The History of Neurologic Rehabilitation
1/59
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
60 Terms
What are the 4 neuromuscular facilitation single approaches?
Brunnstrom
NDT
PNF
Rood
What is the main Brunnstrom's Approach principle?
stroke recovery is predictable and progresses through identifiable stages
What are the 6 stroke progression stages in Brunnstrom's Approach?
1. Extremities are flaccid (no movement and decreased tone)
2. Spasticity begins to develop, gradual voluntary movements
3. Voluntary movements through partial ROM of synergy pattern
4. Begin to move out of synergy, spasticity starts to decline
5. Synergies lose dominance
6. Isolated movement is possible, coordination near normal
What is an abnormal synergy pattern present after stroke?
involuntary, stereotypical muscle linkages that prevent isolated joint movement
What is the abnormal post-stroke flexor synergy pattern for the upper extremity?
Scapula: retraction and elevation
Shoulder: abd and ER
Elbow: flex - what initiates synergy to happen
Forearm: supination
Wrist: flex
Fingers/thumb: flex and add
What is the abnormal post-stroke extension synergy pattern for the upper extremity?
Scapula: protraction and depression
Shoulder: add (initiates synergy to happen), IR
Elbow: extension
Forearm: pronation (initiates synergy to happen)
Wrist: flex or ext
Fingers/thumb: flex and add
What is the abnormal post-stroke flexion synergy pattern for the lower extremity?
Pelvis: elevation and retraction
Hip: flex (initiates synergy), abd, ER
Knee: flex
Ankle: DF and inv
Toe: DF
What is the abnormal post-stroke extension synergy pattern for the lower extremity?
Hip: ext, add (initiates synergy), IR
Knee: ext (initiates synergy)
Ankle: PF (initiates synergy) and inv
Toes: PF
What treatment does Brunnstrom emphasize?
embrace synergies through early recovery and use them to aid in regaining voluntary motor control
Issue with using synergies as a treatment method
difficult to unlearn due to neuroplasticity so only practicing synergies leads to only being able to move in synergies and difficulty in initiating isolated movement
What is the modern shift of the Brunnstrom Approach
dynamic systems theory
What is the view of the dynamic systems theory?
movement emerges from multiple interacting systems rather than single hierarchy
What is the foundation of Neurodevelopmental Treatment (NDT)/Bobath approach?
1. learn normal movement patterns through functional activity
2. reflex mechanisms are central to how movement is organized and relearned
What treatment is emphasized in the NDT/Bobath approach?
manual contact at key points of control is used to facilitate or inhibit movement
What are the goals of the Proprioceptive Neuromuscular Facilitation (PNF) approach?
1. Increase patient's ability to move or remain stable
2. Achieve coordinated, functional movement
3. Build stamina and manage fatigue
PNF Movement Patterns: UE D1 Flexion
flex/add/ER
scapula: anterior elevation

PNF Movement Patterns: UE D1 Extension
ext/abd/IR
scapula: posterior depression

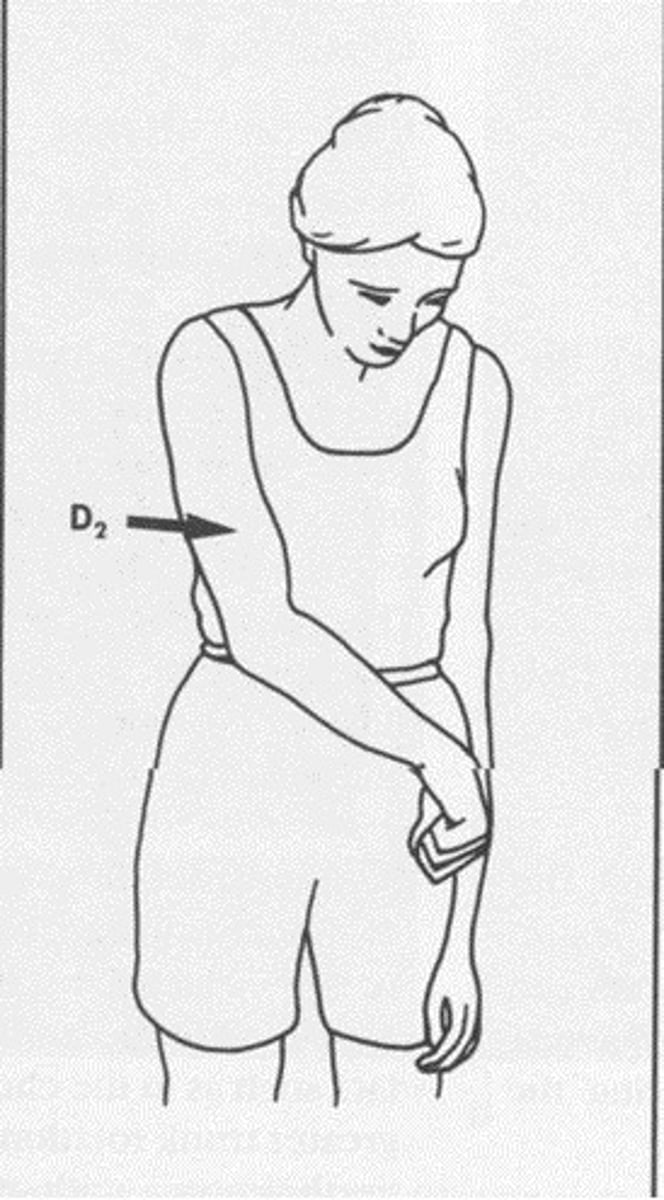
PNF Movement Patterns: UE D2 flexion
flex/abd/ER
scapula: posterior elevation

PNF Movement Patterns: UE D2 extension
ext/add/IR
scapula: anterior depression
PNF Movement Patterns: LE D1 flexion
flex/add/ER
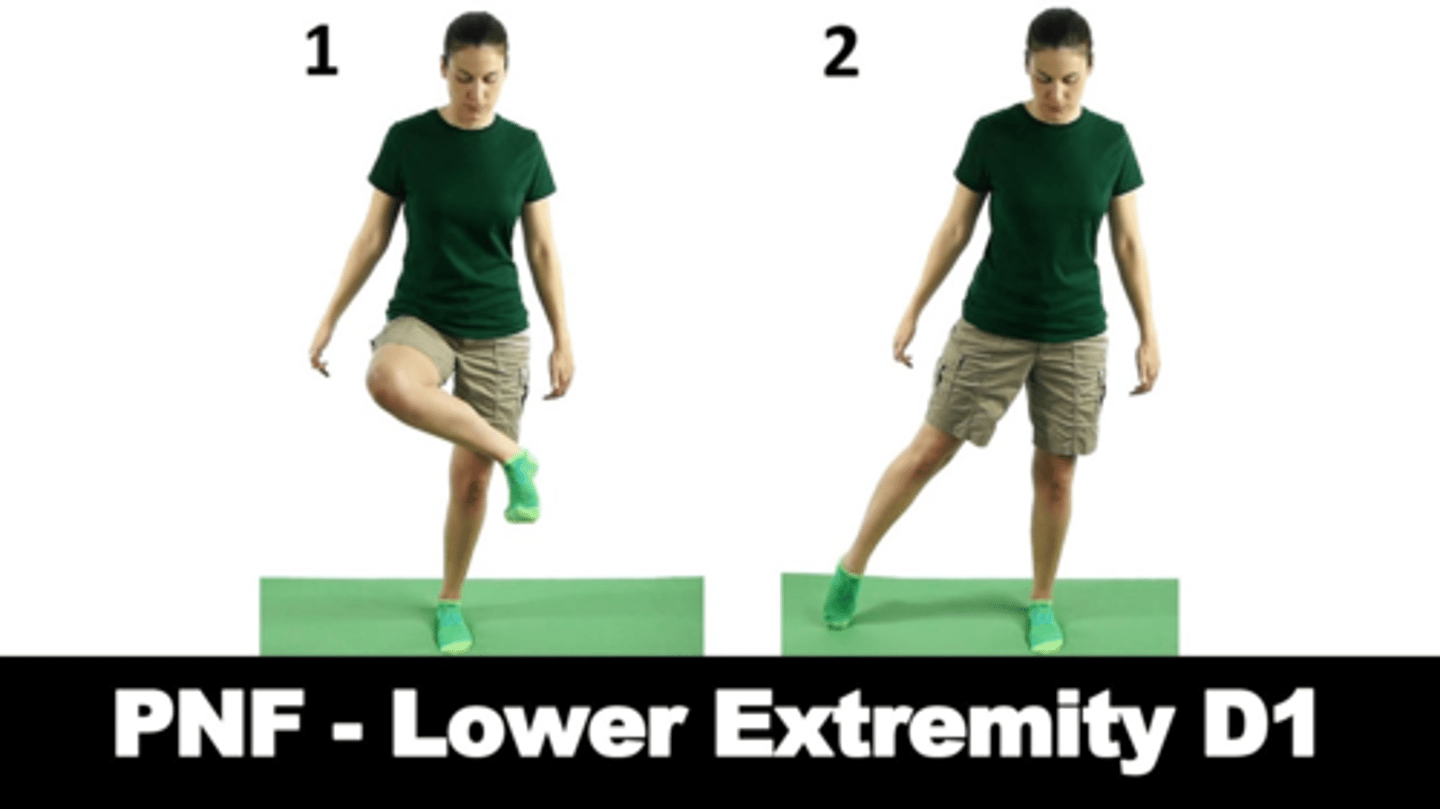
PNF Movement Patterns: LE D1 extension
ext/abd/IR
PNF Movement Patterns: LE D2 flexion
flex/abd/ER
PNF Movement Patterns: LE D2 extension
ext/add/IR
PNF Techniques
Rhythmic Initiation
Agonist Reversals
Repeated Contractions
Slow reversals
Alternating Isometrics
Rhythmic Stabilization
Contract-Relax Active Movement
Hold Relax
Rhythmic Initiation
PROM --> AAROM --> AROM --> resisted ROM
Purpose of Rhythmic Intitiation
initiate movement
facilitate improvement in speed, direction, quality of movement
Agonist Reversal
concentric --> eccentric --> concentric contractions of agonist muscle repeated
Purpose of Agonist Reversals
increase joint ROM
improve strength and coordination of movement
Repeated Contractions
isotonic contraction of agonist
Purpose of Repeated Contractions
increase AROM, strength, and endurance of agonist
relaxation of antagonist
Slow Reversals
concentric contractions of antagonist muscle groups without relaxation between reversals
Purpose of Slow Reversals
increase agonist motion
strengthen agonist/antagonist
Alternating Isometrics
isometric of agonist than antagonist
Purpose of Alternating Isometrics
increase isometric strength of postural muscles of trunk and proximal muscles
Rhythmic Stabilization
simultaneous isometric of agonist/antagonist
Purpose of Rhythmic Stabilization
improve postural control, balance, and stability in various functional, WB positions
Contract Relax
PROM of limb to ROM limitation in the agonist pattern and then a max iso contraction of antagonist is performed and resisted
Purpose of Contract Relax
relaxation of muscles antagonist to active muscle group to increase ROM into agonist movement pattern
Hold Relax
iso contraction of muscle then relaxation and elongation during relaxation phase
Purpose of Hold Relax
relaxation and increased ROM
What is the main principle of the Rood Approach?
sensory stimulus is used to determine/drives motor responses
Sensory Stimulation Techniques Involved in the Rood Approach
light touch
tapping
quick stretch
quick ice
traction
approximation
resistance
prolonged stretch
deep pressure
neutral warmth
slow stroking
prolonged cold
Application of Light Touch
quick light strokes over muscle using either fingers, cotton, or a brush to facilitate contraction of underlying muscle
Application of Tapping
brisk taps with fingertips over tendon or muscle belly of involved muscle to facilitate phasic contraction of muscle
Application of Quick Stretch
A quick over elongation of a muscle (often applied at its lengthened range) facilitates contraction of the muscle.
Application of Quick Ice
quick stroking with ice on the skin over the muscle belly facilitates contraction of the underlying muscle
Application of Traction
manually applied distraction force to a joint or limb segment causes muscle relaxation and promotes movement
Application of Approximation
Compression of a joint or body segment stimulates co-contraction of muscles around the body segment and promotes stability
Application of Resistance
manual application of force away from the axis of motion at the joints as the patient is asked to move or to stabilize
Application of Prolonged Stretch
slow passive lengthening of a muscle to inhibit its contraction
Application of Deep Pressure
manual pressure across longitudinal axis of the muscle tendon causes relaxation of the muscle
Application of Neutral Warmth
wrapping of body or limb in blanket, towel, or air splint for purpose of general relaxation
Application of Slow Stroking
slow stroking with the hand along midline of the back, near the posterior rami, for 3 to 5 min leads to calming of the patient
Application of Prolonged Cold
application of an ice pack or ice massage over a muscle leads to its relaxation and reduction of pain
What 2 systems does the Rood Approach believe neuromuscular function is organized around?
mobility and stability
Mobility System Characteristics
light work
phasic muscles - on/off, concentric/eccentric
Stability System Characteristics
heavy work
tonic muscle - sustained/postural muscles
What are the 2 sequences for organizing treatment progression in the Rood Approach?
vital function sequence - foundational physiologic functions (like responsiveness)
skeletal function sequence - movement and postural control
What are the 4 levels of motor control in the Rood Approach?
1. Mobility - free active motion that translates body through space
2. Stability - fixes body part to allow for WB
3. Controlled mobility - WB position where proximal part moves on fixed distal part
4. Skill - non-WB position where free distal part is moving
What is the main principle of modern neurorehabilitation?
practice function do not just treat impairments (principle of specificity - practice makes perfect, so if you want to progress function practice function)