Topic 13 - Cardiac action potential and excitation (contraction coupling)
1/11
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
12 Terms
every ___ in ___ must depolarize
every cell in the atria and ventricles must depolarize so the heart can beat efficeitnly
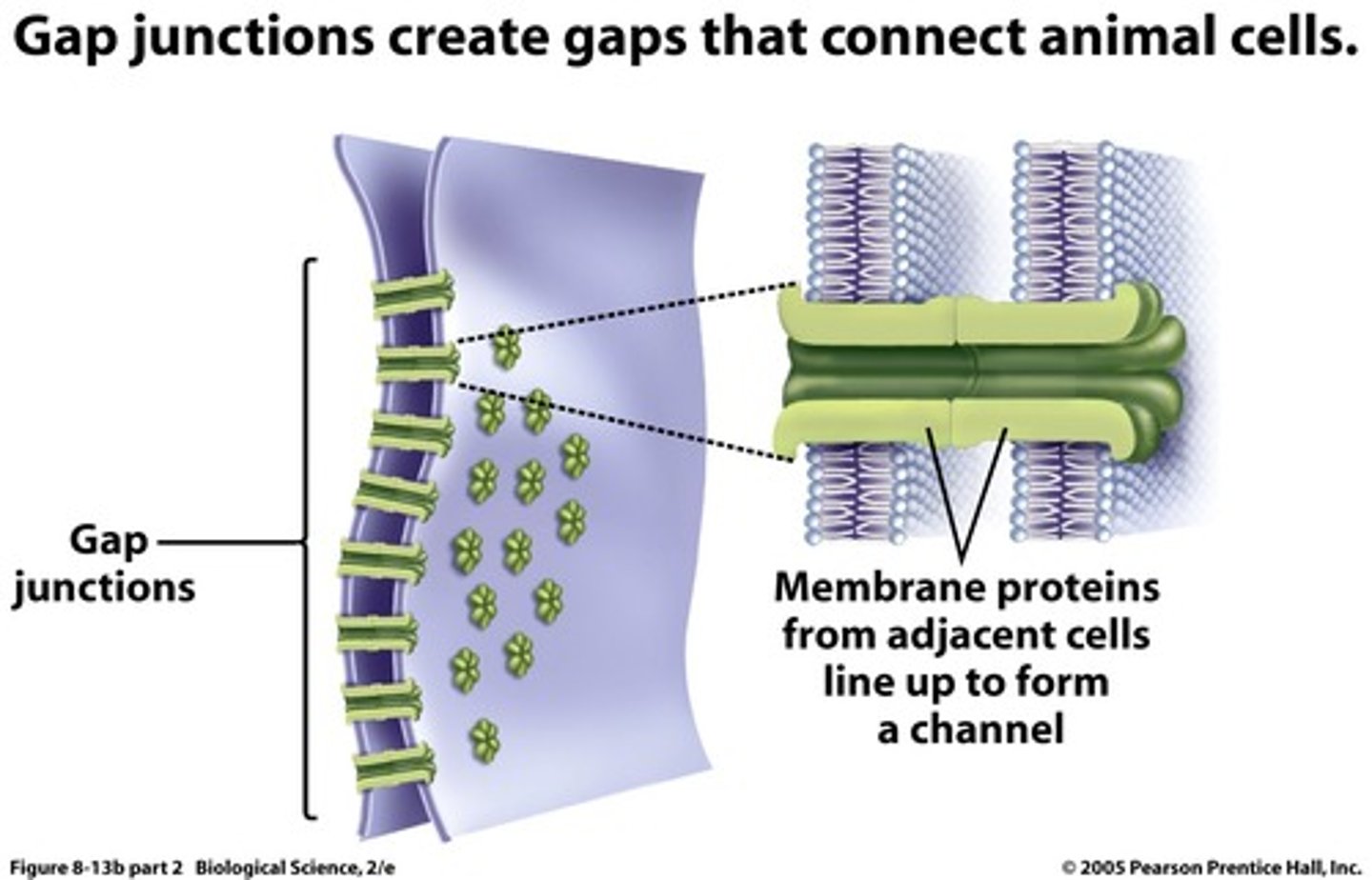
depolarization moves bw the cardiac myocytes
how does depolarization travel bw cardiac myocytes
*Cardiac cells are connected by gap junction channels Present at the lateral endds of the cells to Ensure that all cardiac cells activate simultaneously
how?
1. cell 1 fires action potential causing Na+ and Ca2+ to enter cell
2. (+) ions from Cell 1 diffuse into Cell 2 through gap junctions
3. Membrane potential of Cell 2 becomes more +, triggering action potential
what does action pentials in cardiac muscle cells look like
DIFFERENT FROM PACEMAKER CELL AP
- however also occurs without neural innervation as it gets its AP from neighboring cells thourgh gap junctions
what are the 5 phases of cardiac muscle action potential
phase 4 - resting
phase 0 - depolarization
phase 1 - peak depolarization
pahse 2 - plateau
phase 3 - repolarization
explain each phase of a myocyte AP
phase 4 - resting (-90mV)
- k+ channels are open --> k+ leaves cell
- Na+ from neighboring cells depolarize the cell to threshold (-70mV)
phase 0 - depolarization
- voltage gated FAST sodium channels open --> influx of Na+
phase 1 - peak depolarization (+30mV)
at peak...
- FIRST, fast Na+ channels close
phase 2 - plateau** critcal in myocytes
- instead of quicly repolarizing since the NA channels close --> L-type (long) ca+2 voltage gated chanels open (have a bit of a lag, why we see big dip after peak) --> Ca+ enters the cell
- a minimum amt of K+ is also leaving the cell at th esame time so cell deosnt get more positive
*these two togteher cause a plateau in membrane potential
phase 3 - repolarization
- L-type CA2+ channels close
- more voltage gated K+ channels open --> fast eflux of K+ out the cell --> back to -90mV
The Electrocardiogram (ECG)
cardiac electrical activity as a function of time
- sum of all th the elextricle activites of all the cells in the heaart based on where electrodes are placed
segments of the ECG
Pwave = atrial depolarization
QRS complex = ventricle depolarization
*atrial repolarization is also occuring here but cant see it
T wave = ventricle repolarization
flat portions: minimal electricle activity of the cells i.e.when cells are fully polarized or depolarized as it just catches deviations
- Pq segment = platue of atrial ap
- ST segment = plataeu of ventricular AP
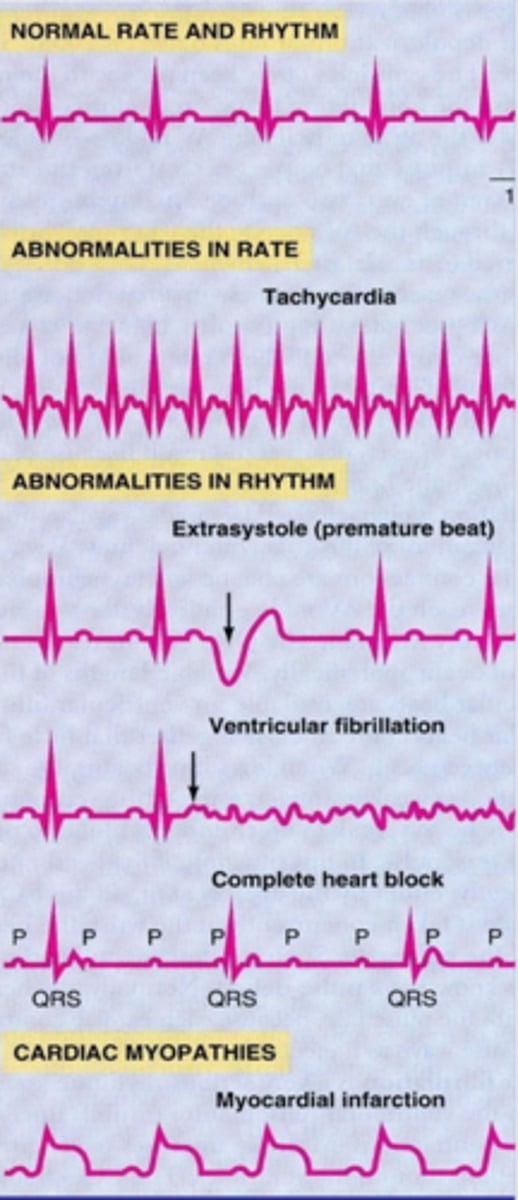
Abnormalitiesz in ECGs
- extrasystole = premature ventricular contraction
- ventricular fibrilation = no excitation of ventricle (no QRS complex)
- complete heart block = seperatrion bw atria and ventricel signals lead to av node acting as its own pacemakr --> dissociation bw P wave and QRS
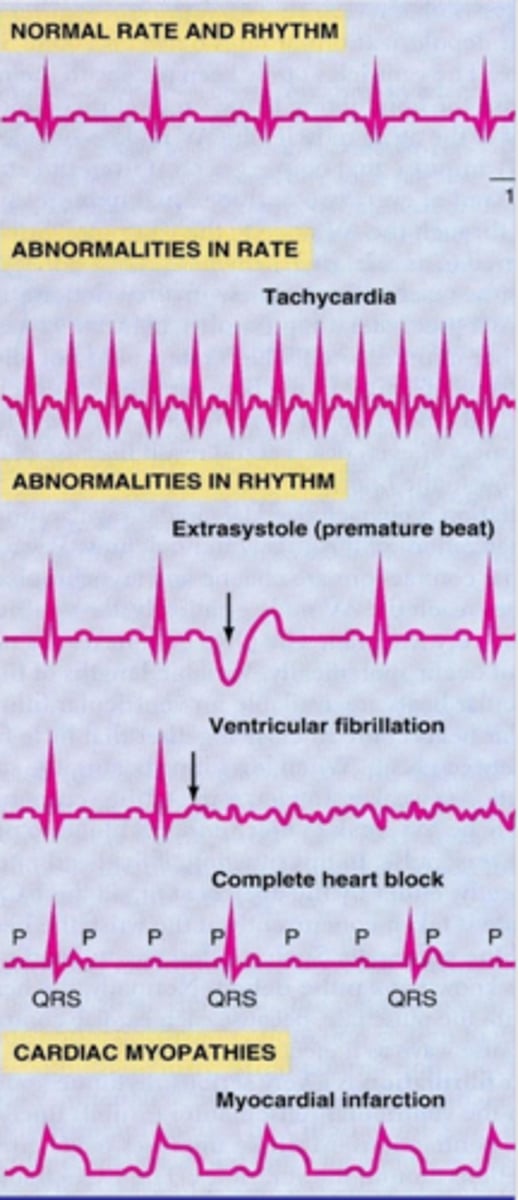
cardiac myopathy ECG
myocardial infarction
- QRS blended w T wave (elevated ST segment) --> tells u theres serve cardiac problems
Membrean depolarization of the heart triggers contraction
- contraction of the heart ocurs DURING the action potnetial (specifically the plateau phase)
- major difference to skeletal muscles which can generate greater force by fusign AP --> tetanus
why does this occur?
--> bc of Ca2+ channels that slow reploarization
--> leads to refractory period: where cell cannot be rexcited to fire a new AP
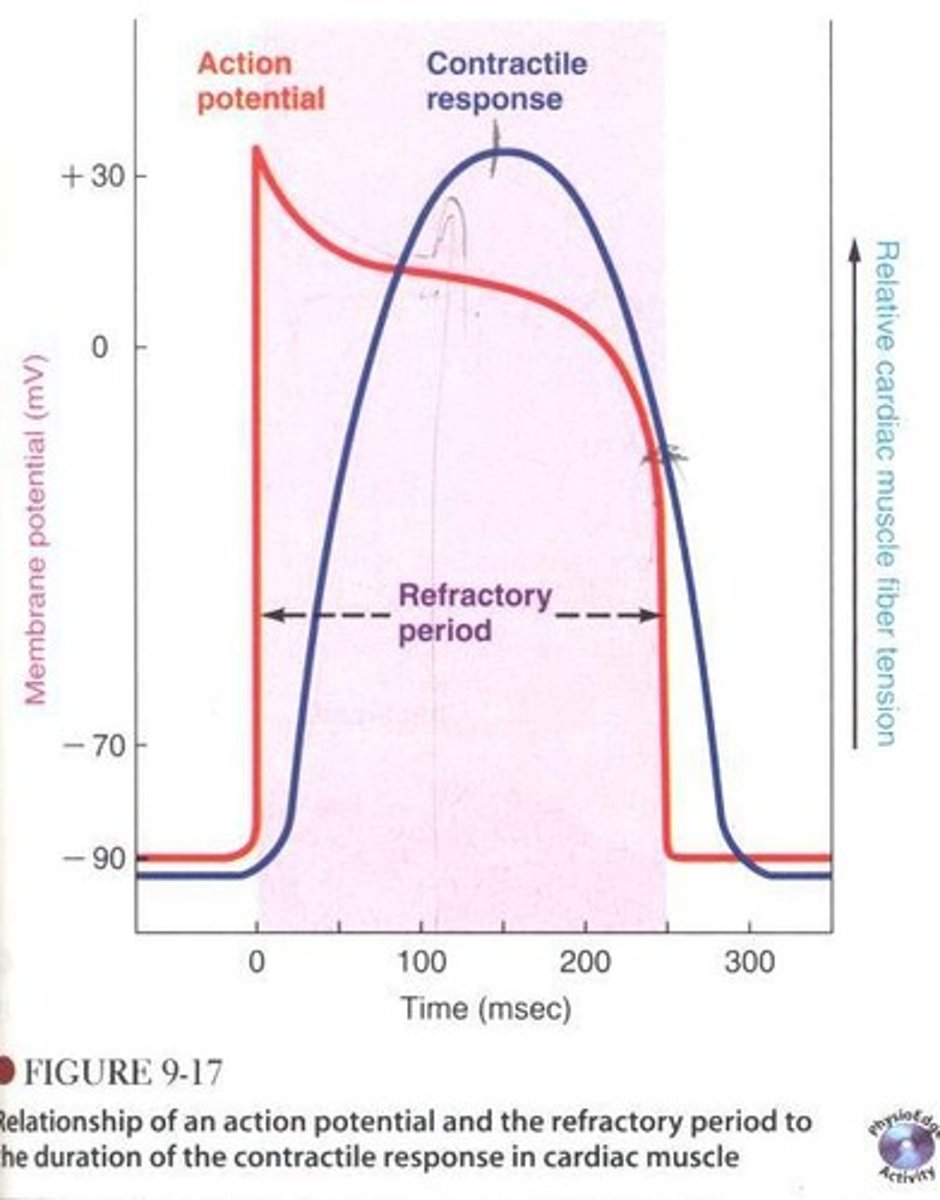
why is cardiac refractory period important
--> so there is NO tetanus so that heart can fill withblood in between contractions
--> to prevent RETROGRADE ACTIVATION via gap junctions: bc there are gap junctions bw myocytes so we dotn what cell 2 to re excite cell 1 which is super unregulated activity and rythym
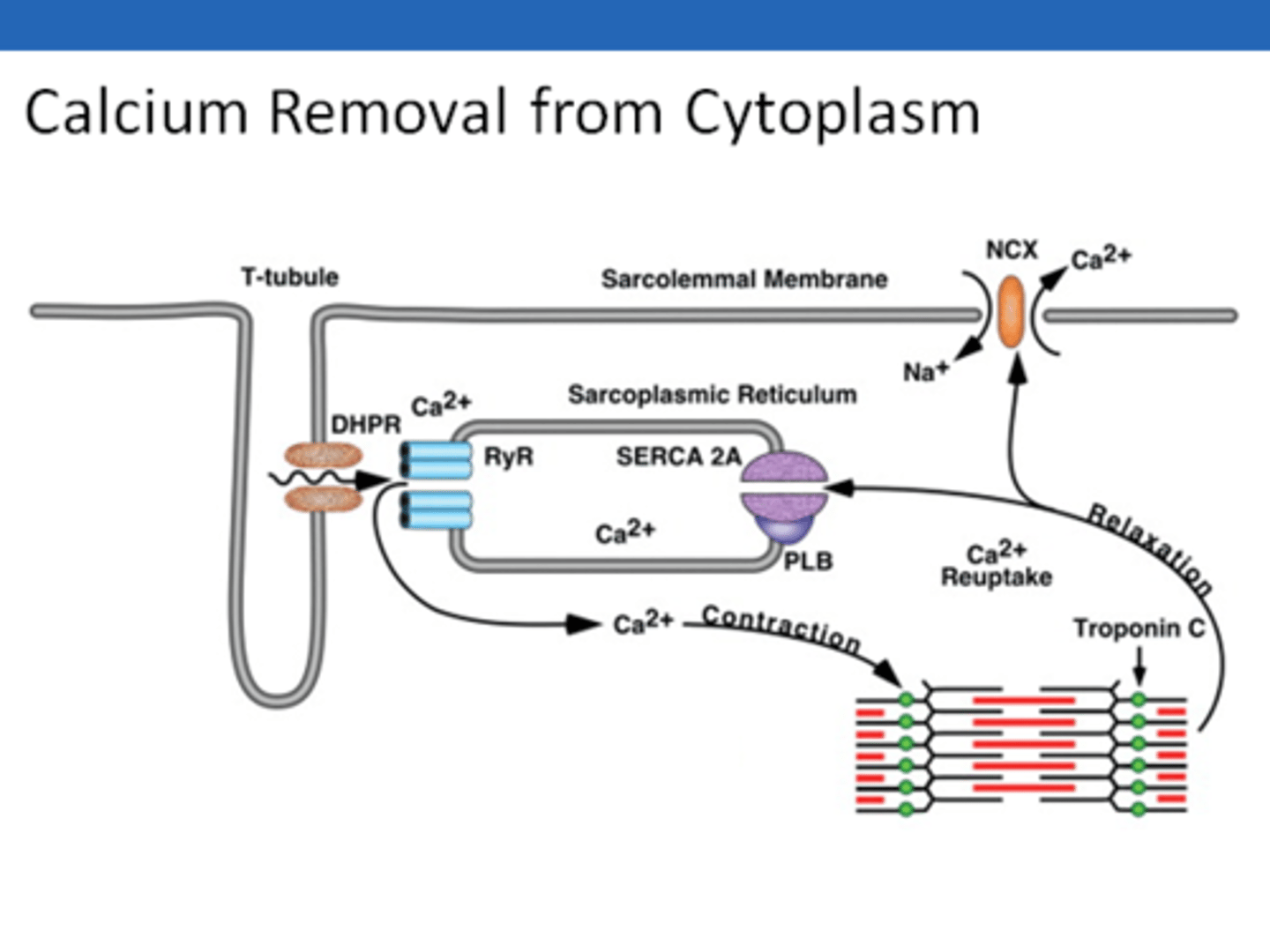
mechanism of excitation contraction coupling in mysocytes
1. when L-type caclium channels open --> ca2+ enters cell at t tubules
2. Ca2+ bind to calcium depended calcium channels called RYANODINE RECEPTORS in the cell on the SR
--> causes release of calcium stored in SR into cytoplasm (CALCIUM INDICED CALSIUM RELEASE)
3. Ca2+ enables contraction → Ca2+ binds troponin, allows actin/myosin cross-bridge formation
4. Ca2+ pumped back into the SR using the SERCA pump