Quiz 10: Biomedical Sciences (Anderson - Sexual Dysfunction + Menopause)
1/142
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
143 Terms
What are common purposes of human sexual activity?
intimacy, reproduction, pleasure, stress relief, and bonding
Physiologic response
automatic body response to sexual stimuli
Desire
wanting sexual activity
Pleasure
enjoyment of sexual activity
What are the 4 phases of the physiologic sexual response cycle?
excitement, plateau, orgasm, and resolution; male and females have the same 4 phases
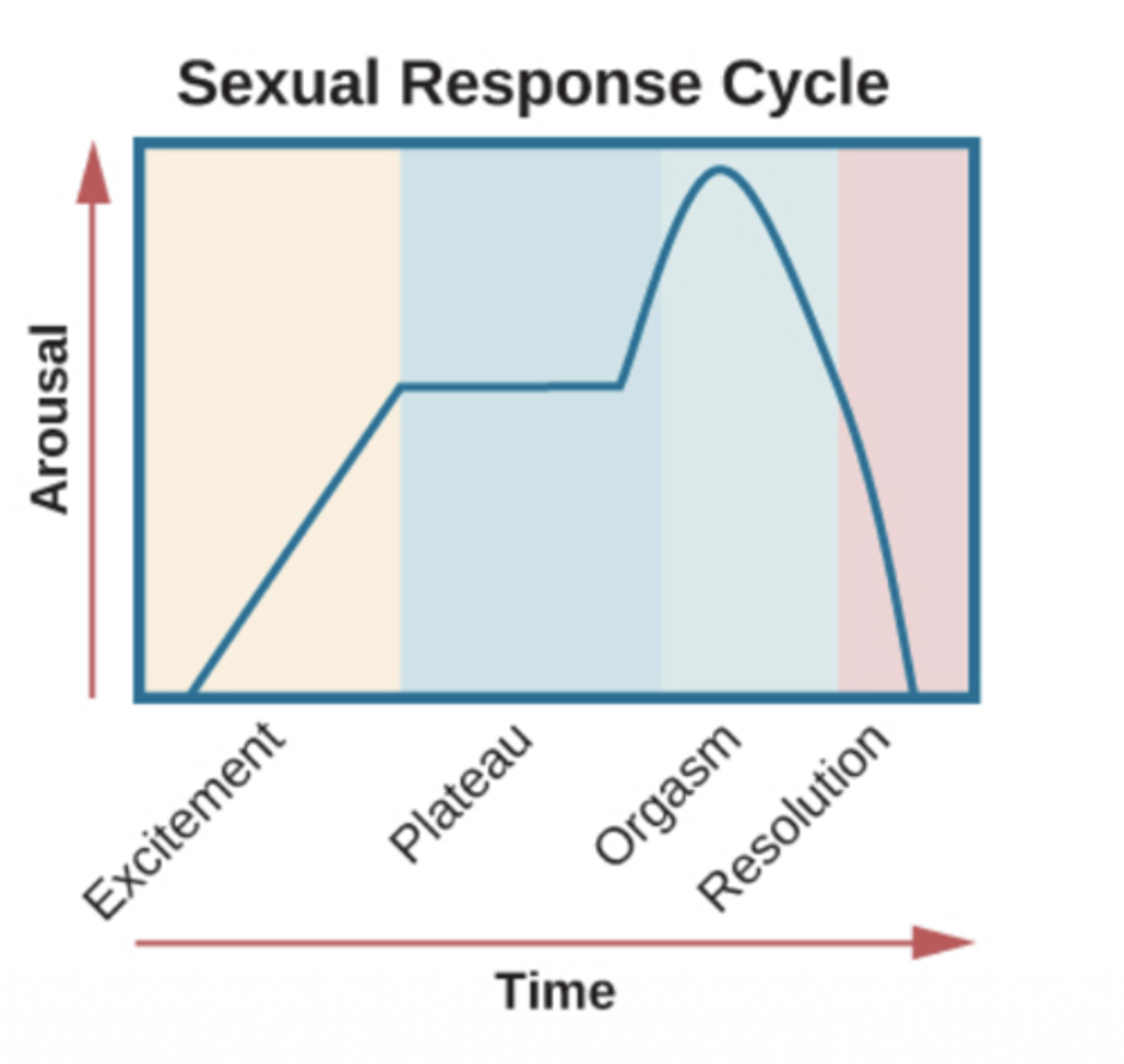
What occurs during the excitement and plateau phases?
arousal rises during excitement and is maintained during plateau
What is a key difference between male and female sexual response cycles?
males have a refractory period after orgasm; females may have multiple response patterns
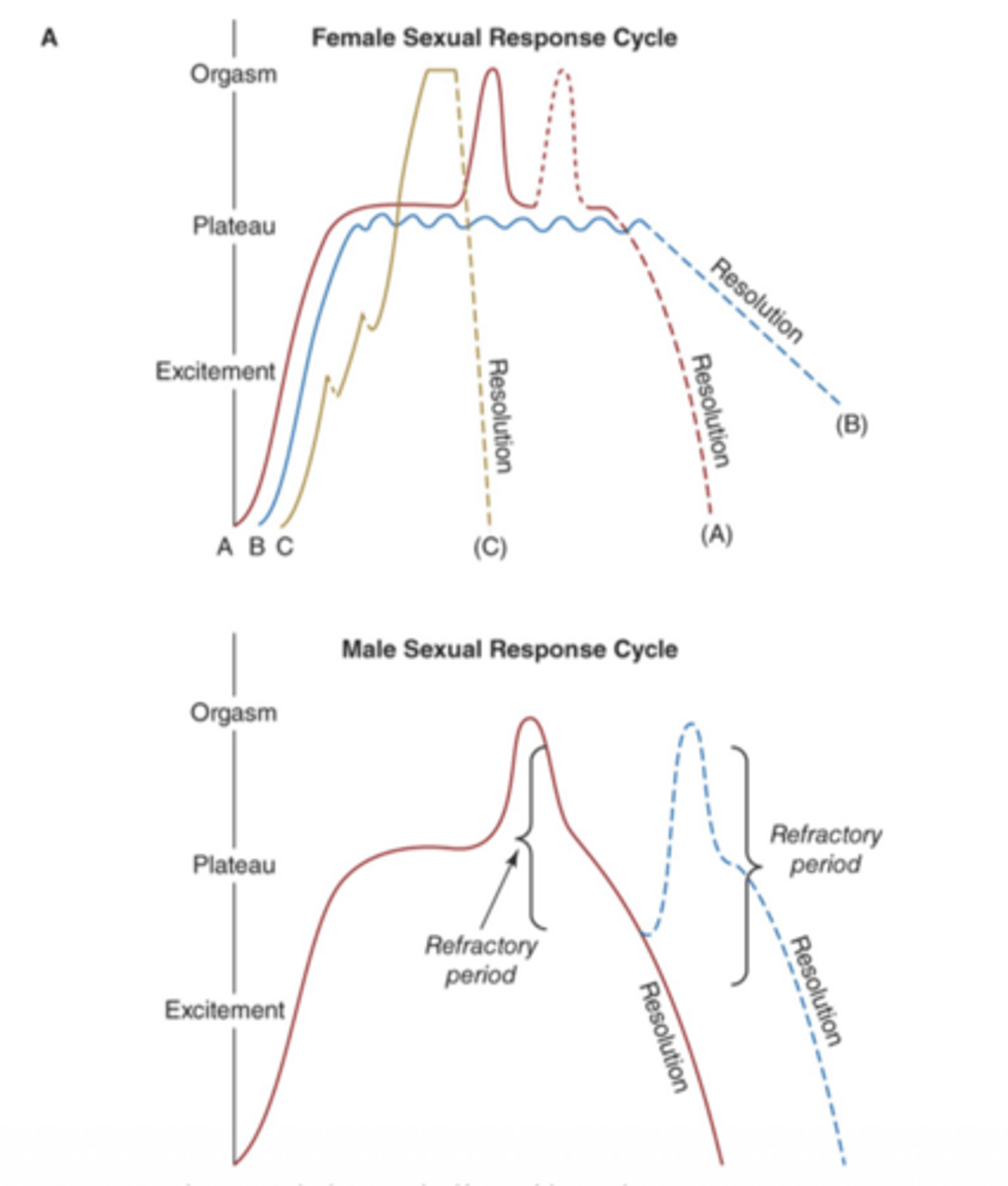
What is the refractory period?
a time after orgasm when sexual excitement is difficult to initiate again
What two types of innervation mediate erectile response?
psychogenic (central) and reflexogenic (peripheral) innervation
What is the difference between psychogenic and reflexogenic sexual responses?
psychogenic responses originate from the brain; reflexogenic responses result from direct genital stimulation via spinal reflexes
Which hormones positively affect central sexual desire and function?
testosterone, progesterone, and estrogens
What sexual functions require the CNS?
desire, excitement, and orgasm
What functions require the peripheral nervous system in sexual activity?
sensation, vasocongestion, and erectile tissue function
How do testosterone and estrogens affect peripheral sexual tissues?
they maintain genital structure and support erectile tissue function
What is vasocongestion?
blood vessel dilation and engorgement during sexual response
What physiologic effects are associated with vasocongestion?
erectile tissue engorgement, secretions/lubrication, and flushing
What is myotonia during sexual response?
increased voluntary and involuntary muscle tension
What changes occur with myotonia?
muscle tension, nipple erection, vaginal dilation, uterine elevation, ↑ BP, ↑ HR, and ↑ respiratory rate
What characterizes the orgasm phase?
peak intensity of physiologic sexual response resulting in orgasm
What physiologic events occur during orgasm?
rhythmic pelvic muscle contractions, ejaculation, euphoria, and intense pleasure
What are the 6 broad categories of sexual dysfunction?
desire, arousal, erectile, orgasm, ejaculation, and pain disorders
When does a sexual dysfunction officially exist?
only when it causes personal distress or pain
What are common causes of sexual dysfunction?
hormonal changes, injury, stress, depression, anxiety, fatigue, trauma, disease, medications, etc.
What is required for normal male sexual function?
libido, erection/tumescence, sympathetic outflow for orgasm, ejaculation, and detumescence
What are major categories of male sexual dysfunction?
hypoactive sexual desire disorder, erectile dysfunction, ejaculatory/orgasmic disorders, and pain disorders
What are treatments for male sexual dysfunction?
communication, therapy, stimulation devices, hormonal therapy, ED drugs, and premature ejaculation drugs
How are male and female erectile tissues related?
they are homologous and structurally very similar
What erectile tissues are homologous between males and females?
corpus spongiosum in males and vestibular bulbs in females
What is the function of the corpus cavernosum?
it fills with blood to produce penile erection
Where do erection and ejaculation innervation originate?
lower spinal cord regions
Are erection and ejaculation controlled by the same neurons?
No, they are controlled by different neuronal pathways
How does spinal cord injury affect male sexual response?
reflexogenic erections may remain intact, but psychogenic responses may be lost
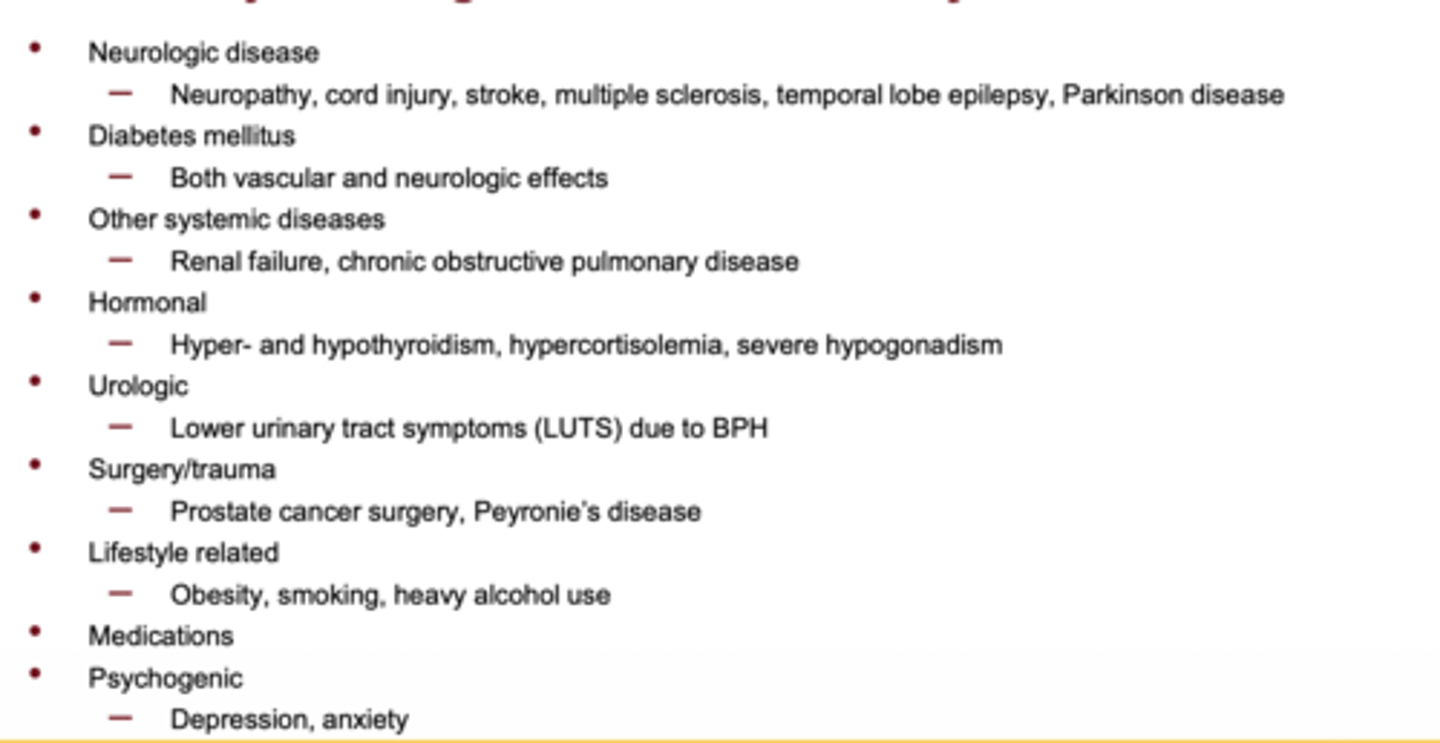
What are major causes of male erectile dysfunction?
neurologic disease, diabetes, systemic disease, hormonal disorders, BPH/LUTS, surgery/trauma, obesity/smoking/alcohol, medications, depression, and anxiety
How do PDE5 inhibitors treat erectile dysfunction?
PDE5 inhibition ↑ cGMP → smooth muscle relaxation → blood trapping in erectile tissue (tumescence)
What is detumescence?
reversal of erection back to the flaccid state
How do topical anesthetics treat premature ejaculation?
they numb the penis and prolong time to orgasm
How do SSRIs help premature ejaculation?
they inhibit psychogenic signaling required for orgasm and ejaculation
What factors influence sexuality in aging adults?
relationships, social changes, mental health, and declining sex hormones
What sexual response changes occur in aging males?
longer plateau/refractory periods, decreased rigidity, lower ejaculatory volume, weaker contractions, faster detumescence, and less defined orgasm
How does testosterone therapy affect male sexual function?
improves psychogenic desire, erections, intercourse, and satisfaction
What is required for normal female sexual function?
libido, sensation, sympathetic outflow for orgasm, and vaginal lubrication
What are major categories of female sexual dysfunction?
hypoactive desire, hypoactive arousal, anorgasmia/delayed orgasm, and dyspareunia
What are common treatments for female sexual dysfunction?
communication, therapy, lubricants, stimulation devices, hormonal/SERM therapy, and medications for hypoactive sexual desire disorder
What are the top 3 sexual problems in older females?
pain during intercourse, inability to climax, and difficulty with lubrication
What post-menopausal genital tract changes contribute to sexual dysfunction?
decreased blood flow, thinning/drying of vaginal lining, narrowing, loss of elasticity, and decreased lubrication
What symptoms can result from post-menopausal genital tract changes?
vaginal dryness, soreness, itching, painful intercourse, and spotting
How are post-menopausal sexual dysfunction symptoms treated?
lubricants, estrogen/SERM therapy, and addressing pain/dyspareunia causes
What role does estrogen play in vaginal tissue health?
maintains vaginal lubrication, thickness, elasticity, rugae, width, and length; all decrease with long-term estrogen loss
How can vaginal atrophy contribute to sexual dysfunction?
causes dryness, painful intercourse (dyspareunia), irritation, and reduced sexual activity
What is the role of the female pelvic floor?
supports pelvic organs and contributes to normal sexual function
How do pelvic floor disorders affect sexual activity in post-menopausal females?
pelvic floor changes and low estrogen can reduce sexual activity and contribute to dysfunction/pain
What is female hypoactive sexual desire disorder (HSDD)?
persistently low sexual desire causing distress/interpersonal difficulty and not explained by psychiatric illness, relationship problems, medical conditions, or substances
What drug is approved for treatment of HSDD in premenopausal women?
flibanserin (Addyi)
How does flibanserin work in HSDD?
alters CNS neurotransmitters by ↑ dopamine/norepinephrine and ↓ serotonin to improve sexual desire
How do testosterone and bremelanotide help treat HSDD?
Testosterone → improves libido/sexual desire
Bremelanotide → melanocortin receptor agonist that increases dopamine signaling related to sexual response
What is menopause?
final phase of female reproductive ability marked by cessation of menstruation
When does menopause officially occur?
12 months after the last menstrual period (FMP)
What is the average age of menopause and perimenopause onset?
menopause ≈ 51 years; perimenopause begins in the 40s (average onset 47)
What marks the beginning of postmenopause?
FMP + 12 months of amenorrhea
How does the menstrual cycle change with reproductive aging?
cycles become variable, irregular, skipped, and eventually absent
What menstrual changes occur during menopausal transition?
shorter cycles, possible long cycles, and irregular bleeding
What are common vasomotor symptoms of menopause?
hot flashes, night sweats, and sleep disturbances
What psychological symptoms may occur during menopausal transition?
depression, irritability, mood swings, poor concentration, and poor memory
What other somatic/physical symptoms may occur with menopause?
headache, dizziness, palpitations, breast pain, joint/back pain, urinary incontinence, dry skin, and weight gain
What characterizes the menopausal ovary microscopically?
atretic follicles with loss of primordial follicles
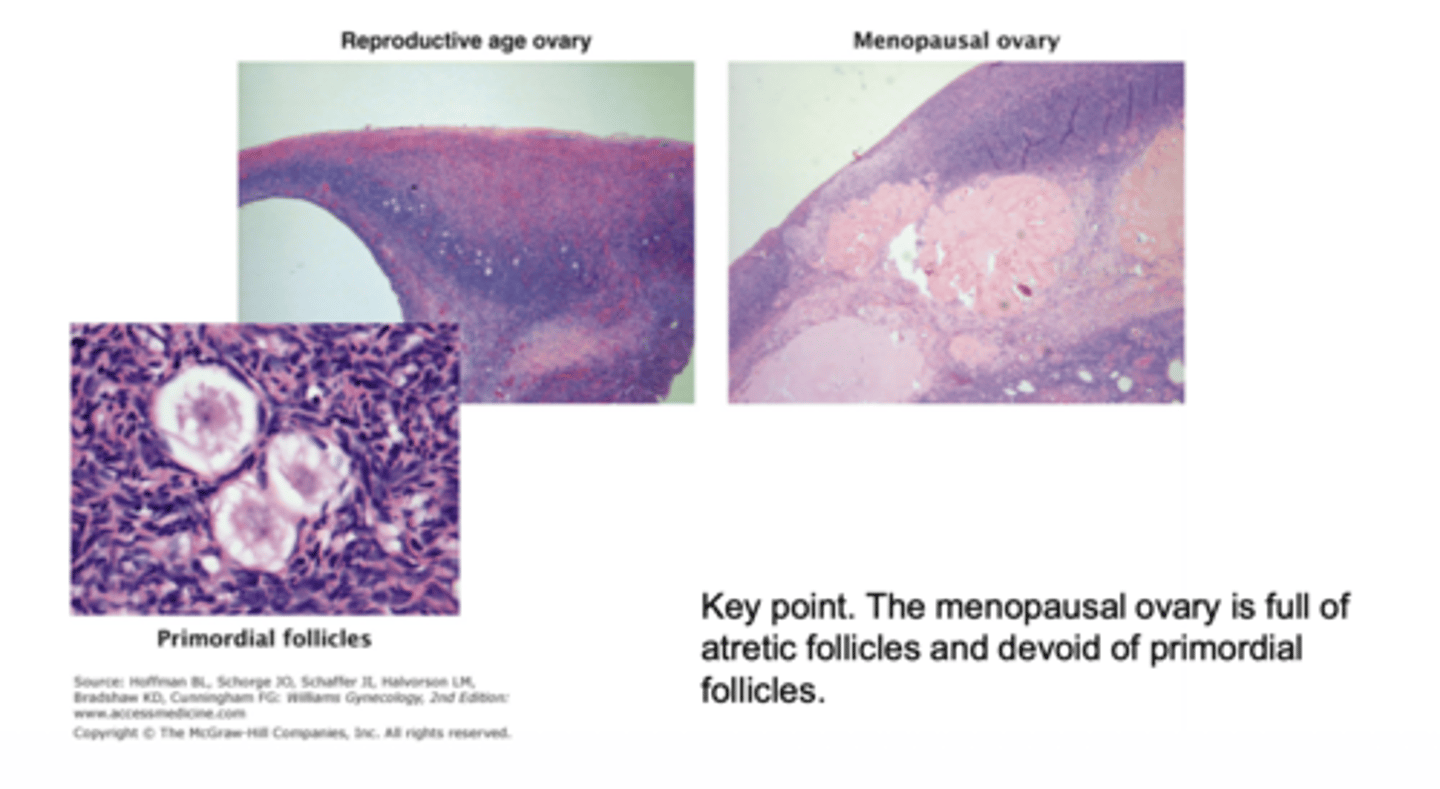
How do primordial follicles change with aging?
they progressively decline and depletion accelerates approaching menopause
What happens after primordial follicle depletion?
the ovary no longer significantly produces estrogen
What hormonal changes occur during menopausal transition?
dysregulated GnRH, ↑ FSH/LH, and ↓ estrogen production
What drives accelerated follicle loss during menopause?
elevated FSH stimulates excessive follicular recruitment/development
How do FSH levels change in women over age 45?
FSH levels become elevated
How do LH and estrogen levels change approaching menopause?
LH peaks are lower/altered and estrogen levels decline (especially in females ≥ 45)
What happens to estrogen and testosterone after menopause/oophorectomy?
levels fall significantly but do not disappear completely
How are estrogens still produced after ovarian failure?
adrenal androstenedione is converted to estrogens in adipose tissue via aromatase
What happens to inhibin B during menopausal transition?
inhibin B decreases
Why does declining inhibin B accelerate menopause?
less inhibition of follicular development → more follicle recruitment → faster follicle depletion
What happens to the endometrium after menopause?
it becomes atrophic
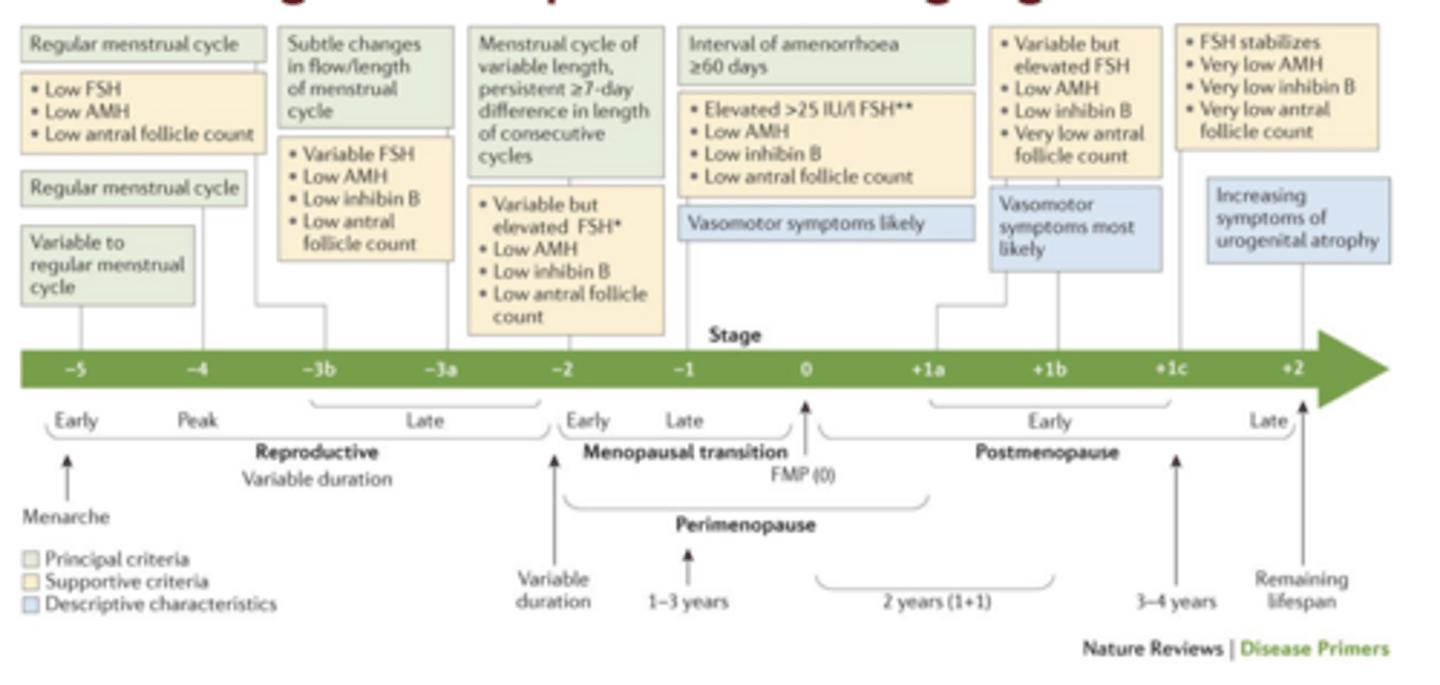
Stages of Reproductive Aging in Females
What hormone changes persist after menopause?
↑ GnRH/LH/FSH and ↓ ovarian estradiol/progesterone
What tissue becomes the major site of estrogen production after menopause?
adipose tissue
What tissues are physiologically affected by estrogen?
uterus, ovary, breast, liver, CNS, and bone.
What are major physiologic effects of estrogen?
endometrial proliferation, breast ductal growth, metabolic modulation, neuroprotection, and bone maintenance
What physiologic changes occur during a hot flash?
rapid changes in core temperature, skin temperature, perspiration, and respiratory exchange
Are vasomotor symptoms experienced by all menopausal females?
No, severity and occurrence vary greatly
What causes vasomotor symptoms during menopause?
altered hypothalamic thermoregulatory set point
How do SSRIs improve vasomotor symptoms?
increase serotonin at synapses to help normalize thermoregulation
Why are women more vulnerable to osteoporosis after menopause?
declining estrogen/progesterone increase bone resorption
What cellular imbalance causes osteoporosis?
osteoclasts remove more bone than osteoblasts replace
What factors contribute to osteoporosis besides menopause?
genetics, corticosteroids, anticonvulsants, immobilization, and lack of exercise
How does estrogen regulate bone remodeling?
controls osteoclast/osteoblast development and activity
Is estrogen loss the only cause of postmenopausal osteoporosis?
No, aging, inactivity, sarcopenia, vitamin D deficiency, and other factors also contribute
What epithelial changes occur in genitourinary syndrome of menopause (GSM)?
thinning epithelium, exposed capillaries, burning, soreness, bleeding, and dyspareunia
How does menopause alter vaginal pH and flora?
↓ lactic acid → ↑ pH → altered commensal bacteria and infections
What urinary symptoms are associated with GSM?
frequency, urgency, and dysuria
Where are estrogen receptors found in the genitourinary tract?
vulva, vagina, bladder, urethra, pelvic floor musculature, and fascia
What structural vaginal changes occur after menopause?
loss of collagen/fat/water storage, flattened rugae, shrinking walls, and reduced flexibility
What vulvar changes occur with menopause?
atrophy, ↓ secretions, fusion of labia minora, and introital narrowing
How does the postmenopausal vagina differ from the premenopausal vagina?
loss of folds/rugae, thinner lining, and reduced glandular function
How does low estrogen affect the pelvic floor?
pelvic floor dysfunction can lead to prolapse of vagina, bladder, or bowel
Why is estrogen important for pelvic floor integrity?
maintains connective tissue and musculature supporting pelvic organs
How does estrogen affect lipid profiles?
maintains high HDL and lower LDL/total cholesterol