Phys Di II - Exam 2 (EKG + Vascular)
1/62
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
63 Terms
EKG paper measurements
small boxes = 0.04 sec
large squares = 0.2 sec + 0.5 mV
5 large squares = 1 sec
15 large squares = 3 sec
Ventricular rhythm on EKG
look at R wave to R wave
Atrial rhythm on EKG
look at P wave to P wave
If p waves are not present, what does the patient require
a pacemaker
PR interval
from beginning of P wave to beginning of QRS
What is normal for a QRS complex
1 or 2 waves can be absent
ST segment
should be flat line and make it to the bottom of the EKG (zero)
Atrial (auricular flutter)
saw tooth appearance
atrial cx in excess 200 bpm
multiple p waves for each QRS
racing heart (palpitations), shortness of breath, dizziness
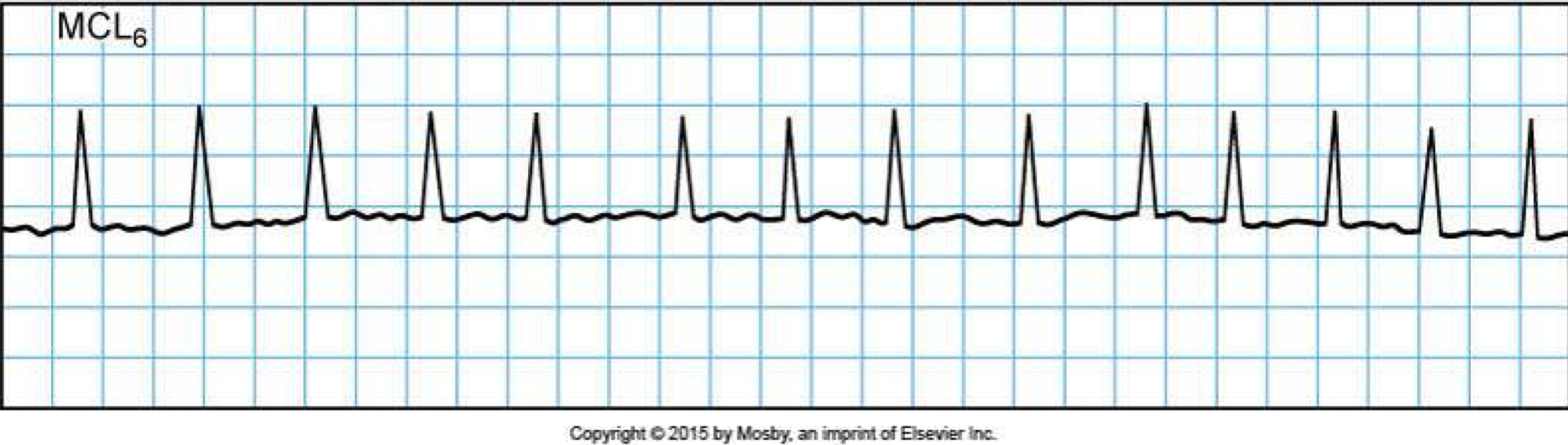
Sinus bradycardia
<60 bpm HR
slow but normal EKG
good cardiovascular conditioning, drugs, heart block
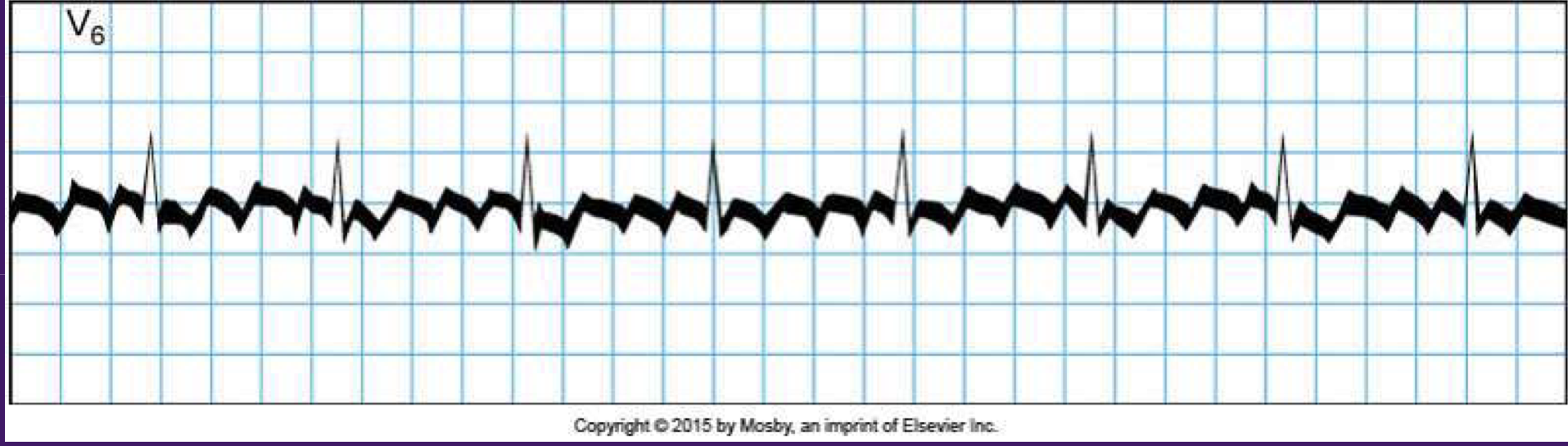
Atrial fibrillation
quivering/irregular HR
irregular spasms of atria w/NO P waves
lead to blood clots, stroke, HF
fluttering feeling in chest

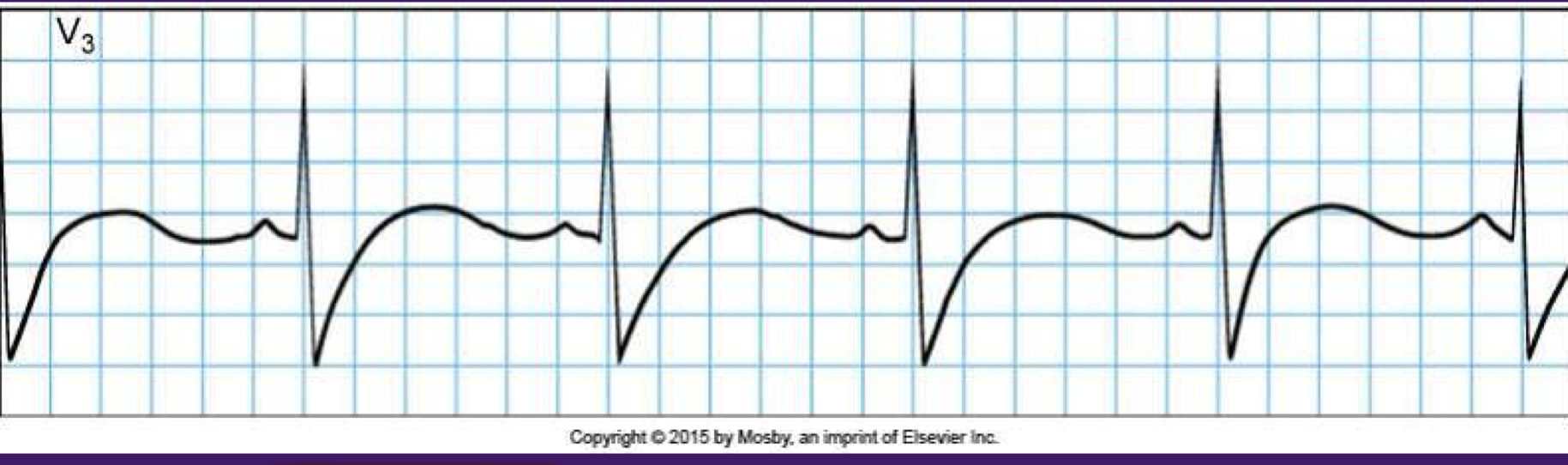
Heart block - 1st degree
PR interval longer than 0.20 sec
benign and asymptomatic
etiology - intrinsic AVN disease, enhanced vagal tone, acute MI, myocarditis, hypokalemia, hypomagnesmia
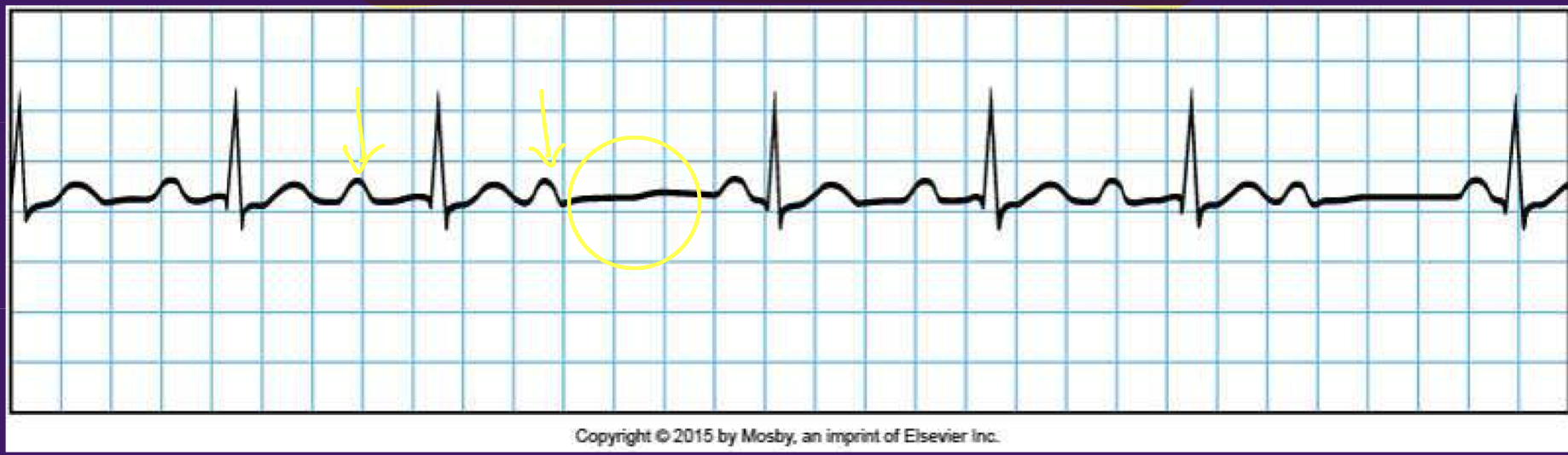
Heart block - 2nd degree type 1 (Wenckenbach/Mobitz 1)
benign
PR interval increases with each beat until a QRS is missed
due to conduction block at AV node
Heart block - 2nd degree type 2 (Mobitz 2)
PR interval stays the same but QRA complex dropped
failure of conduction of
Palpable and sometimes visible arterial pulses are the result of
ventricular systole (pressure wave)
Time it takes for wave to be felt in dorsal pedis + RBC migration
takes 0.2 sec for wave to be felt in dorsal pedis
takes 2 sec for RBC to travel same distance
The activity of the right side of the heart is transmitted back through the
jugular veins as a pulse (visualized only)
three peaks and two descending slopes
Jugular venous pulse components - a wave
result of a brief backflow of blood to vena cava during right atrial contraction
Jugular venous pulse components - c wave
transmitted impulse from vigorous backward push produced by closure of tricuspid valve during ventricular systole
Jugular venous pulse components - v wave
caused by increasing volume and concomitant increasing pressure in right atrium
after c wave in late ventricular systole
Jugular venous pulse components - x slope
caused by passive atrial filling
Jugular venous pulse components - y slope
reflects the open tricuspid valve and the rapid filling of ventricle
Ductus arteriosus closes in first
12-14hrs of life
Foramen ovale closes after
pressures shift
In pregnant women, what happens to their blood pressure
decreases
Aterial walls in older adults
lose elasticity and vasomotor tone
Pulse amplitude characteristics
+0 = absent, not palpable
+1 = diminished, barely palpable
+2 = expected
+3 = full, increased
+4 = bounding, aneurysmal
Three P’s of occlusion
pain
pallor
pulselessness
Pain that results from muscle ischemia in PAD
claudication
Normal BP
<120 mmHg systolic
AND
<80 mmHg diastolic
Elevated BP
120-129 mmHg systolic
AND
<80 mmHg
HTN Stage 1
130-139 mmHg systolic
OR
80-89 mmHg diastolic
HTN stage 2
>140 mmHg systolic
OR
>90 mmHg diastolic
Can the jugular venous pressure be palpated
NO! - Only visualized
Measuring jugular venous pressure
horizontally from meniscus of top of blood column
vertically from the sternal angle
add 5 cm
Jugular venous pressure should be less than
9cm (more = sign of HF)
Hepatojugular reflux is a sign of
right sided HF
Central venous pressure (hand veins) grading
before sternal angle = low venous pressure
at sternal angle = normal venous pressure
above sternal angle = high venous pressure
Homan sign
calf pain with passive dorsiflexion of the foot
Edema grading
+1 = slight pitting, disappears rapidly, 2mm
+2 = deeper pitting, disappears in 10-25 sec, 4 mm
+3 = noticeably deeper, last 60 sec, 6 mm
+4 = very deep, lasts 2-5 min, 8mm or more
Brawny edema
non-pitting edema of chronic venous insufficiency
Capillary refill should be
less than 2 seconds
What is common in children
venous hum (using bell)
turbulence of blood flow in internal jugular veins
Venous thrombosis occurs less commonly in children and is most often associated with placement of
venous access devices (port in chest)
HTN in children is most commonly caused by
kidney/renal disease, coarctation, or phenochromocytoma
Pregnant women vascular changes
CO increases
jugular a and v waves easier to see (pressure remains normal)
BP decreases
What should you tell older adults to do to decrease their blood pressure
exercise
What part of the stethoscope do you use to detect bruits
bell
Alternating pulse (pulsus alternans) cause
left ventricular failure
Pulsus bisferiens cause
aortic stenosis combined with aortic insufficiency
Bigeminal pulse cause
disorder of rhythm
Large, bounding pulse cause
exercise, anxiety, fever, hyperthyroidism, atherosclerosis
Paradoxic pulse (pulsus paradoxus) cause
premature cardiac contraction
tracheobronchial obstruction
bronchial asthma
emphysema
pericardial effusion
constrictive pericarditis
Water-hammer pulse (Corrigan pulse)
patent ductus arteriosus
aortic regurgitation
Temporal arteritis (giant cell arteritis)
inflammation of branches of aortic arch (including temporal arteries)
ischemia of masseter, tongue, optic nerve (tongue and jaw pain)
>50 adults
polymyalgia rheumatica of hips, neck, shoulders
headache in temporal region on one or both sides
Arterial aneurysm
1.5x the normal diameter
4x more common in men
severe ripping pain (mid-back pain = thoracic aorta)
bruit over aneurysm
How can you see an aneurysm on an x-ray
calcifications on the LEFT side
Arteriovenous fistula
congenital or acquired via catherization
may result in aneurysmal dilation
continuous bruit/thrill over area
edema may develop in involved extremity
Peripheral artery disease (PAD)