ANA 852 EXAM 6
1/221
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
222 Terms
Valley 2013
1. When endothelial lining of the blood vessel is damaged, platelets adhere to subendothelial collagen. What substances anchors platelets to subendothelial collagen?
· Von Willebrand’s factor (VII:vWF:R)
1. What clotting factor activates the platelet at the site of vascular injury?
· Factor IIa- Thrombin
What two substances, released from the activated platelet, stimulate platelet aggregation?
· ADP and thromboxane A
1. What substances link platelets together (aggregates them)
· Fibrinogen (factor I)
1. What agents inhibit plt aggregation by impairing cyclooxygenase
· ASA and NSAIDS
What clotting factors are found in the extrinsic pathway
· 3 (III), 7 (VII)
1. What clotting factors are found in the intrinsic pathway?
· 8 (VIII), 9 (IX), 11(XI), 12 (XII)
1. What clotting factors are found in the common pathway?
· 1 (I), 2 (II), 5 (V), 10 (X), 13 (XIII)
1. What clotting factor is considered the physiologic initiator of the coagulation cascade
· III (3)
1. What factor promotes fibrin cross linking?
· 13 (XIII)
1. Antithrombin III inhibits what 5 clotting factors? Which of these 5 is intrinc and what 2 of these 5 clotting factors are most profoundly inhibited?
· 2 (II), 9 (IX) ,10 (X) ,11 (XI), 12 (XII)
· Intrinsic = IX, XI, XII
· II and X are most profoundly inhibited
EXAM Which four factors are vitamin K dependent? Which of these is in the extrinsic pathway?
· 2 (II), 7 (VII), 9 (IX), 10 (X)
o Only 7 VII is extrinsic
1. How does heparin work?
· Heparin increases the activity of antithrombin III
1. How does coumadin work?
· Coumadin competitively inhibits the vitamin-K dependent clotting factors
1. What anticoagulant affects the extrinsic and final common pathway?
· Warfarin (Coumadin)
1. What anticoagulant affects the intrinsic and final common pathway
· Heparin
1. What two coagulation tests assess the extrinsic & common pathway?
· PT/INR
1. What two coagulation tests assess the intrinsic & common pathway?
· PTT/ACT
1. How does protamine work to reverse heparin? What kind of reaction is this?
· Protamine combines electrostatically with heparin this is a neutralization reaction
1. What enzyme is responsible for breaking down fibrin?
· Plasmin
1. What two pharmacological agents inhibit plasmin?
· Epilson-Aminocaproic Acid (Amicar) and Aprotinin (Trasylol)
1. Name three substances that convert plasminogen (inactive) to plasmin.
· Streptokinase, urokinase plasminogen activator (uPA), and tissue plasminogen activator (tPA)
1. When is aproptein generally used in anesthesia? How does it work?
· Aprotinin is used for repeat sternotomies and works by inhibiting plasmin
1. What is the normal activated coagulation time?
· 80-150 second
1. What is the is the best test of primary hemostasis or platelet function?
· Standardized skin bleeding time
EXAM What is the most common reason for coagulopathy after a massive blood transfusion?
· Thrombocytopenia, lack of functioning platelets
1. What clotting factors are found in fresh frozen plasma?
· all procoagulants and naturally occurring inhibitors, no platelets
EXAM Cryoprecipitate contains what clotting factors?
· Fibrinogen (I), 8 (VIII), 13 (XIII)
1. What are the typical manifestations of DIC?
· Bleeding and oozing from wounds, tubes, and sites of vascular access
1. Transfused blood is deficient in what two coagulation factors?
· Factor 8 (VIII) and 5 (V)
Valley 2013 QUIZ Hemostasis
1. What is the most common inherited coagulation defect
A. Hemophilia A
B. hemophilia B
C. VWB
D. Christmas disease
C. VWB
3. What antiplt agent prevents ADP- induced platelet aggregation
A. ASA
B. Ibuprofen
C. Ketorolac
D. Ticlopidine
D. Ticlopidine
3. Each factor is made in liver EXCEPT
A. II
B. IV
C. X
D. XII
B. IV
3. Clotting factor responsible for cross- linking fibrin
A. I
B. II
C. 7 VII
D. 13 XIII
D. 13 XIII
3. What anticoagulant works one extrinsic pathway and what test assesses effectiveness of anticoagulant?
A. Coumadin; PT
B. Coumadin; PTT
C. Heparin; PT
D. Heparin; PTT
A. Coumadin; PT
8.When antithrombin III is activated by. Heparin, antithrombin III
A. releases factors I, III, VII, and XIII
B. Binds factors I, III, VII, ZII
C. releases factors II, IX, X, XI, and XII
D. binds factors II, IX, X, XI, and XII
D. binds factors II, IX, X, XI, and XII
(2,9,10,11,12)
EXAM 9. A patient scheduled for CABG is heparanized, and the ACT is <300seconds. The result is the same after a second dose of heparin. Why is the patient unresponsive to heparin and what should the next action be?
A. deficiency of plasmin; give FFP
B. Deficiency of plasmin; cancel case
C. Deficiency of antithrombin III; give FFP
D. deficiency of antithrombin III; Cancel case
C. Deficiency of antithrombin III; give FFP
10. normal prothrombin time is
A. 3-5 seconds
B. 12-14 seconds
C. 25-35 seconds
D. 80-150 seconds
B. 12-14 seconds
11. The reaction of protamine with heparin is a
A. neutralization reaction
B. Covalent reaction
C. hydrogen bonding reaction
D. counterbalanced reaction
A. neutralization reaction
12. What substance converts fibrin to fibrin split products
A. tissue plasmingeon activator
B. Amnicar
C. Plasmin
D. Streptokinase
C. Plasmin
A. tPA | Activates plasminogen → plasmin (indirect) |
B. Amicar (aminocaproic acid) | Inhibits plasmin (prevents breakdown) |
D. Streptokinase | Activates plasminogen → plasmin (indirect) |
EXAM 13. Which of the following is true about aprotinin EXCEPT
A. May cause allergic reactions when administered for the first time
B. May cause anaphylactic reaction if administered the second time
C. Indicated for pts undergoing sternontomy for the second time
D. Accelerates breakdown of fiber
D. Accelerates breakdown of fiber
15. Which is increased in pts with DIC
A. FSP
B. Fibrinogen
C. prothrombin
D. Factor VIII
A. FSP
Short answer: 1. Name the three layer of the normal vessel wall and list the properties associated with each layer.
1. Intima— secrete procoags, anticoags, and fibrinolytics
2. Media— contains collagen and fibronectin
3. Adventitia—NO and prostacyclin act here to control vasodilation
Short Answer: 1. What is INR, and why is it important?
1. Eval of extrinsic and common pathways
2. Standardizes PT results
3. Eval of coumadin effects on ex. pathway
CJ Exam Review Sheet
EXAM 1. Pt w/ von wild, no response to DDAVP. Give next?
Cryo
EXAM: Final pathway of fibrin involves?
All
EXAM: ALl true for factor 5 and 8 EXCEPT
replaced with blood bank
EXAM: releaxes from ACT plt in hemostatis to aid in plt aggreation
· B and C (thromb A and ADP)
EXAM prothrombinase complex includes
· 3, 5, 10
EXAM process of plt before administration
· Rh matching only
EXAM 11. treat Von Wild Disease w/ all except
· Recombinant factor 8
EXAM 12. WBC origin
bronchioles
EXAM 13. treat hemolytic anemia transfusion w/ all except
Hydrocortisone
EXAM gen causes of decrease eryth w/ anemia all except
· Hypoxemia
EXAM 15. pt w/ which of the following diseases are most likely to exhibit a cholinergic crisis
Myasthenia gravis
EXAM 16. improves plt fx
· Desmopressin
EXAM decreased w/ DIC all except
Fibrin split products
EXAM cross link of fibrin strands requires
13
EXAM . lab test w/ long standing iron deficiency
Decreased serum iron
FENG LECTURE HINT
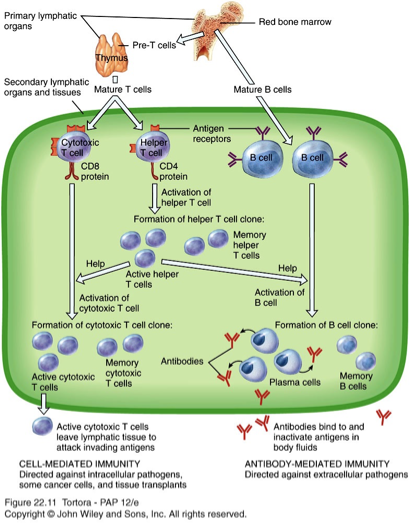
EXAM One questions test: foreign pathogen. Immediately talks about lymphocytes not neutrophils. Lymphocytes carry most important B cells and T cells and natural killer cells. B cells= antigen presenting cells (APC) –
WBC have to recognize there is a pathogen. APC cells recognize pathogen by presenting to WBC.
Antigene release specific chemotaxis to tell body where to go
EXAM Fixed is also called resident= stays in skin, klymph nodes, alveoli, liver & spleen so macrophages stay there bc they hae a lot fopathogens to fight
1st line cells= fixed or resident macrophages = EXAM
2nd line= neutrophils
3rd line cells= wandering macrophages
Faster= neutrophils
What is most abdunt ig
IgG
2nd= IgM
EXAM: Interferon fxn
•IFNs are cytokines with antiviral activity- stops viral replication in S phase
•Released from many cell types within hours of viral infection
•Act on neighboring noninfected cells (paracrine=signals cells that virus is near) to prevent spread of virus
•Promote proliferation and activation of NK cells
•Synthetic IFNs used to treat hepatitis B, neoplasms, nervous system inflammation, chronic granulomatous disease
study this for acquired immunity
hypersensitivy , autoimmune and immunodeficiney is tested a lot
hypersensitive and allergic reactions
•Hypersensitivity: Exaggerated immune response to antigen
•Classified into Types I, II, III and IV (overlapping MOA in I, II, & III)
•Triggering Mechanisms Type I:
•Binding of antigen to IgE on mast cells and basophils to trigger mediator release:
•Histamines (key mediator)
•Leukotrienes
•Cytokines
•Direct activation
•Opioids
•Vancomycin
•Radio contrast media
•Complement
•Allergens
type I hypersensitivity
•Rapidly developing reaction of antigen-antibody interaction in patient previously exposed/sensitized to antigen
•Antigen (allergen) reacts with IgE antibodies on Mast Cell
•Triggers mediator release (histamine)
•Allergens: grass, pollen, dust, mites, mold, dander
•Symptoms: rhinitis, conjunctivitis, urticaria, pruritus, anaphylaxis
type I hypersensitivity anaphylaxis vs anaphylactoid
Anaphylaxis
Severe, generalized, immediate hypersensitivity type 1 reaction with IgE increase that includes:
Pruritis, urticaria, angioedema
Hypotension, wheezing, bronchospasm
Direct cardiac effects
Shock
Clinical manifestations can occur within minutes or hours of exposure to antigen
Biphasic: Early symptoms previously resolved recur several hours later
Severity of anaphylaxis related to magnitude of stimulus
May occur with exposure to minute amounts of allergen in highly sensitive patient
Anaphylactoid
•Reactions caused by mediator release from basophils and mast cells in response to a non-IgE-mediated triggering event (NO igE RELEASE)
•Clinical manifestations are similar to anaphylactic manifestations, but less severe
•Tryptase is a marker for mechanistic delineation of an allergic response= differentiates between anaphylaxis & anaphylatoid
type II hypersensitivity
•IgG & IgM antibodies bind to antigens on cell surfaces
•Antigen-antibody reaction activates complement
•Activates membrane attack complex
•Examples:
–Transfusion reactions
–Autoimmune
–Hemolytic anemia
–Myasthenia gravis
–Graves disease
Type III hypersensitivity
•Antigen-antibody complexes deposit in tissues and cause injury all across body
•Normally these complexes are cleared by phagocyte system
•Protracted infections or autoimmune processes can l/t type III rxns
•Examples of immune complex diseases include:
–Lupus
–Glomerulonephritis
—RA IS TYPE 4 BUT HAS TYPE 3 CHARACTERISTICS
TYPE IV hypersensitivity
•Delayed type hypersensitivity (>12 hours after contact with antigen)
•Migration of antigen-specific lymphocytes to reaction site is followed by cytokine release and local inflammatory response
•Contact hypersensitivity is one form of type IV rxn (skin comes in contact with antigen, examples:
–Contact dermatitis (can be type 1 & 4)- i.e latex allergy
–Poison ivy
•Another form is granulomatous hypersensitivity (chronic infection l/t granulomas in tissues, examples:
–Tuberculosis
–Sarcoidosis
–Crohn’s disease
drug rxns
–2/3 anaphylactic (immune-mediated)
–1/3 anaphylactoid (non-immune-mediated)
–NMBAs Most frequently= succs, vecuronium, and rocuronium (in that order)
–Latex
–Antibiotics
–Hypnotics
–Opioids
–Colloids
–Other agents (contrast, protamine)
–Local anesthetics (esters due to PABA metabolite)
EXAM •Retrovirus whose genome contains two strands of single-stranded RNA
EXAM Angioedema
•Hereditary (CI esterase inhibitor dysfunction) or acquired (ACE inhibitor)
•Causes: release of mast cell mediators and bradykinin does not cause allergic symptoms.BRADYKININ RELEASED NOT HISTAMINES
•Mechanisms: increase vascular permeability, produce edema
•Tx: androgen, antifibrinolytic therapy, antihistamine, catecholamines
•Anesthesia consideration: Intubation
EXAM 15 points= matching
Extrinisc pathway steps
injury occurs outside of vessels
damaged tissues release tissue factor (III) which activates proconvertin 7 (VII)
•Activated factor 7 VII activates factor 10 (X), which activates final common pathway
Intrinisc pathway- EXAM MATCHING ON WHAT FACTOR ACTIVATES WHICH ONE
•When injury occurs within the blood vessels,
prekallikrein, high molecular-weight kininogen and calcium activate Factor 12 (XII)
•Factor 12 (XII) activates factor 11 (XI)
•Factor 11 (XI) activates factor 9 (IX)
•Factor 9 (IX) activates factor 8 (VIII)
•Factor 8 (VIII) activates factor 10 (X), which activates common pathway
final common pathway- EXAM MATCHING ON WHAT FACTOR ACTIVATES WHICH ONE
factors 3 & 5 make Factor X form complex Xv (prothrombinase complex)
•Factor Xv activates factor II (prothrombin)
•Factor II (prothrombin) converts to factor IIa (thrombin)
•Factor IIa (thrombin) activates factor I (fibrinogen) to form activated factor I (fibrin)
•Factor 13 (XIII) converts factor Ia (fibrin) to dense fibers/stable clot
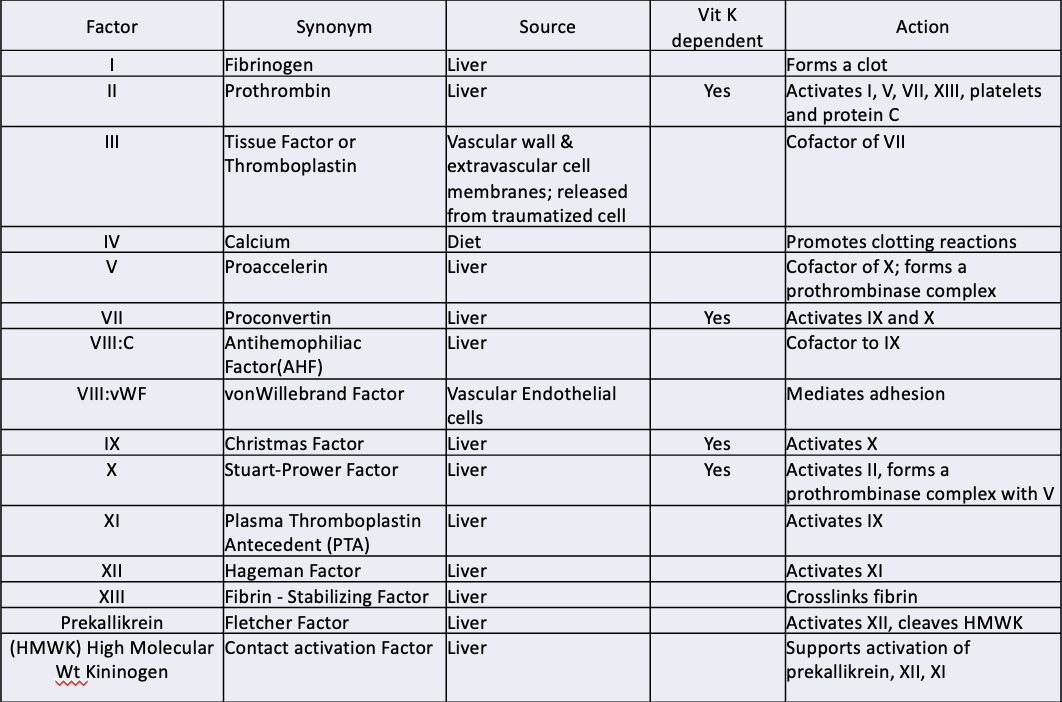
EXAM coag factor factrs
"a" (IIa) means that the factor is activated
•All factors produced in Liver except III, IV and VIII:vWF
•Vitamin K dependent Factors: 2 (II), 7 (VII), 9 (IX) and 10 (X). They are not functional in absence of Vitamin K.
•Factors V and VIII do not become "activated" enzymes. They serve as Cofactors in the reaction complex.
•Factors V and VIII are NOT durable in banked blood.
Massive transfusions of PRBCs will lead to dilutional coagulopathy as a result.

EXAM classification of anemias
MCV hgb content (MCHC) causes
Normocytic (80-100) normochromic (32-36) bone marrow failure, renal dx, hemolytic anemia
Macrocytic ( >100) normochromic (32-36) megaloblastic anemia
Microcytic (<80) hypochromic (<32) iron deficiency, chronic diseases
Microcytic anemia (MCV <80) causes 4
iron deficiency
thalassemia trait
chronic diseases
sideroblastic anemia
Normoctyic anemia 80-100
elevatied reticulocyte
acute blood loss
Hemolysis
normal or low reticulocyte
kidney disease
chronic disease
bone marrow disorder
medication
macrocytic anemia MCV >100
megaloblastic
vitamin B12
folate
Non Megaloblastic
elevated reticulocyte (bleeding; hemolysis)
normal/ low reticulocyte (Liver disease, Alcoholism Hypothyroidism)
Guyton 13ed- Chapter 33 Red Blood Cells, Anemia, and Polycythemia
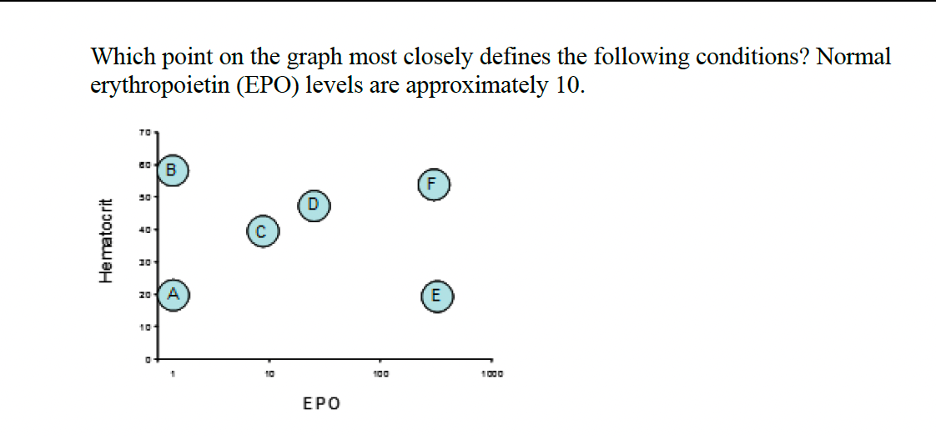
1. A 52-year-old woman with type 1 diabetes has had progressive renal failure over the past 3
years. She is not on dialysis and her examination shows no abnormalities. Her hemoglobin
level is 9 g/dL, hematocrit is 29%, and mean corpuscular volume is 92 fL, and a blood smear
shows normocytic, normochromic cells. Which of the following is the most likely cause of the
anemia?
A. Acute blood loss
B. Pernicious anemia
C. Sickle cell disease
D. Erythropoietin deficiency
E. Hemolytic anemia
F. Polycythemia vera
D. Erythropoietin deficiency
olympic marathon runner
polycythemia vera
chronic disease
D
B
E
5. A healthy 3-year-old girl is brought to the emergency department because of severe
uncontrolled nosebleed. She has a history of ear infections that have improved after treatment.
Her temperature is elevated. She has numerous small bruises on her arms and legs. Her
laboratory studies show the following:
• Hemoglobin 4.6 g/dL
• Leukocyte count 3,000/mm3
Reticulocyte count 0.1%
• Platelet count 12,000/mm3
Which of the following is the most likely explanation for these findings?
A. Anemia due to blood loss
B. Aplastic anemia
C. Sickle cell disease
D. Mononucleosis
B. Aplastic anemia
6. In the fifth month (middle trimester) fetus hematopoiesis is most active in which of the following?
A. Yolk sac
B. Spleen
C. Liver
D. Bone marrow
C. Liver
7. Following the donation of a unit of blood, how long before hematocrit begins to increase?
A. 1 hour
B. 2 hours
C. 24 hours
D. 5 days
E. 2 weeks
D. 5 days
8. How would a cell that has a diameter of 9 micrometers and an mean corpuscular volume of 106 be classified?
A. Macrocyte
B. Microcyte
C. Normal
D. Either normal or slightly microcytic
A. Macrocyte
9. Which of the following is true regarding erythropoietin?
A. Erythropoietin is mainly secreted by the liver
B. Injection of erythropoietin leads to a rapid increase in the number of circulating red blood cells within the next 48 hours
C. Excessive exposure to x-rays with destruction of the bone marrow leads to an increased erythropoietin secretion
D. Erythropoietin also acts on the spleen by decreasing red blood cell destruction
C. Excessive exposure to x-rays with destruction of the bone marrow leads to an
increased erythropoietin secretion
10. A 50 year-old man comes to your office complaining only of fatigue, and has the following
laboratory findings:
• Hemoglobin = 9.9 g/dL
• Hematocrit = 29.8%
• Mean corpuscular volume = 76 fl
Mean corpuscular hemoglobin= 21 pg/cell
• Platelet count= 375,000 /μl
What is the most likely diagnosis?
A. Aplastic anemia
B. Vitamin B12 deficiency
C. Chronic gastrointestinal bleeding
D. Acute gastrointestinal bleeding
E. Folate (folic acid) deficiency
F. Sickle cell anemia
C. Chronic gastrointestinal bleeding
11. A 65-year-old with persistent diarrhea is found to be severely underweight and to have a hematocrit of 26% with mean corpuscular volume of 110 fl. Her peripheral blood smear shows oversized red blood cells with bizarre shapes. What is the most likely cause of her anemia?
A. Iron deficiency due to intestinal blood loss
B. Absence of erythropoietin because of poor nutrition
C. Gastrointestinal cancer
D. Deficiency of folate, and potentially also vitamin B12
E. Aplastic anemia
D. Deficiency of folate, and potentially also vitamin B12
12. An 82-year-old man presents with fatigue and pallor. His hemoglobin is 7.8, hematocrit is 23.1, leukocyte count is 1,750, and platelet count is 68,000. What is the most likely diagnosis?
A. Blood loss anemia
B. Pernicious anemia
C. Aplastic anemia
D. Hemolytic anemia
E. Sickle cell anemia
C. Aplastic anemia
Guyton 14ed. Ch 33