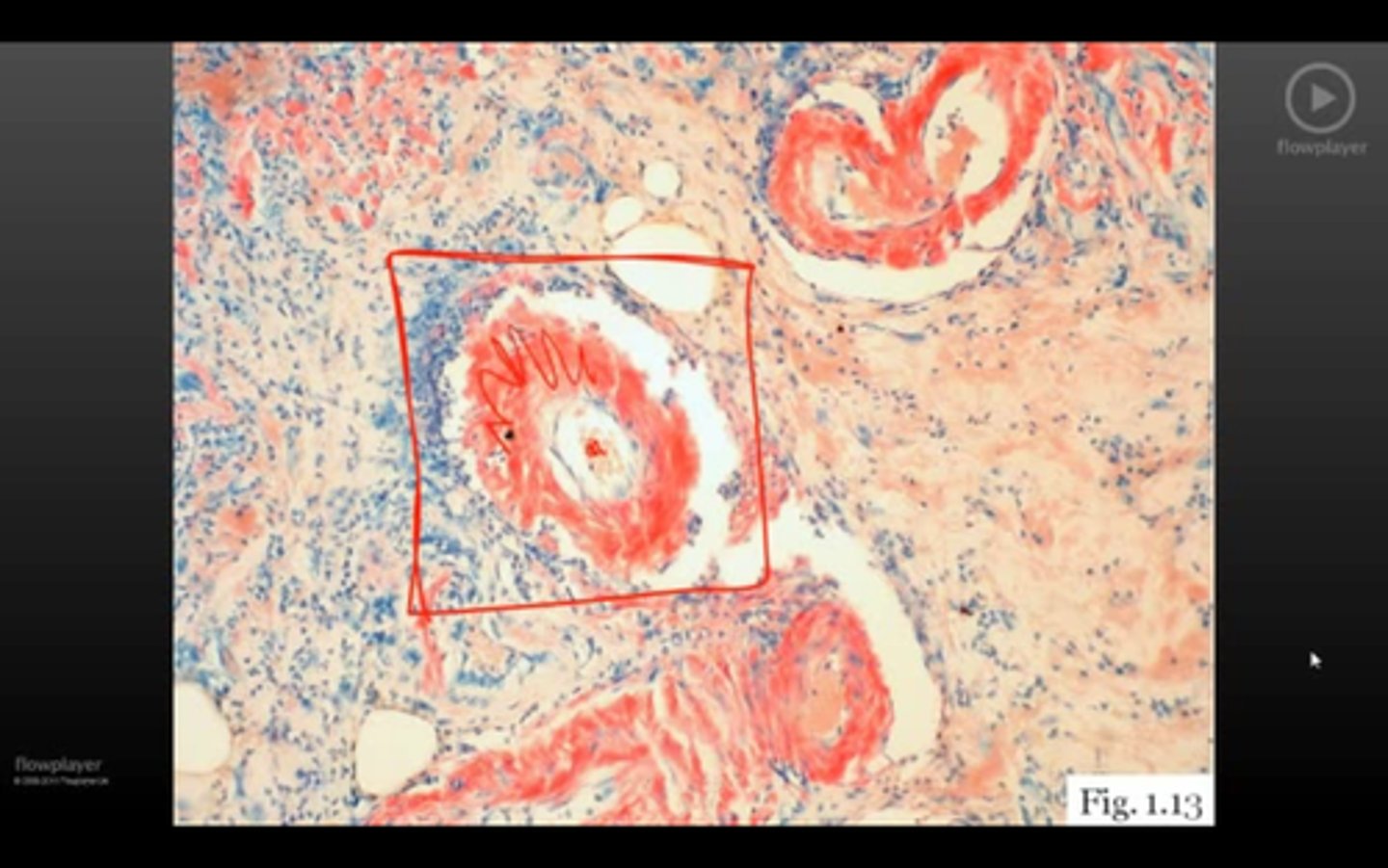
amyloid here has apple-green birefringence
same slide as before placed under polarized light showing what
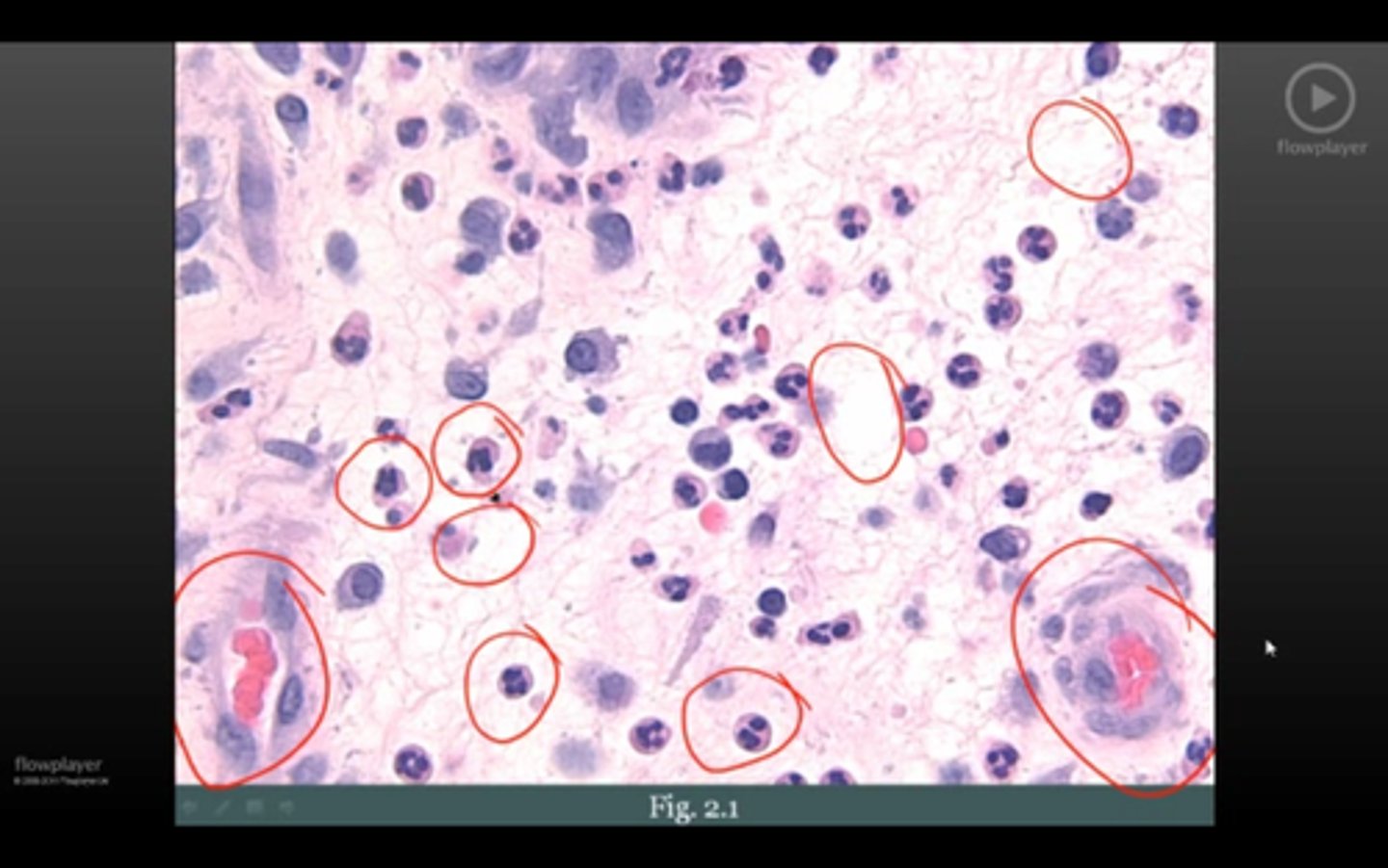
interstitial space during acute inflm
-bottom corner circles = vessels so you know we're outside of them
-smaller circles above = PMN's
-empty circles = fluid building up in tissue = edema
what are we seeing here
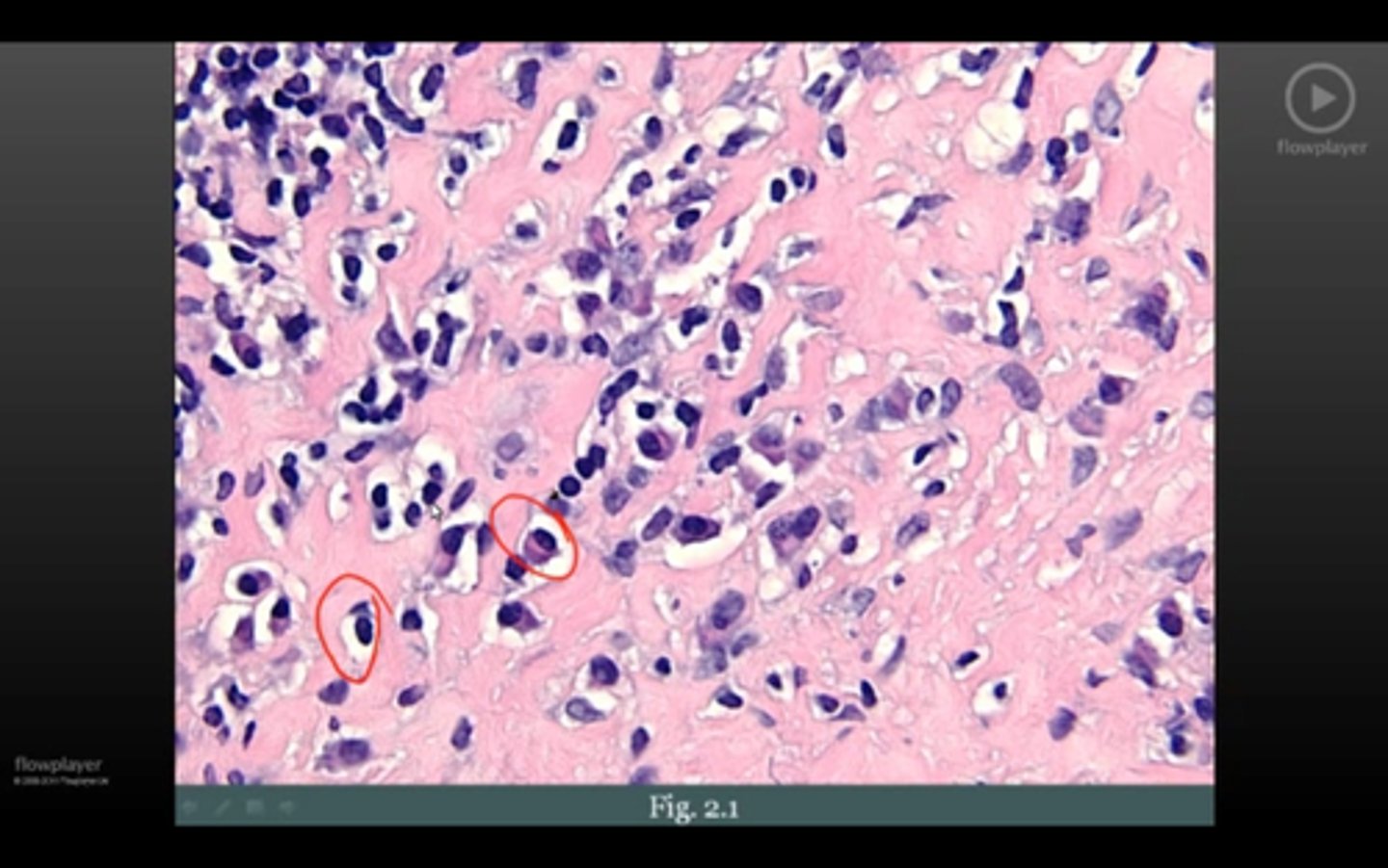
chronic inflm
L - lymphocyte
R - plasma cell
what can you tell by presence of cells
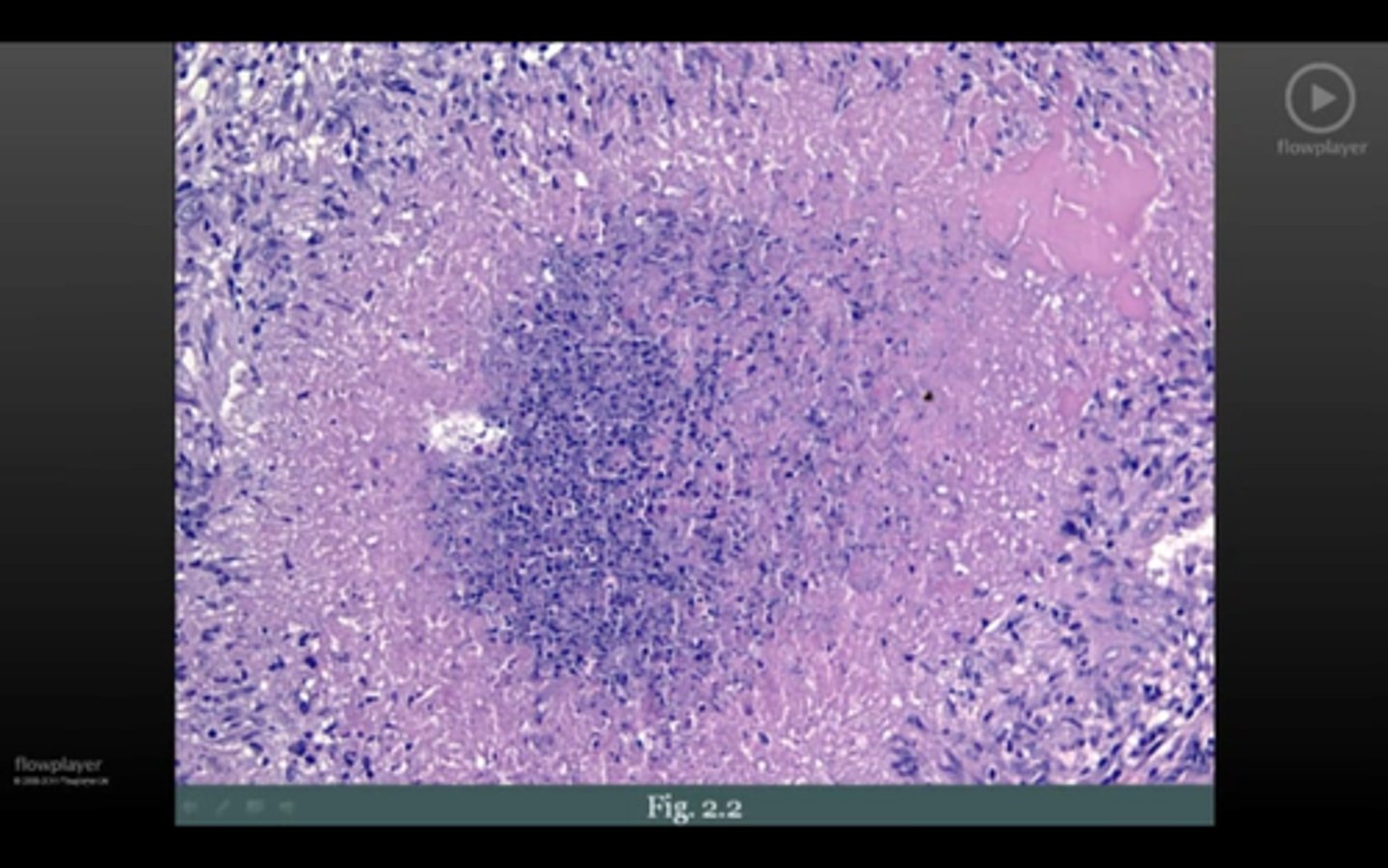
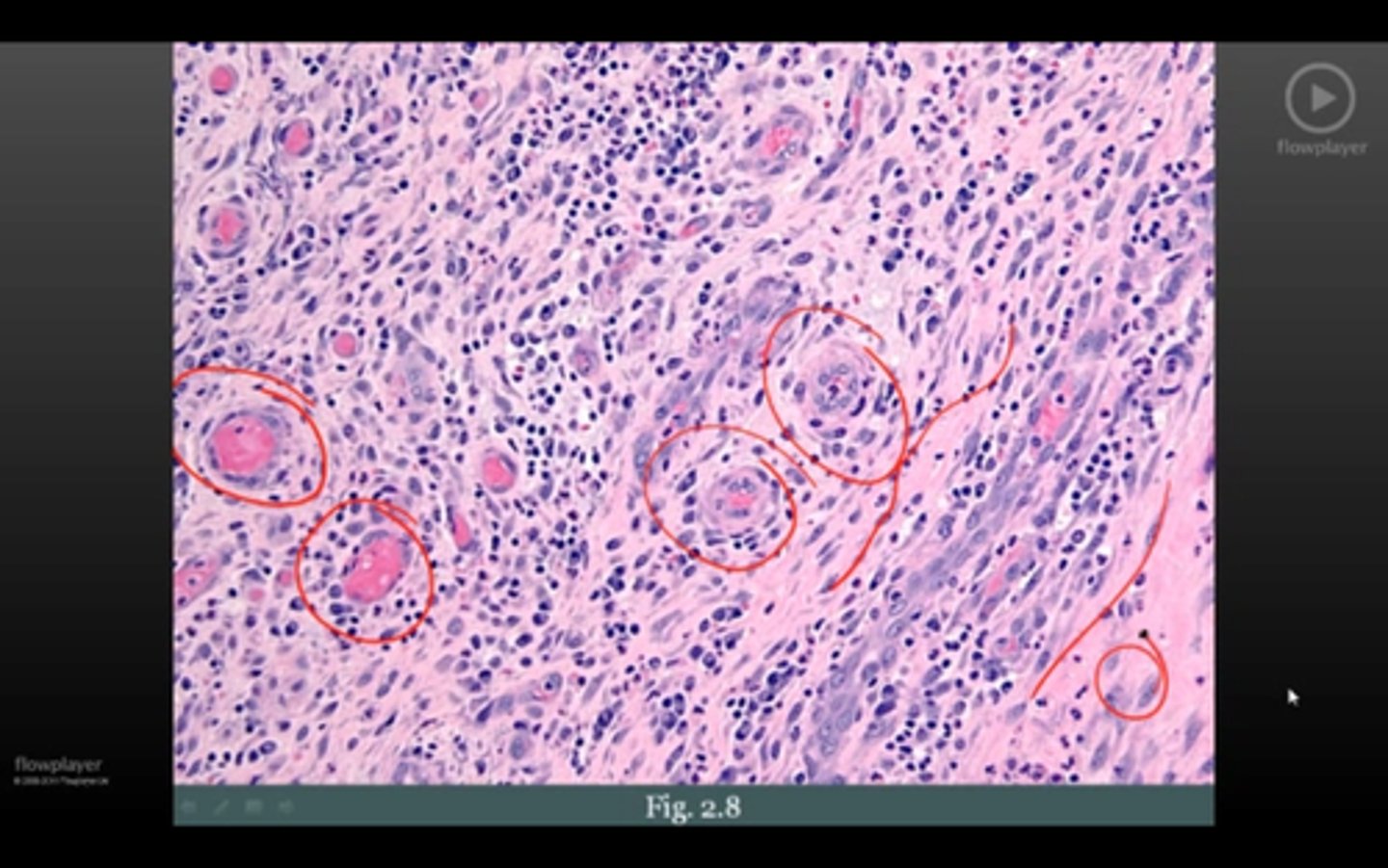
granuloma (notice rim of lymphocytes around epithelioid histiocytes); it's non-caseating bc each of the histiocytes (small circles) has their nuc present so it's not yet necrotic like caseating
what is this? how can u tell?
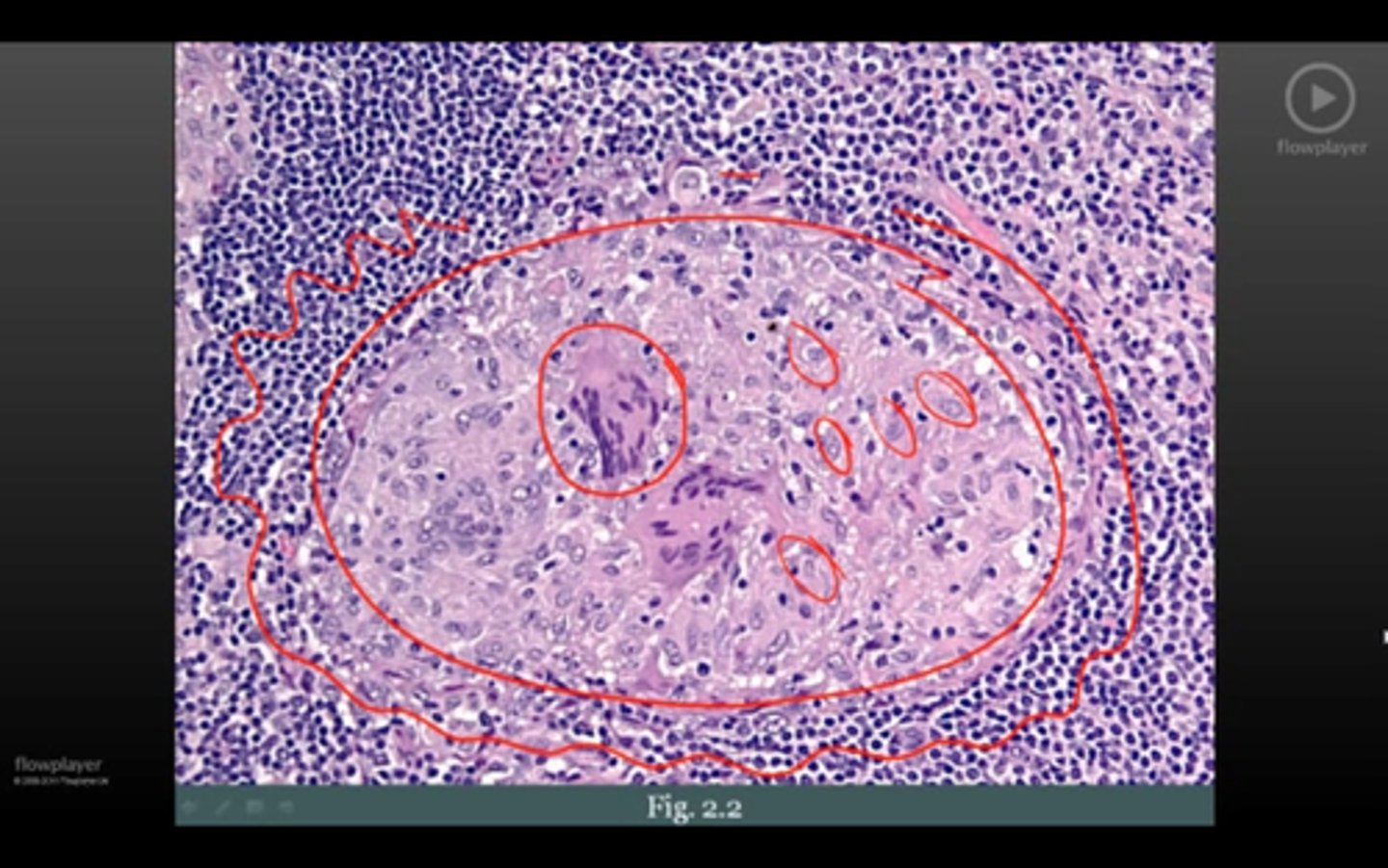
notice how in center there's necrosis & cell death. that makes it caseating granuloma
how is this diff from prev one
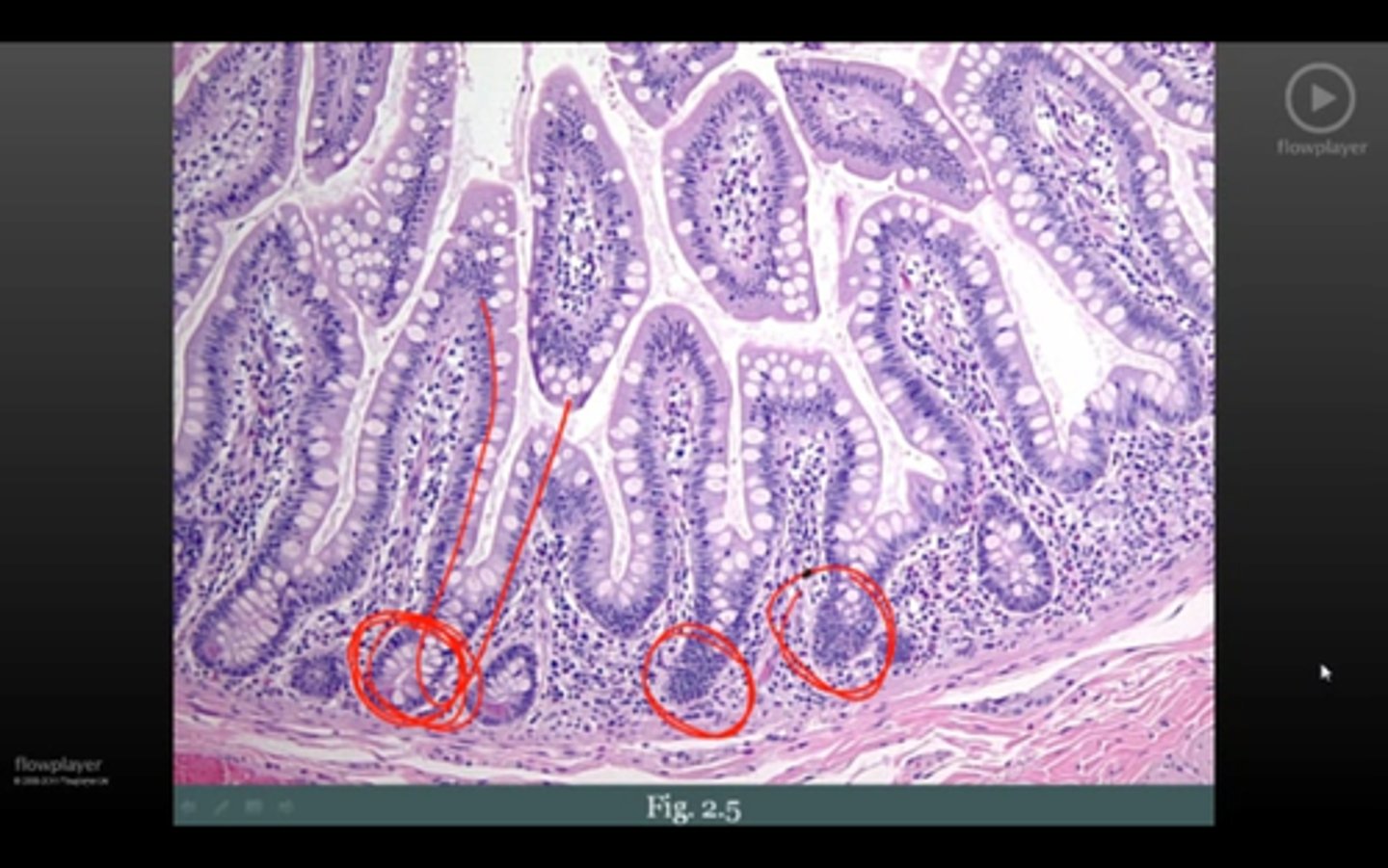
mucosal bowel crypts;
at base of crypts are gut stem cells
ID circles at bottom; contain what
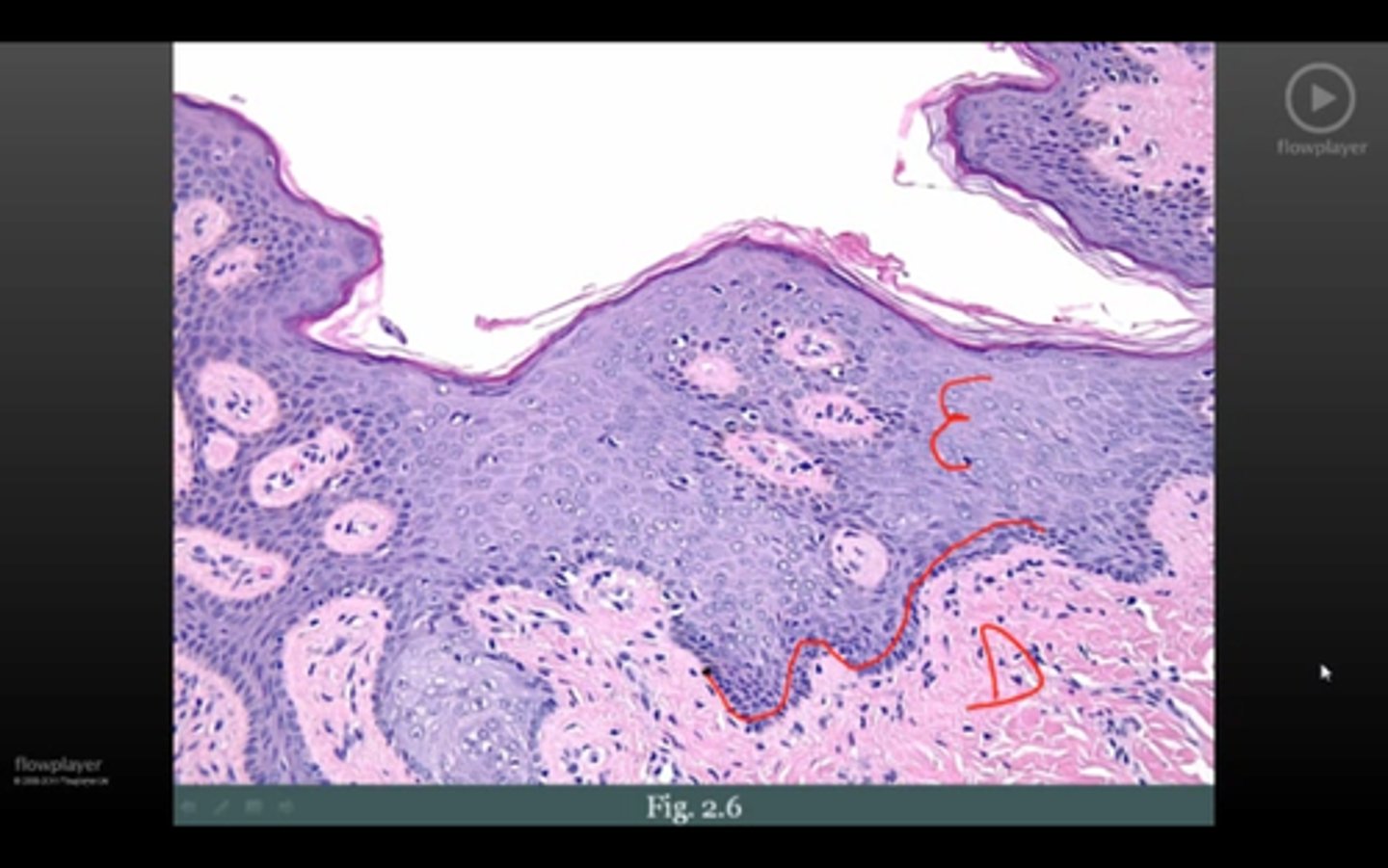
E = epidermis, D = dermis
squiggly line = basal layer of dermis that houses SC's
what is this
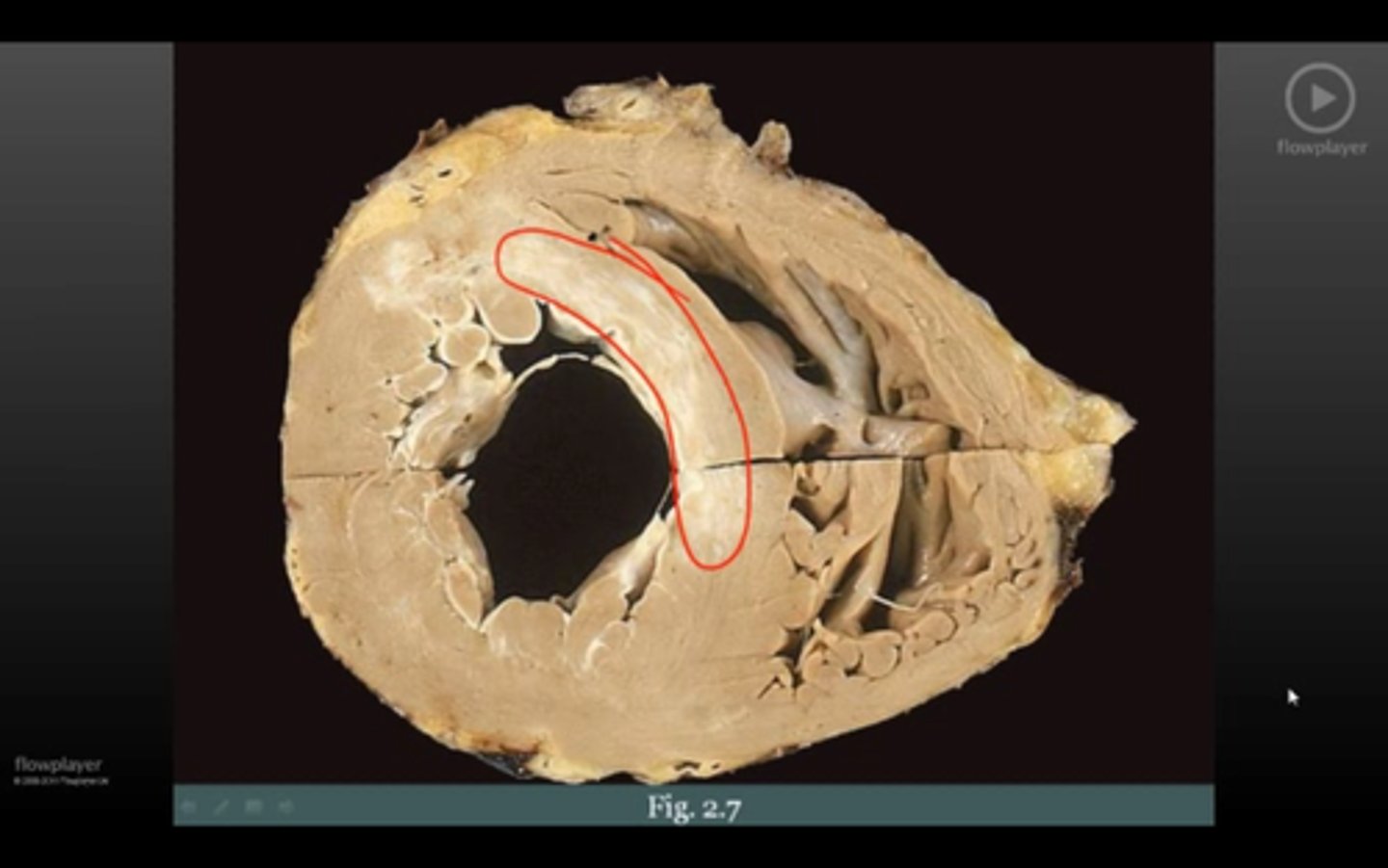
white scar indicates previous MI
-rmr myocardium is a permanent tissue w/ no regen capacity
what we lookin at doe
-why does this form
L circles = granulation tissue (during wound repair)
R circles = vessels (sprouting capillaries)
squiggly = deposition of collagen via fibroblasts
what this be
keloid
-earlobes of blacks
-T3 collagen
wtf are we looking at here; clin pres; made of

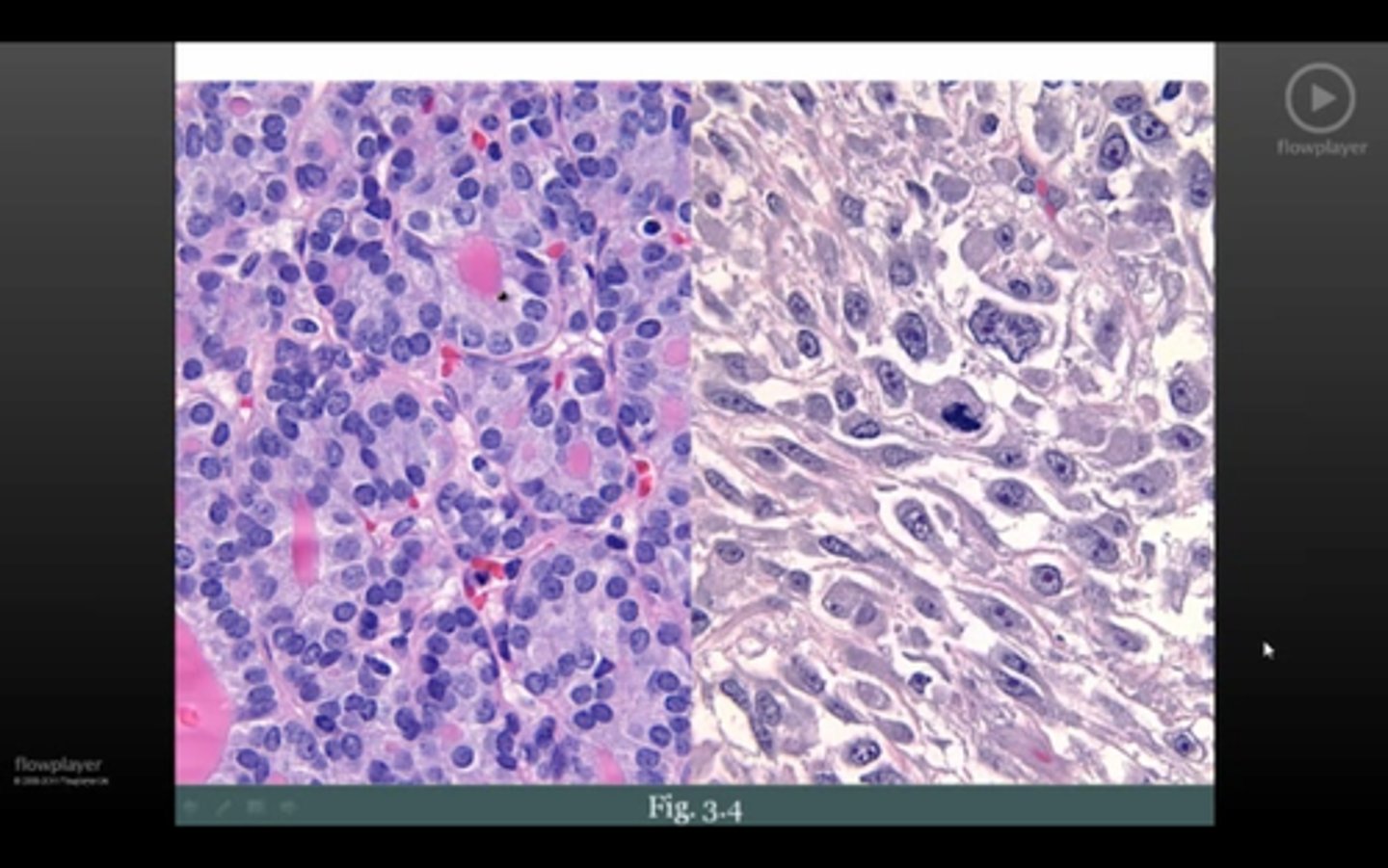
L = b9 adenoma of thyroid
R = mal ADCA (disorg growth, hi n:c ratio)
L vs R
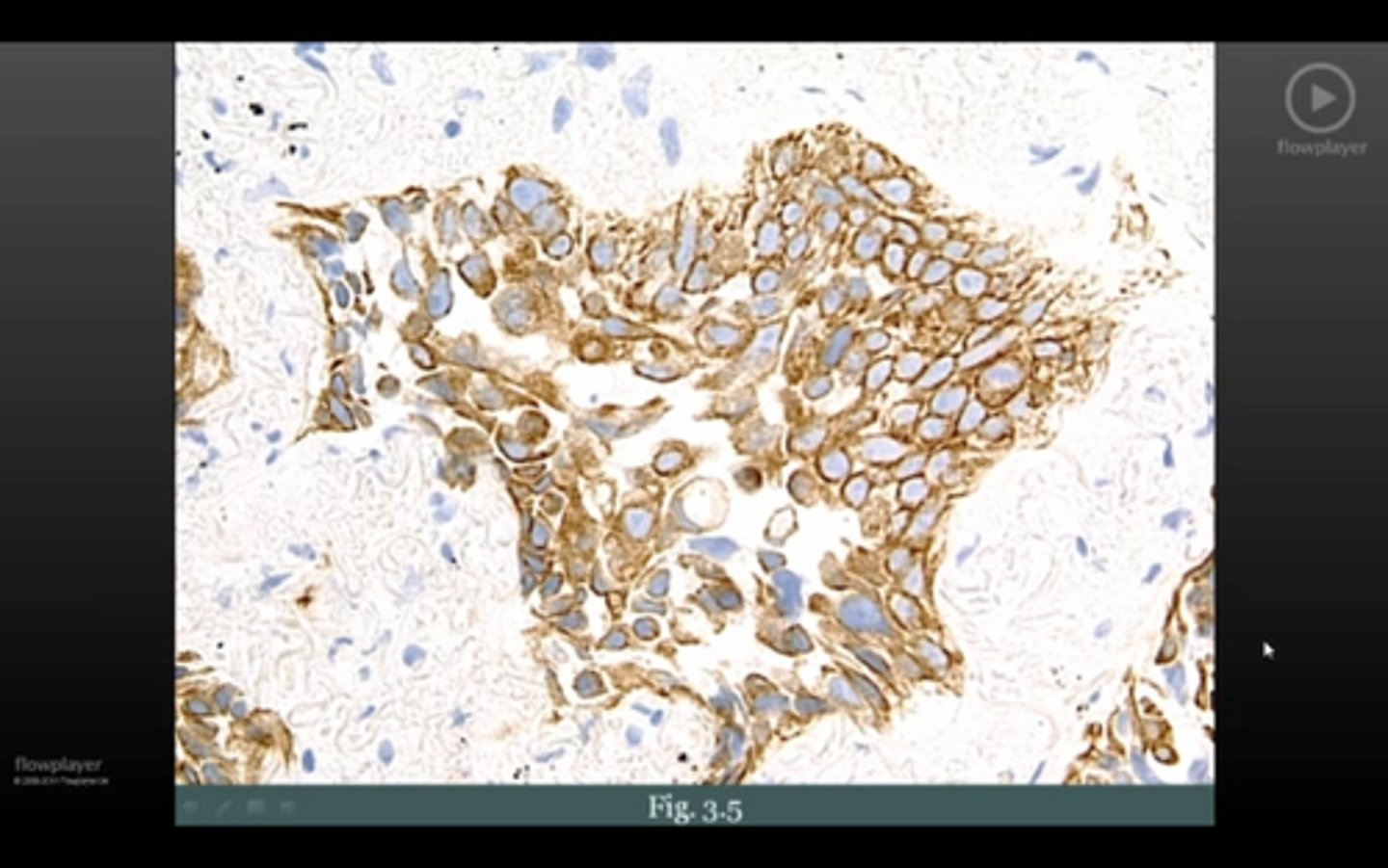
brown so think IHC stain
what stain is this
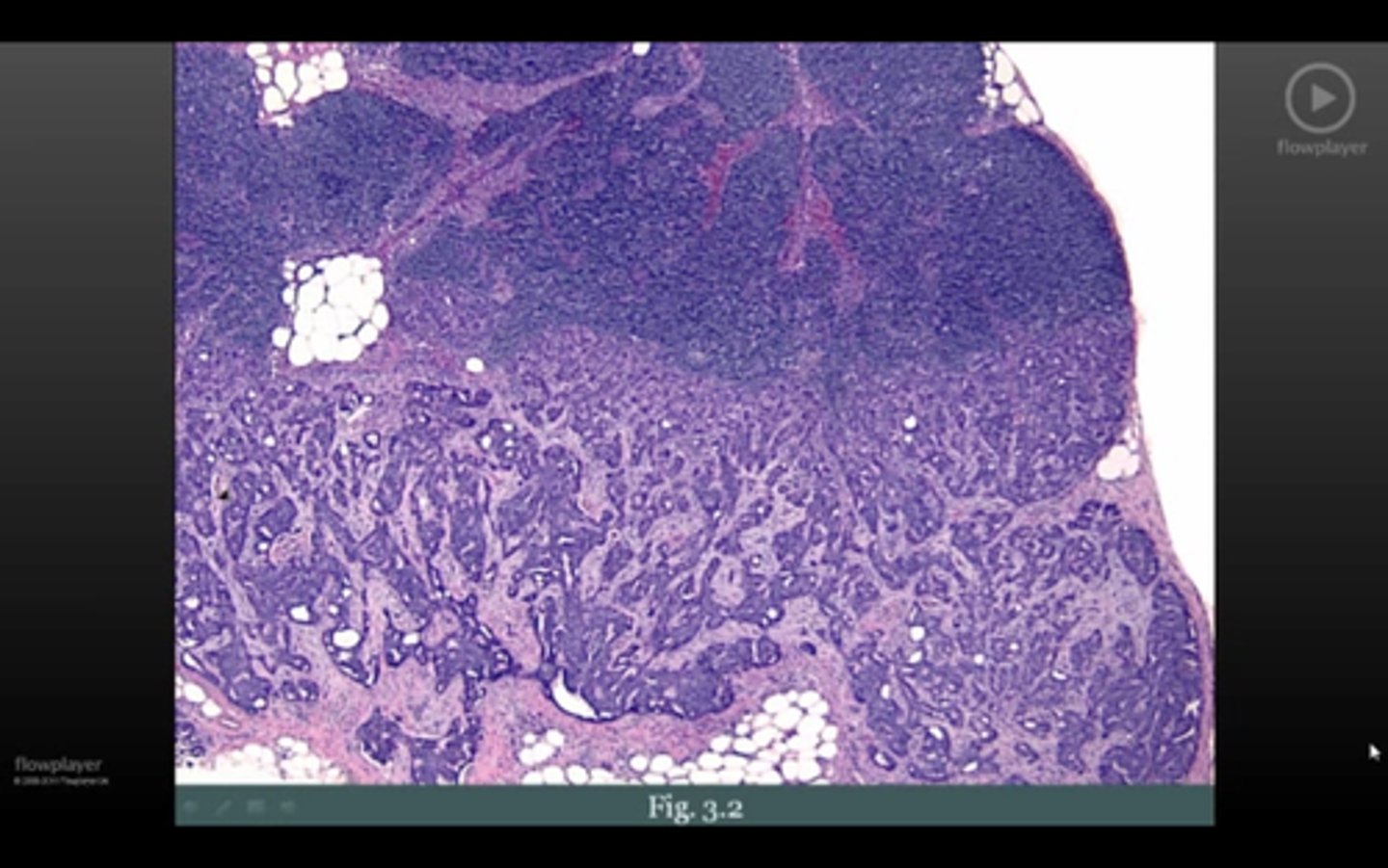
spread to axillary LN
top = normal tissue; bottom = tumor replacing LN
-white spaces @ bottom = glands = ADCA (rmr CA spread via LYMPHATICS)
BRCA in what tissue
ovarian CA spread to abdominal omentum via body seeding
-aka omental caking
wtf is this
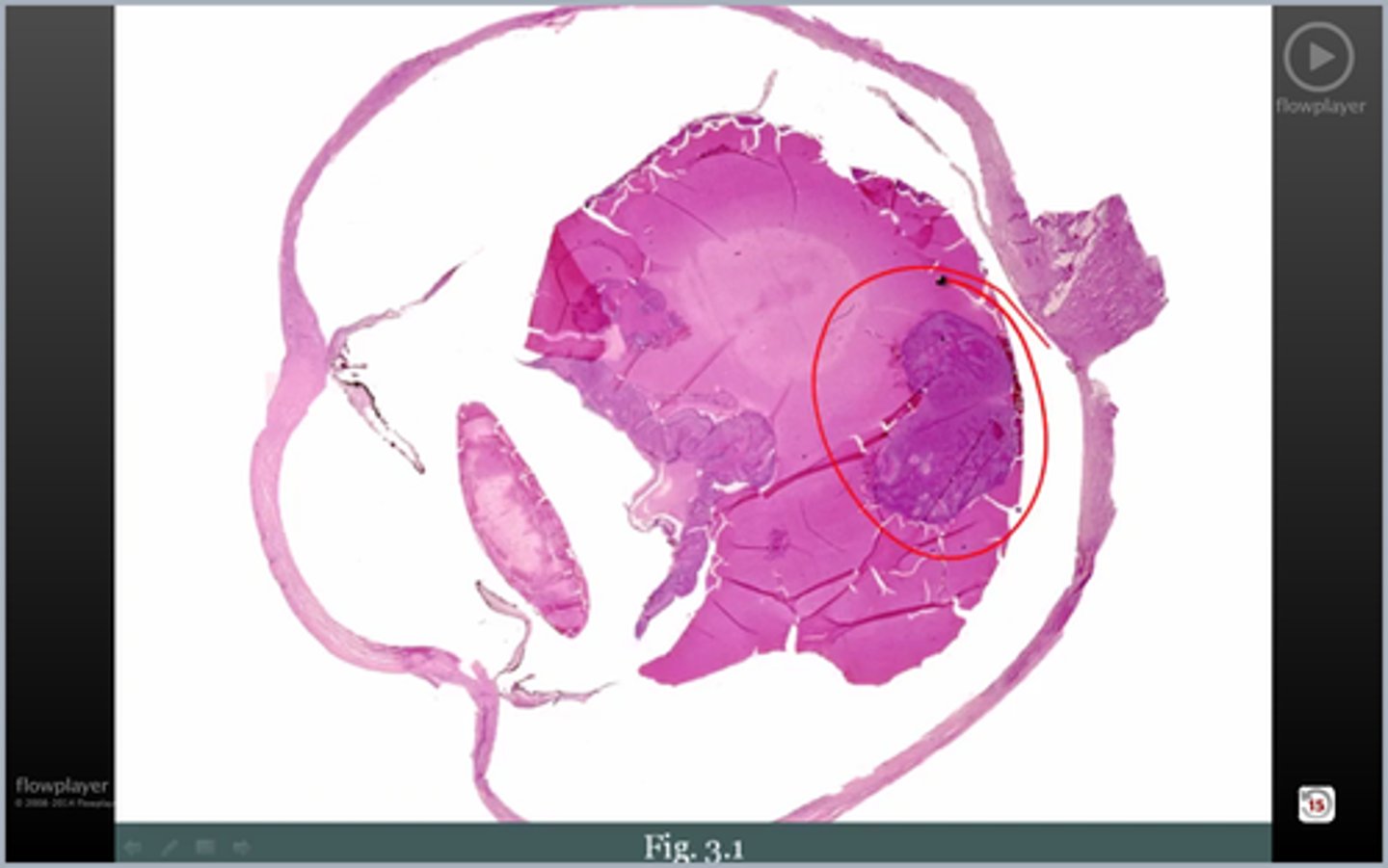
retinoblastoma (Rb TSG needs double hit)
looking at eye. what's circled?
discoid rash seen in SLE
ID the rash

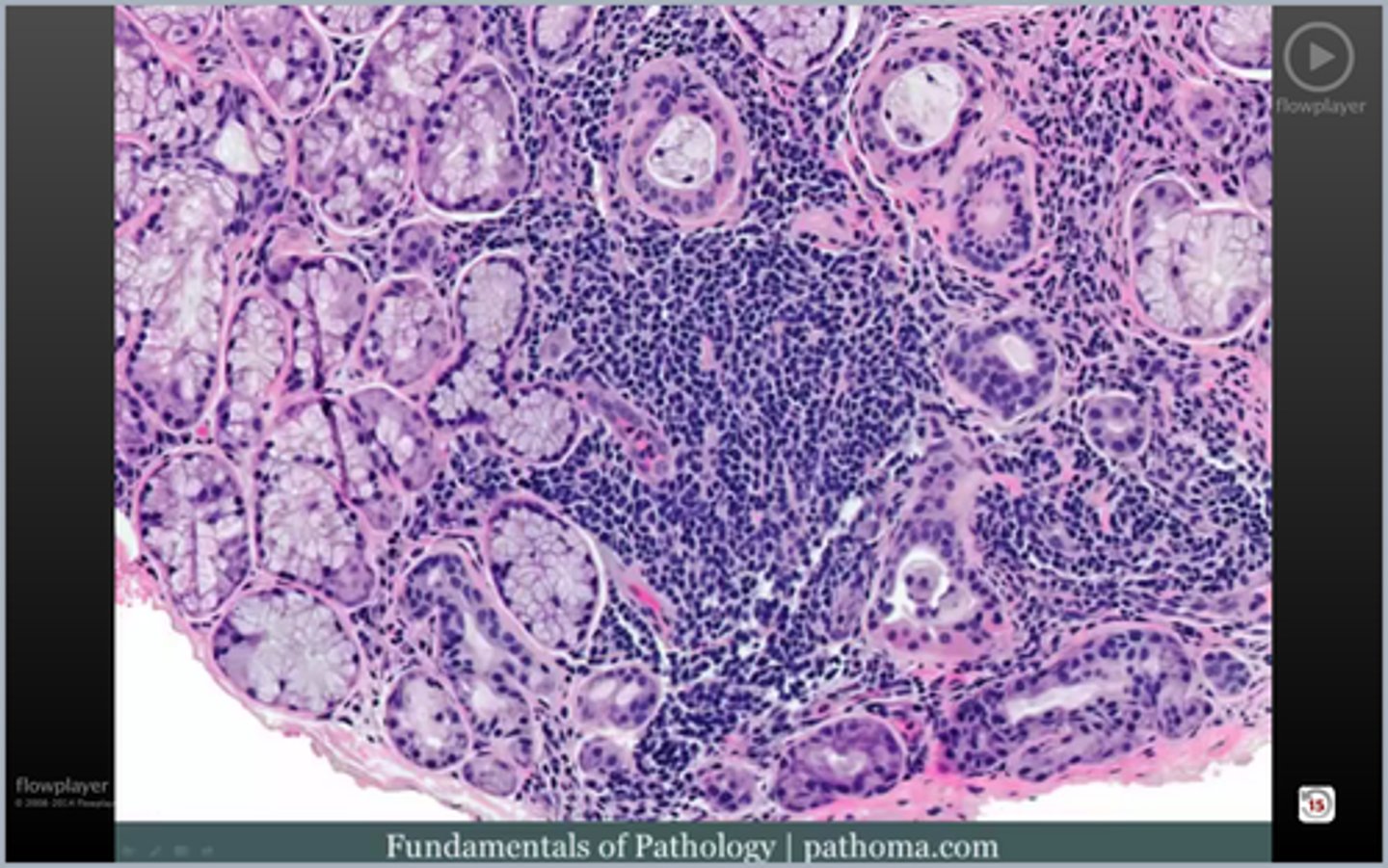
L = normal cells
middle = lymphocytic infiltrate destroying gland = Sjogren's
salivary gland shows
sclerodactyly in scleroderma (CREST)
-notice decreased wrinkles at fingertips bc of tightening of skin (d/t fibrosis)
hand exhibits what

on R = petechiae (pin point bleeds)
on L = ecchymoses (> 1 cm)
purpura > 3 mm
skin bleeds

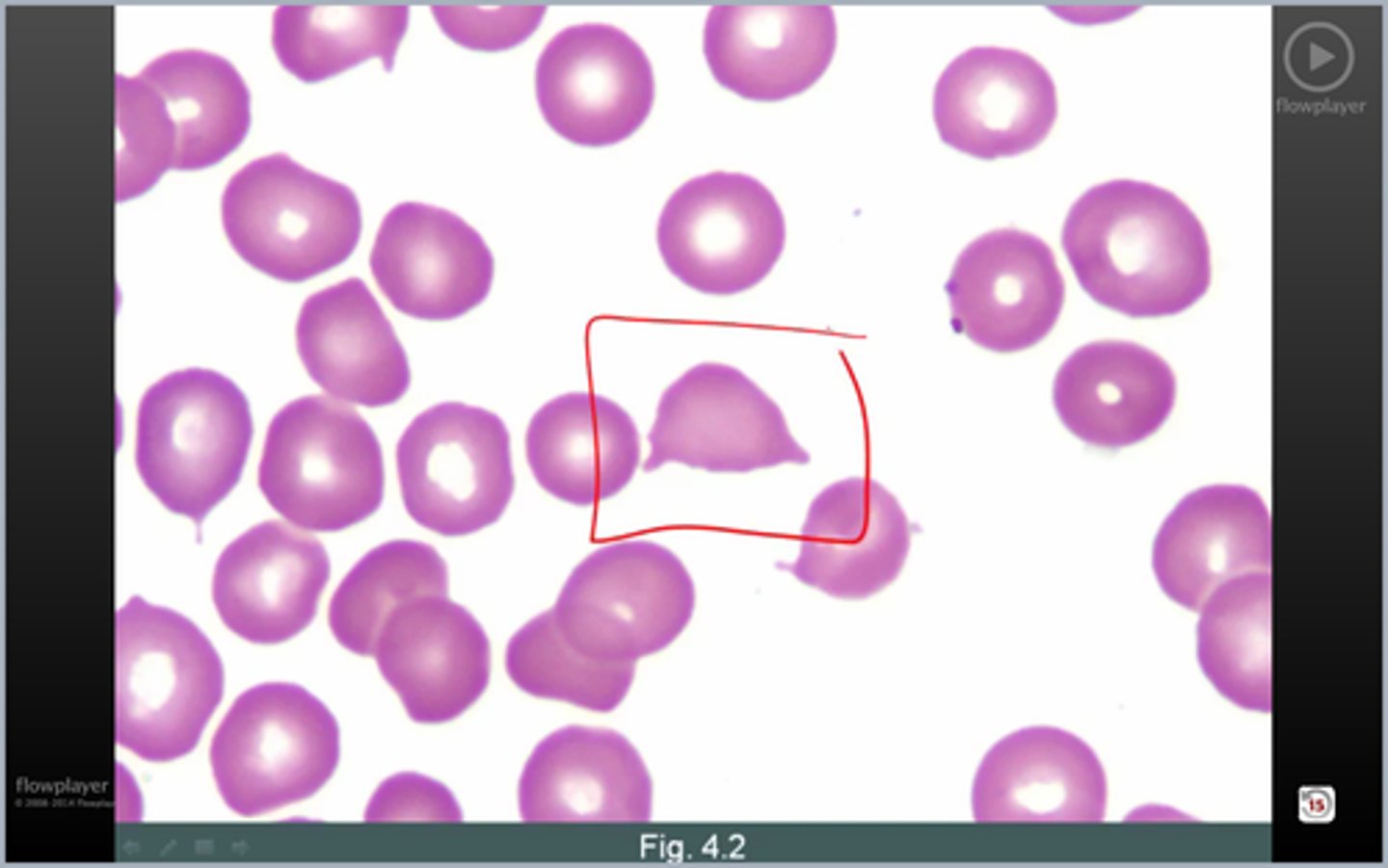
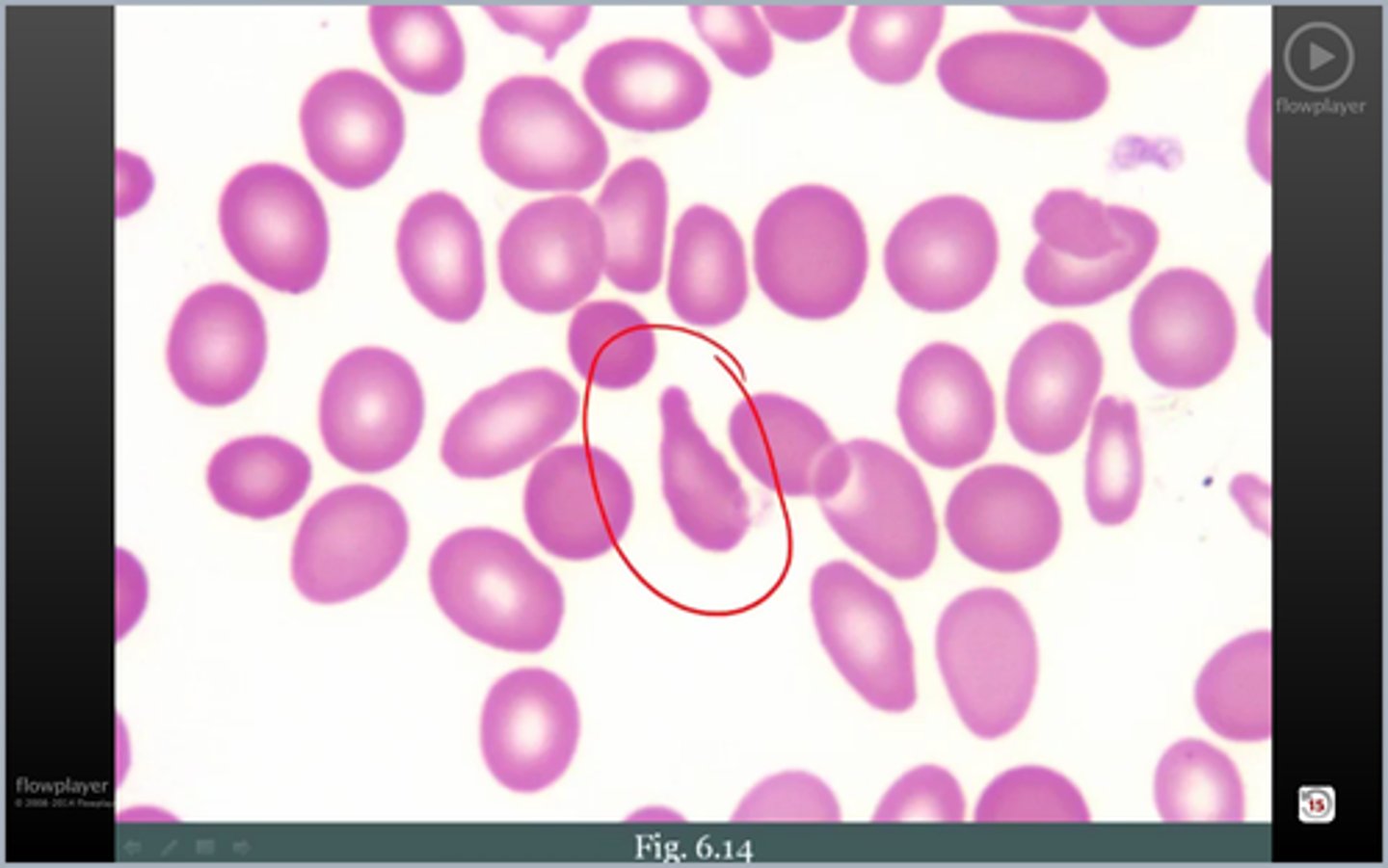
sheared RBC = schistocyte (helmet cell)
microangiopathic anemia
what cell highlighted; seen in?
lines of Zahn: tells us Pt. had pre-mortem clot
R = RBC
f = platelets + fibrin (clot)
but what diz; what do they tell us
blood vessel occluded by atherosclerotic embolus (white long gaps in middle are cholesterol crystals)
what this
fat emboli (circular spaces = fat cells)
and this
keratin debris in blood vessels = pink cells = amniotic emboli (baby's fetal skin soaking in amniotic fluid)
preg woman
saddle embolus
-embolus has saddled across and knocked out both pulm aa.
my word what is this

Iron Def Anemia:
-lymphocyte nuc & RBC size should be same so as reference you can tell RBC size small
-also notice spectrum of RBC exists (bc this first has normocytic anemia b4 microcytic)
-also increased central pallor = hypochromic
what is this and how can you tell
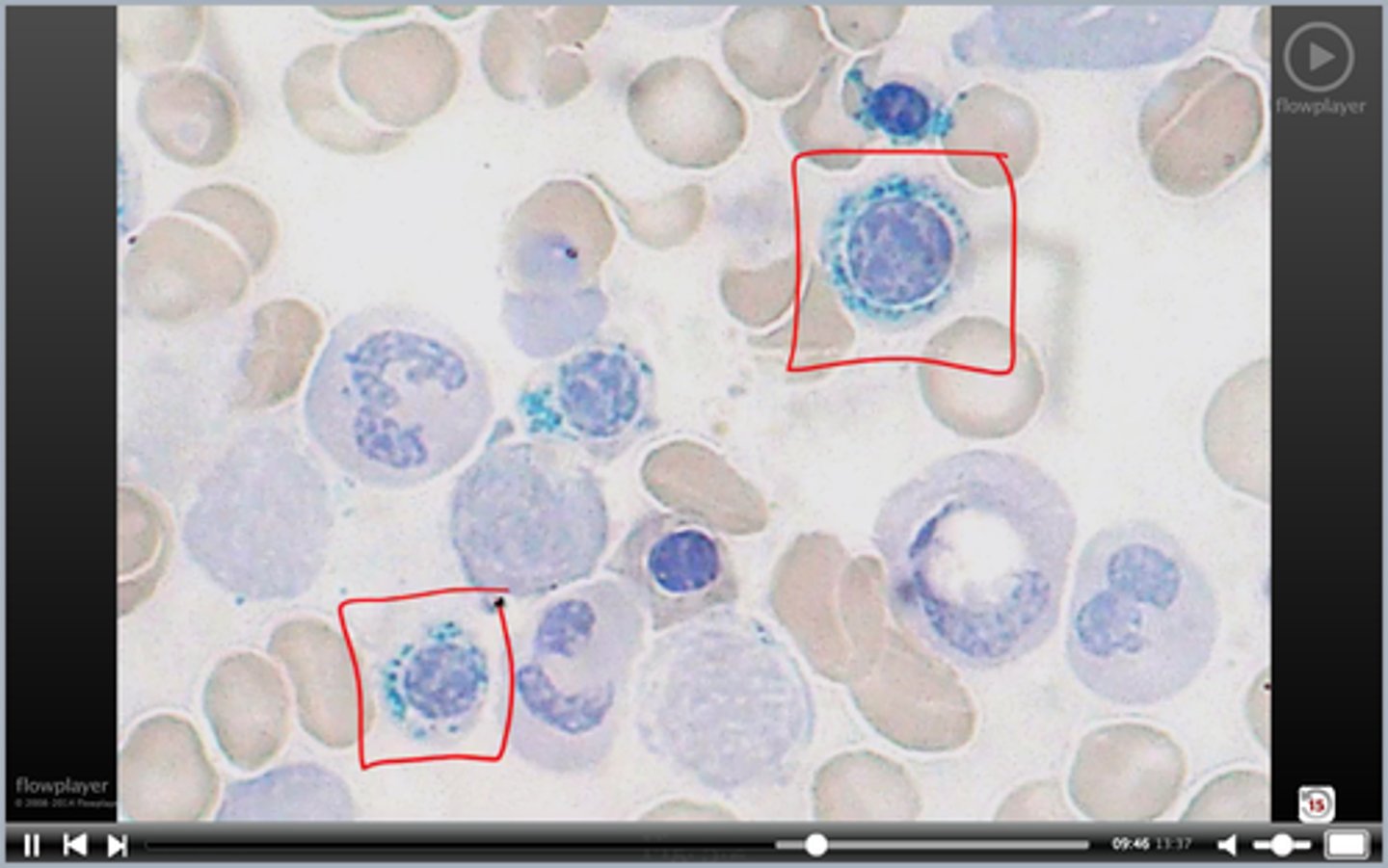
prussian blue stain (stains for Fe) shows iron accum in Mt rings around nuc = sideroblastic anemia
this is a BM biopsy of erythroblast cells
blue ring indicates what; stain?
target cell in HALT: HbC Dz, Asplenia, Liver Dz, Thal
name the cell; found in what Dz's

massive expansion of hematopoiesis in new parts of bone to make new RBC's (d/t increased loss)
Dx = B-thal MAJOR or SCA forming "CREW CUT" -> sk. deformities -> chipmunk facies
why does skull look like that; Dx; sequelae?

chipmunk facies d/t B-thal major
and this?

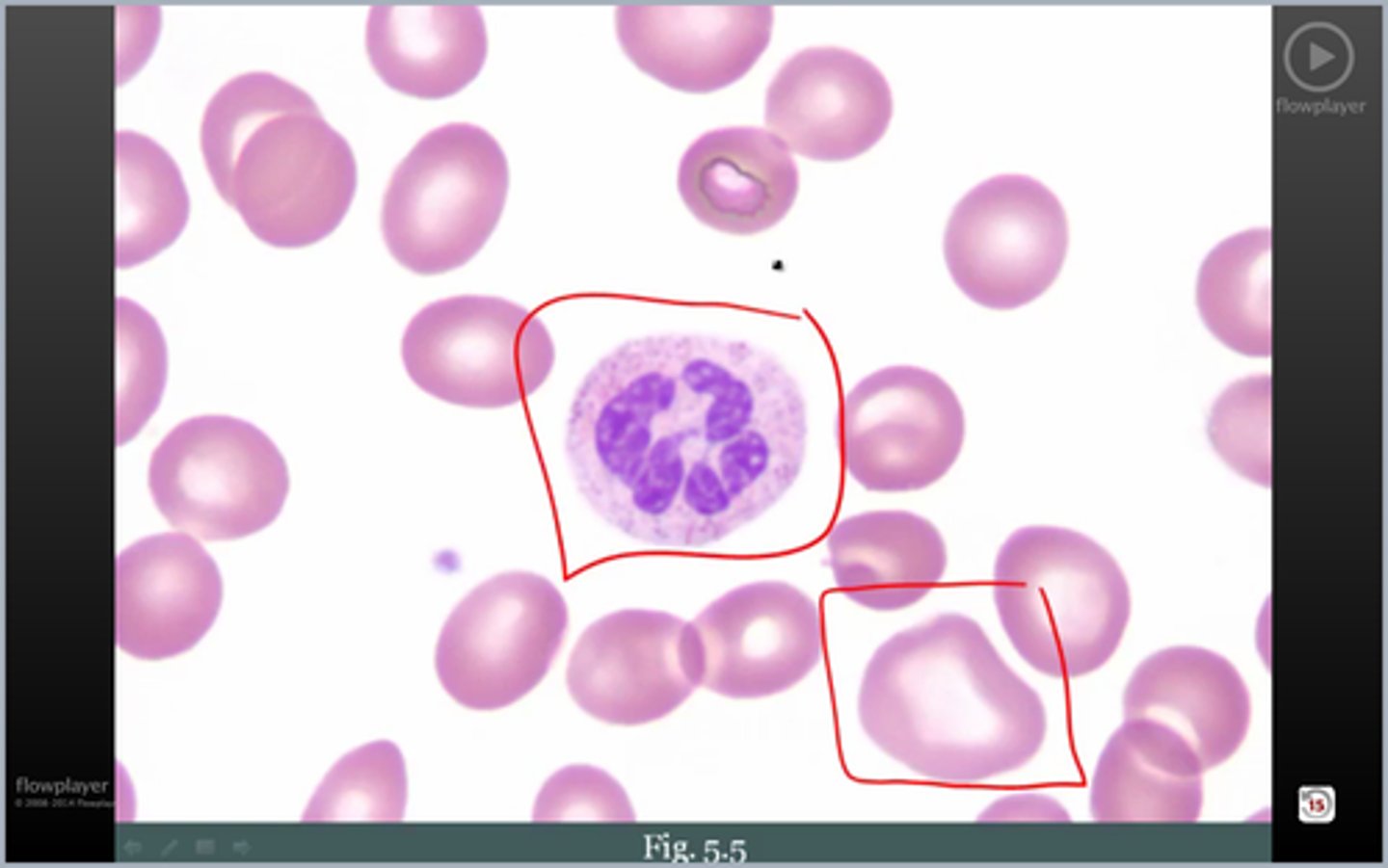
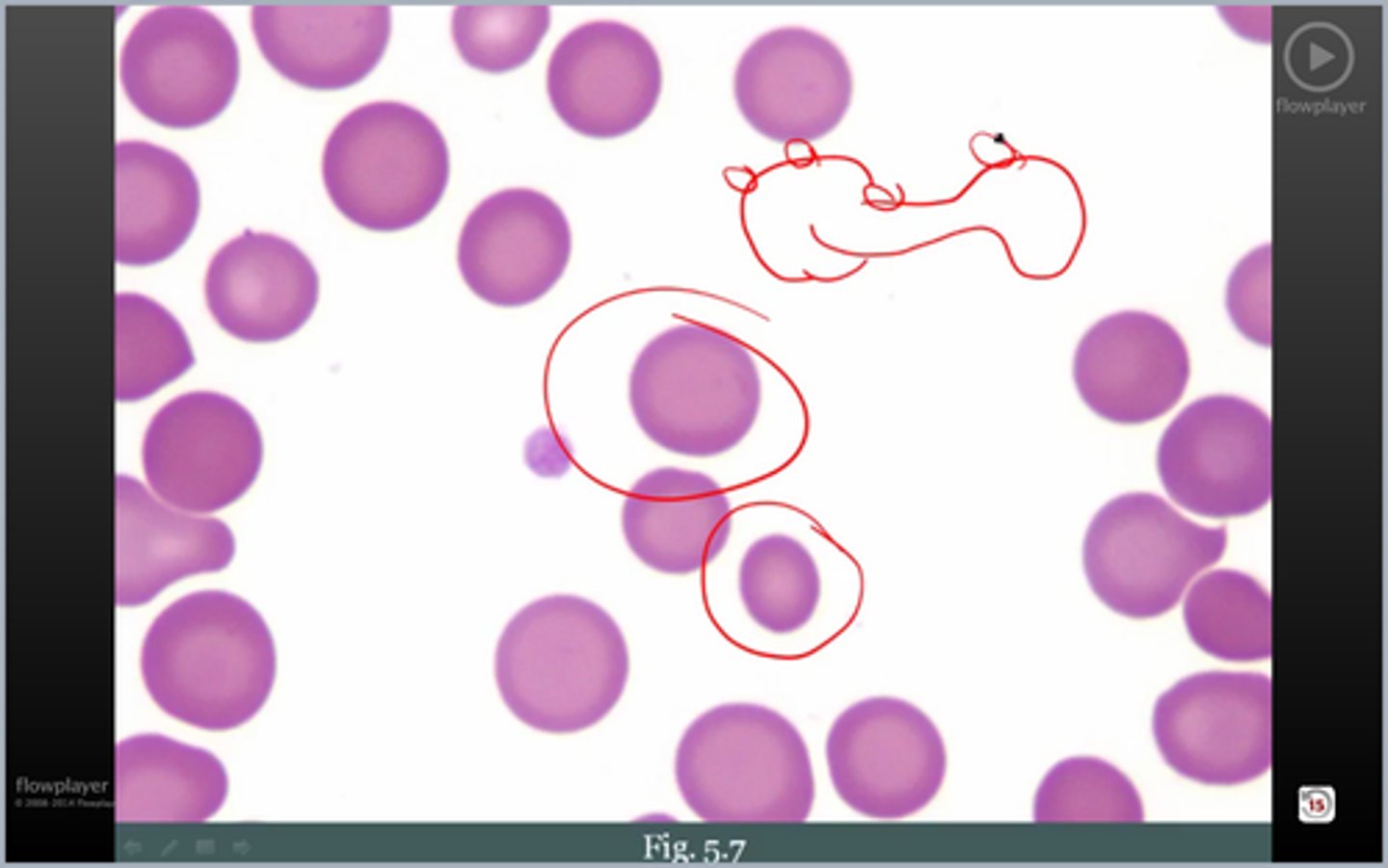
on L = hyper-segmented PMN (> 5 lobes, has 7)
on R = macroovalocyte (big RBC, MCV > 100)
Dx = megaloblastic anemia d/t folate or B12 def
Dx?
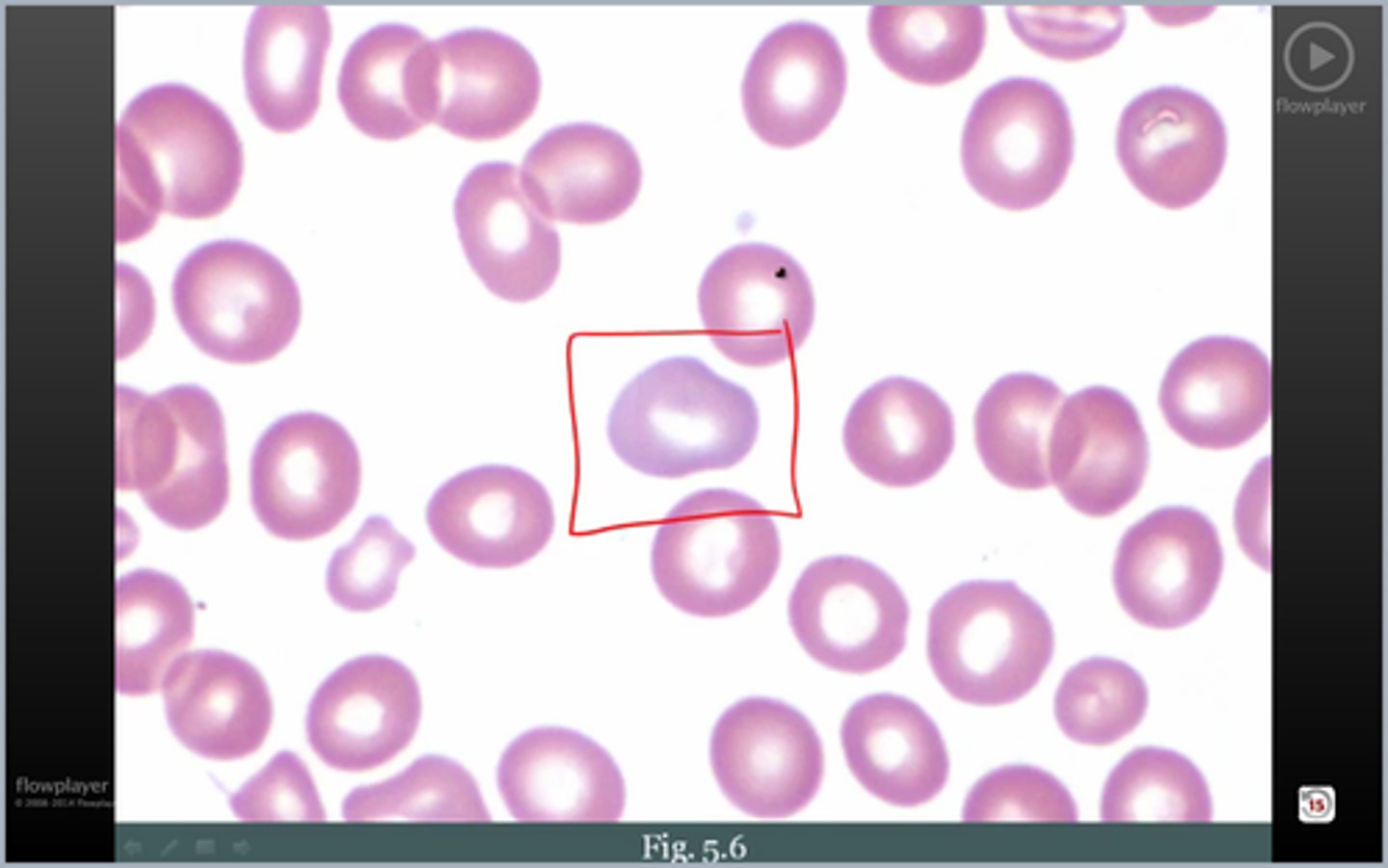
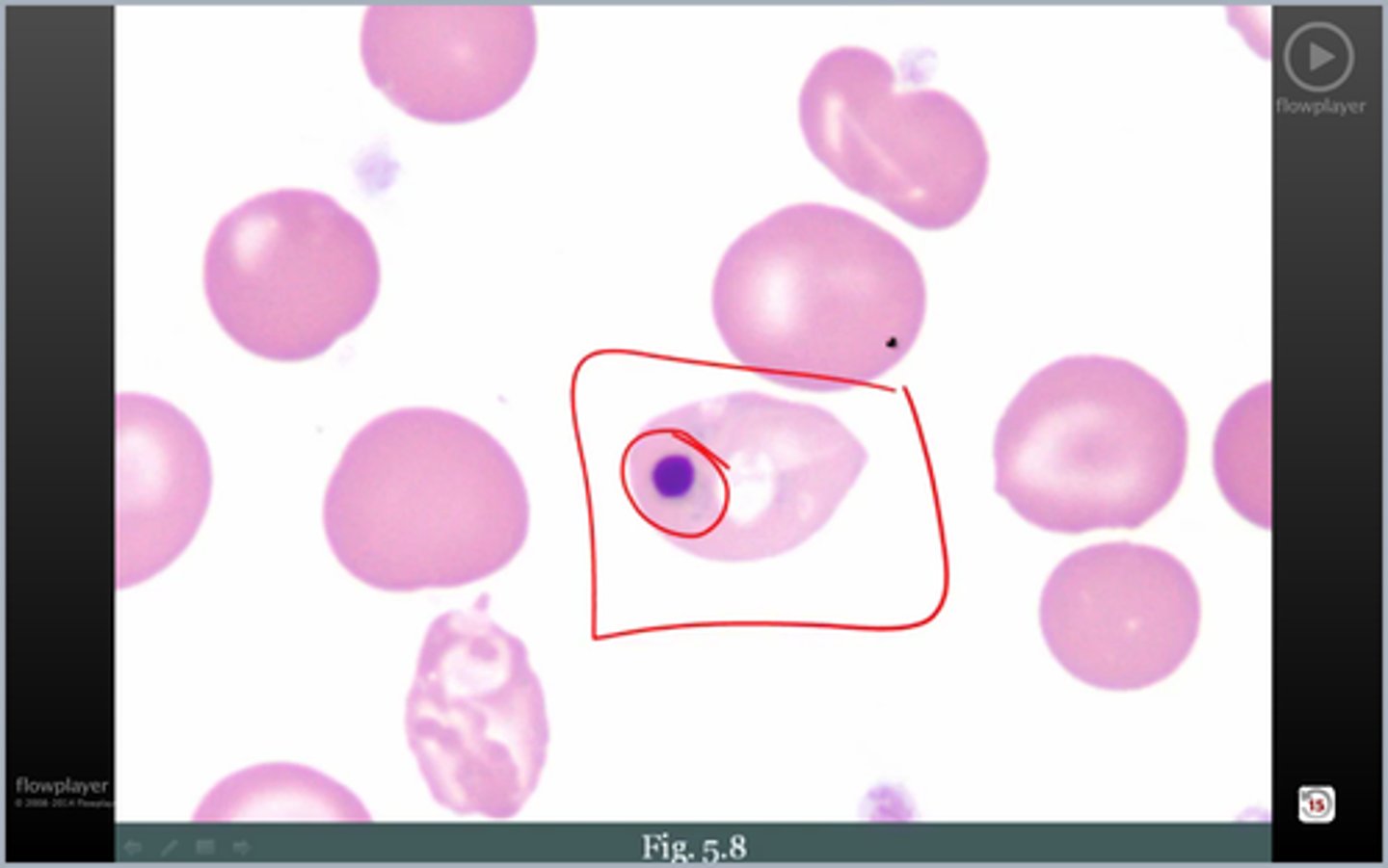
it's larger and has a bluish tinge (d/t increased RNA in cytoplasm) = reticulocyte (baby RBC)
what's weird abt this RBC?
HS (smaller than avg RBC w/ no central pallor)
-range of size d/t fact that oldest cells lose more membrane (smaller RBC than newer ones)
what's wrong w/ cells here
nuclear remnant in RBC = howell-jolly bodies d/t splenectomy
wtf rbc? cause?
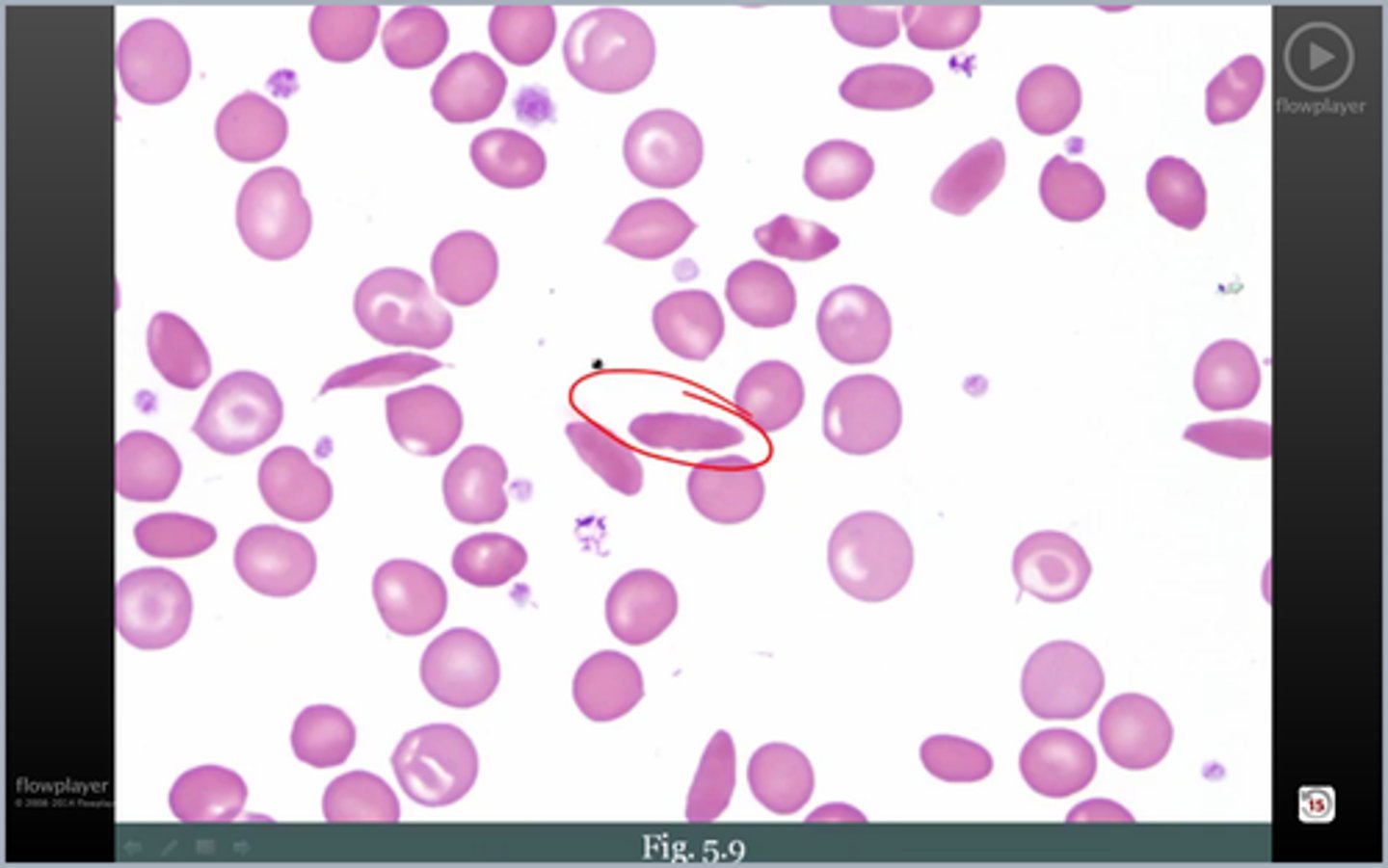
SCA: banana shaped RBC d/t polymerization of HbS in low O2, dehyd, acidosis
wtf rbc2? cause?
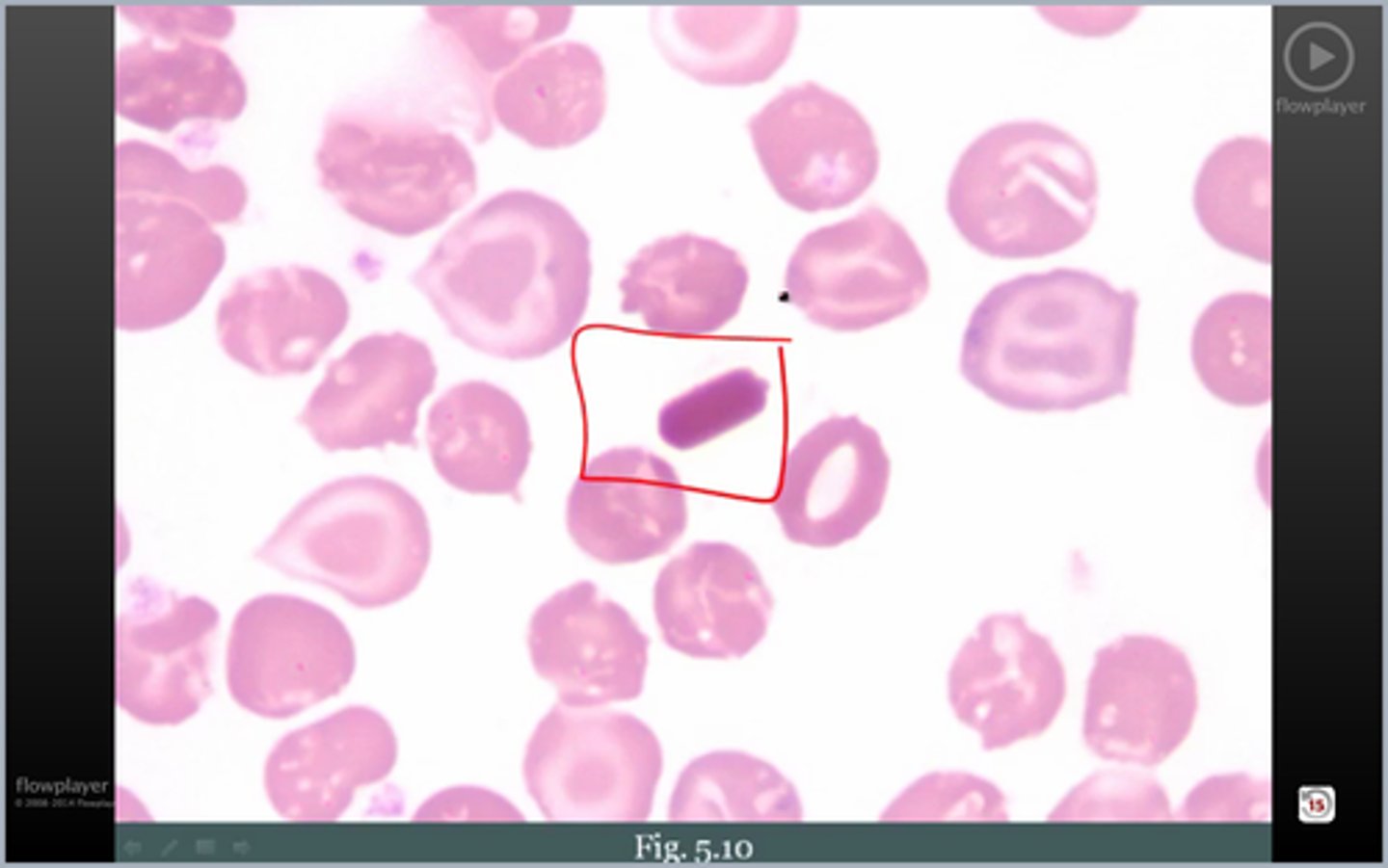
HbC crystal d/t glutamic acid to LYSINE (C for LyCn) mut
wtf rbc3? cause?
bite cells in G6PD def
wtf rbc4? cause?

Heinz prep showing precipitated Hb (G6PD def)
HUH wtf rbc4? cause?

malarial org present w/in RBC's (Plasmodium)
wtf rbc5? cause?
notice empty BM replaced by adipocytes (NO HEMATOPOIETIC ELEMENTS) = aplastic anemia
BM shows
atypical lymphocyte (CD8+ T-cell) in Infectious mono (d/t EBV or CMV); 2nd flashcard of this know this
whart dafuquh
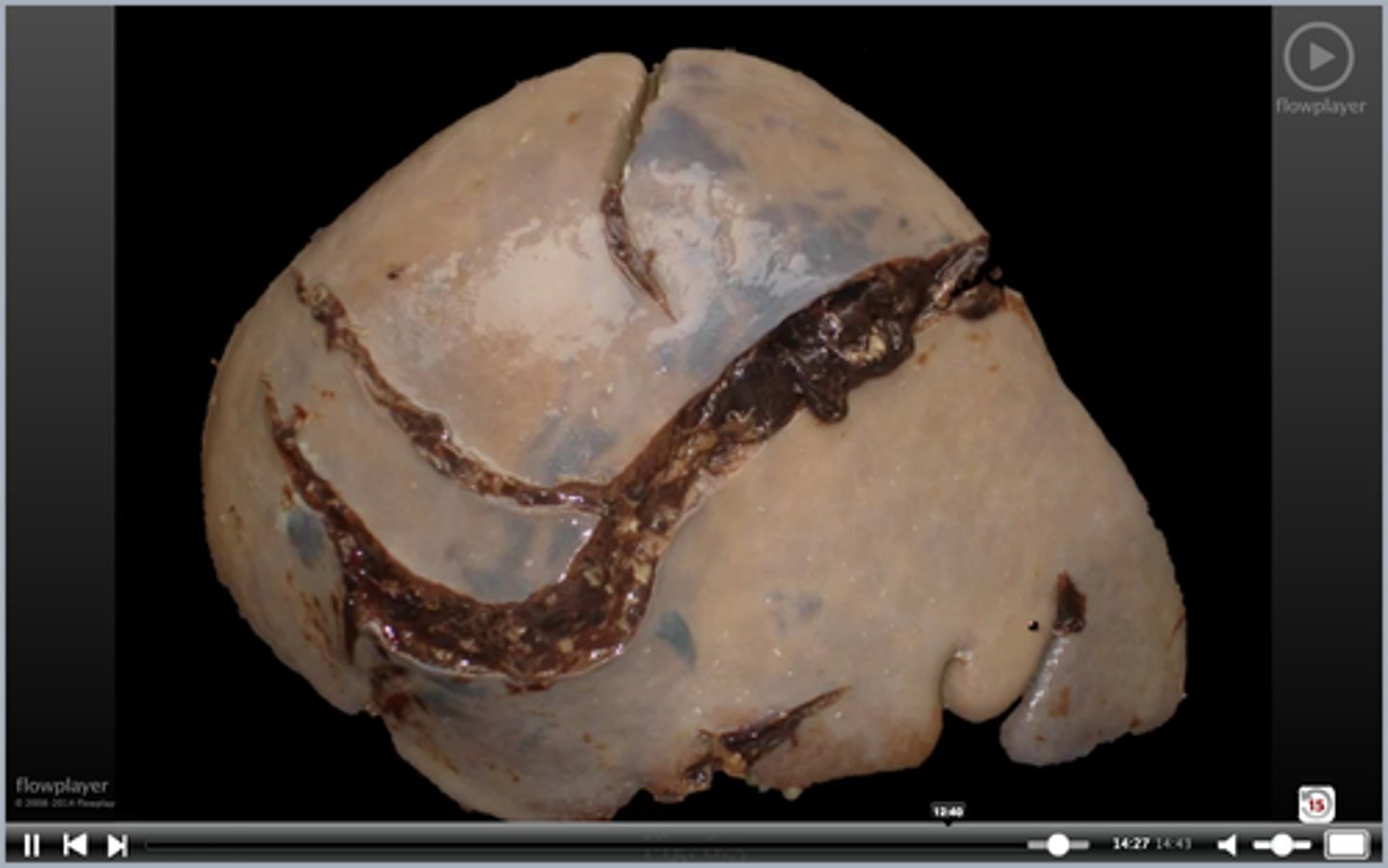
splenic rupture d/t EBV induced mono (causes spleen to enlarge, now more susceptible to rupture thru capsule)
-we tell Pt. to avoid contact sports for 1 yr bc any light contact with spleen can cause this
what are ur eyes seeing right now
plz spk thru lips
-viral cause?
-Tx
erythroblast (immature RBC, lacking cytoplasm, w/ "punched out" nucleolus circled)
-can't tell if myeloidblast or lymphoidblast
and vut dis?
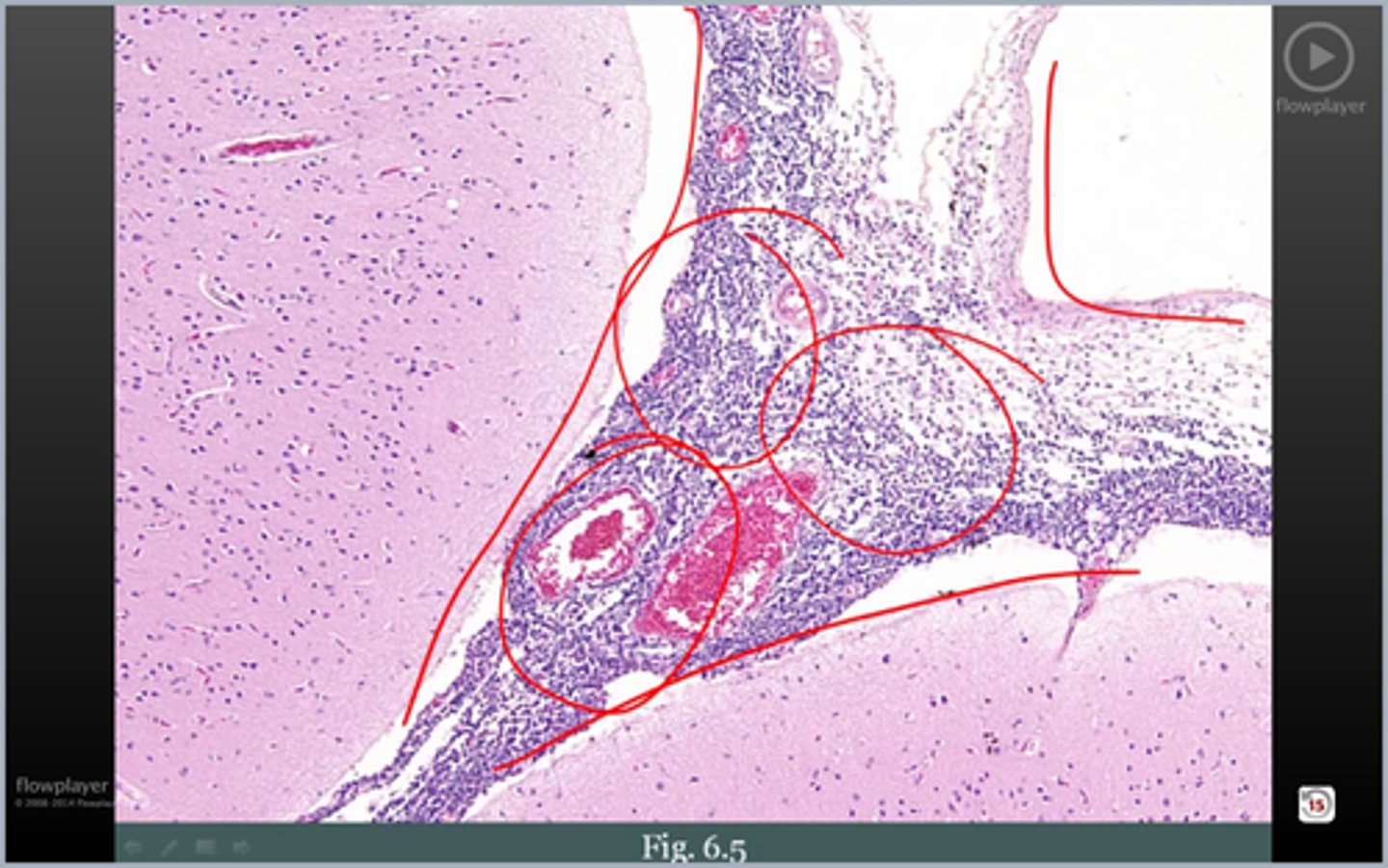
blue dots in meninges = ALL spread to CNS
meninges of child
Auer rods in AML
rmr Auer rods are crystal aggregates of MPO, which are only prod by MYELOblasts
-also notice it's large w/ punched out nucleolus = blast
for 2nd time; notice thin rod
AML type (acute monocytic leukemia)
-monoblasts love to infiltrate gums
masses in gums

smudge cell in CLL (neoplastic prolif of naive B cells)
what's going on top L

notice "hairy" cytoplasmic processes: Hairy Cell Leukemia; Dx by TRAP (get TRAPPED in hair)
what diz be doe? Dx confirm?
notice how T cell has "brain-like lobes" = cerebriform nuclei d/t Sezary Syndrome in Mycosis fungoides
bad T cell
we see a basophil amongst many granulocytes. if basophil ct. increases, think CML
hint top L
ton of platelets; Dx = essential thrombocytosis (backup = iron def anemia)
ton of these; Dx
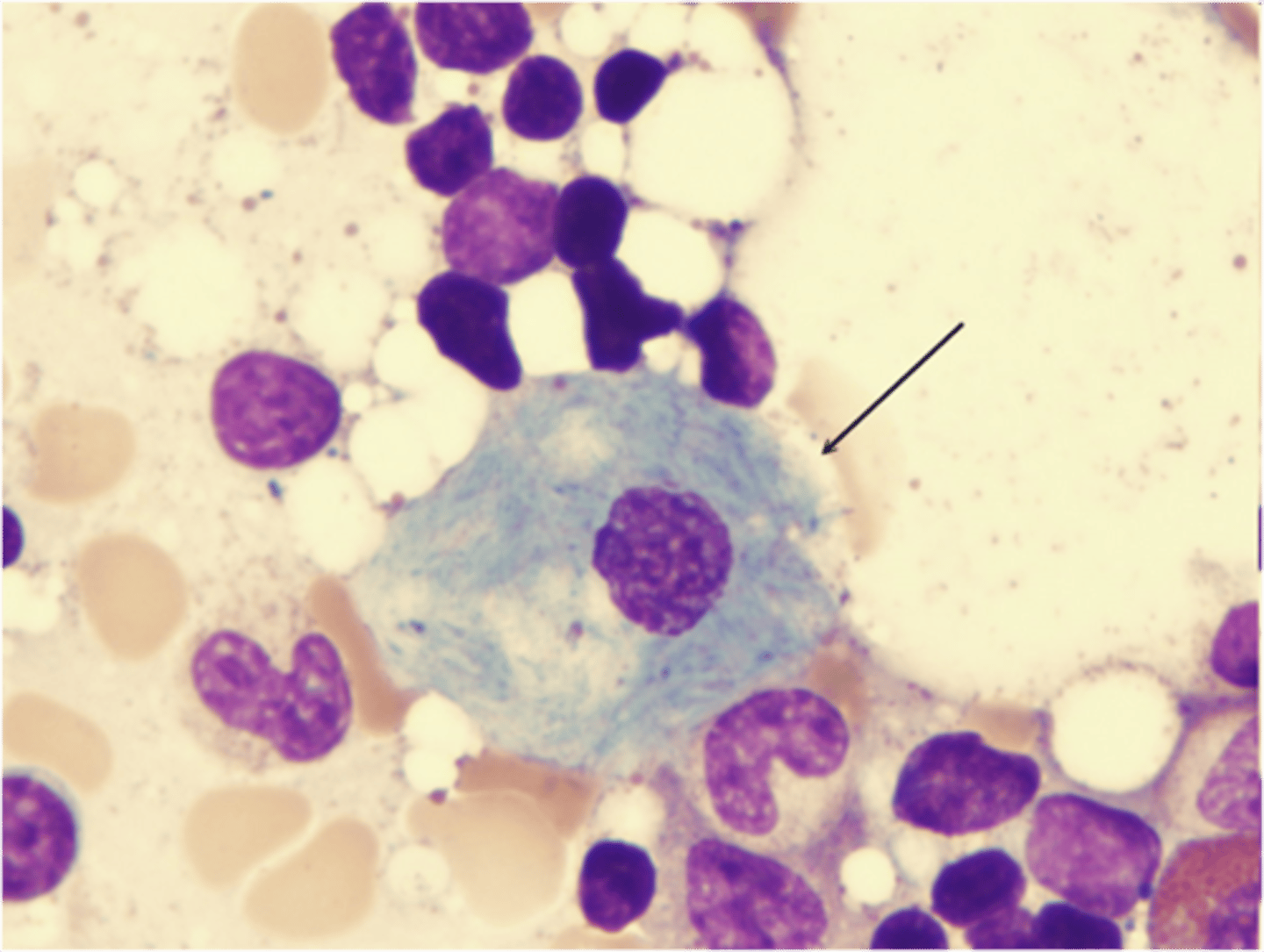
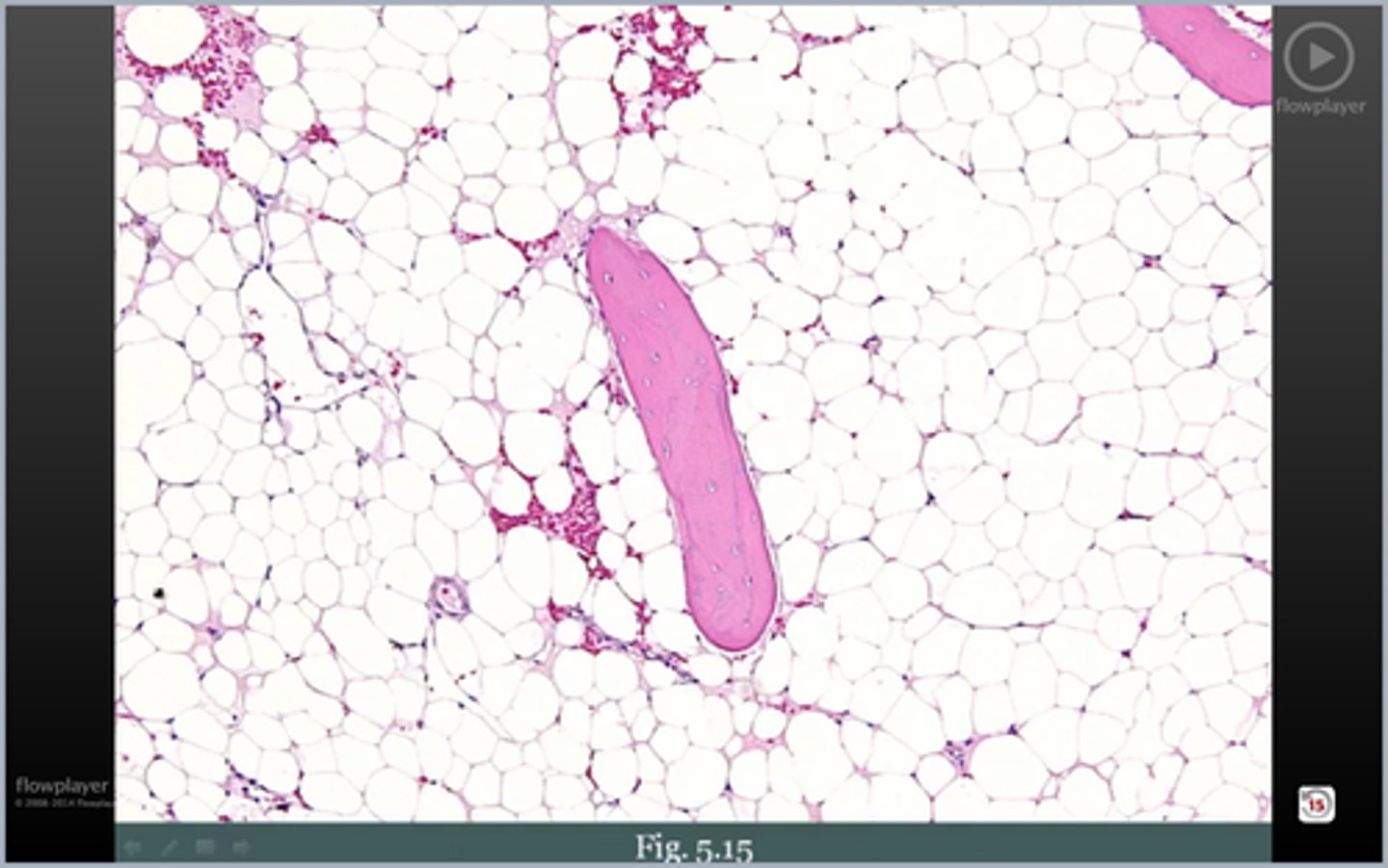
look at all the other stuff (squiggly = light pink collagen), we should only see circles (fat) & BM elements
Dx = myelofibrosis
pink bar in middle = spicule of bone
BM
in fibrosed BM, when RBC leaves it gets stretched out = teardrop cell in myelofibrosis
"BM is crying bc it's fibrosed"
weird RBC
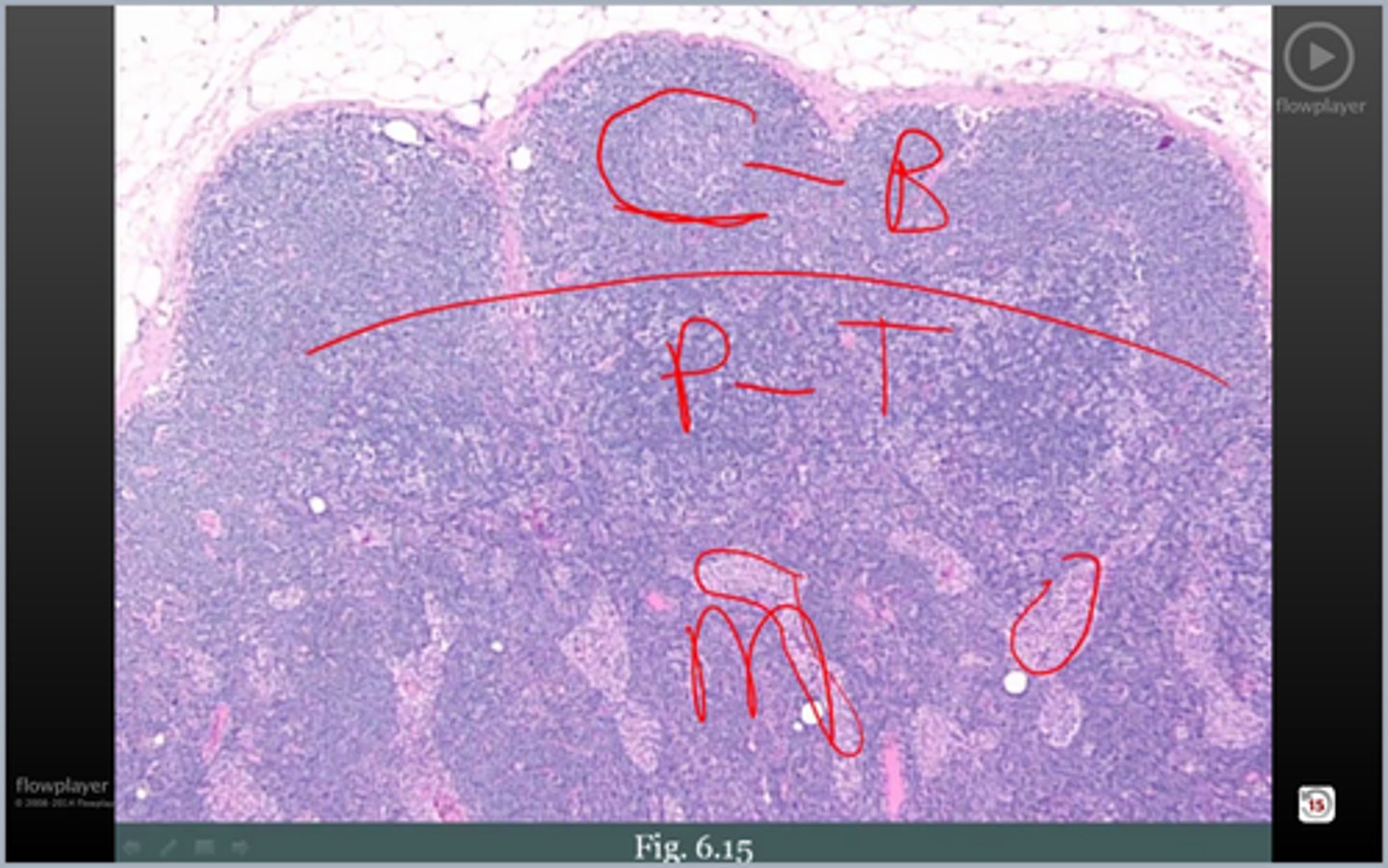
LN
-Cortex = B-cells (hyerplasia in RA, early HIV)
-Paracortex = T-cells (all viral)
-Medulla, site of sinus histiocytosis (reactive hyperplasia to cancer)
what lymphoid tissue is this
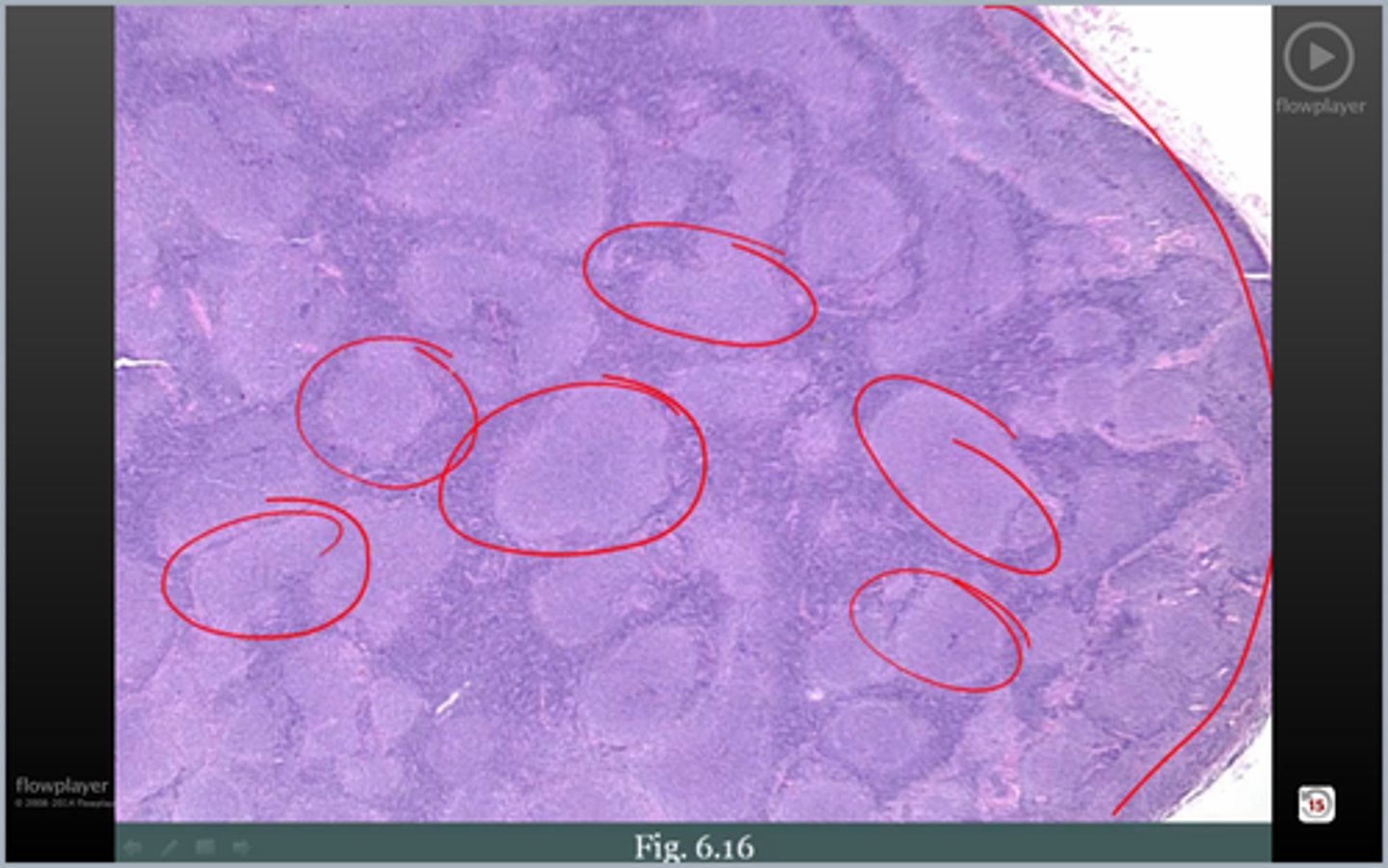
notice how many follicles there are thru ENTIRE LN (instead of just cortex; so not simply reactive hyperplasia) = follicular lymphoma
another LN; what's interesting? Dx?
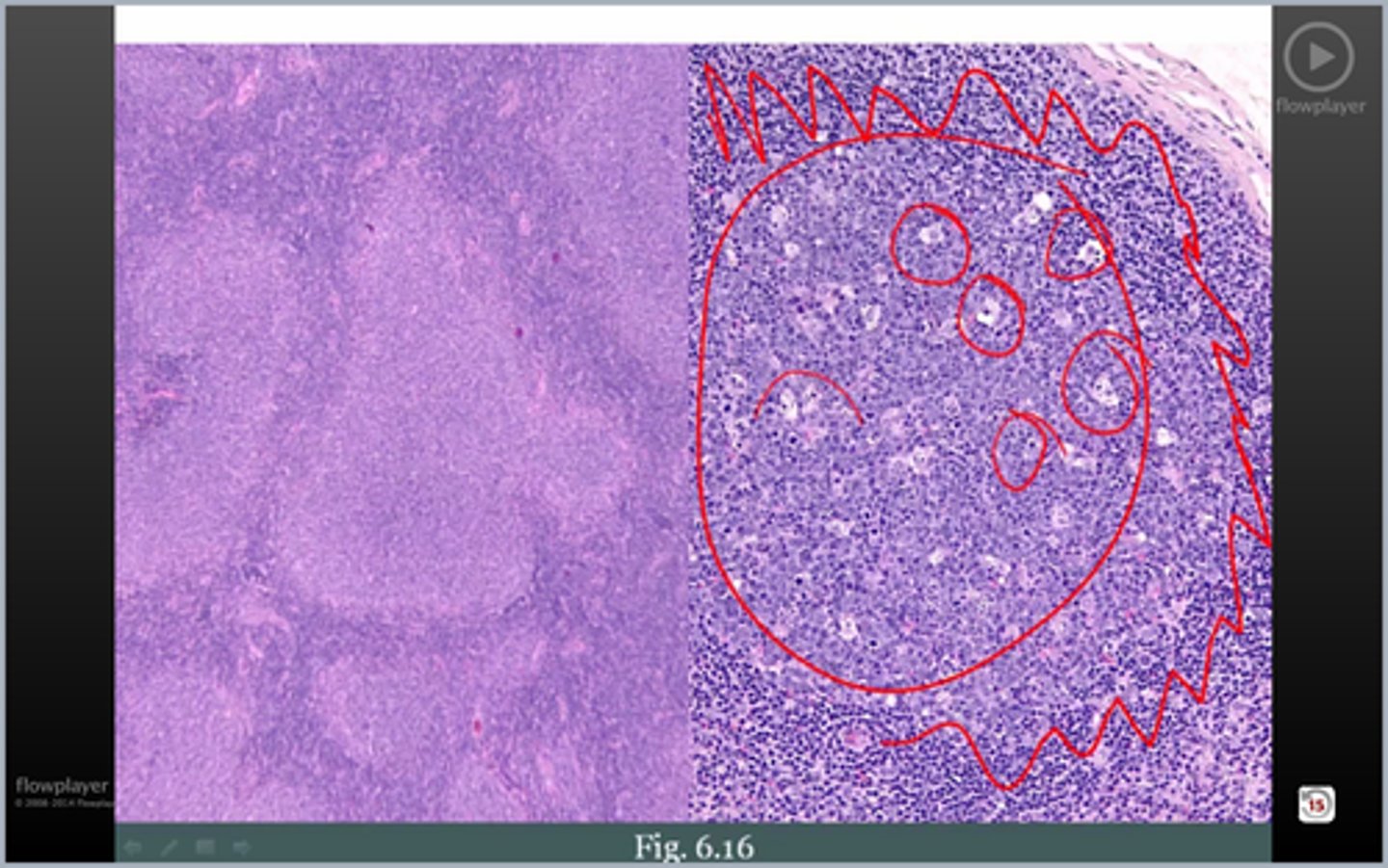
R = reactive hyperplasia in germinal center (white spaces = tingle body macrophages apoptosing dead B-cells that underwent somatic hyper-mut & didn't survive)
L = follicular lymphoma (increased b-cl2 blocks apoptosis)
LN: L vs R
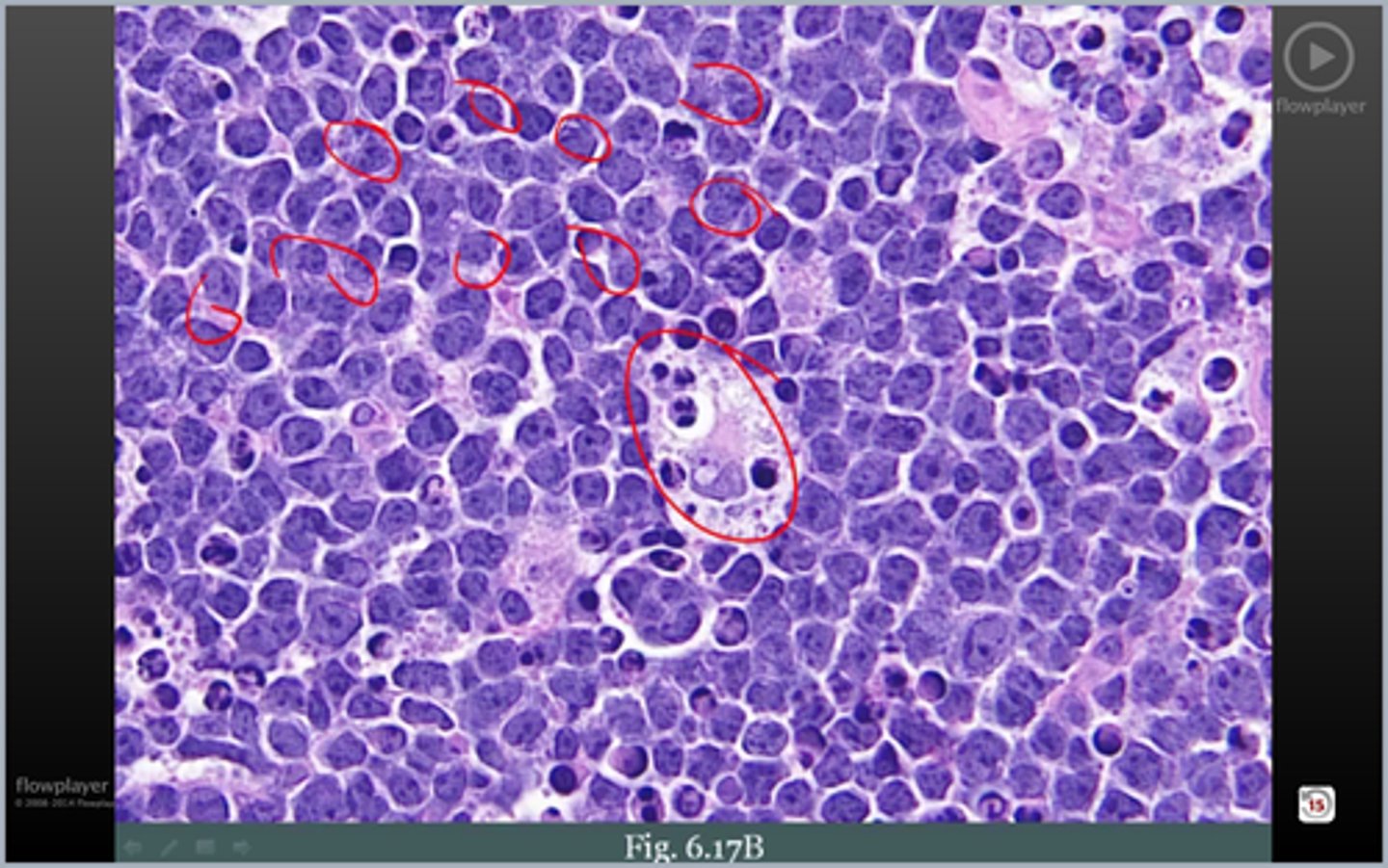
starry sky = Burkitt's Lymphoma
blue = the sky, tumor cells
white = star, tingible body macrophages that are eating the dead tumor cells that grow so fast they die
classic pic
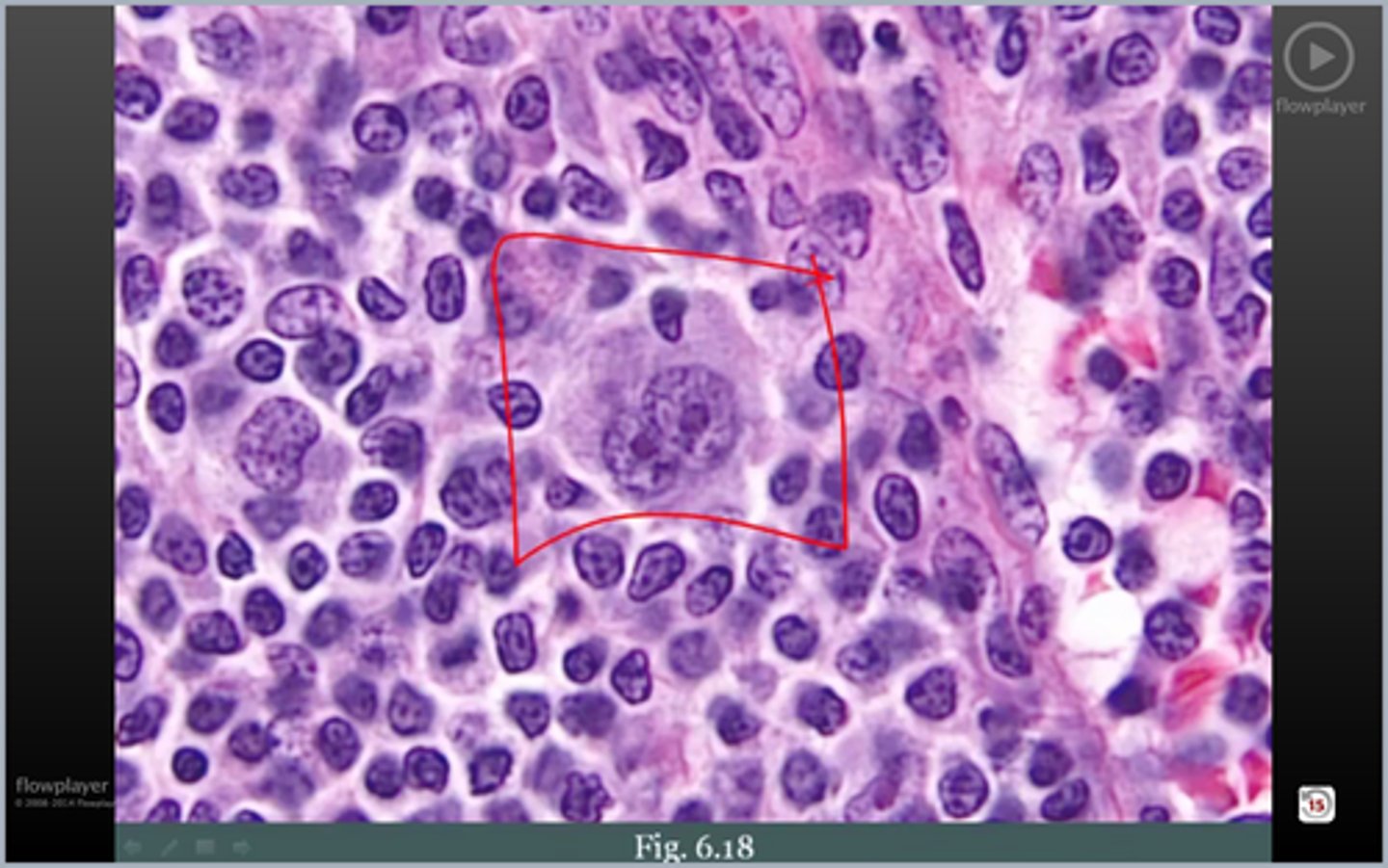
RS cell (HL) notice "owl eyes"
what this guy
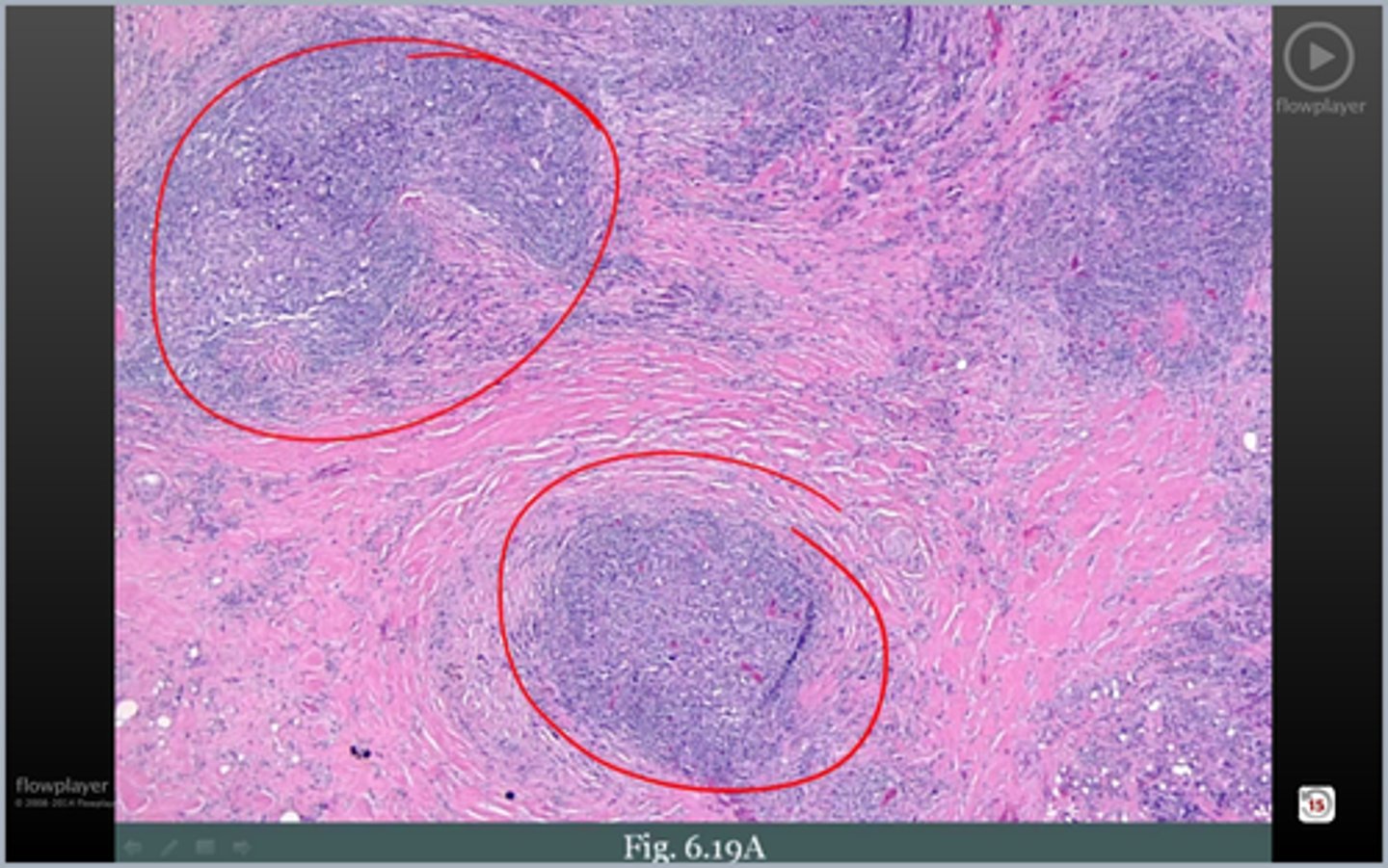
broad pink bands of fibrosis cut LN into "nodules" = nodular sclerosing HL (most common form)
sclerosing = hard, bc all this fibrotic tissue
what abt this LN
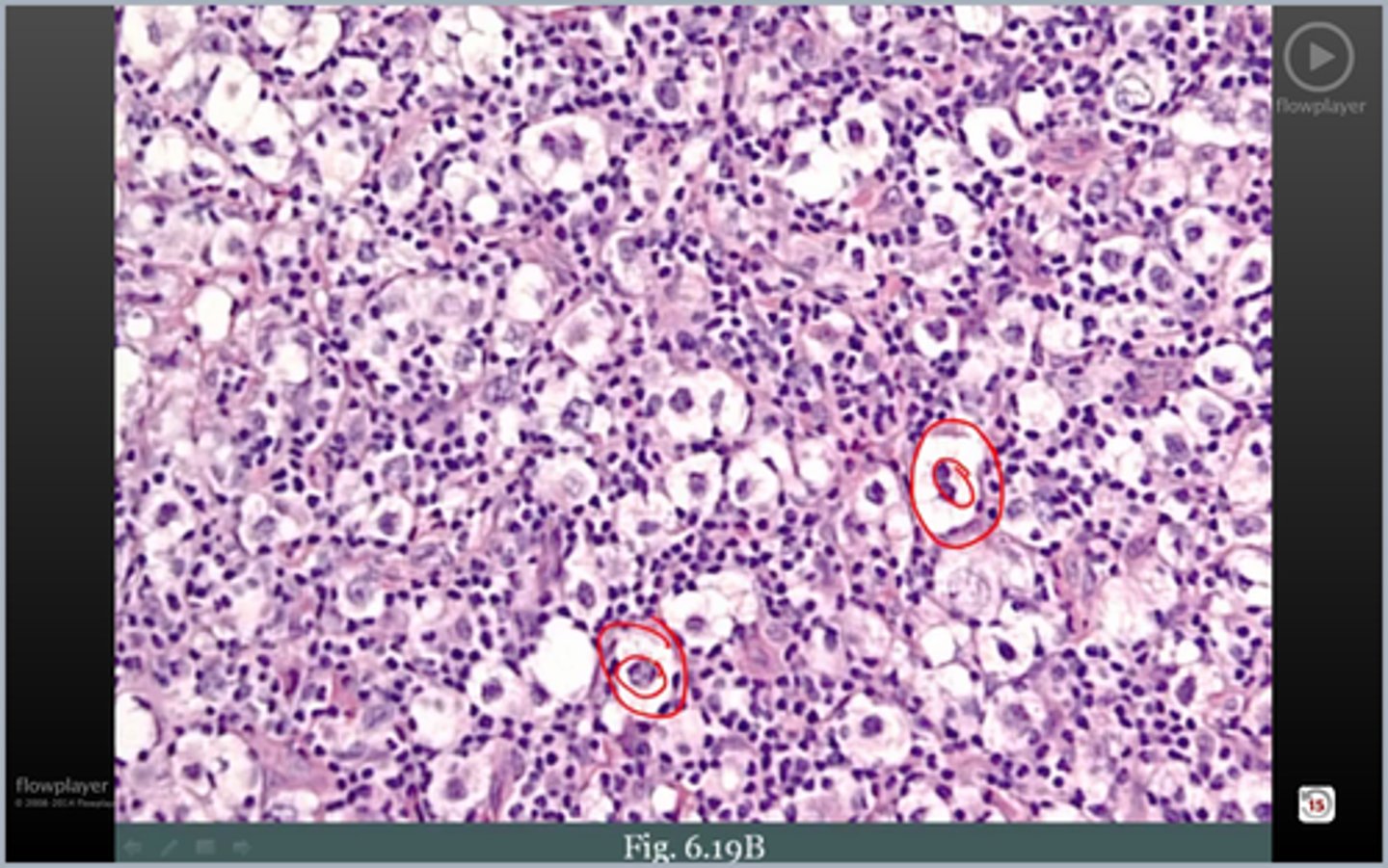
lacunar cells bc now RS cells sit in these "big lakes"
Cx of nodular sclerosing HL (most common form)
Cx RS Cells
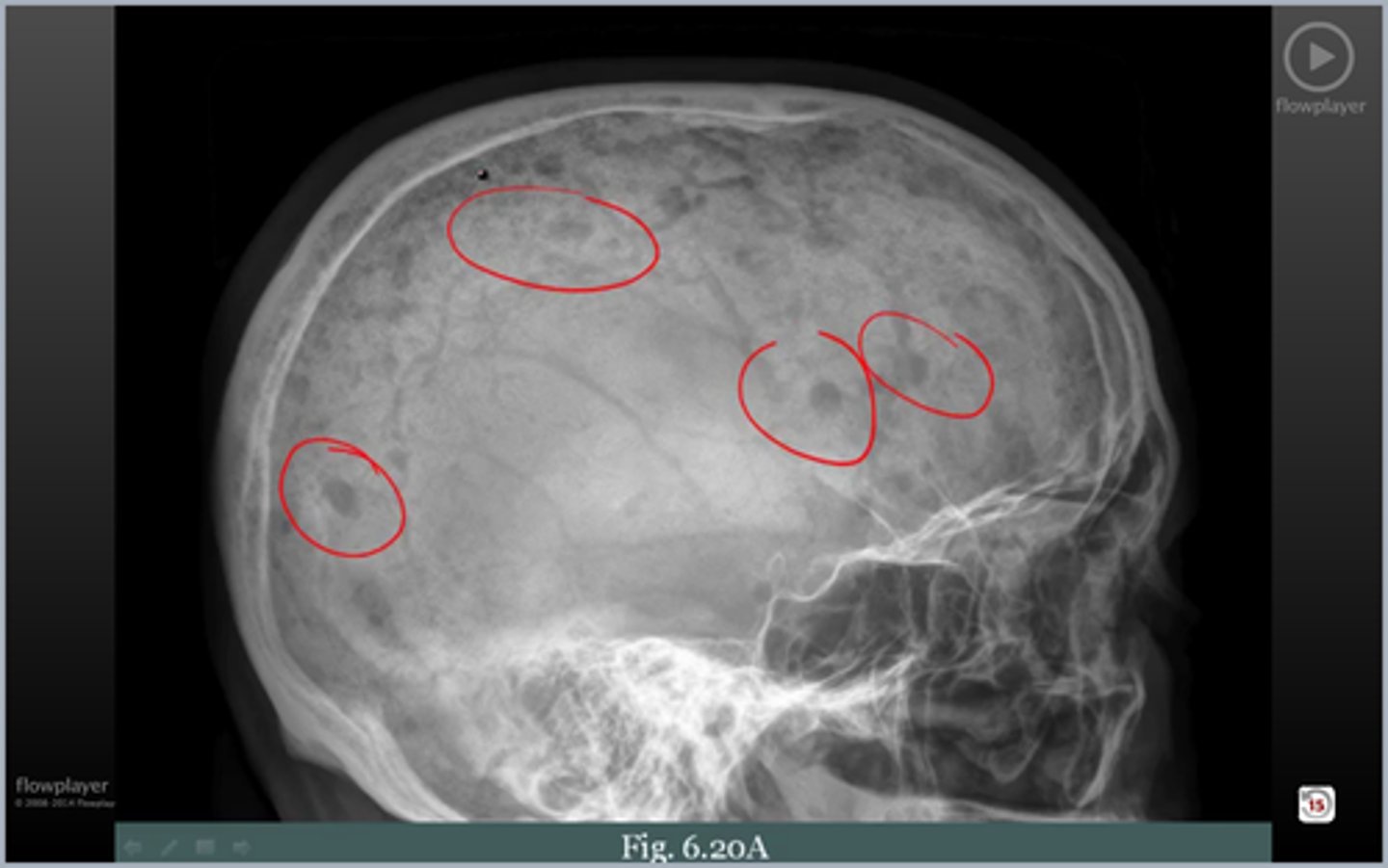
MM
punched out lesions on x-ray
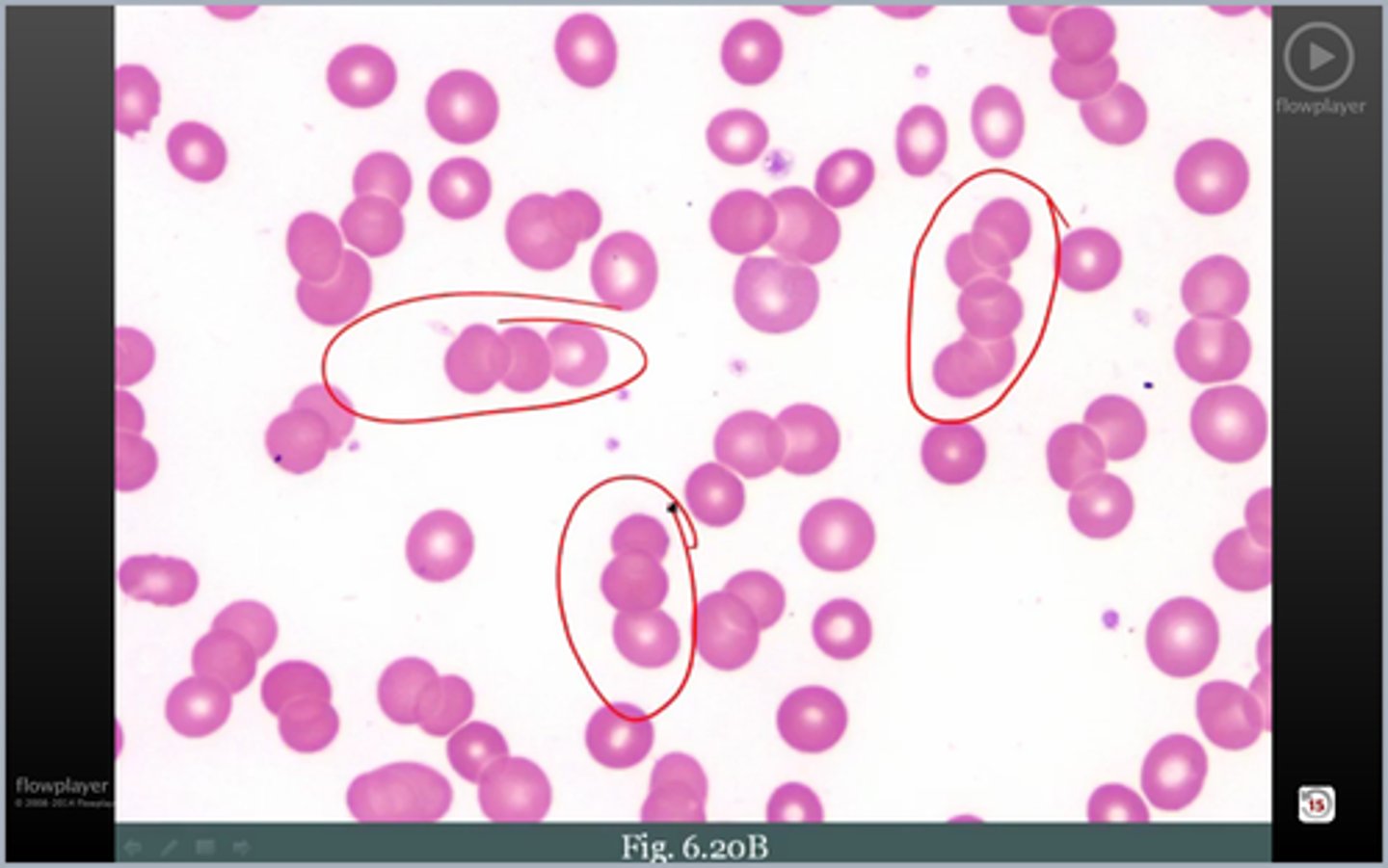
rouleaux formation d/t MM (increased protein in serum decreases charge b/w RBC's causing them to clump)
poker chips
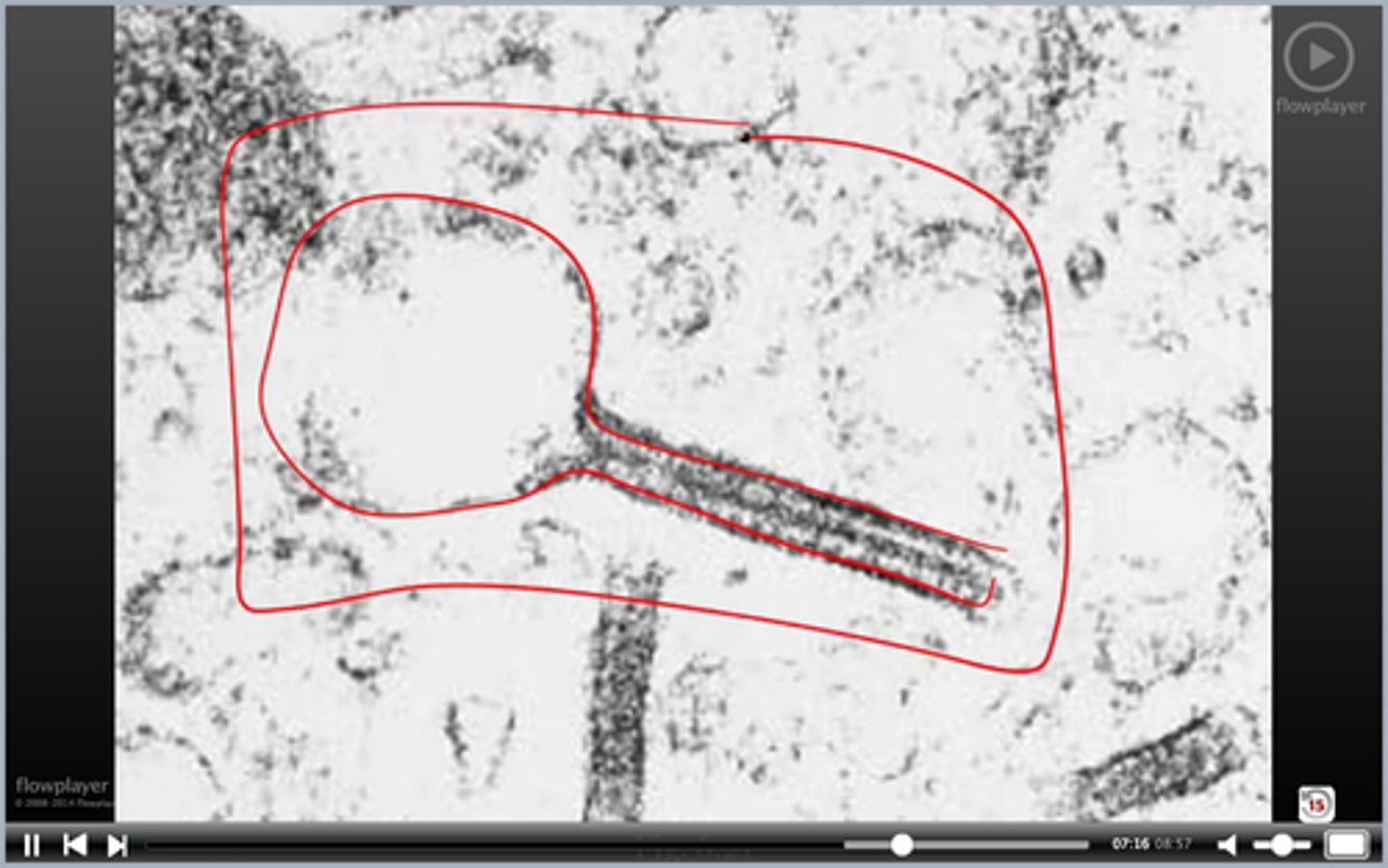
tennis racket = birbeck granule = LH cell histiocytosis
hi