Shock Syndromes
1/80
Earn XP
Description and Tags
Dr. McMath
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
81 Terms
How is shock characterized?
Inadequate global tissue perfusion
Is the presence of hypotension required to define shock?
Nope!!
What are the 4 etiologic mechanisms of shock?
Hypovolemic
Cardiogenic
Obstructive
Vasodilatory/Distributive
What should be measured in all patients in whom shock is suspected?
Blood lactate
Why should blood lactate be measured when shock is suspected?
Lactate increases in shock primarily due to reduced O2 delivery to the tissues, leading to anaerobic metabolism and increased lactate production
For circulatory insufficiency associated with hemodynamic instability, what is the first-line fluid of choice?
Crystalloid solutions
When volume resuscitation fails in patients with shock, in order to maintain adequate blood pressure and hypoperfused tissues, what therapy is required?
Vasopressors and inotropes
What is the preferred initial vasopressor for shock?
Norepinephrine
In terms of SBP and MAP, what is the defining values that determine diagnosis of shock?
SBP < 90 mmHg, MAP <70 mmHg with tachycardia and organ perfusion abnormalities
Preload
All factors that contribute to passive ventricular wall stress (or tension) at the end of diastole
Volume of blood in the ventricles at the end of diastole
Afterload
All the factors that contribute to total myocardial wall stress (or tension) during systolic ejection
Pressure that must be overcome by the ventricles during systole
When does circulatory shock develop?
When cardiovascular system is unable to deliver an adequate oxygen supply to meet tissue oxygen demands resulting in cellular dysfunction
What are the two main consistencies throughout all shock syndromes?
Inadequate tissue and organ perfusion
When is lactate considered evidence of end organ dysfunction in shock?
> 2 mmol/L
When is INR / aPTT considered evidence of end organ dysfunction in shock?
INR > 1.5
aPTT > 60 seconds
When is platelet count considered evidence of end organ dysfunction in shock?
< 100,000
When is bilirubin considered evidence of end organ dysfunction in shock?
> 2 mg/dL
When is creatinine considered evidence of end organ dysfunction in shock?
> 2 mg/dL (damage to the kidneys)
When is urine output considered evidence of end organ dysfunction in shock?
< 0.5 mL/kg/hour x 2 hours
When is SBP and MAP considered evidence of end organ dysfunction in shock?
SBP < 90 mmHg, or decreased more than 40 mmHg from previously recorded patient normal
MAP < 70 mmHg
Vasodilatory/distributive shock
Tissue hypoperfusion resulting from decreased systemic vascular resistance (SVR)
What is the most common type of shock?
Distributive shock
Cardiogenic shock
Results from a loss in pump function, through decreased cardiac contractility (e.g., MI), acute valvular abnormality, or an arrhythmia (e.g., ventricular tachycardia)
heart is not pumping correctly
Hypovolemic shock
Inadequate venous return, from internal or external loss of intravascular fluids (e.g., trauma, surgery, or hemorrhage), resulting in insufficient cardiac preload and decreased stroke volume
not enough blood to go around
Obstructive shock
Extracardiac obstruction to blood flow into or out of the heart, such as tension pneumothorax, cardiac tamponade, or pulmonary embolism
How does hypovolemic shock affect Preload, CO, and Afterload?
Preload ↓
CO ↓
Afterload ↑
How does cardiogenic shock affect Preload, CO, and Afterload?
Preload ↑
CO ↓
Afterload ↑
How does obstructive shock affect Preload, CO, and Afterload?
Preload ↑
CO ↓
Afterload ↑
How does vasodilatory/distributive shock affect Preload, CO, and Afterload in pre-resuscitation?
Preload ↓
CO ↓
Afterload ↓
How does vasodilatory/distributive shock affect Preload, CO, and Afterload in post-resuscitation?
Preload ↑
CO ↑
Afterload ↓
In hypovolemic shock, what is the target?
Preload
In cardiogenic shock, what is the target?
Inotrope
In obstructive shock, what is the target?
Not specific, pharmacotherapy is limited (e.g., surgery, fibrinolytic)
In vasodilatory/distributive shock, what is the target?
Afterload
What is afterload?
Pressure that the ventricles must overcome in order to eject the blood into circulation
Symptoms seen in shock syndromes
Not very profound
Dizziness
Light-headedness
Confusion
Low urine output
Signs seen in shock syndromes
Tachycardia (e.g., HR > 120 bpm) — heart trying to compensate for poor CO
Tachypnea (e.g., RR > 30 rpm)
Hypotension (not always diagnostic)
Body temperature abnormalities
Impaired capillary refill time (e.g., > 3 seconds) — low fill state
AMS up to obtundation — decline in mental state
Laboratory tests for shock diagnoses
Blood lactate (e.g., > 2 mmol/L)
Serial lactate concentrations are recommended in the early phases of shock treatment because lactate clearance and normalization correspond with improved global tissue perfusion
Evidence of end-organ hypoperfusion — ↑ bilirubin, ↑ creatinine, ↑ INR
Anemias in bleeding
Positive cardiac troponin with acute MI — cardiogenic shock
MAP
Average pressure throughout one cardiac cycle → one cardiac cycle = systole & diastole
Functions to perfuse blood to all the tissues of the body to keep them functional
Should remain at least 60 mmHg so that blood can effectively reach all tissues
Measured via usage of an arterial line
MAP = [SBP + (2 x DBP)] / 3
What is the MAP goal when treating patients with shock?
≥ 65 mmHg
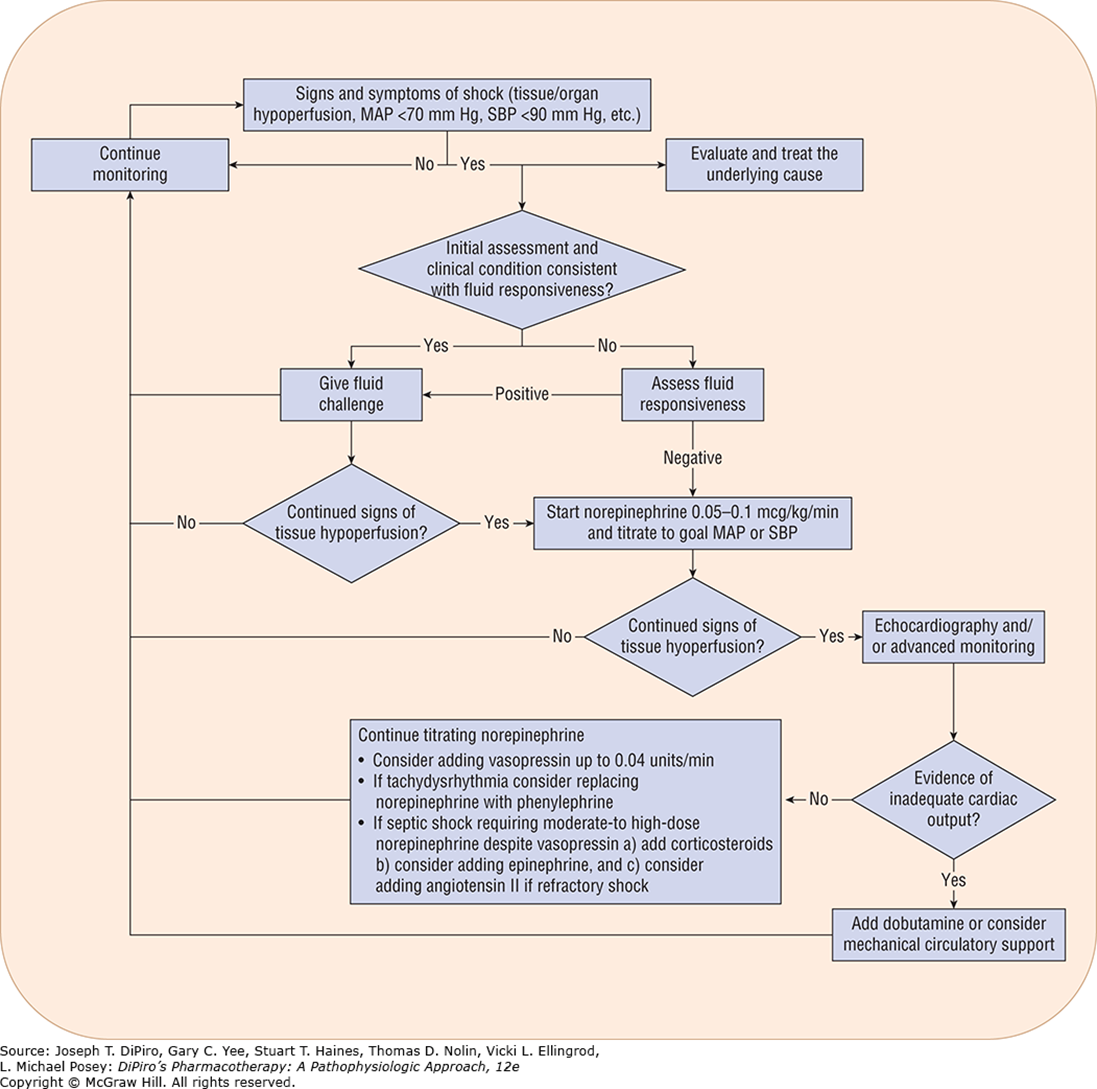
Treatment algorithm for shock syndromes
What are blood products used for in the treatment of shock?
Predominantly associated with acute large volume blood loss
What is the goal of administering IV fluids when treating shock?
↑ SV
↑ CO
↑ DO2
↑ BP
Passive Leg Raise (PLR)
Transiently increases venous return in patients who are preload responsive, as such it is a diagnostic test not a treatment
Predictor of fluid responsiveness (i.e., helps identify patients who are on the ascending portion of their starting curve and will have an increase in SV in response to fluid administration)
When using crystalloid solutions such as NS or LR, how much fluid should there be in the interstitial and intravascular compartments?
Interstitial: 750 mL
Intravascular: 250 mL
What is the major indication for using NS or LR?
Intravascular volume expansion
In distributive (septic) shock, what is the dose for fluid resuscitation?
Start with 30 mL/kg IV crystalloid (based on ABW)
> 30 mL/kg in total may be needed to obtain goal MAP, reverse global hypoperfusion, or achieve clinical indication of regional organ-specific perfusion
What has been known to occur with excess fluid administration in septic shock?
Higher mortality, especially in patients with heart failure or impending pulmonary edema
Why is it harmful to give fluid resuscitation beyond minimal levels in patients with penetrating abdominal trauma?
Hemodilution and clot destabilization (risk of bleeding to death)
T/F: In hemorrhagic/traumatic shock, fluids should be given in small aliquots to yield a palpable pulse and to maintain MAP no more than 60 mmHg and SBP no more than 90 mmHg based on accurate measurements (e.g., arterial monitoring).
True
What is the fluid of choice in hemorrhagic/traumatic shock therapy, due to being associated with a lower risk of adverse effects?
Isotonic crystalloids
What solutions should be avoided in patients with severe TBI as it may worsen cerebral edema?
Balanced salts solutions
What causes an increase in sympathetic tone in hypovolemic shock?
Decreased preload directly reduces cardiac output, which activates baroreceptors
If hypovolemic shock is left untreated, what will happen?
Circulatory shock will continue
Complications associated with hypovolemic (hemorrhagic) shock
Loss of RBCs may further ischemic damage to vital organs (i.e., end organ damage)
Clotting factors and platelet counts may also be reduced in presence of hemorrhage
Dilutional effect with crystalloid resuscitation can further decrease clotting activity
Coagulopathy persists and is often accompanied by acidosis and hypothermia, leading to the “lethal triad”
What 2 pharmacotherapy options are required in patients with shock, when volume resuscitation is not indicated or fails to maintain adequate BP (MAP ≥ 65 mmHg) and organs and tissues remain hypoperfused?
Vasopressors and Inotropes
What can be used to temporarily treat life-threatening hypotension when tissue perfusion is inadequate despite ongoing aggressive fluid resuscitation?
Vasopressors
Norepinephrine as pharmacotherapy for shock
Combined strong α1 activity and less potent β1 agonist effects; Weak vasodilatory effects of β2 stimulation
↑ MAP, ↑ SVR
↓ HR due to reflex bradycardia from ↑ SVR
↑ Cardiac filling pressure by ↑ venous return through via vasoconstriction (i.e., its more prominent α effects on all vascular beds)
Inconsistent effect!
Dosing of Norepinephrine IV for shock therapy
Start when MAP ≤ 65 mmHg and/or adequate tissue perfusion is not achieved with fluid resuscitation
Initial → 0.05 to 0.1 mcg/kg/min (titrate to goal MAP)
Usual range → 0.025 to 1 mcg/kg/min
Max. (for refractory shock) → 1 to 3.3 mcg/kg/min
What is the absolute maximum dose for IV norepinephrine?
3.3 mcg/kg/min
Epinephrine as pharmacotherapy for shock
Adjunctive therapy to Norepinephrine
Associated with tachydysrhythmias and lactate elevation
Combined α and β effects
What pharmacotherapy would be preferred if a patient has anaphylactic shock requiring β stimulation for opening the airways?
Epinephrine, due to β effects
Dosing of Epinephrine IV for cardiogenic shock therapy
0.01 to 0.5 mcg/kg/min; titrate based on clinical end point (e.g., BP, end-organ perfusion)
Dosing of Epinephrine IV for post-cardiac arrest shock therapy
0.01 to 1 mcg/kg/min; titrate based on clinical end points (e.g., MAP, end-organ perfusion)
Max. (for refractory shock) → 2 mcg/kg/min
Dosing of Epinephrine IV for septic shock & other vasodilatory shock states (adjunctive agent) therapy
0.01 to 0.2 mcg/kg/min; titrate to goal MAP or end-organ perfusion
Usual range → 0.01 to 0.5 mcg/kg/min
Max. (for refractory shock) → 0.5 to 2 mcg/kg/min
Phenylephrine as pharmacotherapy for shock
Should not be used as an initial vasopressor in shock patients with impaired myocardial performance
A pure α1 agonist; increases blood pressure primarily through vasoconstriction (via IV)
Dosing of Phenylephrine IV for septic shock & other vasodilatory shock states (adjunctive agent) therapy
0.5 to 2 mcg/kg/min; titrate to desired MAP
Usual range → 0.25 to 5 mcg/kg/min
Dosing of Phenylephrine IV for cardiogenic shock therapy
Not ideal — concern for issues in the myocardium
0.1 to 10 mcg/kg/min; titrate to clinical end point
Dobutamine as pharmacotherapy for shock
Selective β1 agonist with mild β2 and α activity
Strong inotropic activity without concomitant vasoconstriction
Greater increase in CO compared to dopamine and is less arrhythmogenic
What are optimal uses of Dobutamine in shock therapy?
In patients with low CO and high filling pressures (e.g., left ventricular dysfunction demonstrated with echocardiography) or ongoing signs of global/regional hypoperfusion despite adequate resuscitation
What types of shock is Dobutamine primarily used?
Septic and cardiogenic shock; ↑ CO
What is the typical increase range for CO with Dobutamine treatment in septic/cardiogenic shock?
25% to 50%
Dosing of Dobutamine for inotropic support
Initial: 2 to 5 mcg/kg/min; titrate based on clinical endpoint (e.g., BP, end-organ perfusion)
Usual range → 2 to 10 mcg/kg/min
Max. dose → 20 mcg/kg/min
Vasopressin as pharmacotherapy in vasodilatory/distributive shock
Increases SVR and arterial blood pressure in patients with vasodilatory/distributive shock
Reduction in dosage requirements of catecholamine adrenergic agents (e.g., NE)
Enhances urine production
Dosing of Vasopressin IV for septic shock & other vasodilatory shock states (adjunctive agent)
0.03 units/minute (0.04 units/minute) added to norepinephrine as a fixed dose (not titrated)
Usual range → 0.01 to 0.04 units/minute
>0.04 units/minute for salvage therapy due to potential risk for ischemic complications
What is Angiotensin II?
Naturally occurring peptide hormone of RAAS that causes vasoconstriction and increases aldosterone release, which raises blood pressure and ↑ SVR
When should Angiotensin II be used with extreme caution?
In patients with impaired left ventricular systolic function
What adverse effects are commonly reported with Angiotensin II?
Delirium and lactic acidosis
Dosing of Angiotensin II IV for septic shock & other vasodilatory shock states (adjunctive agent)
10 to 20 ng/kg/minute; titrate by up to 10-15 ng/kg/minute every 5 minutes based on goal MAP
Decrease dose by ≤ 15 ng/kg/minute every 5-15 minutes based on response ONCE SHOCK HAS IMPROVED
Corticosteroids as pharmacotherapy in shock
Improves arterial pressure while minimizing the dosage of catecholamine vasopressors
Use is controversial — optimal dosing ~260 mg/day of hydrocortisone or equivalent
Dosing of Hydrocortisone IV for septic shock, inadequate response to fluid resuscitation and vasopressor therapy
50 mg bolus every 6 hours OR 100 mg every 8 hours for 5-7 days