personality & mental illness
1/20
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
21 Terms
what is mental illness?
significant clinical disturbance in cognition, emotion/emotion regulation, or behaviour
associated with distress & impairment in functioning
due to biological, developmental, and/or psychosocial factors
what is mental health?
state of well-being involving realizing one’s abilities, coping with life stressors, learning/working well, & contributing to one’s community
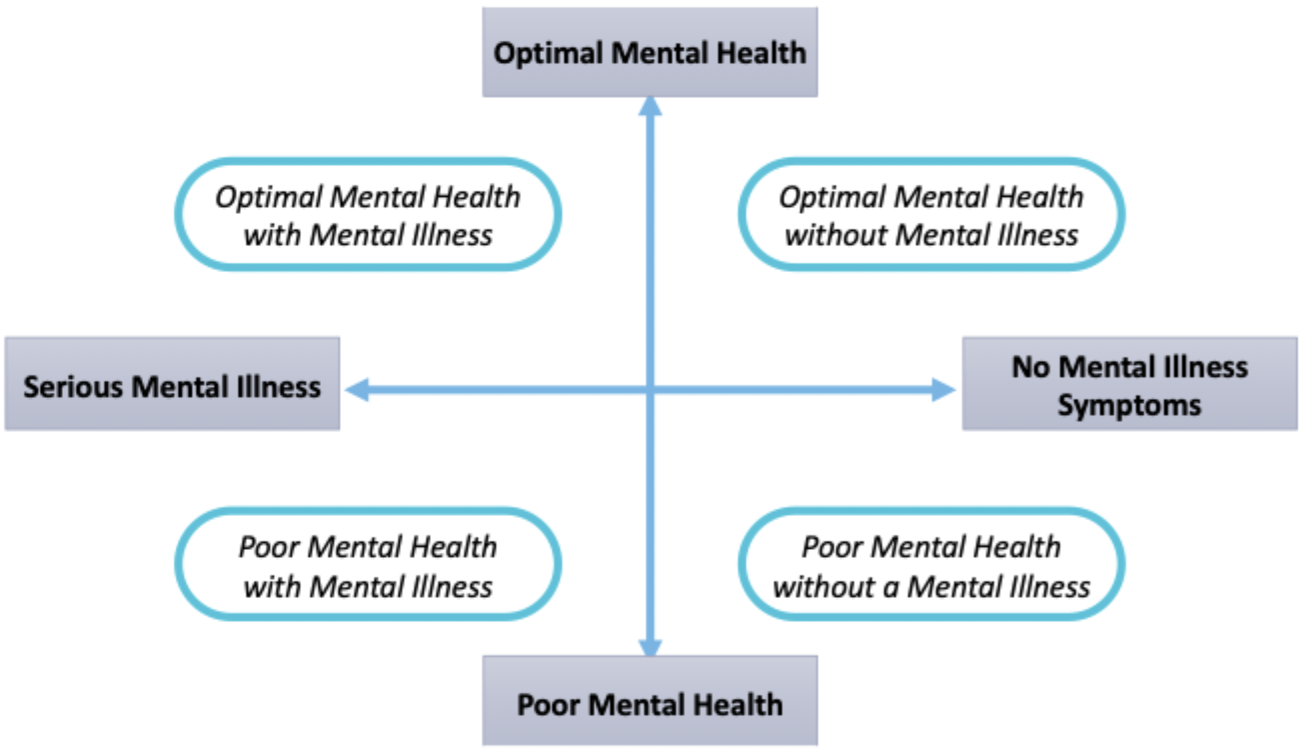
explain the mental health/illness diagram
how is society impacted?
up to 1/8 people will experience mental illness in their lifetime (underestimated)
several estimates are as high as 1/5
~50% of mental health difficulties emerge by age 14
~75% of mental health difficulties emerge by 24
how is stigma tied to mental illness?
a major barrier to help-seeking, treatment, recovery
public stigma
enacted stigma
self-stigma
anticipated stigma
what are the 4 types of stigma?
more extrenal:
public stigma: negative attitudes/views, prejudices, etc.
enacted stigma: discrimination, mistreatment (behavioural in nature)
more internal:
self-stigma: internalization of public stigma
anticipated stigma: expectation of being stigmatized (with or without prior stigma experiences)
what is the general health questionnaire (GHQ)?
brief but reliable measure of mental health
social dysfunction + anhedonia
poor concentration, feeling disconnected, lack of enjoyment
depression + anxiety
feeling unhappy, overwhelmed, under pressure
loss of confidence
feeling worthless
how is the big 5 associated to mental health?
data from >12k participants
high neuroticism
higher levels of ALL GHQ domains
lower extraversion
higher social dysfunction & anhedonia
lower agreeableness & conscientiousness
higher social dysfunction & anhedonia
lower openness
higher depression & anxiety
what is DID?
2 or more distinct identities (aka alters) - each with its own pattern of perceiving, relating to, & thinking about the self/environment
2 or more identities recurrently yielded discontinuity in sense of self and thus changes in affect, behaviour, memory, perception, cognition, etc.
recurrent gaps in memory regarding personal information, daily life events, and/or past trauma (concerning 1 or more identity) - not simple forgetting
what is DID associated with?
PTSD, somatic complaints, depression, anxiety, self-harm, aggression, suicidal behaviour
rate: ~1.5% (based on DSM-5)
rates have been debated historically
what does DID report?
reports of sexual & physical abuse are common
as are reports of repressed memories (often in relation to past trauma)
1+ identity is often hostile/aggressive/protective
amnesia is common (less so for hostile/aggressive identity)
what are treatments for DID?
psychotherapy
promote safe, secure environment & help re-integrate identities
treat comorbid disorders
pharmacotherapy
treat comorbid disorders & symptoms
what are some personality traits & depression?
several traits often implicated… but they are non-specific risk factors
high neuroticism
high self-criticism & perfectionism
low extraversion/positive emotionality
low conscientiousness
part of the personality-depression link may be due to shared etiology
unlikely that depressive episodes yield enduring personality changes…
but, personality may affect the course of depression & it treatments
how is depression treated?
high neuroticism may indicate better response to medication
high agreeableness may indicate better response to psychotherapy
high extraversion may indicate better overall response treatment
high conscientiousness + high openness may indicate better overall treatment response
what is anorexia nervosa?
persistent restriction of energy intake that yields significantly low body weight (relative to one’s age, sex, developmental stage & physical health)
intense fear of gaining weight/becoming obese or enduring behaviours that impact weight gain (even in presence of low body weight)
disturbance in how one views/body shape; very low self-evaluation based on weight; denial/lack of recognition of the seriousness of low body weight
what is bulimia nervosa?
recurrent binge-eating episodes which include:
eating high quantities in short time intervals (more than most:) ~2hrs sense of lack of control over-eating during the episode
recurrent compensatory behaviour to prevent weight gain
induced vomitting, laxative misuse, fasting, excessive exercise
binge-eating & compensatory behaviour occur >= 1 per week for >= 3 months
self-evaluation influenced by body shape/weight
does not occur exclusively during episodes of anorexia nervosa
explain personality & ED models
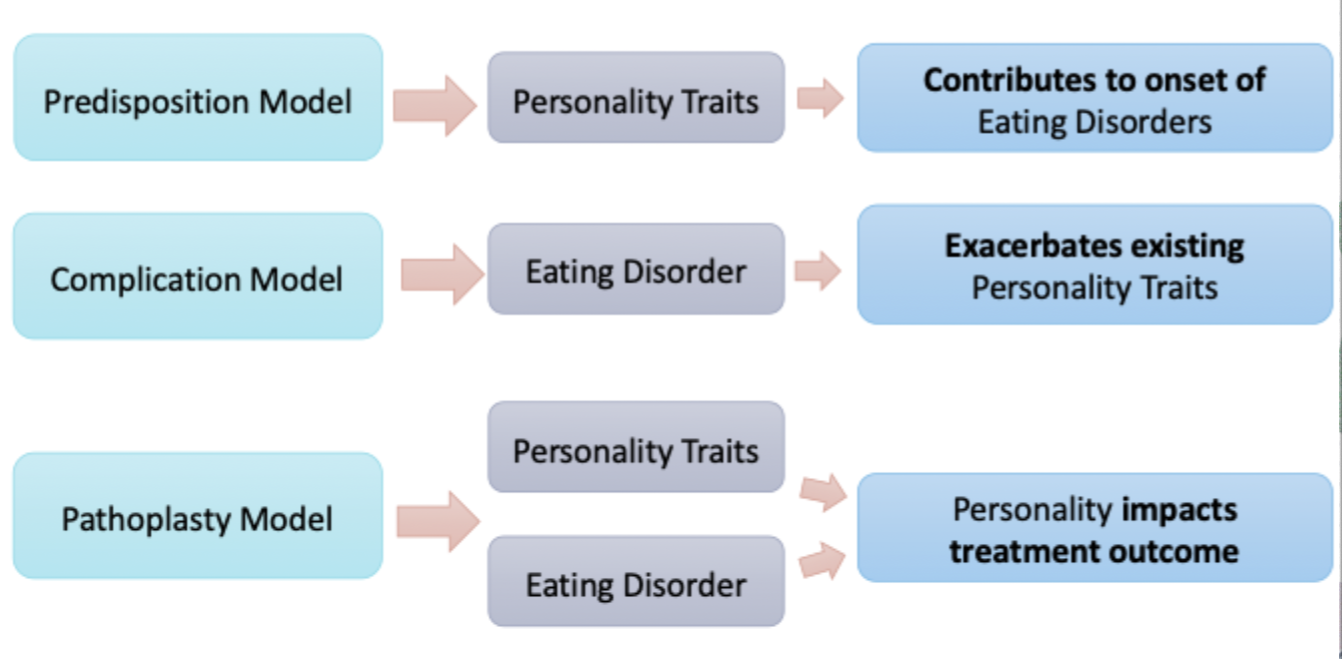
what is the predisposition model?
personality traits should predict future ED & trait levels should be higher among those with an ED (even after treatment) vs. those with no ED
longitudinal data → high levels of neuroticism → predicts ED over 1.5-2 yrs
pre-post treatment → negative affectivity, drive for thinness, perfectionism, & obsessiveness → reduced but still higher among people with an ED, both pre & post-treatment vs. people with no ED history
empirical support for → perfectionism + obsessiveness → anorexia nervosa
what is the complication model?
personality traits should be higher among those currently diagnosed vs. recovered
anorexia
obsessiveness: currently ill » recover » no diagnosis
over treatment neuroticism decreases, extraversion increases
bulimia
impulsivity decreases post-treatment
emotional instability decreases post-treatment
what is the pathoplasty model?
personality impacts the course effectiveness of ED treatment
anorexia
higher levels of obsessive-compulsiveness & perfectionism may be more difficult to treat
bulimia
comorbid traits related to borderline personality disorder more difficult to treat
what are major features of BPD?
unstable self-image
unstable affect
unstable relationships
marked impulsivity