Burns, Hypothermia, and Hyperthermia
1/87
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
88 Terms
What are the 3 main layers of the skin?
- epidermis
- dermis
- subcutaneous
What are the functions of the skin?
- SHAPES
- sensation
- heat regulation
- absorption
- protection
- excretion
- secretion
- vitamin D production
What temperature does cell damage occur at?
>45°C (113°F)
What are the 3 zones of damage in a thermal burn?
- zone of coagulation: irreversible damage by thrombosis of blood vessels
- zone of stasis: stagnation of microcirculation
- zone of hyperemia: increase in circulation
What can injury to the skin result in?
- Disruption of Na+ pump
- Depression of myocardial contractility
- Increased systemic vascular resistance
- Metabolic acidosis
- Increased hematocrit, and blood viscosity
- Secondary anemia
- Tissue injury
What are 1st-degree burns?
- epidermis only
- tissue is red, painful, tender, "sunburn" appearance
- no blisters
- heals 7-14 days without scarring
What are superficial partial thickness 2nd-degree burns?
- into but not through dermis
- blisters, exposed dermis is red/moist
- very painful
- 14-21 days to heal with minimal scarring
What are deep partial thickness 2nd-degree burns?
- into but not through dermis
- possible blisters, but no blanching
- exposed dermis is dry, leathery, waxy, white
- pain with pressure
- heals in 3-8 weeks with scarring
- surgical debridement and skin grafting are needed
What is a 3rd degree burn?
- full-thickness
- damage to dermis and epidermis and adnexal structures
- waxy white to charred black
- painless
- surgical repair/skin grafting
What is a 4th degree burn?
- injury to SubQ fat, fascia, muscle, and bone
- charred & hard to the touch
- grafting required if the patient survives
- amputation & reconstruction needed
What needs to be done to calculate fluid replacement with a thermal burn?
Determine Total Body Surface Area (TBSA)
Describe the palmar rule?
- patient's palm is 1% of body surface area
- good for smaller burns
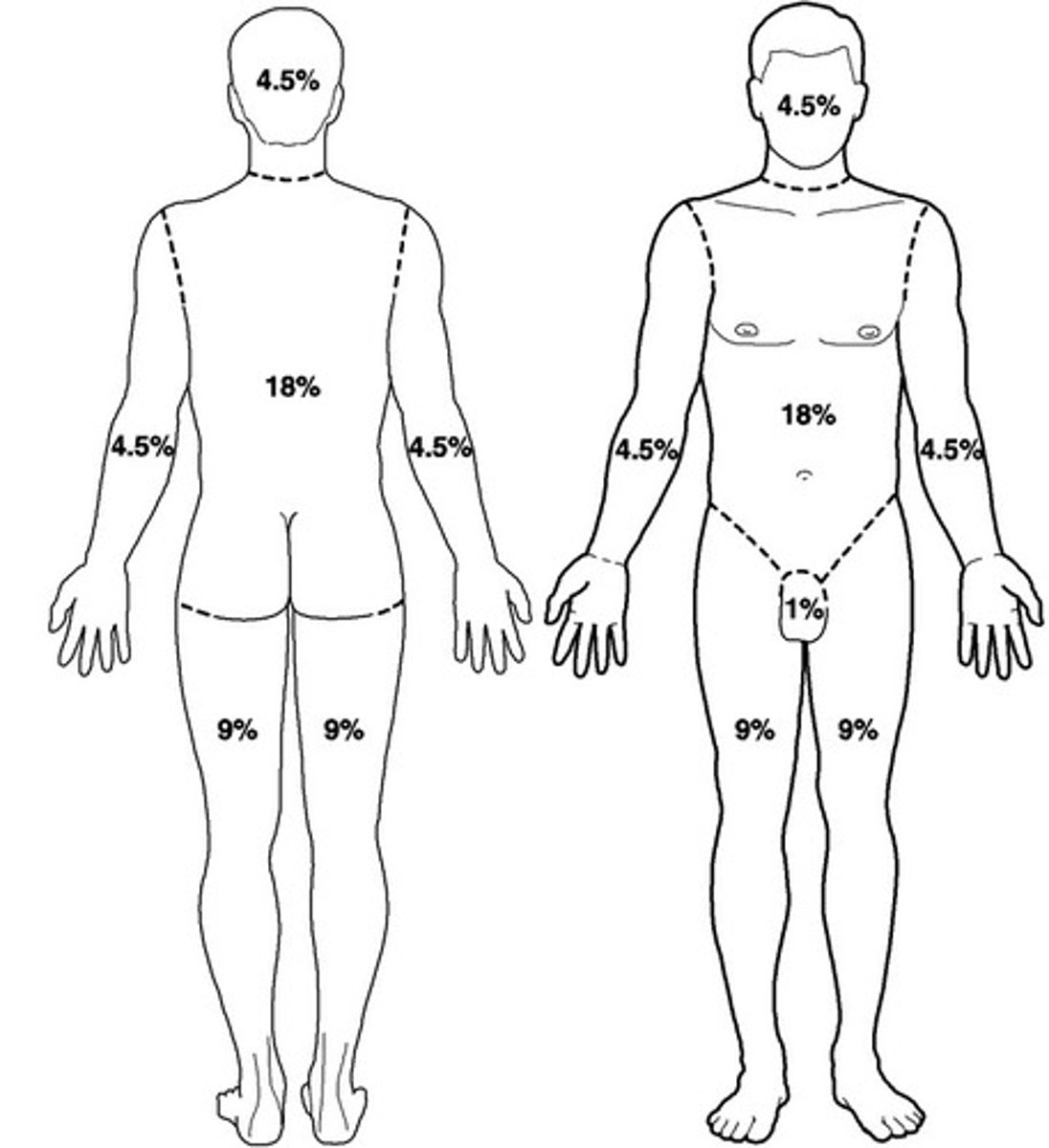
What is the rule of nines?
- division of body surface area in multiples of 9
- good for larger burns
What is the Lund and Browder chart?
gold standard age based assessment
How is the rule of nines calculated?
- for children over the age of one year, for each year above one, add 0.5% to each leg and subtract 1% for the head
- this formula should be used until the adult rule of nines values are reached
What is the initial management of thermal burns?
- Stop the burning process
- ABCs
- History (mechanism of injury, allergies, Td status)
- PE (extent/depth of the injury, calculations)
What is inpatient management of thermal burns?
establish IV access using body surface area, watch urinary output, NG tube (burns >25% TBSA), saline dressing, IV narcotics, labs
What is outpatient management of thermal burns?
- analgesics
- cleanse burn with mild soap and water
- topical antimicrobial: 1% silver sulfadiazine cream, Bacitracin, or triple antibiotic ointment
- sterile daily dressing changes
what is the secondary management of thermal burns if standard treatment fails?
escharotomy
What is an escharotomy?
- limb saving, purposeful cuts
- relieves compromise to distal circulation or mechanical restriction
What are the minor criteria for burns treated outpatient according to the American Burn Association?
- <10% TBSA in adult
- <5% in young/old
- <2% full thickness
What are the moderate criteria for burns treated in a hospital according to the American Burn Association?
- 10-20% TBSA in adult
- 5-10% in young/old
- 2-5% full thickness
- high-voltage injury
- suspected inhalation
- circumferential burn
- concomitant medical problem
What are the major criteria for burns treated in a burn center according to the American Burn Association?
- >20% TBSA in adult
- >10% in young/old
- >5% full thickness
- high-voltage burn
- known inhalation
- burn to face, eyes, ears, genitalia, or joint
- significant other injury
What are RF of inhalation burns?
- Enclosed smoke exposure
- Facial burns
- Increased size of burn area
- Old age
- Oropharyngeal inflammation
- Decreased mentation (overdose/substance abuse, head injury, loss of consciousness)
- Exposure to steam, particulate matter, or toxic gases
How does an inhalation burn occur (three diff ways)?
- particulate matter results from incomplete combustion of materials
- steam can burn deeper tissues below glottis
- toxic inhalants (CO, hydrogen cyanide, acrolein)
What is the most common toxic inhalant?
carbon monoxide
What are two other possible inhalants?
- hydrogen cyanide
- acrolein
What is the clinical presentation of an inhalation burn?
- facial burns
- singed nasal hair
- soot in mouth/nose
- carbonaceous sputum
- hoarseness
- dyspnea
- expiratory wheezing
- stridor
What is the management for inhalation burns?
- prophylactic antibiotics
- bronchodilators
- intubate early
- 100% O2
- Hyperbaric oxygen
What parts of the body are most affected by chemical burns?
- face
- eyes
- extremities
What are the different classifications of chemical burns?
- chemical activity
- acid
- base
- strength of agent
- duration on body
- quantity
What happens to the skin in an acid burn?
- pH <2.0
- coagulation necrosis
- superficial deep tissue burns
What happens to the skin in a basic burn?
- pH >12.0
- liquefaction necrosis
- deeper tissue damage
What is the management of chemical burns?
- flush
- cardiac monitor
- BMP
- Tetanus
- fluids/analgesics
What are the exceptions to not flush a chemical burn?
- powders: brush off prior to irrigation
- hydrofluoric acid: tx with calcium gluconate to bind the fluoride iron
- sodium metal burns: may ignite spontaneously --> use sand/class D fire extinguisher
How do you treat ocular injuries related to chemical burns?
- irrigate: minimum of 1L NS for a minimum of 20-30 minutes
- check acuity
- check pH via sclera
What are the 2 etiologies of electrical burns?
- AC (alternating current)
- DC (direct current)
Where is AC found normally, and what do the entrance and exit wounds look like?
- household electricity
- entrance and exit wounds are same size
Where is DC found normally, and what do the entrance and exit wounds look like?
- industrial injuries, batteries, and lightning
- small entrance wound, large exit wound
- resistance varies based on tissue type
What are S/S of electrical burns?
- loss of consciousness
- confusion to coma
- Seizures
- Headache
- Tinnitus
- Stroke
- Spinal cord-like injury
- Vascular problems
- trauma
What is the management of electrical burns?
- ABCs (assume spinal injury)
- IV Fluids (vigorous lactated ringers)
-ECG/cardiac monitors
- thorough examination of all major organs and for any sign of vessel thrombosis
What is a flashover?
a high voltage electric short circuit made through the air between exposed conductors
What are the 4 types of lightning exposures and which is the most common?
- direct strike
- side flash
- contact strike
- ground strike (MC)
What is the presentation of lightning injuries?
- Lichtenberg figures
- star cataracts
- tympanic membrane rupture
- cardiac damage
- internal organ contusion
- visual problems
What is the management of lightning injuries?
- O2
- tetanus status
- cardiac monitoring
- seizure prevention
- assess for additional injury/internal injury
What are 4 ways heat is lost?
- conduction
- convection
- radiation
- evaporation
What are 5 ways heat is gained/conserved?
- controlled by hypothalamus
- shivering
- thyroid-mediated increase in metabolic rate
- peripheral vasoconstriction
- behavioral response
What temperature does hypothermia occur at?
less than 35 degrees C (95°F)
How is core body temp measured?
- rectal
- tympanic
- esophageal
- intravascular
- bladder
What are some causes of hypothermia?
- Accidental environmental exposure
- Metabolic disorders
- Hypothalamic/CNS dysfunction (head trauma, tumors, stroke)
- Drugs
- Sepsis
- Dermal Disease
- Acute incapacitating illness
- Massive fluid/blood resuscitation
What are the predisposing factors to decreased heat production?
1. hypoglycemia
2. malnutrition
3. hypopituitarism
4. extreme age
What are the predisposing factors of increased heat loss?
1. alcohol abuse
2. DM
3. Drug OD
4. burns
What is the presentation of someone who has mild hypothermia (CBT 32°C - 35°C)?
- Tachycardia
- Tachypnea
- Hypertension
- Shivering
- Impaired coordination
- Poor judgment
- Apathy
- Pale, cold, numb skin
- Dysarthria
things are FAST
What is the presentation of someone who has moderate-severe hypothermia (28°C - 32°C)?
- Shivering stops
- Bradycardia
- Dilated pupils
- Slowed/absent DTR
- Cold diuresis
- Loss of voluntary muscle control
- Confusion
- Lethargy
- Loss of consciousness
everything is SLOOOOOW
What kinds of cardiac dysfunction occur in hypothermia?
- sinus bradycardia to }slow atrial fibrillation to ventricular fibrillation to asystole
- Increased cardiac muscle irritability
What ECG changes are present in hypothermia?
- prolonged p wave & QRS duration
- T wave inversion
- Muscle tremor artifact
- Osborne (J wave): delayed ventricular depolarization and early repolarization
What are methods of passive rewarming for mild hypothermia?
- Transport from cold
- Adequate shelter/heat
- Remove wet garments
- Layer clothes/blankets
- Warm, sweet beverage
What are methods of active external rewarming for mild hypothermia?
- Heated blankets
- Warm bedding/blankets
- Warm packs to trunk
- Immersion into a 40°C bath
What are methods of active internal rewarming for moderate and severe hypothermia?
- Heated humidified O2
- Heated IV fluids (43°C)
- Warm lavage to bladder or stomach
- Peritoneal dialysis or hemodialysis
- Open cardiac massage
- Esophageal or endovascular rewarming
If CBT < 30C, what is done immediately?
- active rewarming + CPR
- one defibrillation attempt
- once CBT reaches 30oC cardiac medication can be given
- continue active rewarming to 32oC
What is the temperature frostbite occurs at?
-20°C (-4°F)
What groups of people are at increased risk for frostbite?
- Military
- Outdoor workers
- Elderly
- Homeless
- Drug/ETOH
- Psych
Describe 1st-degree frostbite and its prognosis?
- numbness, erythema, swelling, dysesthesia, white plaques, no loss of tissue
- excellent prognosis
Describe 2nd-degree frostbite and its prognosis?
- edema, erythema, blister formation in 6-12 hours
- good prognosis
Describe 3rd-degree frostbite and its prognosis?
- tissue loss involving the entire thickness
- hemorrhagic blisters
- Blue-gray discoloration
- "block of wood" then burning, throbbing pain
- poor prognosis
Describe 4th-degree frostbite and its prognosis?
- freezing of tissue, muscle, bone, tendon
- little edema, skin is mottled with non-blanching cyanosis
- deep, dry black mummified eschar
- very poor prognosis
What is the management of frostbite?
- Cover and protect
- Remove wet/constrictive clothing
- Constant warmth without rubbing
- rapid rewarming for full-thickness frostbite
- IV fluids/analgesics
- local wound care
When is surgery done for frostbite?
not until definite tissue necrosis (3-5 weeks after injury)
What is hyperthermia?
elevation of core body temperature above the normal diurnal range of 36 to 37.5ºC due to failure of thermoregulation
What is the main etiology of hyperthermia?
Imbalance between metabolic heat production/environmental heat load and normal heat capacity/loss heating
What are 3 other etiologies of hyperthermia?
- Serotonin Syndrome
- Malignant Neuroleptic syndrome
- Malignant hyperthermia of anesthesia
What is M&M related for hyperthermia?
duration of core temperature elevation
What are the 4 predisposing factors for hyperthermia?
1. age (young or old)
2. drugs (anticholinergics, tricyclic antidepressants, diuretics, cocaine)
3. occupational hazards
4. chronic disease
What does the clinical presentation, pathophys, and treatment look like for heat edema?
- mild severity
- lower extremity edema
- normal temp, BP, CNS
- sweating present
- cutaneous vasodilation and pooling of interstitial fluid in dependent areas
- treatment is symptomatic
What does the clinical presentation, pathophys, and treatment look like for heat cramps?
- mild severity
- painful muscle contractions
- normal temp, BP, CNS
- profuse sweating
- dilution hyponatremia
- treatment is symptomatic
What does the clinical presentation, pathophys, and treatment look like for heat exhaustion?
- moderate severity
- syncope, N/V, HA
- temp nL-104oF
- orthostatic BP
- profuse sweating
- decrease PVR, decreased volume, respiratory alkalosis/hyperventilation
- IV saline, evaporative cooling, electrolyte replacement
What does the clinical presentation, pathophys, and treatment look like for heat stroke?
- severe
- HA/MS changes
- temp >105 F
- abnormal CNS
- failure of thermoregulation
- rapid cooling, fluid and electrolyte management
What is the other management of heat exhaustion?
- move to shaded area
- lay supine
- feet above head
- fluids
- avoid sudden or prolonged standing until fully recovered
What are 2 types of heat stroke?
1. Classic/nonexertional
2. Exertional
What is the presentation of classic/non-exertional heat stroke?
- elderly
- no exercise
- sweating absent
- volume contracted: mild/moderate
- respiratory alkalosis
- underlying illness
What is the presentation of exertional heat stroke?
- young
- exercising
- sweating present
- volume contracted: severe
- metabolic acidosis
- no underlying illness
What is the evaluation and management of classic heat stroke?
- ABCs
- manage airway, ventilation, and circulation
- Rapid cooling until goal rectal temp of 38 to 39ºC (100.4 to 102.2ºF)
- assess volume status & give fluids
- CHECK EVERY LAB LIKE FR
What are prehospital treatments for exertional heat stroke?
- ABCs
- remove equipment and excess clothing
- rapid cooling
- stop cooling when rectal temp is 102.2
What are hospital treatments for exertional heat stroke?
- protect airway and maintain adequate oxygenation, ventilation, and circulation
- monitor vitals
- fluid resuscitation
- correct electrolyte issues
What is the pathophysiology of malignant hyperthermia?
- some patients have genetic skeletal mm receptor anomalies which allow for excess Ca2+ accumulation in the presence of certain agents
- this leads to sustained mm contraction, breakdown, metabolism, and acidosis causing more heat generation than the body can get rid of
- presents as marked hyperthermia minutes to hours past initial onset of sx
What are early signs of malignant hyperthermia?
- Hypercarbia
- Sinus tachycardia
- Masseter muscle rigidity
- Generalized muscle rigidity
What are late signs of malignant hyperthermia?
- Hyperthermia
- ECG changes w/ hyperkalemia
- Ventricular ectopy/ bigeminy/ tach/ fib
- Myoglobinuria
- Excessive bleeding
What is the treatment of malignant hyperthermia?
- Dantrolene
- supportive measures & remove causative agent