Wound Management & LAB
1/63
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
64 Terms
wound
injuries that break the skin or other body tissues
*includes cuts, scrapes, scratches, and punctured skin
**often happen because of an accident, but surgery, sutures, and stitches also cause wounds
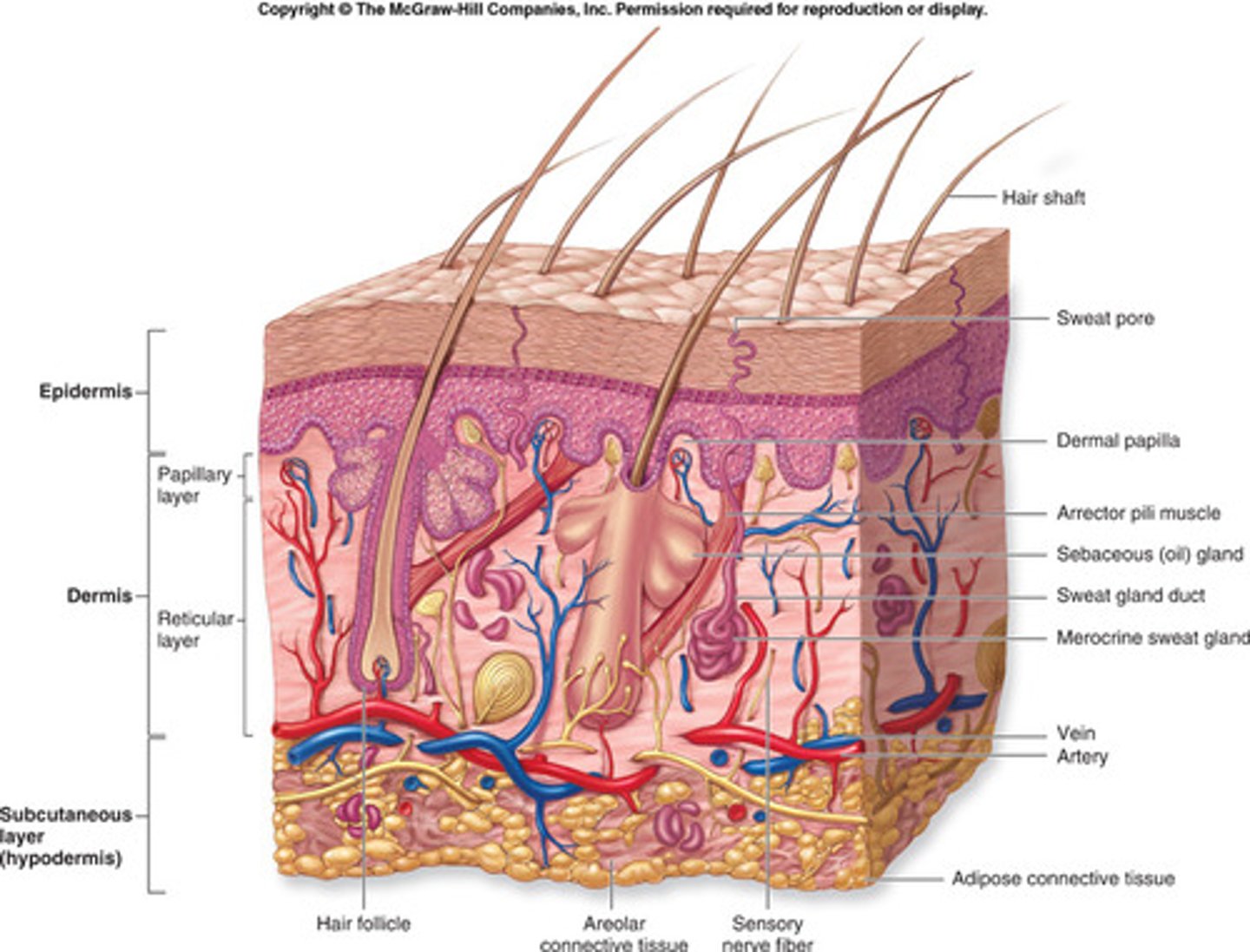
integumentary system
LAYERS:
1) epidermis
- outer most layer
- 5 layers--> stratum basal
avascular
2) dermis
- 2nd layer
- papillary dermis & reticular dermis
vascularized
3) subcutaneous
FUNCTIONS:
- protection
- regulation
- sensation
sensory mechanoreceptors
found in dermis layer
1) pacinian--> vibration
2) ruffini--> stretch
3) merkel--> pressure
4) meissner--> movement
5) hair follicles--> light touch
*NOT all at the same depth
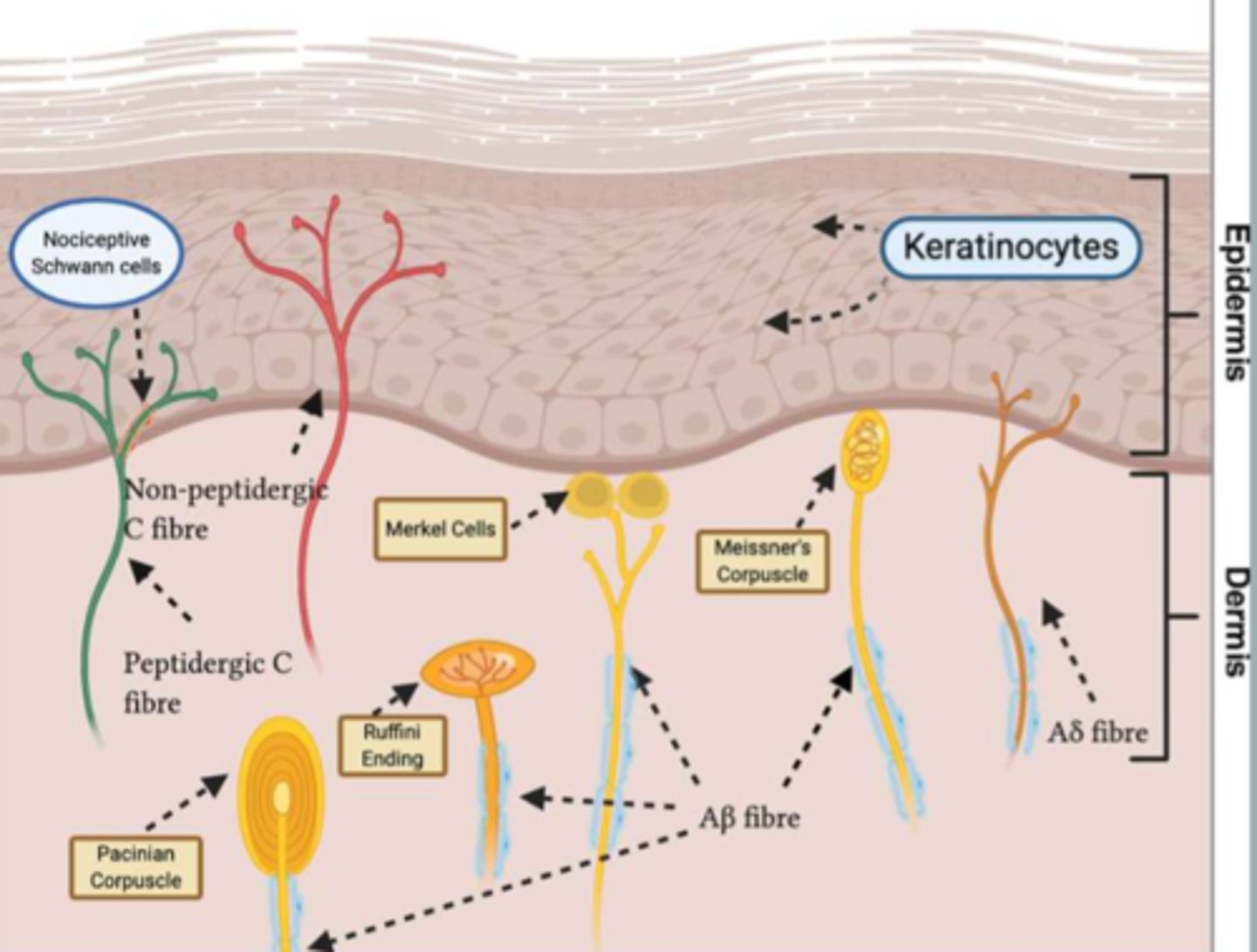
unmyelinated C fibers
free nerve endings that transmit pain impulses
*found into epidermal layer
(why a skin injury can be painful even w/o bleeding)
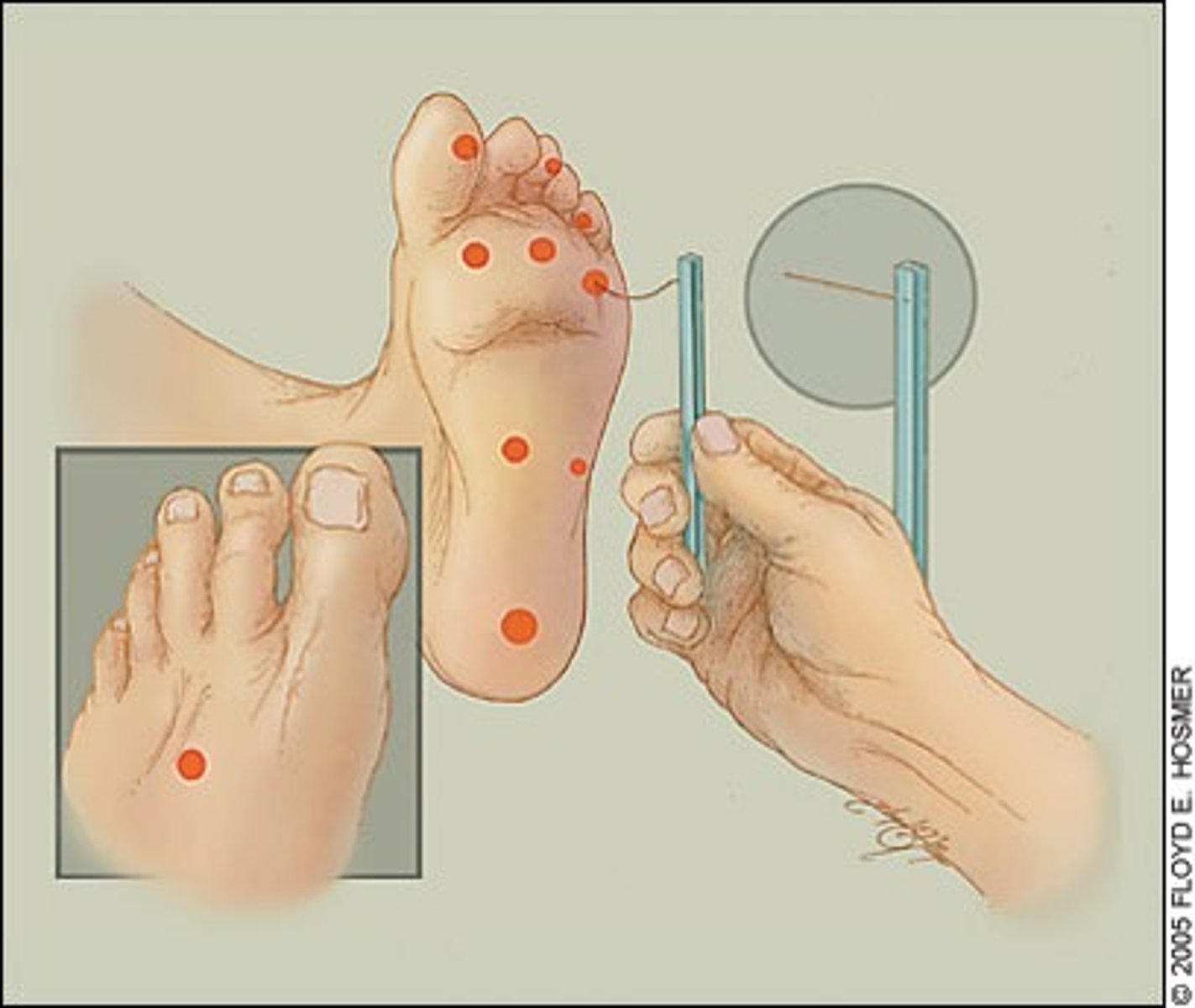
Semmes Weinstein Monofilament Test
test for protective sensation (deep pressure)
5.07/10g
*frequently diminished or absent secondary to neuropathy
**NOT a vascular test
- test all "high risk" sites in random order (pt should be looking away)
- may apply stimulus up to 3x to check for responsiveness
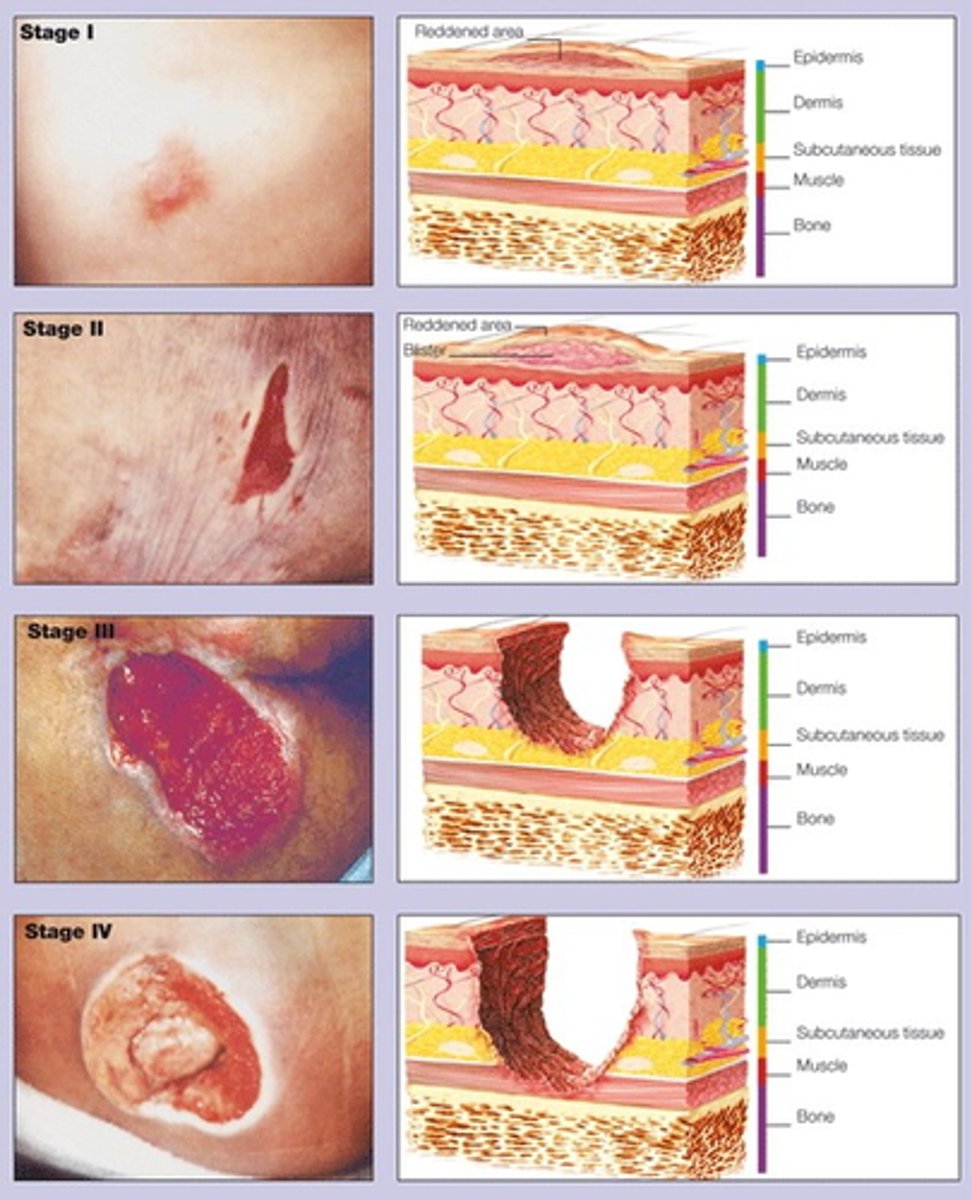
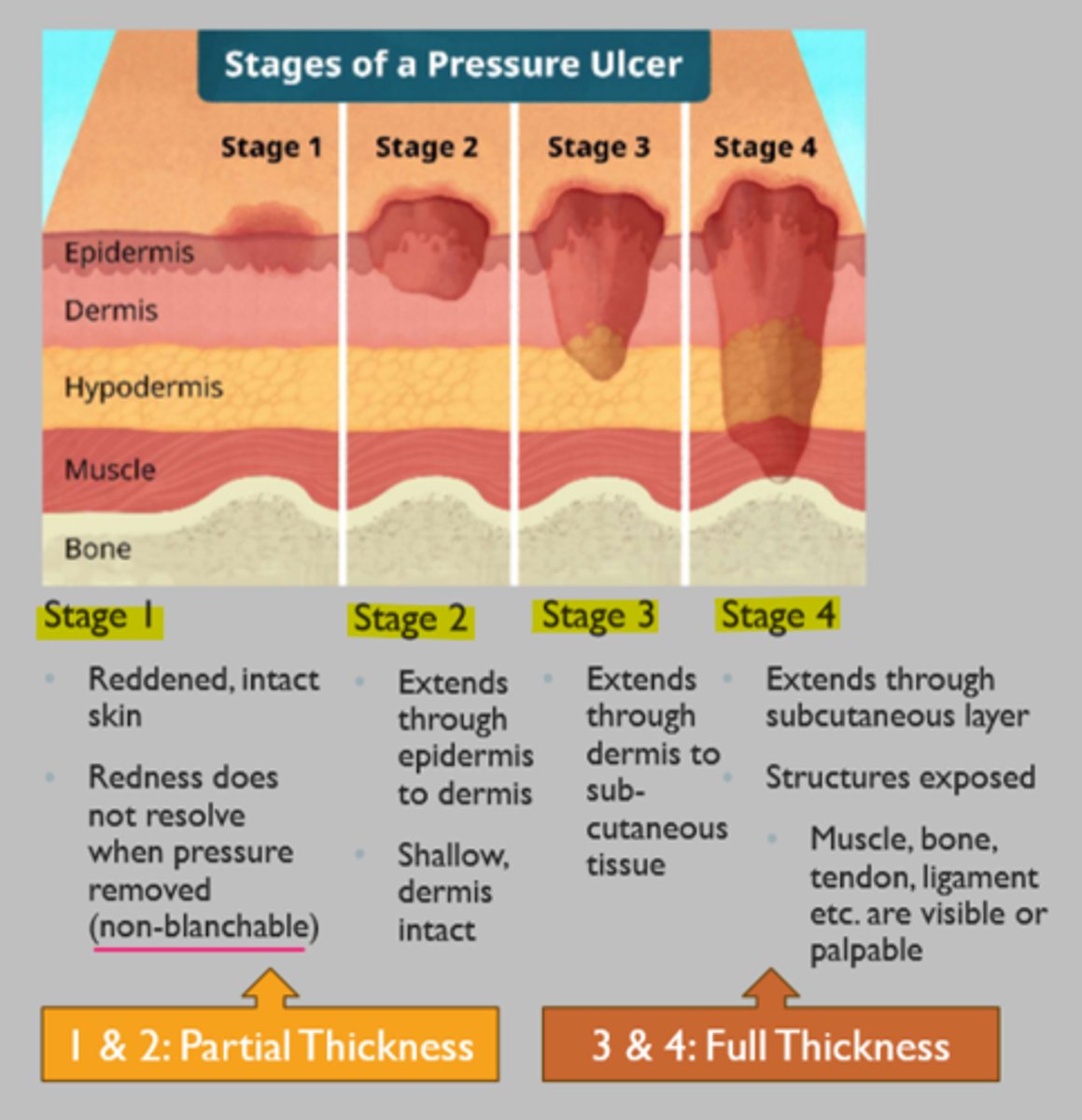
wound classification by depth
1) superficial
- damage to epidermis
- normal upward migration of epidermal cells
2) superficial partial thickness
- papillary dermis (1ST LAYER)
- re-epithelialization
3) deep partial thickness
- reticular dermis (2ND LAYER)
- granulation formation
4) full thickness
- subcutaneous
- granulation formation
*tendons/ligaments/bone visible
wound classification by timeline
1) acute
- wound that either heals by regeneration or in a timely & orderly process
- wound closure within 2-4 weeks
- progressed through normal stages of wound healing
2) chronic
- wound that has failed to proceed through a normal, orderly and timely sequence of repair or in which the repair fails to restore anatomic and functional integrity
- after 3 months
- all wounds have potential to become chronic due to underlying disease process, bacteria, nutrition, foreign material
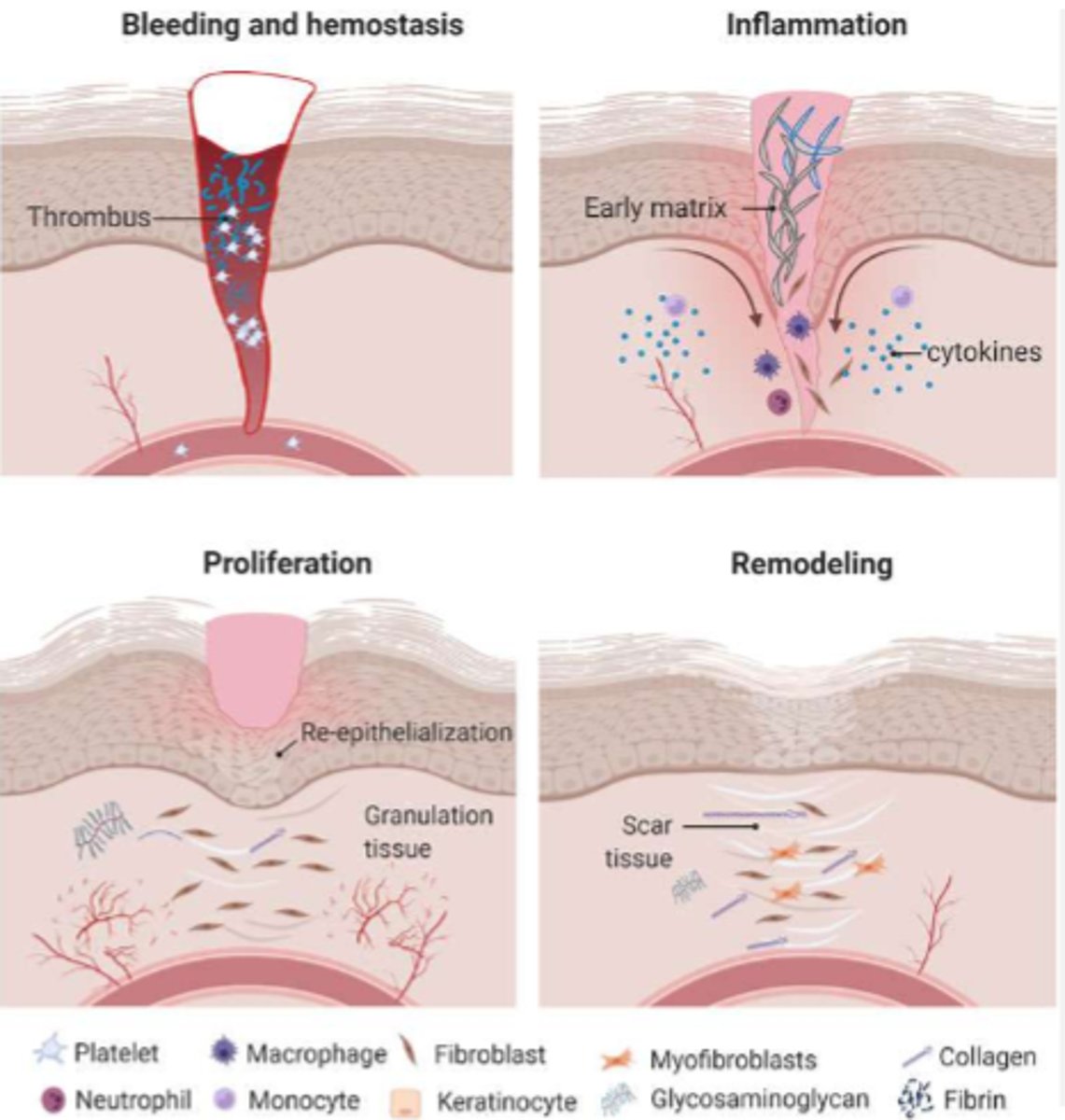
stages of wound healing
0-3 days: hemostasis
- insult to skin
- vasoconstriction occurs to stop bleeding
- clot formation
1-25 days: inflammation
(4 days)
- cytokines released to activate cells that breakdown foreign material/bacteria
(macrophages, T cells, neutrophils, etc.)
- vasodilation of capillaries
- redness, edema, warmth, peripheral sensitization
1-25 days: proliferation
(3-21 days)
- reaction of the body to start wound closure
- collagen (type III) synthesis, capillary proliferation, granulation formation
- TISSUE IS FRAGILE
20-365 days: maturation/remodeling
- closed wound but still healing
- skin shrinkage
- final tensile strength 80% of original
inflammation
Chronic wounds often do not progress past which stage of healing?
abnormal wound healing
FACTORS:
- imbalance of growth factors and inflammatory factors
(wound infection, biofilm, etc.)
- hypoxia
(ex. smoker)
- poor nutrition
- medication
(immunosuppression, NSAIDS)
- trauma/stress
- disease/chronic illness
(poor circulation, peripheral neuropathy, etc.)
- age
(flattening of rete ridges, decrease collagen synthesis and vascularization)
biofilm
multicellular community held together by a self-produced extracellular matrix that can halt the healing process
*invisible to the naked eye
**must be removed from wound to heal fully!!
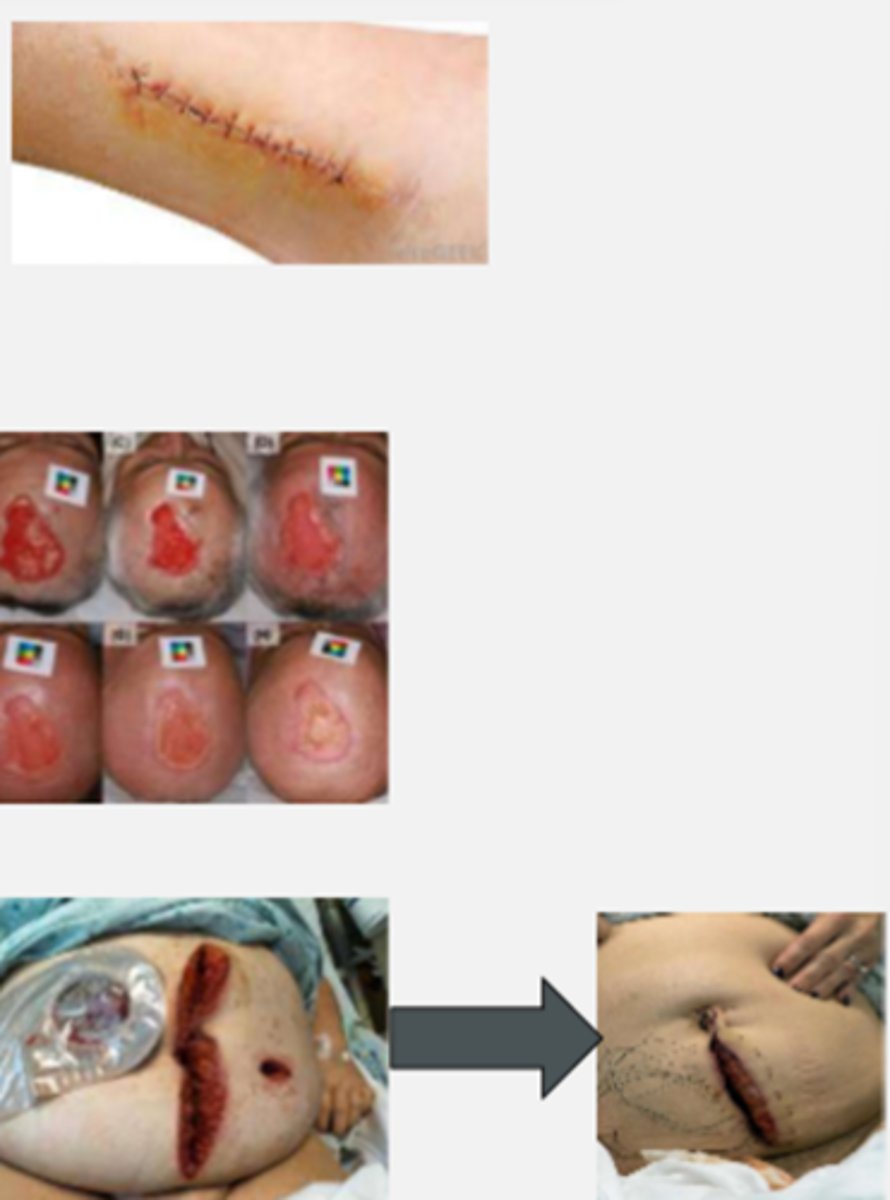
wound closures
PRIMARY INTENTION
- surgical wound closure
(stitches, staples, etc.)
SECONDARY INTENTION
- wound edges can't approx. initially
(heals by granulation)
- natural healing process
(wound "fills in")
TERTIARY INTENTION
(delayed primary)
- intentionally leaving the wound open to start healing
wound assessment and documentation
1) wound depth
- superficial
- superficial partial thickness
- deep partial thickness
- full thickness
2) chronicity
- acute
- chronic
3) stage of healing
- inflammation vs proliferation vs remodeling
- normal vs abnormal
4) closure
- primary
- secondary
- delayed primary
5) location
- based on bony landmarks
- digital photography weekly
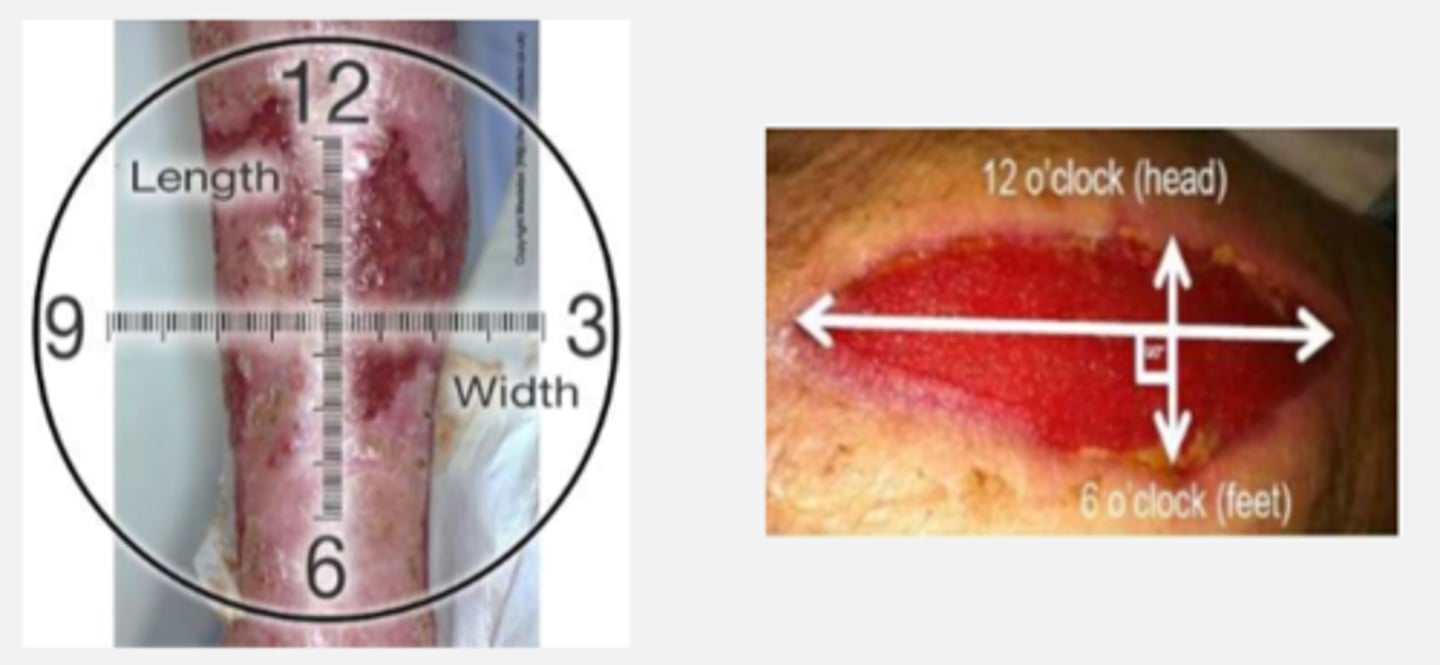
clock method
assessment method for size measurement of wound
(in cm)
1. greatest length at longest point (12-6)
2. greatest width at widest point (9-3)
3. greatest depth from wound edge
(add clock location for added accuracy)
"12 o'clock" is ALWAYS towards the head of the patient
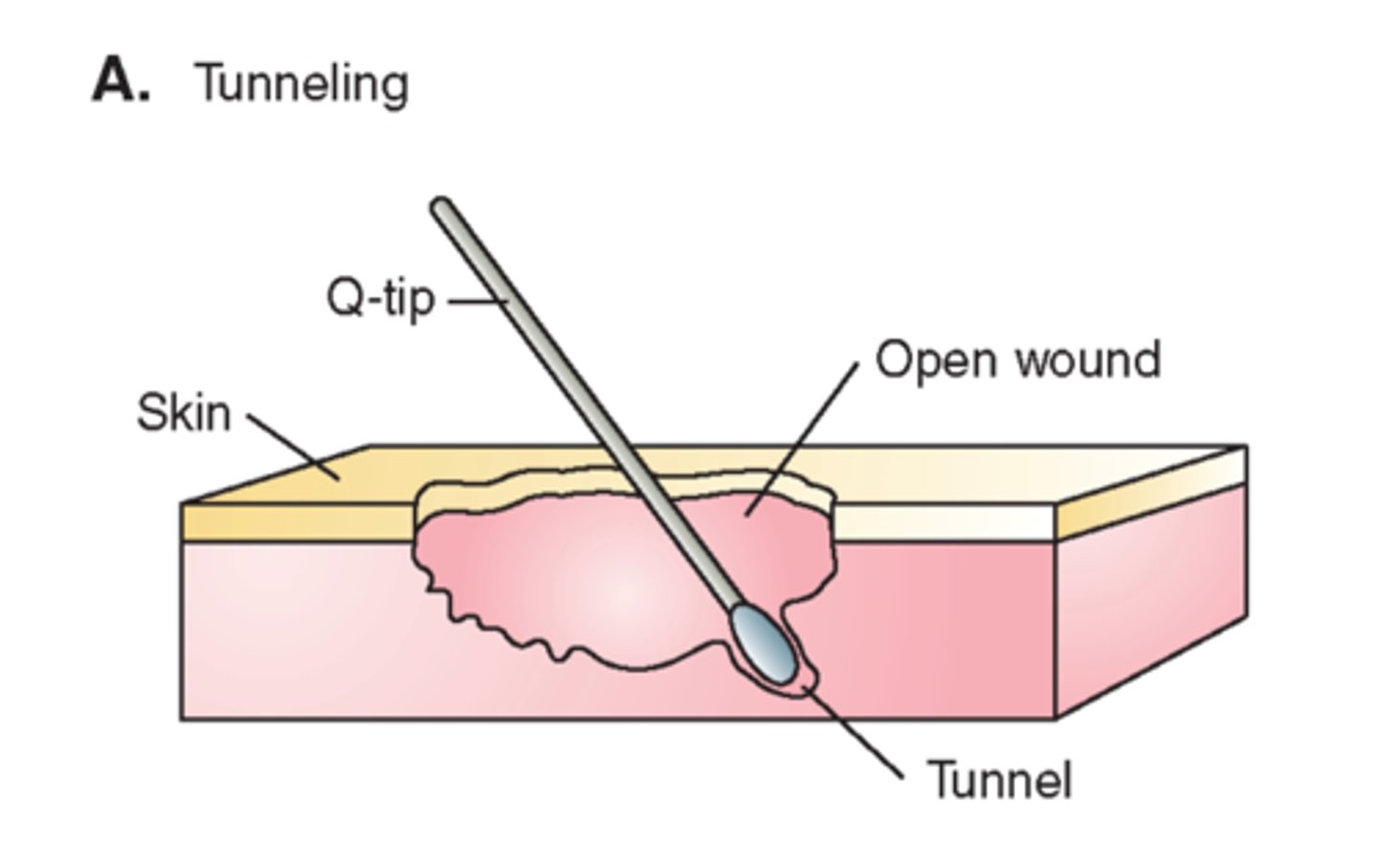
tunneling (wound)
subcutaneous opening or tract/tunnel under the wound surface in any direction
*insert sterile cotton-tipped applicator for depth/length of tunnel
**measure in cm at o'clock positioning
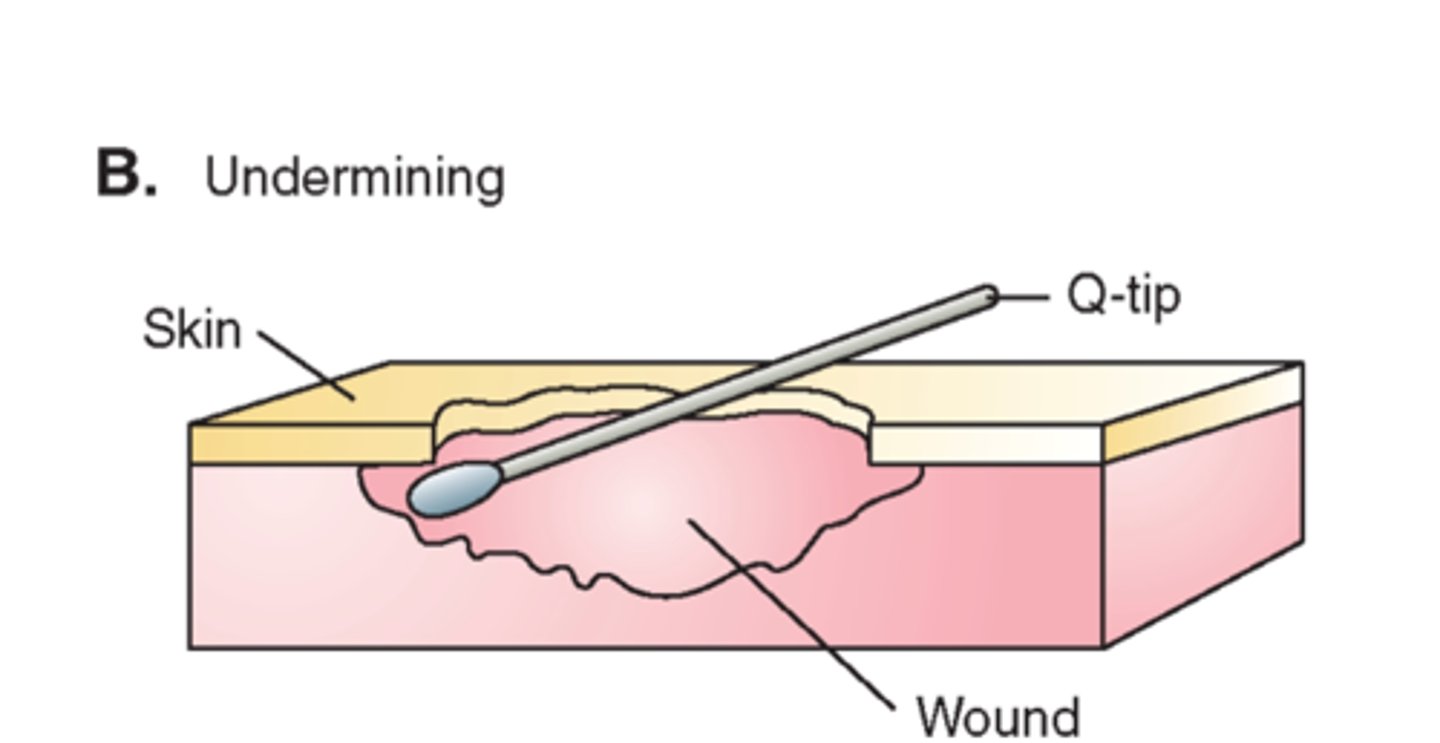
undermining
erosion of tissue from underneath intact skin at wound edge
*insert sterile cotton-tipped applicator for depth
**measure in cm at o'clock positioning
necrotic tissue
WOUND BED ASSESSMENT
gangrene--> dead/decaying tissue
*usually greenish-black color
**can be dry or wet

eschar
WOUND BED ASSESSMENT
dry, hard, very adherent "scab" with some degree of thickness
*black, yellow/brown
**DO NOT REMOVE FROM ARTERIAL WOUND

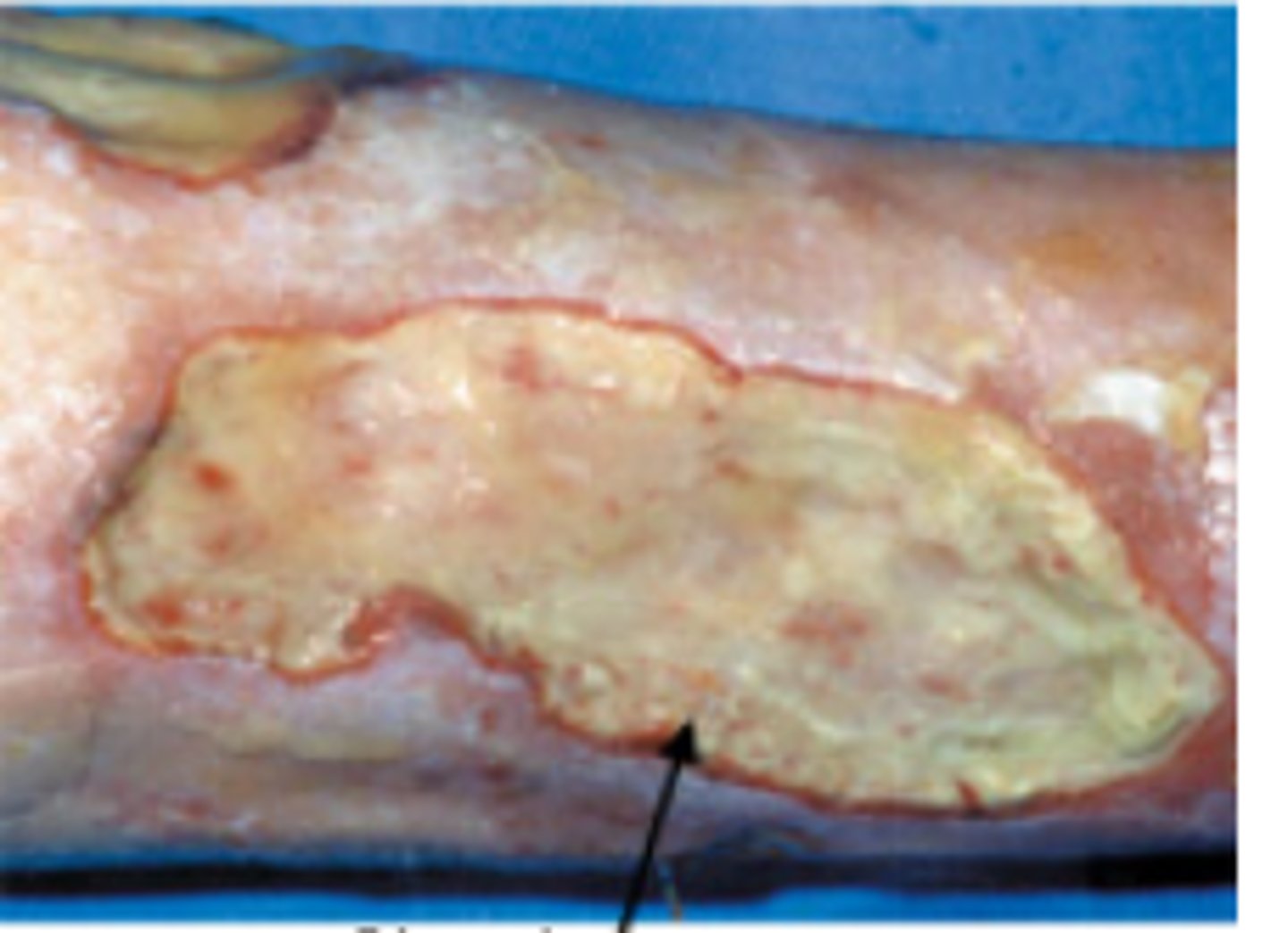
slough
WOUND BED ASSESSMENT
fibrin, degraded extracellular matrix proteins, exudates, white blood cells, and bacterial
*usually yellow/white color
**stringy, may be moist or dry; both have some degree of adherence
GET RID OF TO ALLOW WOUND TO HEAL
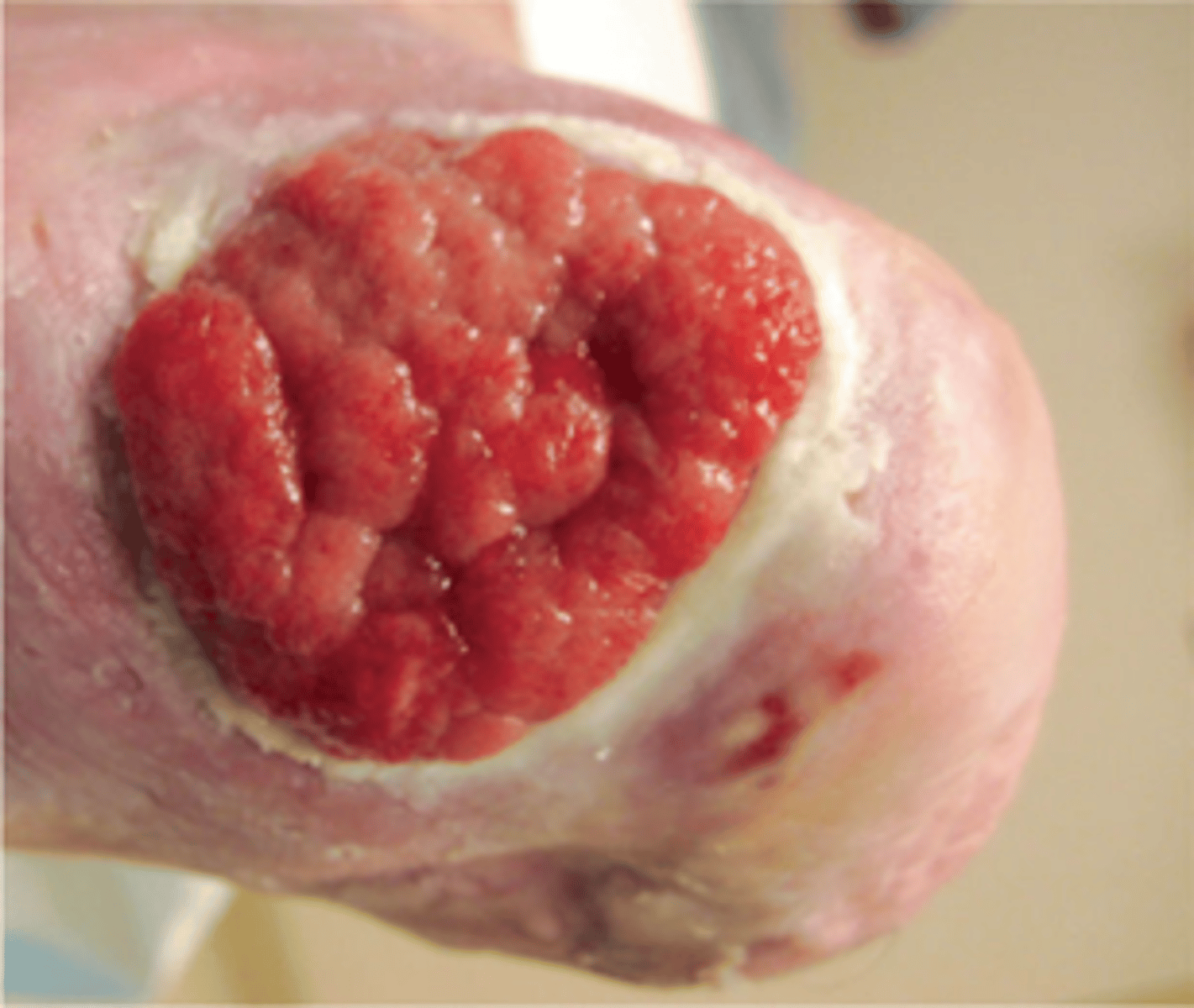
granulation tissue
WOUND BED ASSESSMENT
healthy, living, vascular tissue
"beefy red" or dark pink
*uneven texture

hypergranulation tissue
WOUND BED ASSESSMENT
granulation tissue that overgrows above the edges of the epithelializing tissue
*often due to infection or excessive moisture
**will impede healing unless treated
epithelial tissue
WOUND BED ASSESSMENT
new growth of epidermis stratum basal
*faint purple
**speed of occurrence (0/5-1 mm/day)

percentage of each (ex. 60% healthy, 40% necrotic)
How are types of tissue present within a wound bed measured/documented?
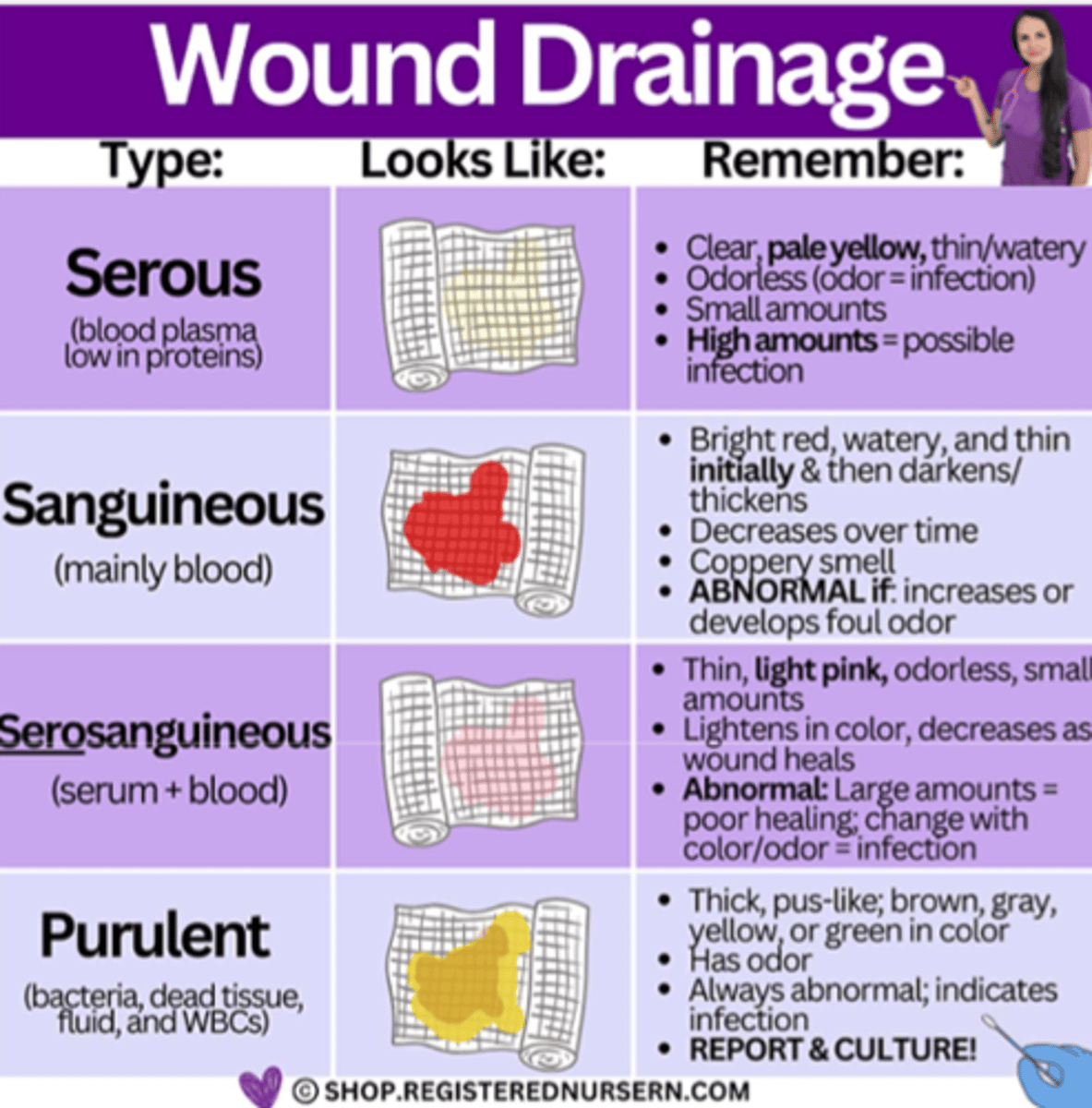
wound drainage assessment
normally expected during inflammatory response in the absence of infection
*can indicate an infection*
1. AMOUNT
- minimal
- moderate
- copious
2. TYPE
- serous (clear, watery)
- serosanguinous (thin, red)
- purulent
3. ODOR
- absent/present
- mild/strong
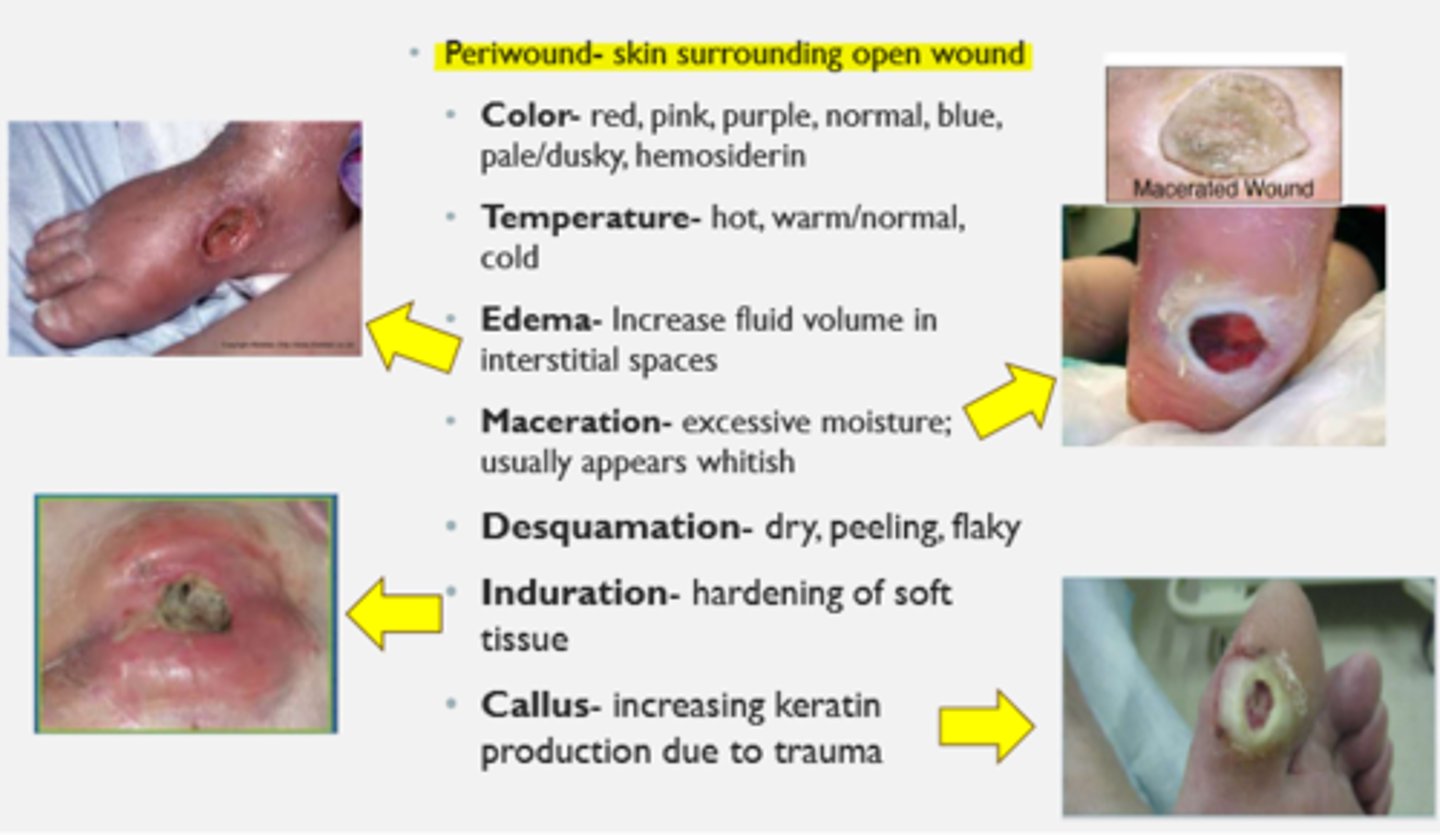
periwound assessment
skin surrounding open wound
- color: red, pink, purple, normal, blue, pale/dusky, hemosiderin
- temperature: hot, warm/normal, cold
- edema: increase fluid volume in interstitial spaces
- maceration: excessive moisture, appears whitish
- desquamation: dry, peeling, flaky
- induration: hardening of soft tissue
- callus: increasing keratin production due to trauma
epibole
rolled under edges of wound
*inhibits healing

denuded skin
loss of integrity (usually epidermis) often presenting with damaged, removed, or lost skin layer
- result from trauma
- often appear red, raw, moist
- may be confused with pressure ulcers (friction) or incontinence-associated dermatitis (secondary to body fluids)

excoriated skin
erosion of the skin caused by scratching, rubbing, etc.
*typically appear as a linear scrape or abrasion

wound additional assessment components
- ROM
- strength
- positioning
- pulses
- gait assessment
- special tests
[rubor dependency, capillary refill, venous filling, claudication, ABI (normal = 1.0-1.4), pain level]
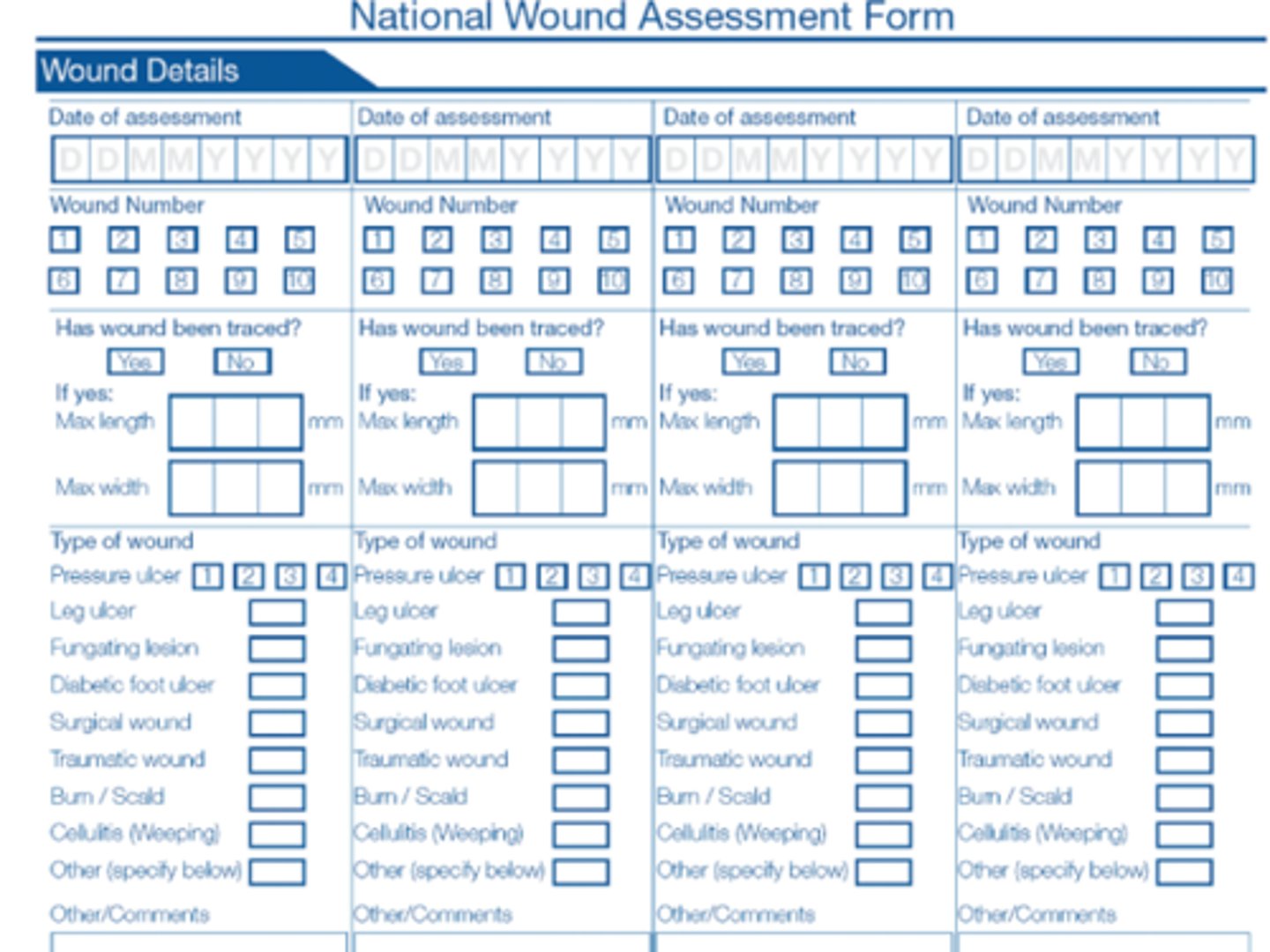
wound assessment forms
1) National Wound Assessment Form
(every discipline uses - including PT)
2) Braden Scale
(nursing documentation - pressure ulcers)
venous insufficiency ulcers
MOST COMMON TYPE OF CHRONIC WOUND
caused by incompetent valves in deep, superficial, and/or perforator veins
- regurgitation
- increased venous pressure
- damage to capillaries
hemosiderin staining--> edema and seepage of red blood cell components and fibrinogen into surrounding tissues
CHARACTERISTICS:
- gaiter area
(medial supramalleolar aspect of LE)
- edema
- shallow, irregular borders
- mod to heavy exudate, weeping
- little to no eschar

venous ulcer treatment
- leg elevation
- strengthening to gastroc/soleus complex
(improve calf mm pump)
- compression therapy (30-40 mmHg)
*must rule out arterial disease
- debridement
(biofilm, slough)
- wound dressing goals
(clean, and moisture management)
0.8-1.2 (<0.8 = PAD, >1.2 = noncompressible calcified or fibrotic vessels)
What is the safe ABI range?
arterial/ischemic ulcers
caused by occlusive disease leading to poor tissue perfusion due to peripheral arterial disease (PAD)
CHARACTERISTICS:
- pale wound base
- necrotic eschar (gangrene)
- dry (minimal drainage)
- well demarcated with symmetrical edges/borders
(punched out edges)
- deep
- painful (rest & claudication)
____________
- shiny, hairless skin
- thick, brittle nails
- diminished/absent pulses
- + rubor dependency
- ABI <0.9
*distal extremities, lateral malleolus, dorsal foot/toes
**CHECK PULSES
tissue perfusion measures
1) ABI (ankle-branchial index)
2) tcPO2 (transcutaneous partial pressure of oxygen)
3) laser doppler flow measure
4) indocyanine green fluorescent imaging (CIG)
debridement (non-healing and infection risk), compression therapy (risk of obliterating main LE artery)
What 2 interventions are contraindicated for a patient with an arterial wound?
(
arterial ulcer treatment
GOAL = RE-ESTABLISH VASCULARIZATION
- surgical or pharmacologic intervention
- wound dressing goals : clean and moisture management
- ambulation program
- open chain exercises
- modalities
NO:
- debridement
- leg elevation, smoking, exposure to cold, caffeine (avoid vasoconstriction)
cilostazol (pletal)
pharmacologic management for intermittent claudication
1. antiplatelet
2. vasodilator
USE--> improve walking distance and speed in patient with IC
SIDE EFFECTS--> GI upset, HA, dizziness, tachy, HTN, malaise
CONTRAINDICATIONS--> CHF
diabetic (neuropathic) ulcers
MOST COMMON CAUSE OF LE AMPUTATION
CONTRIBUTING FACTORS:
- neuropathy
- PAD
- structural deformities
- altered biomechanics
(Charcot foot)
COMMON LOCATION--> feet and toes
*metatarsal heads, hallux, plantar surface
**usually caused by pressure due to improper footwear
***thick CALLOUS usually present

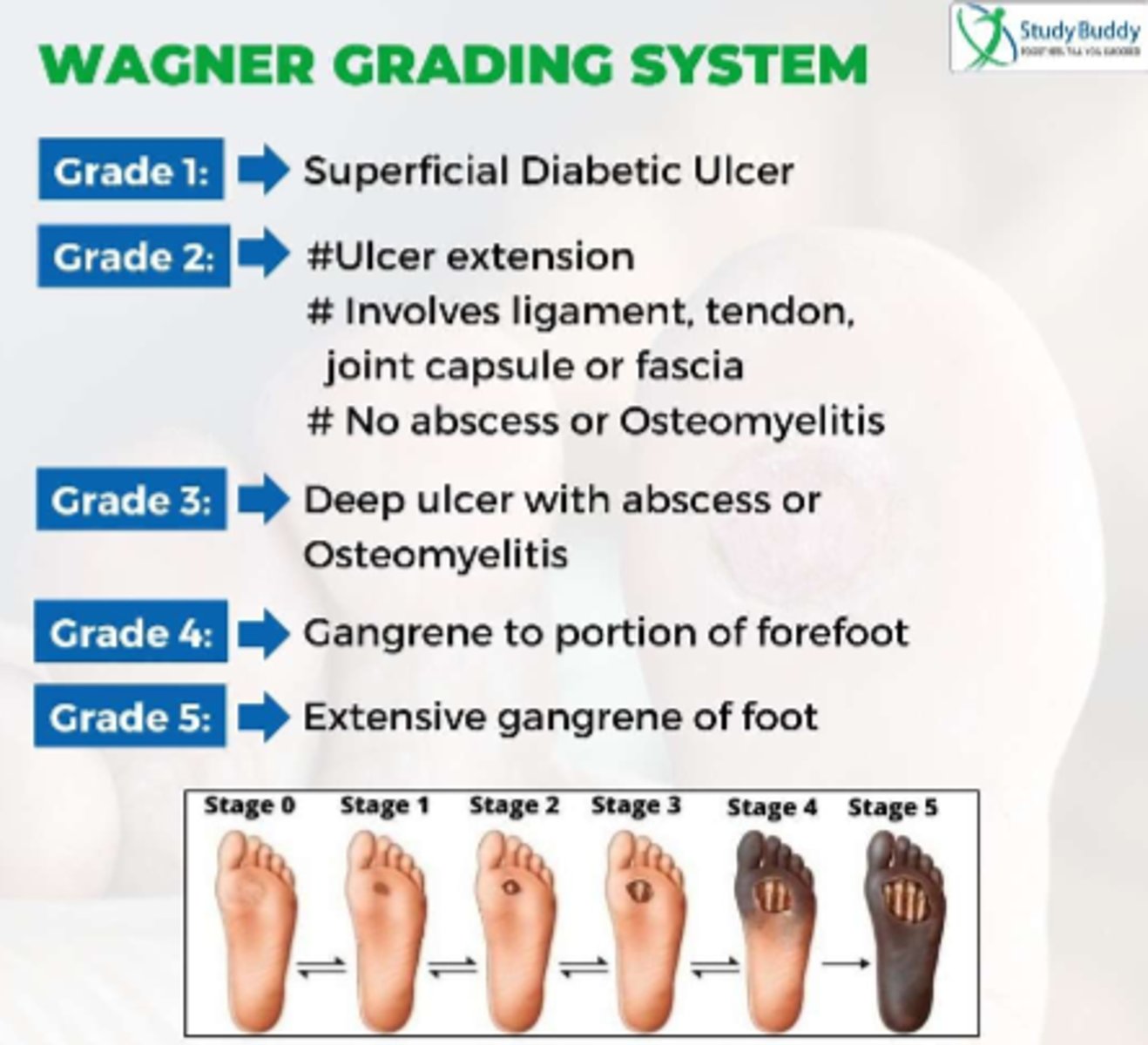
Wagner Grading System
assesses diabetic ulcer depth and the presence of osteomyelitis or gangrene using different "grades"
diabetic ulcer treatment
- control blood glucose levels
(<150 for wound healing, A1C <8%)
- management of any PAD
- surgical debridement of any thick callus
- OFFLOADING IS ESSENTIAL
(footwear or total contact cast)
- nutrition
- foot, ankle ROM, strengthening, & balance exercises
- daily foot checks, proper foot care and shoes

hyperkeratosis (callus)
APPEARANCE:
- whitened
(macerated around a wound)
- translucent
(dry)
- hemorrhagic
(tissue trauma underneath, shearing and bleeding under callus)
TOOLS FOR REMOVAL:
- dremel sanding discs or cone
- pedicure clippers
- forceps, scissors, blade
- specific antiseptic cream applied, easier to remove callus
needs to be removed for a wound to heal

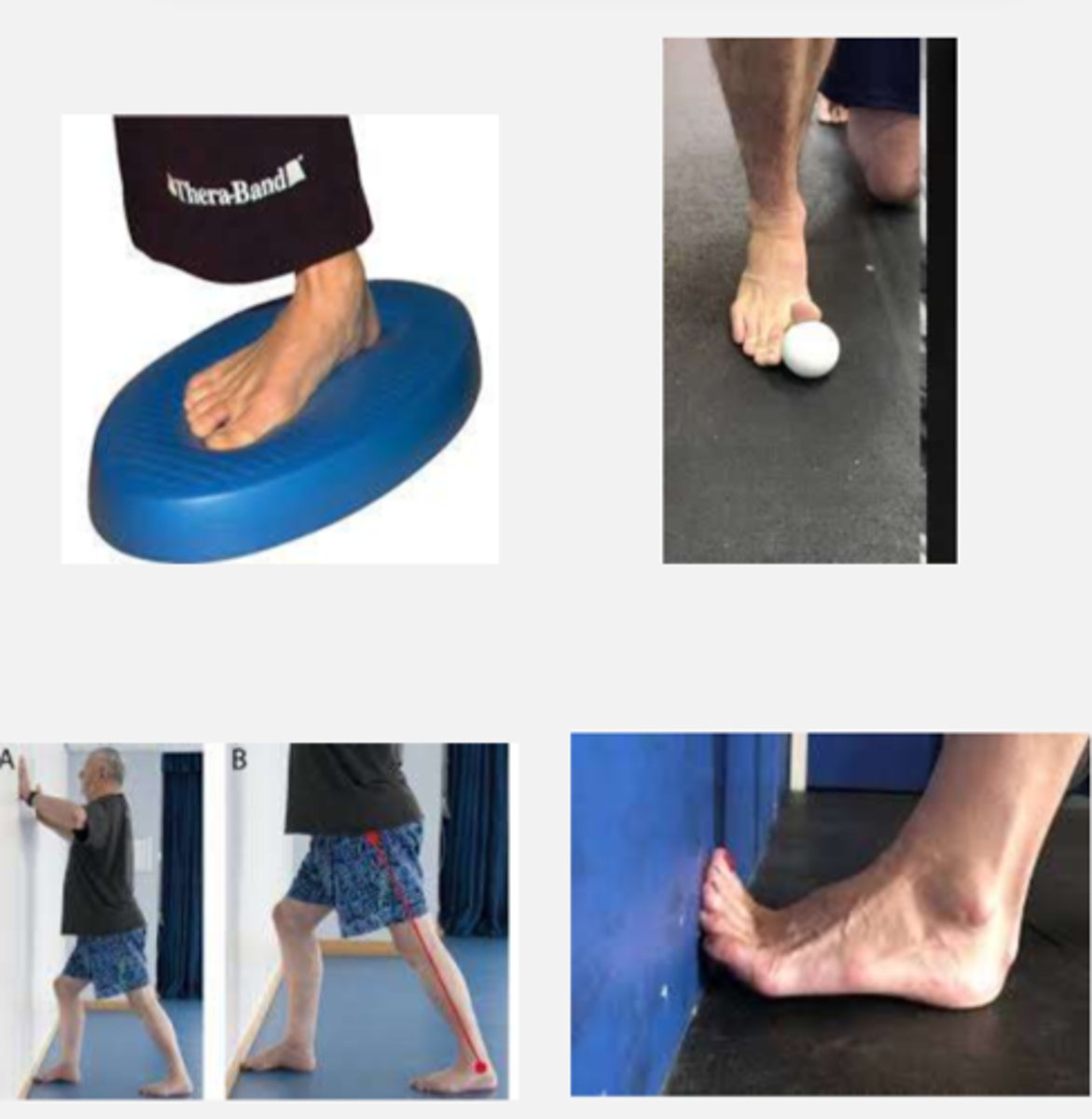
therapeutic exercise (wound)
- toe, foot, and ankle mobilization
- hallux/toe stretching into extension
- extensor strengthening exercises
- gastroc stretching
- DF strengthening exercise
- stretching and strengthening in any other areas of limited ROM and weakness
- static and dynamic balance, proprioception, ambulation on uneven surfaces
- assistive device training
- endurance/cardiorespiratory fitness
wash feet in warm water, dry completely, moisturize
What are the 3 most important steps in a daily skin & nail care routine?
pressure ulcer
localized area of tissue necrosis that develops when soft tissue is compressed between a bony prominence and an external surface for a prolonged period of time
high risk areas = any bony prominence
STAGING RULES:
- DO NOT reverse stage during documentation of the healing process
- UNSTAGEABLE if necrotic tissue is covering true depth
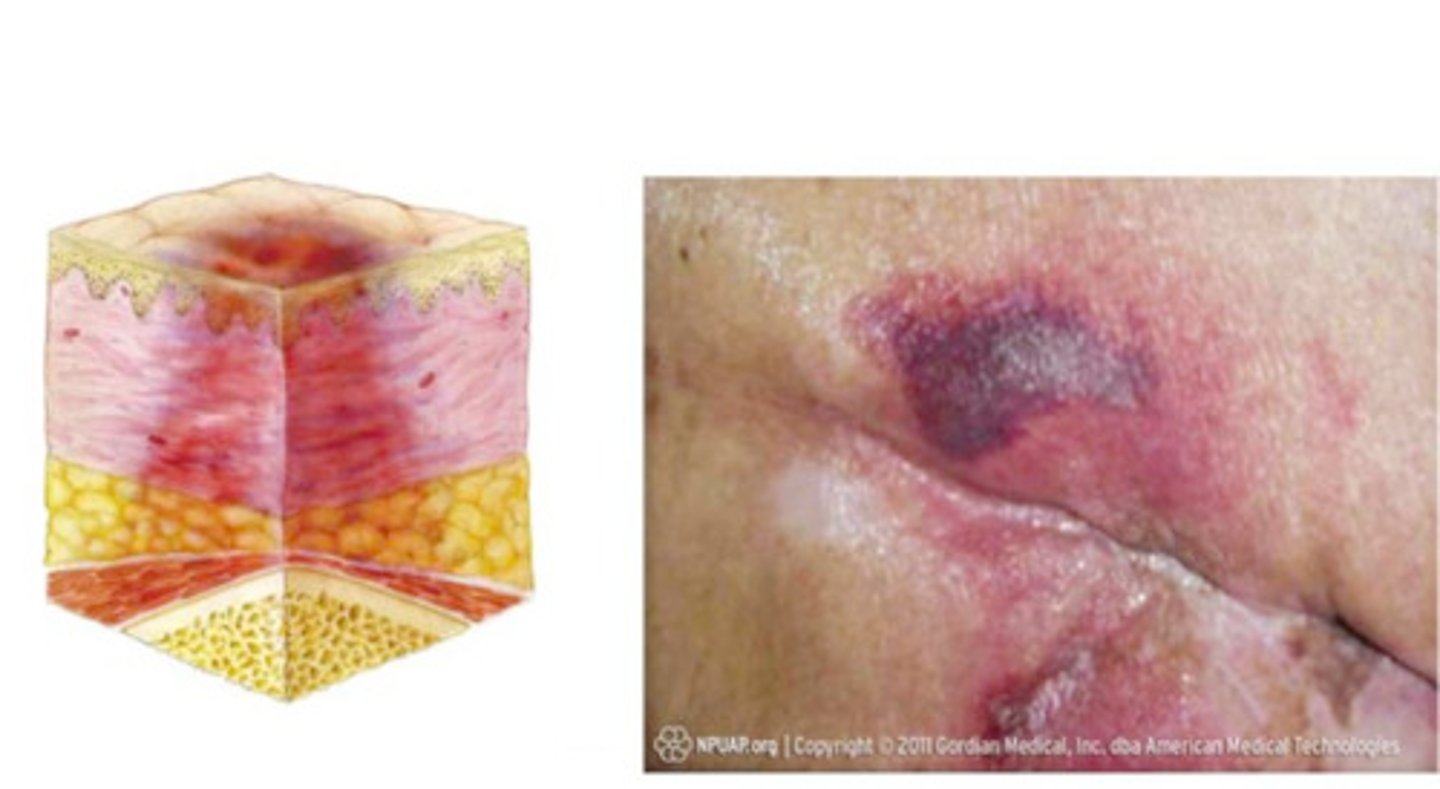
deep tissue pressure injury
persistent non-blanchable deep red, maroon, or purple discoloration
NO (impedes blood flow to contact area and will worsen existing ulcer)
Should you recommend the use of donut style cushion for a sacral pressure injury?
pressure injury contributing factors
1) pressure
- can result in ischemia/hypoxia causing cell damage
2) sheer forces & friction
*keep HOB <30 degrees to prevent sliding and reduce
**maintain best practice for proper positioning and turning techniques
3) moisture
- can result in a decrease in skin integrity
pressure injury treatment
PRESSURE REDISTRIBUTION
- every 2 hrs, 30 degree angles
- adequate hydration and nutrition
- keep bony prominences apart and off support surfaces
- pressure reducing support surfaces

wound summary
REFER TO IMAGE

wound infection
S/Sx:
- erythema
- edema
- change in character/increase in drainage
- change in pain
- increased odor
- fever
- altered mental status
- increased WBC count
- delay in healing
TREATMENT:
- systemic antibiotics
- removal of surface bacteria (if able)

contamination
the presence of non-replicating microbes in the wound
*NO adverse impact on wound healing
**ALL OPEN WOUNDS ARE CONSIDERED THIS
colonization
presence of multiplying microorganisms w/o evidence of infection
*all chronic wounds have some degree of this
**once at critical level, wound healing stalled > halted
infection
the presence of multiplying microorganisms WITH s/s of disease in the wound
*microbes have invaded healthy tissue and start to destroy cells and cause host response
**NOT all wounds are considered this
culture
a test to determine microbial presence (bacterial, viral, or fungal) that may cause an infection

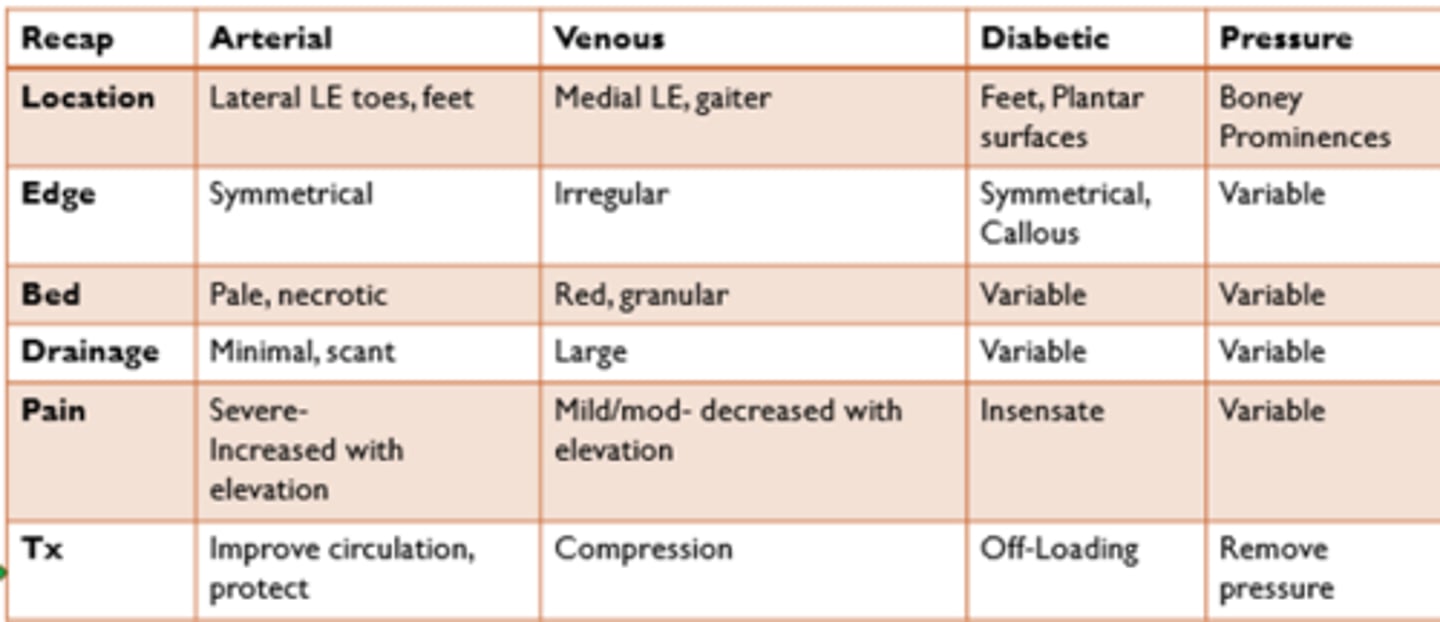
wound key characteristics and management
TYPES:
- arterial
- venous
- diabetic
- pressure
REFER TO IMAGE
sterile technique
involves strategies to reduce and maintain objects and areas as free from microorganisms as possible
KEY STEPS:
1. meticulous handwashing
2. use of sterile field
3. sterile gloves for application of sterile dressing
4. sterile instruments
*required with sharp debridement and pulse lavage with suction (PLWS)

clean technique
involves strategies to reduce the overall number of microorganisms or to prevent or reduce the risk of transmission of microorganisms from one person to another or from one place to another
KEY STEPS:
1. meticulous handwashing
2. clean environment & field
3. clean gloves
4. sterile instruments

aseptic technique
APPLICATION: when treating multiple ulcers on the same patient, attend to the most contaminated ulcer last
tissue debridement, infection control, moisture balance, edge of wound
What does the TIME principle stand for in the treatment of wounds?
biofilm
According to the NIH, 80% of wound infections are due to what?
tissue debridement
TYPES:
1) surgical
- use of forceps or scalpel
2) mechanical
- use of mechanical force
ex. pulse lavage, irrigation
3) autolytic
- natural process by which endogenous phagocytic cells and proteolytic enzymes break down necrotic tissue
4) enzymatic
- involves topical agents containing proteolytic enzymes to break down necrotic tissue
5) biologic
- use of sterile larvae/maggot
- often used in large wounds
(offers painless removal of necrotic tissue)
mechanical
Which type of tissue debridement is considered to be non-selective?
HINT: removes both healthy and devitalized tissue
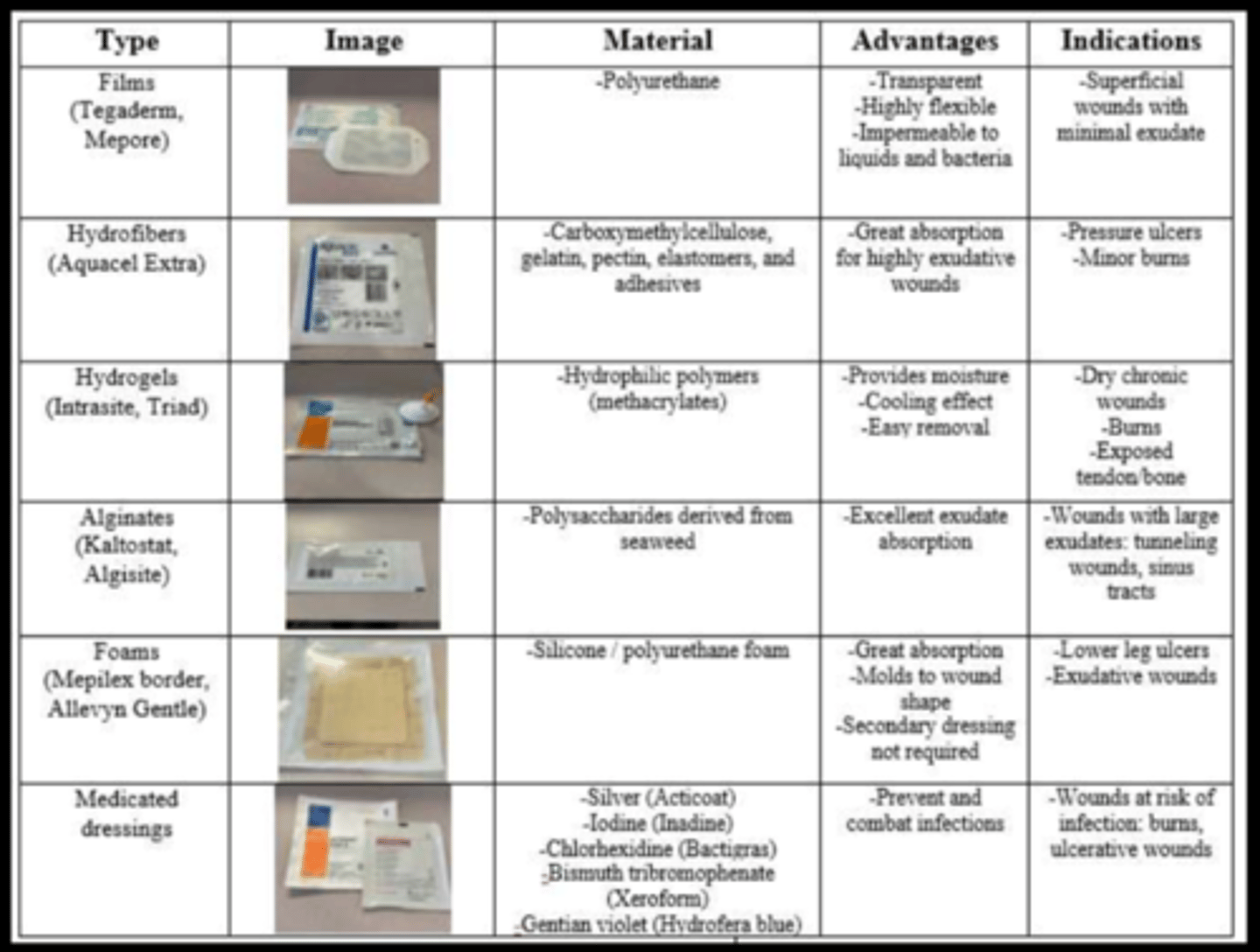
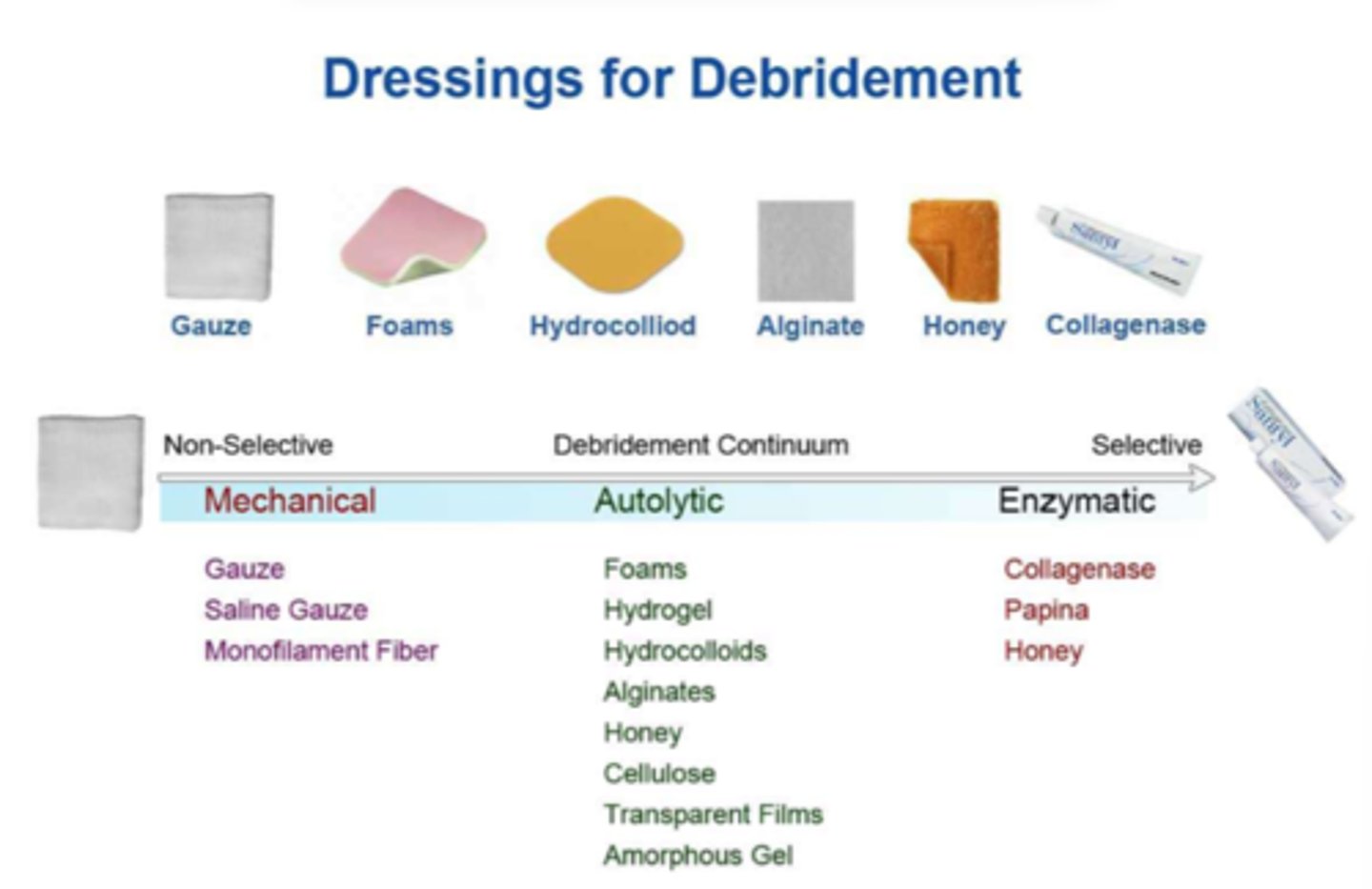
dressing types
1) hydrogels
- minor burns, painful wounds, dry wounds
2) films
- shallow or minor wounds, may be used as secondary dressing
3) alginates
- medium-to-high exuding wounds
4) foams
- medium-to-high exuding wounds, pressure ulcers, mold for grafts, venous ulcers w/ compression
5) hydrocolloids
- small solitary non-draining wounds, light to moderate exudate wounds, after debridement, granulating wounds
ADVANCED:
- PROMOGRAN PRISMA
(freeze-dried composite of collagen, oxidized regenerated cellulose and silver--> for wounds with no necrotic tissue)
- Hydrofera Blue
(combines methylene blue and gentian violet to manage bioburden for all wound types --> antibacterial protection)
- Honey
(natural biologic wound dressing w/ broad-spectrum antibacterial activity)