essay 20 - surgical Sutures and suturing - Instruments and Materials. Types of sutures and knots. Techniques
1/38
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
39 Terms
what are Surgical sutures
the term “ suture” refers to any strand of material used to ligate blood vessels or approximate tissues for the purpose of closing a wound.
sutures are fundamental in both minor and major surgical procedures
what are the optimal suture characteristics
high, uniform tensile strength
prolonged tensile retention in vivo followed by controlled absorption
consistent uniform diameter
sterility
pliability for ease of handling and knot security
freedom from tissue irritating substances
predictable performance during and after placement
list the classification of sutures
absorbable sutures
non absorbable sutures
What are Absorbable sutures
these are broken down by enzymatic digestion (natural) or hydrolysis (synthetic) and absorbed by the body overtime. premature suture wetting may begin early degradation. absorbable sutures are unsuitable for patients with fever, infection, protein deficiency or impaired healing
list the absorbable sutures
natural absorbable sutures (Digested by enzymes)
collagen
plain surgical gut
fast absorbing surgical gut
Chromic gut
synthetic absorbable sutures (Broken Down via hydrolysis)
vicryl (polyglactin 910)
dexon II (polycaprolate)
monocryl (poliglecapron 25)
polysorb
PDS II (polydioxanone)
maxon
V-Loc
list the structures of Sutures and examples
monofilament = e.g caprosyn
multifilament = various e.g vicryl
describe non absorbable sutures
these sutures resist enzymatic degradation and remain indefinitely unless removed
describe the types of non absorbable sutures
natural
silk
cotton
surgical steel
synthetic
nylon
polyester (mersiline , ethibond)
Polybutester (novafil, vascufil)
polypropylene (prolene, surgipro II)
indications for non absorbable sutures
permanent internal support
Skin Closure (to be removed)
patients with Reactions to absorbables or hypertrophic/ keloid tendencies
prosthetic fixation
describe the structures of sutures
monofilament = single, smooth strand - less tissue drag, but more difficult to handle
multifilament: braided - easier handling and knot security, but more tissue drag and risk of harbouring bacteria
what are the knot tying principles
firm, non slip knot (flat and square)
minimal bulk to reduce tissue reaction
avoid friction or “sawing” to prevent suture weakening
handle suture gently - avoid crushing with forceps
apply appropriate tension - avoid over tightening
maintain traction on the first loop
final throw should lie horizontally
Change position to tie Flat, secure knots if needed
extra throws don't increase strength but may be needed for slippery materials
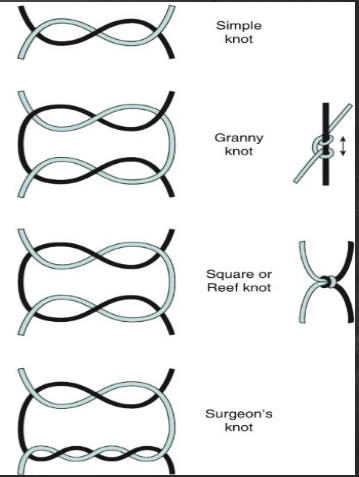
List the types of knots
simple knot
square knot (reef knot)
surgeon's knot
slip knot
granny knot (crossed knot)
describe a simple knot
one overhand throw; not used alone because it lacks security
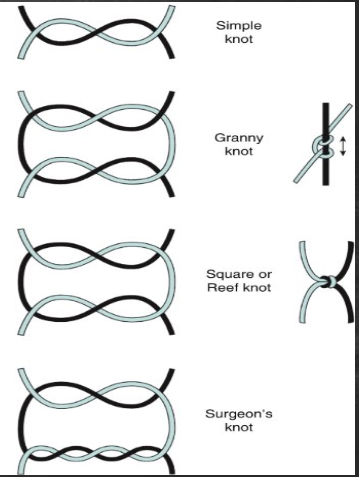
describe a square knot (reef knot)
most common surgical knot
made by alternating the direction of each throw (right over left, then left over right)
provides a secure and stable closure
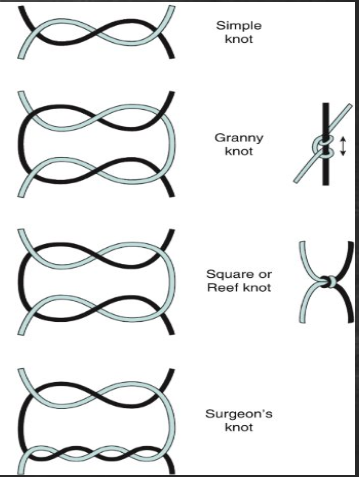
describe a surgeon's knot
Modified Square Knot with an extra turn in the first throw (Double overhand), followed by a standard second throw
useful for maintaining tension during knot tying when tissues are under stress (e.g elastic tissues)
offers increased friction and temporary stability before completing the knot
Describe a slip knot
forms a loop that can be tightened or loosened
occasionally used for ligating vessels or deep tissue closures
less secure than square or surgeons knot if used alone
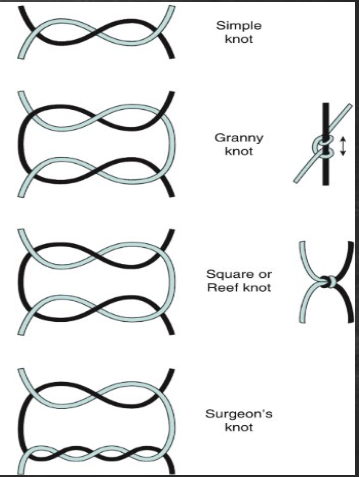
describe a granny knot (crossed knot
formed by repeating the same direction in throws (e.g Right Over Left Twice)
should be avoided- prone to slipping and reduced knot strength
describe suture removal - clinical protocol
once tissue healing allows non absorbable sutures must be removed to avoid infection or scarring
steps:
Clean Area with antiseptic (e.g hydrogen peroxide to remove crust)
pick up one end of the suture with forceps
cut near the skin entry point
pulled through the side opposite the knot to avoid dragging contaminated suture through tissue
what are some considerations that should be taken when selecting suture material
select suture material based on
— Tissue Type
— required strength and healing time
— risk of infection
— patient specific factors
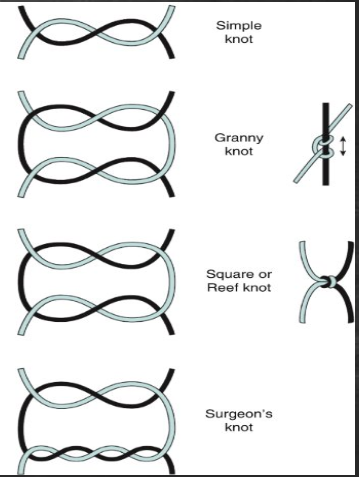
choosing the correct needle shape and size during suturing
curved needles (e.g 3/8, ½ circle) are common in oral surgery
cutting needles for tough tissues (e.g skin)
tapered needles for softer tissue (e.g mucosa)
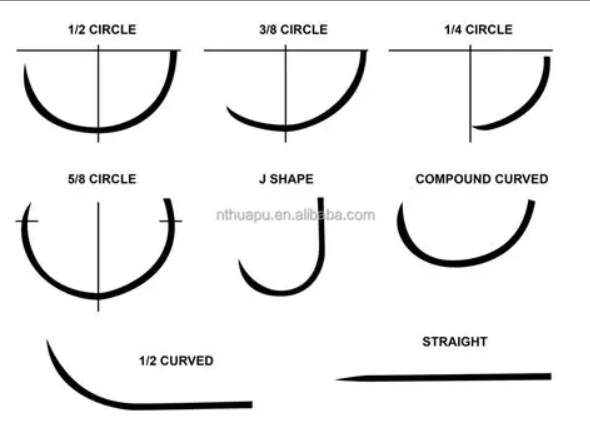
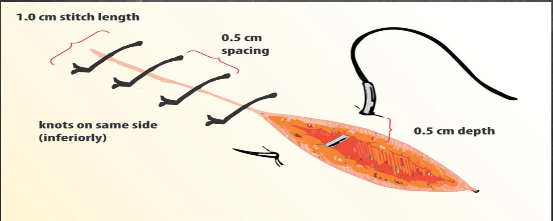
General Principle for suturing technique
use atraumatic technique - handle tissue gently
the needle should enter tissue at 90 degree angle to avoid tearing and ensure even depth
the bite distance from the incision line should be ~2-3mm
pass the needle through equal amount of tissues on both sides of the wound to avoid tension
use the minimum number of sutures required for effective wound approximation
knot should not lie over the incision line - place laterally to reduce irritation and risk of dehiscence
do not over tighten - sutures should approximate, not strangulate
cut tails short, unless longer lengths are needed for future adjustments or removal
list the types of suturing techniques
interrupted sutures
continuous sutures
figure of eight (Criss cross) sutures
purse-string suture
sling suture
suspensory sutures
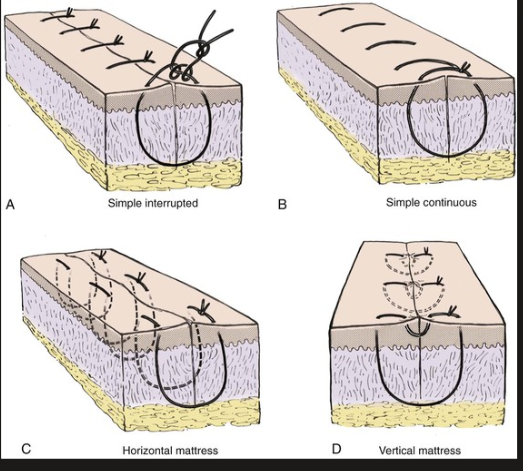
describe interrupted sutures
each is tied and cut individually
advantages = secure, good tension control, less likely to fail as a whole
disadvantages = time consuming, more foreign material
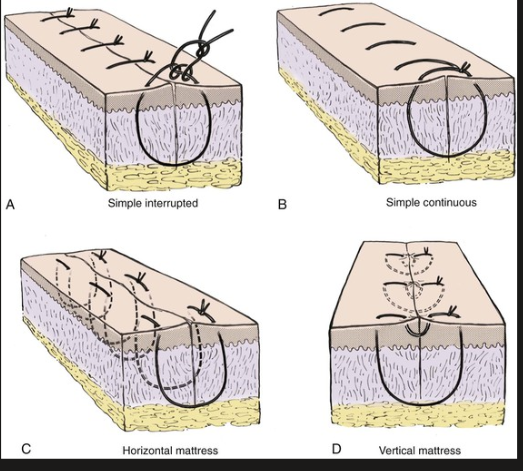
Simple interrupted = Standard and Most used; good for basic closure
horizontal mattress = provides tension release. Often used in flap edges
vertical mattress = ensures deep and superficial tissue approximation. For thicker issues
describe continuous sutures
a single strand runs through the entire wound and is tied only at the ends
advantages = faster, distributes tension evenly
disadvantages= if one point fails, the whole line can loosen
simple continuous = basic running stitch
locking continuous (ford interlocking) = Each pass locks the stitch. bad tension distribution, often used in skin
subcuticular = placed in dermis only (not used in intraoral mucosa)
describe Figure of eight (Criss cross) stitches
often used for socket closure after extraction
forms in “X” across the wound
provides a secure hemostasis and covers open sockets or membranes
describe purse string sutures
circular stitch that tightens like a drawstring
rarely used intraorally; occasionally for closing biopsy punches or around tubes
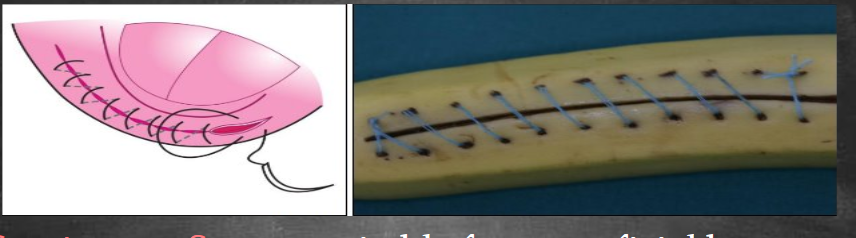
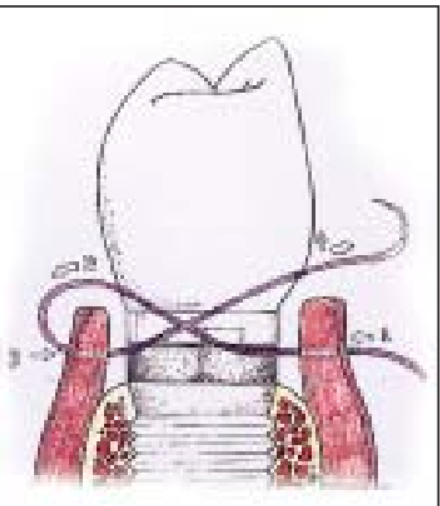
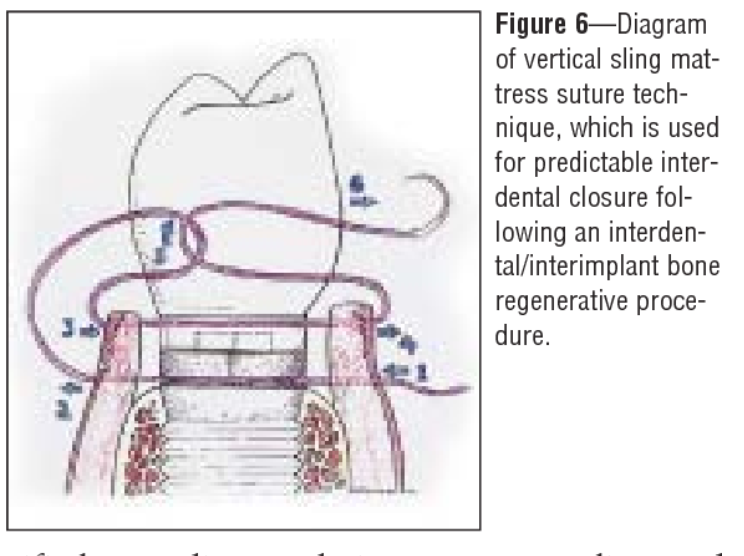
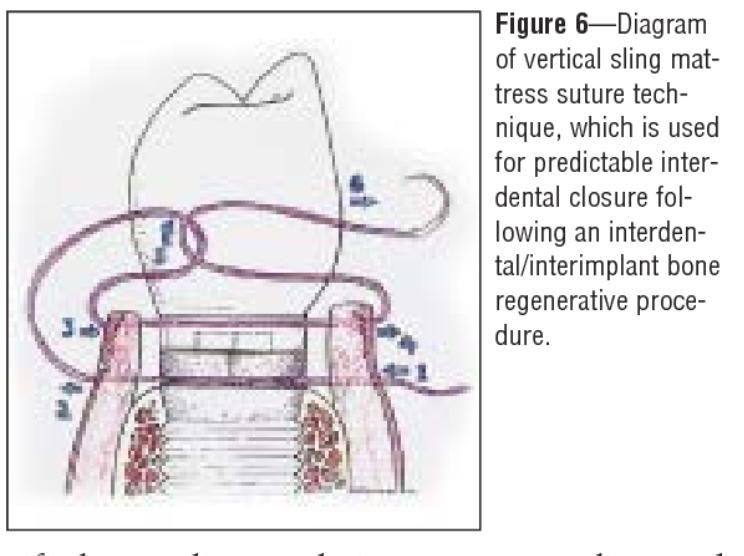
describe sling sutures
especially useful in periodontal flap surgeries
wraps around a tooth to stabilised a flap on one side
Two types:
single sling = around one tooth
double sling = around two adjacent teeth
describe suspensory sutures
anchor the tissue flap to the periosteum or bone
provide enhanced stability, especially in implant or grating procedures
what are the instruments for suturing
needle holder (mayo-hegar) = to grasp and drive the needle
tissue forceps (adson or Debakery) = to hold tissue gently
scissors (suture scissors) = to cut sutures precisely
suture needle = swaged (eyeless), curved, often 3/8 or ½ circle
suture material = absorbable or non absorbable
List the suture patterns
U-shaped vertical (vertical mattress)
U-shaped vertical (attached)
U-shaped vertical (not attached)
P-shaped suture
P-shaped attached
P-shaped not attached
Base vertical (vertical mattress variant)
Base horizontal (classic horizontal mattress)
Intradermal/subcuticular
describe U-shaped vertical (vertical mattress)
how to do it:
First bite = far from wound edge on one side → exit far on opposite side
second bite = return near the wound edge → Exit Near on opposite side
tie
Entry/ exit
far-far than Near-near (vertical plane)
important
create U shape
gives excellent eversion and strong tension control
Describe U-shaped vertical (attached)
How to do it:
Same as vertical mattress, but the loop is anchored by taking a small extra bite at the edge before tying.
Entry/Exit:
Far–far, near–near + small anchoring bite.
Important:
Prevents loop sliding.
More stable in mobile mucosa.
describe U‑Shaped Vertical (Not Attached)
How to do it:
Standard vertical mattress only.
No anchoring bite.
Entry/Exit:
Far–far, near–near.
Important:
Loop is free.
Used when you only need eversion, not anchoring.
describe P‑Shaped Suture
How to do it:
First bite: deep bite on one side → exit opposite side.
Second bite: small, superficial bite near the corner or flap tip → exit close by.
Tie so the long limb pulls tissue in one direction.
Entry/Exit:
Long bite + short bite = P‑shape.
Important:
Used for corners, flap tips, directional traction.
describe P‑Shaped Attached
How to do it:
Same as P‑shaped, but the short bite is anchored into the tissue edge.
Entry/Exit:
Long bite + anchored short bite.
Important:
Prevents corner from rotating or tearing.
Best for flap apex stabilization.
describe P‑Shaped Not Attached
How to do it:
Long bite + short superficial bite, but no anchoring.
Entry/Exit:
Long bite + free short bite.
Important:
Used when you want gentle directional pull without fixing the corner tightly.
describe Base Vertical (Vertical Horizontal Mattress Variant)
How to do it:
Two bites placed above and below the wound (vertical orientation).
Tie to distribute tension vertically.
Entry/Exit:
Enter above wound → exit opposite above.
Enter below wound → exit opposite below.
Important:
Spreads tension vertically.
Good for fragile tissue.
describe Base Horizontal (Classic Horizontal Mattress)
How to do it:
Enter left side of wound → exit right side.
Move a few millimeters distally.
Re‑enter right side → exit left side.
Tie to create a horizontal “box”.
Entry/Exit:
Enter left → exit right.
Re‑enter right → exit left.
Important:
Spreads tension horizontally.
Good for friable tissue and wound edges under tension.
describe Intradermal / Subcuticular
How to do it:
Continuous suture placed within the dermis, running parallel to wound.
No external stitches.
Entry/Exit:
Enter at one end of wound → weave through dermis → exit at opposite end.
Important:
Best cosmetic closure.
No eversion needed.
Common in facial or clean surgical wounds.