CM II Week 8 (Orthopedic/MSK Disorders)
1/167
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
168 Terms
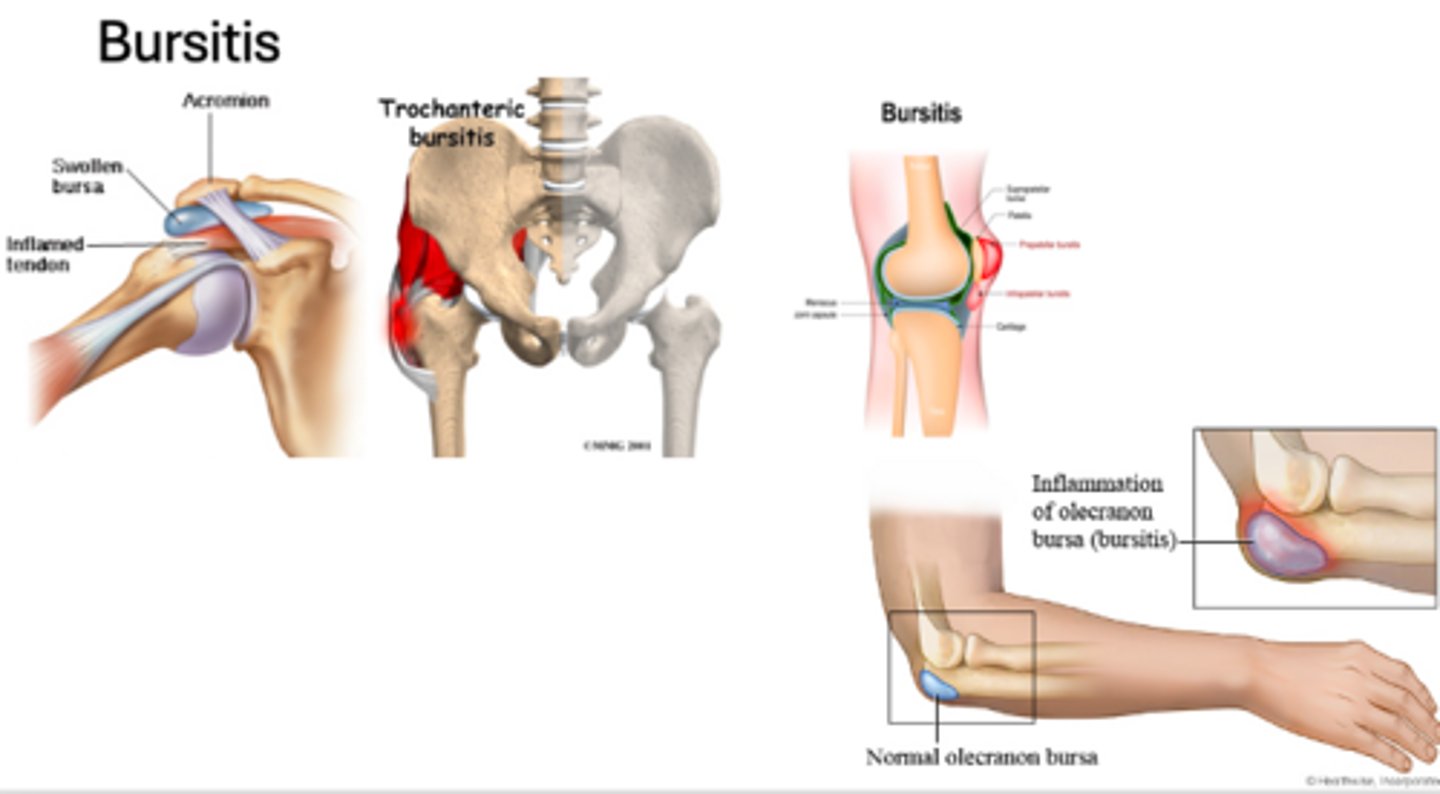
bursitis definition
Painful or painless swelling of the bursa, that function as cushions at major joints
most common locations of bursitis
- Subacromial bursitis (shoulder)
- Olecranon bursitis (elbow)
- Trochanteric Bursitis (hip)
- Prepatellar Bursitis (knee)
history consistent with bursitis
- Overuse, repetitive activity, trauma
- Pain with ROM
- Stiffness, achy, painful, swelling not cosmetically appealing
PE for bursitis
Edema at bursa site, mild tenderness
Rule out infection!! bursa can become infected
Warm to touch, pain with palpation, edema with erythema to surrounding tissues, and pain with ROM
treatment for bursitis
- NSAIDs, stretching, PT, corticosteroid injections
- Bursa aspiration and Ace wrap
- Aspiration, gram stain, culture, and antibiotics if infection is suspected
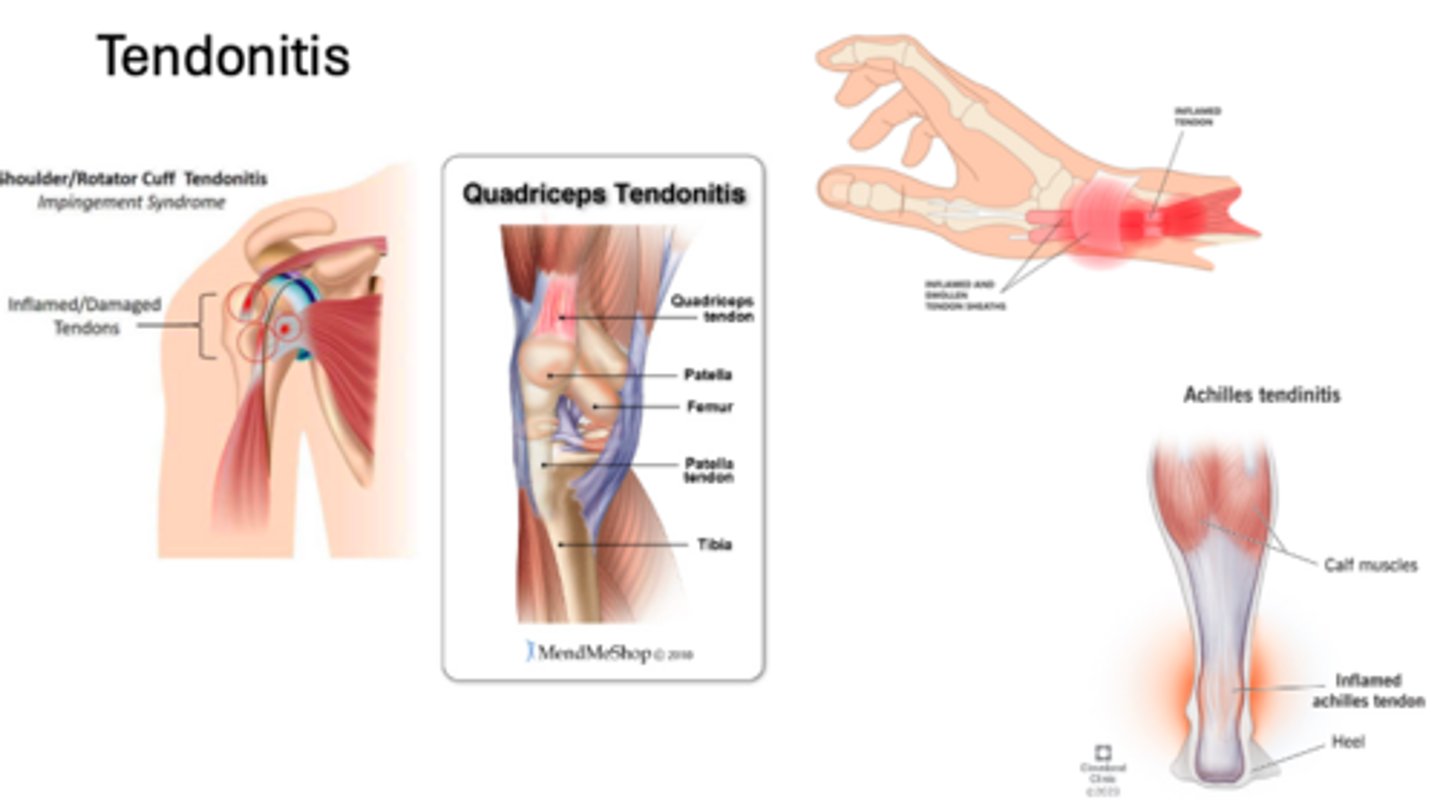
tendonitis
condition where a tendon (tissue that connects muscles to bone) becomes inflamed and causes pain
most common locations for tendonitis
- Shoulder tendonitis
- Tennis/Golfers elbow
- Achilles tendonitis
- Patella/Quad tendonitis
- Wrist tendonitis
- De Quervain's tenosynovitis
history consistent with tendonitis
- Overuse, repetitive activity, trauma
- Pain, worse with ROM and activity
PE of tendonitis
Pain to palpation localized at tendon site. May have associated swelling.
treatment for tendonitis
- Rest
- NSAIDS
- stretching
- PT
- corticosteroid injections (be careful of tendon rupture)
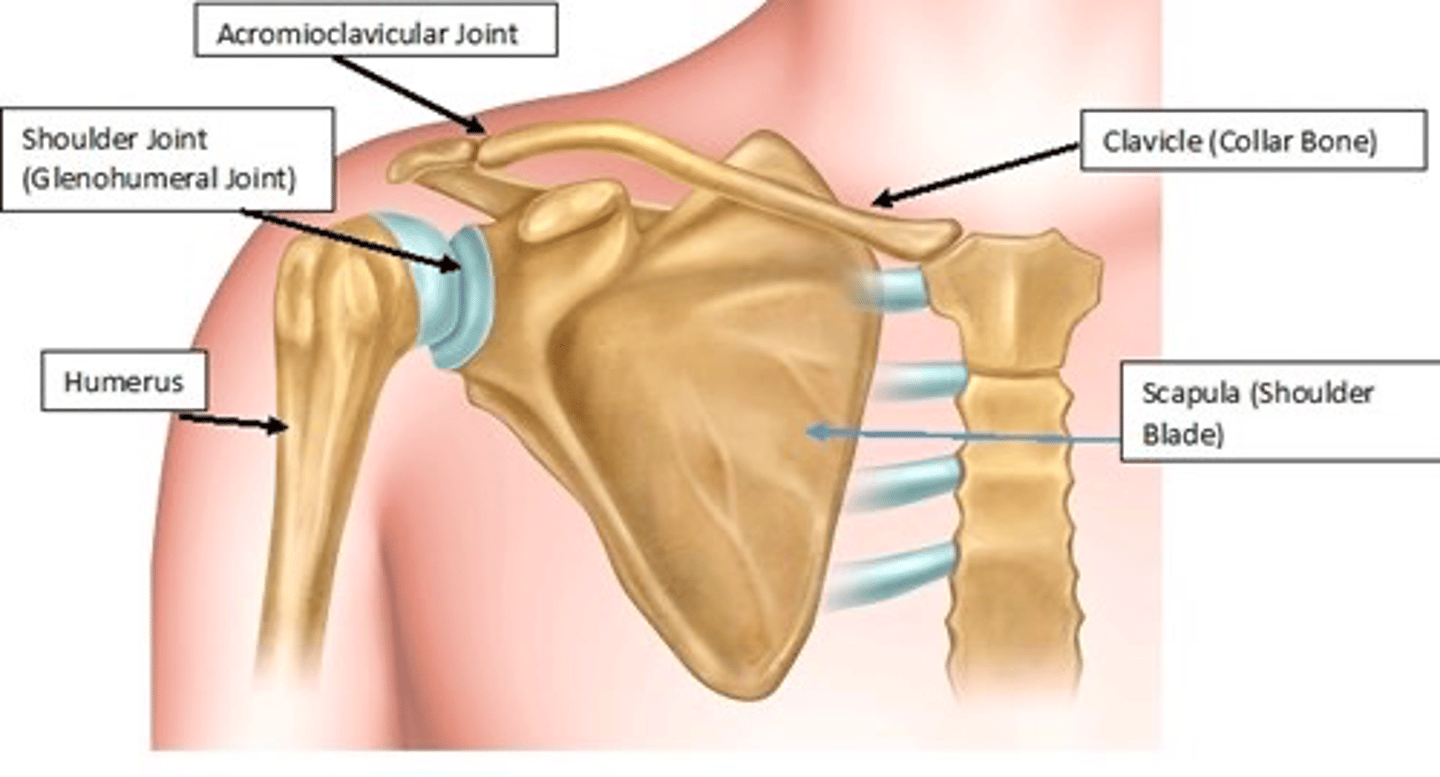
what are the three bones of the shoulder?
- Scapula
- Humerus
- Clavicle
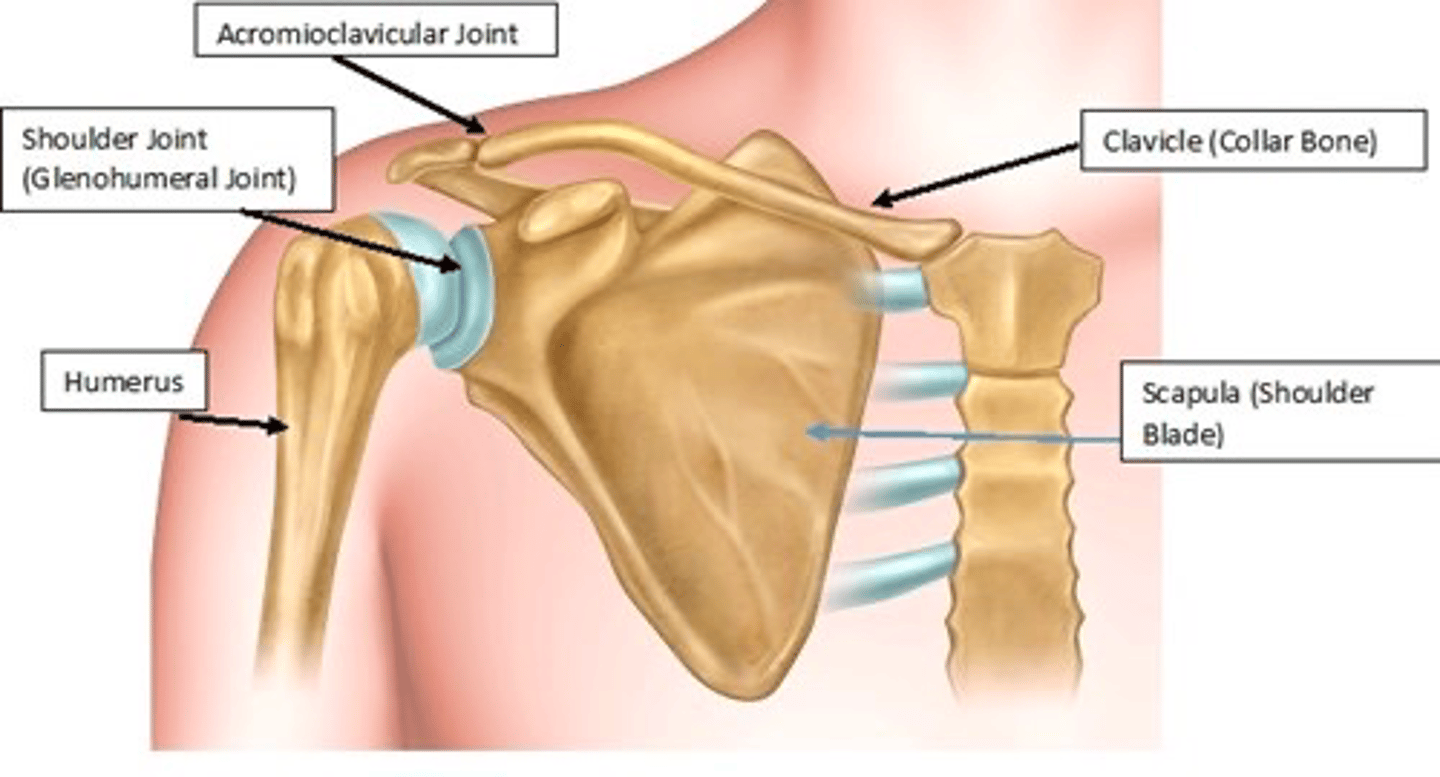
joints of the shoulder
- Glenohumeral
- Acromioclavicular
- Sternoclavicular
- Scapulothoracic
epidemiology of subacromial impingement syndrome
- Most common cause of shoulder pain
- Accounts for 44-65% of shoulder disorders
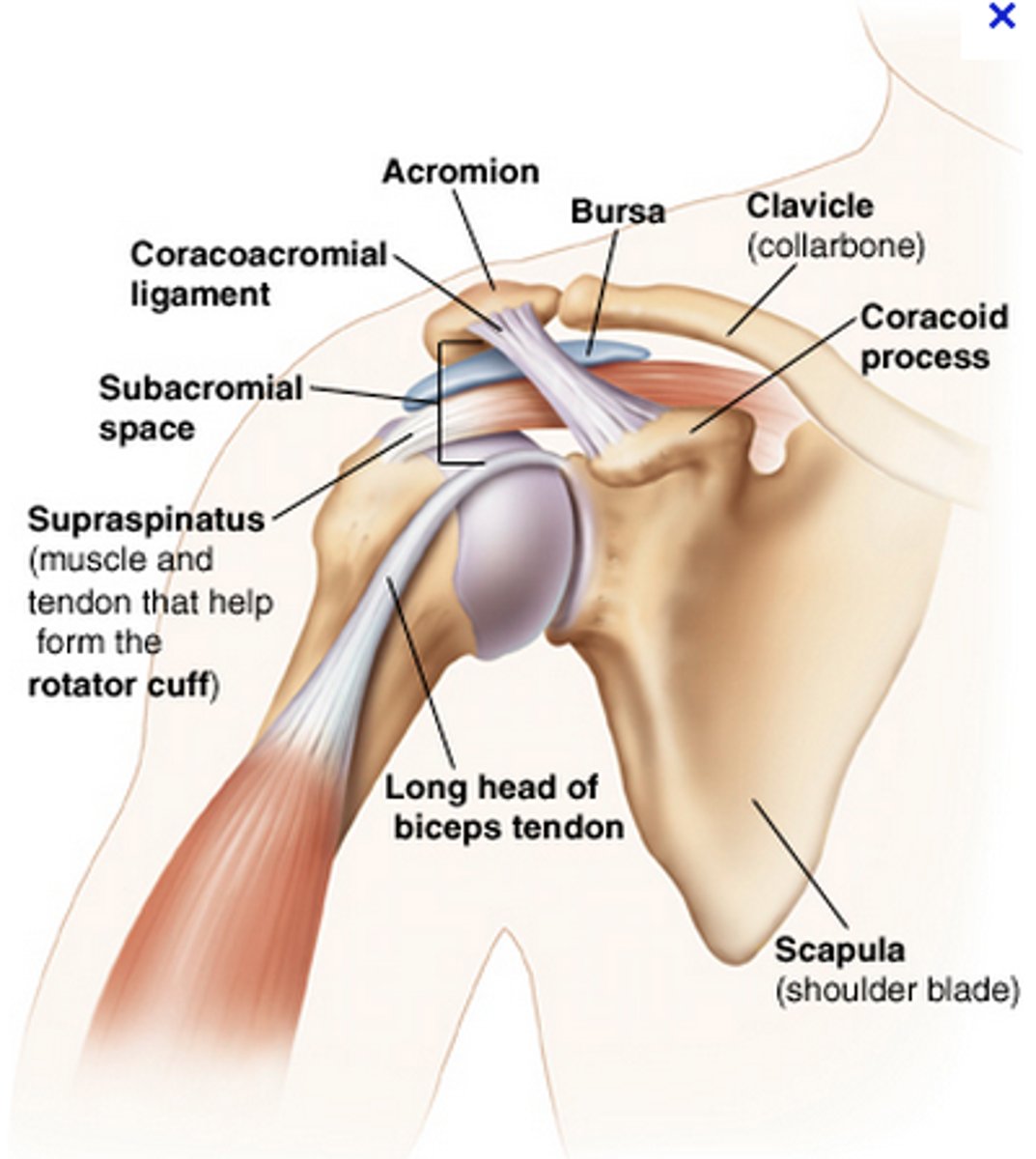
what is the pathophysiology of subacromial impingement syndrome?
Combination of....
Extrinsic compression: Rotator cuff is between humeral head, anterior acromion, coracoacromial ligaments, and acromioclavicular joint
Intrinsic degeneration: Supraspinatus- constant microtrauma of the supraspinatus leads to degeneration and imbalance of the glenohumeral joint causing superior migration of the humeral head and narrowing of the subacromial space
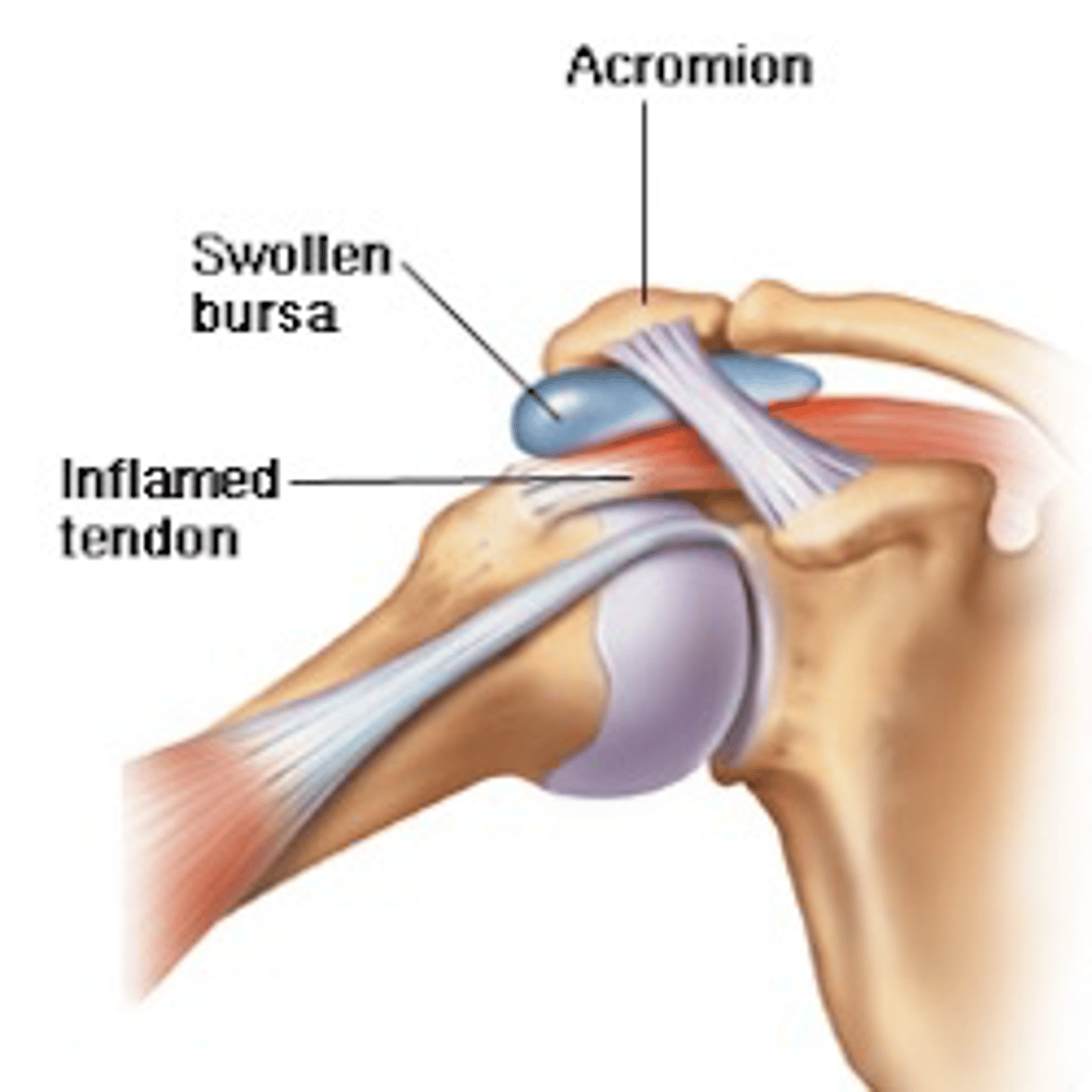
Inflammatory process: Inflammation of subacromial bursa causing impingement surrounding structures (humerus, rotator cuff, and acromion)
subacromial impingement is the first stage of
rotator cuff disease which is a continuum of disease:
- Impingement, bursitis, tendonitis
- Partial to full-thickness tear
- Massive rotator cuff tears
- Rotator cuff arthropathy
hx consistent with subacromial impingement syndrome
- Overuse, repetitive activity
- Shoulder pain, worse with overhead lifting or reaching, can radiate to lateral upper arm (deltoid area)
PE findings of subacromial impingement syndrome
May have pain to palpation along subacromial joint space
Range of motion (ROM) typically normal (if not think adhesive capsulitis)
+/- weakness secondary to pain with abduction or supraspinatus strength testing
PE findings of subacromial impingement syndrome - special tests
- Hawkins test - positive if internal rotation and passive forward flexion to 90° causes pain
- Neer impingement test - positive if passive forward flexion >90° causes pain
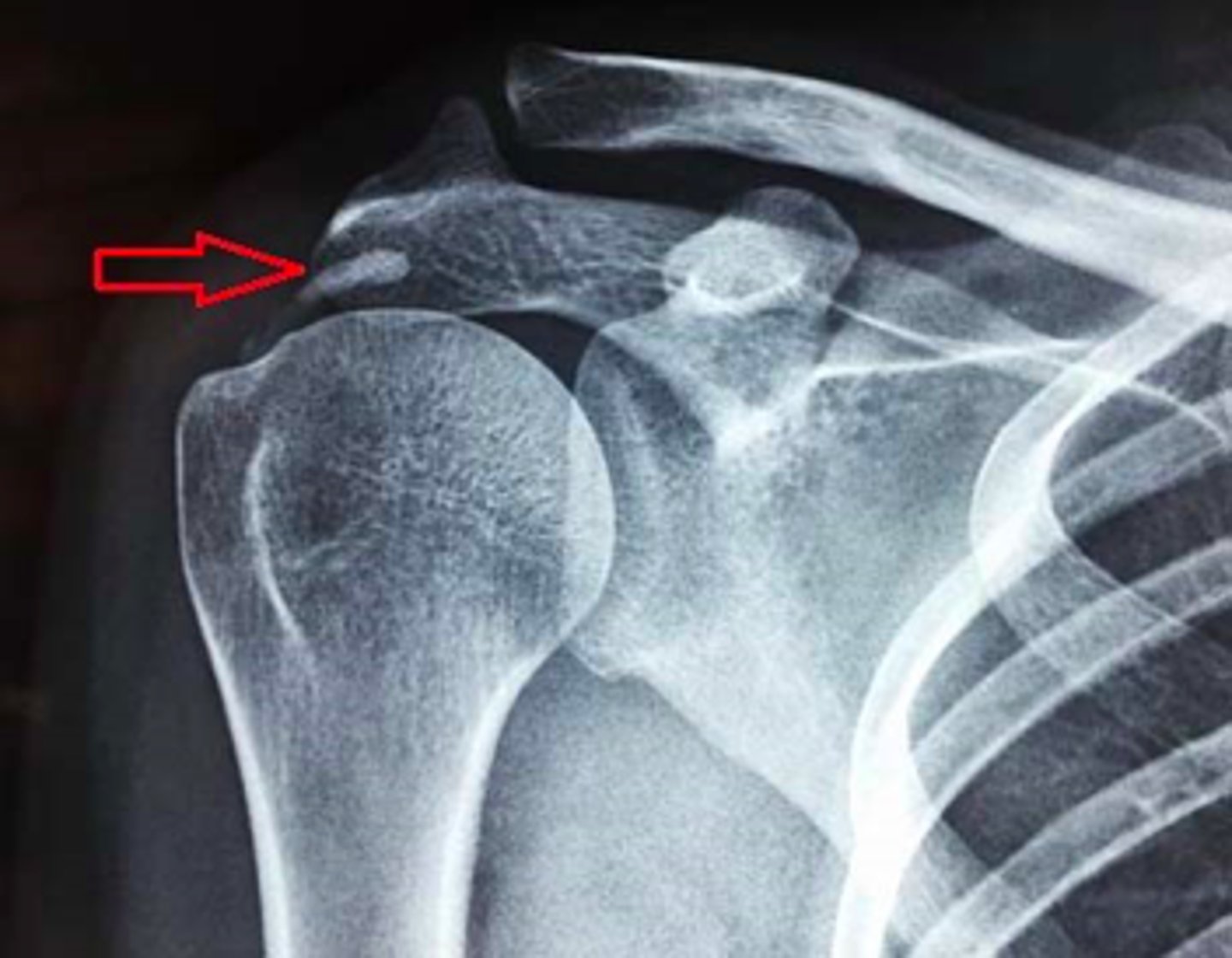
imaging for subacromial impingement syndrome
XR: AP and lateral (Y-view)
- +/- Proximal migration of the humerus
- Traction osteophytes
- Calcification of the coracoacromial ligament
- Cystic changes within the greater tuberosity
treatment for subacromial impingement syndrome
- Anti-inflammatory (NSAIDs), Ice, activity modifications
- Physical therapy (rotator cuff strengthening)
- Subacromial steroid injection
- DO NOT put patients in a sling for impingement syndrome!!! to avoid stiffness and adhesive capsulitis
If patients fail conservative management, order an MRI of the shoulder to evaluate for underlining rotator cuff injury
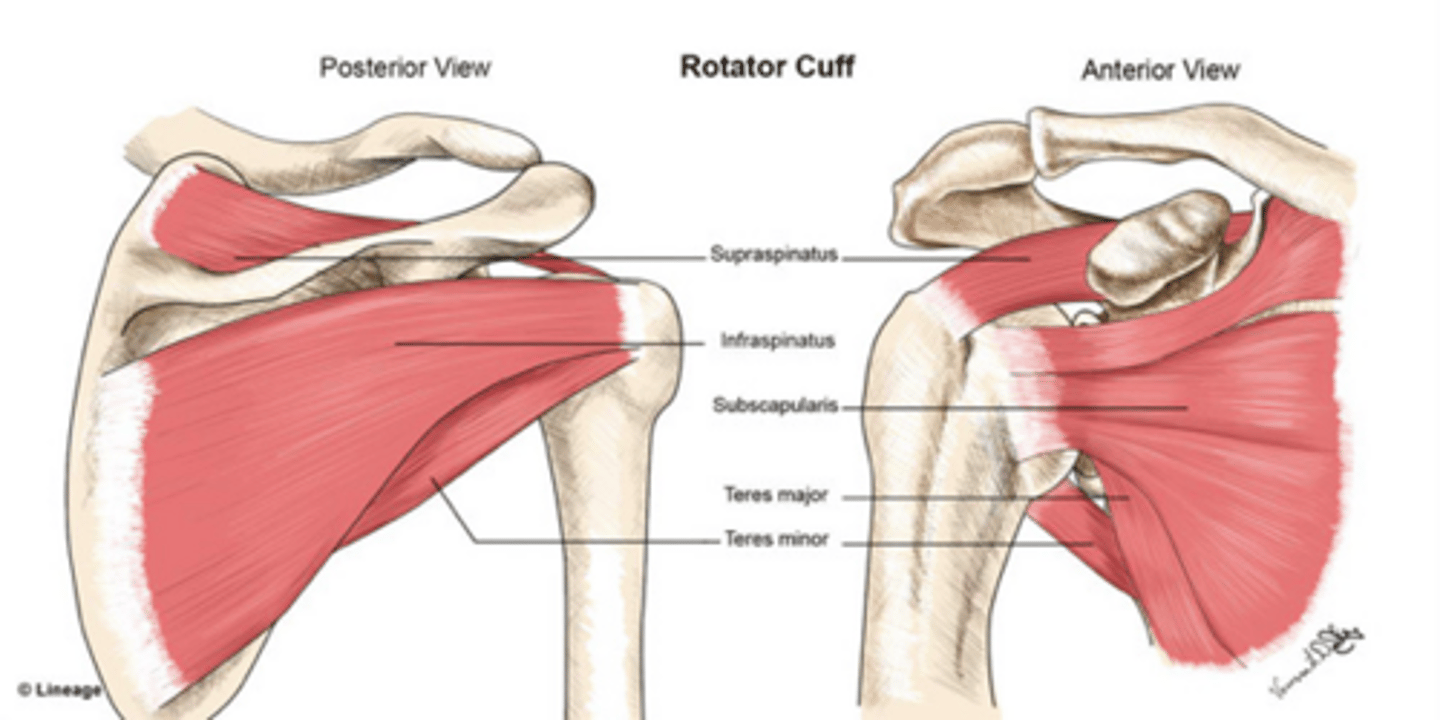
what are the four muscles that cover the scapula?
SITS!
- Supraspinatus
- Infraspinatus
- Teres minor
- Subscapularis
epidemiology of rotator cuff tears
- Age > 60: 28% have full-thickness tear
- Age > 70: 65% have full-thickness tear
risk factors of rotator cuff tears
- age
- smoking
- hypercholesterolemia
- family history
pathophysiology of rotator cuff tears
Chronic degenerative tear:
- Older patients: usually involves supraspinatus, infraspinatus, and teres minor (SIT)
Chronic impingement
- Bursal surface or within the tendon
Acute avulsion injuries:
- Acute subscapularis tears seen in younger patients following a fall
- Acute SIT tears seen in patients > 40 yrs following a shoulder dislocation
hx consistent with rotator cuff tears
- Pain located anterior and lateral shoulder
- Pain radiating to the deltoid and down the arm (pain does not radiate below elbow)
- Tears are mostly atraumatic, with progression of pain and weakness over time
- Acute tears are associated with trauma (sports injures, direct blow to shoulder or fall on outstretched hand)
- Pain at night or inability to sleep
- +/- Arm weakness
PE findings of rotator cuff tears
- +/- Limited active ROM, passive ROM is generally full
- +/- Neer and Hawkins impingement signs
Mainstay of PE -- special tests to evaluate each rotator cuff tendon:
- Drop arm test (inability to hold the arm in an abducted position against gravity) indicates large rotator cuff tear
- Positive Empty can or Jobe test (weakness with resisted abduction) indicates supraspinatus tear
- Weakness with resisted external rotation indicates infraspinatus tear
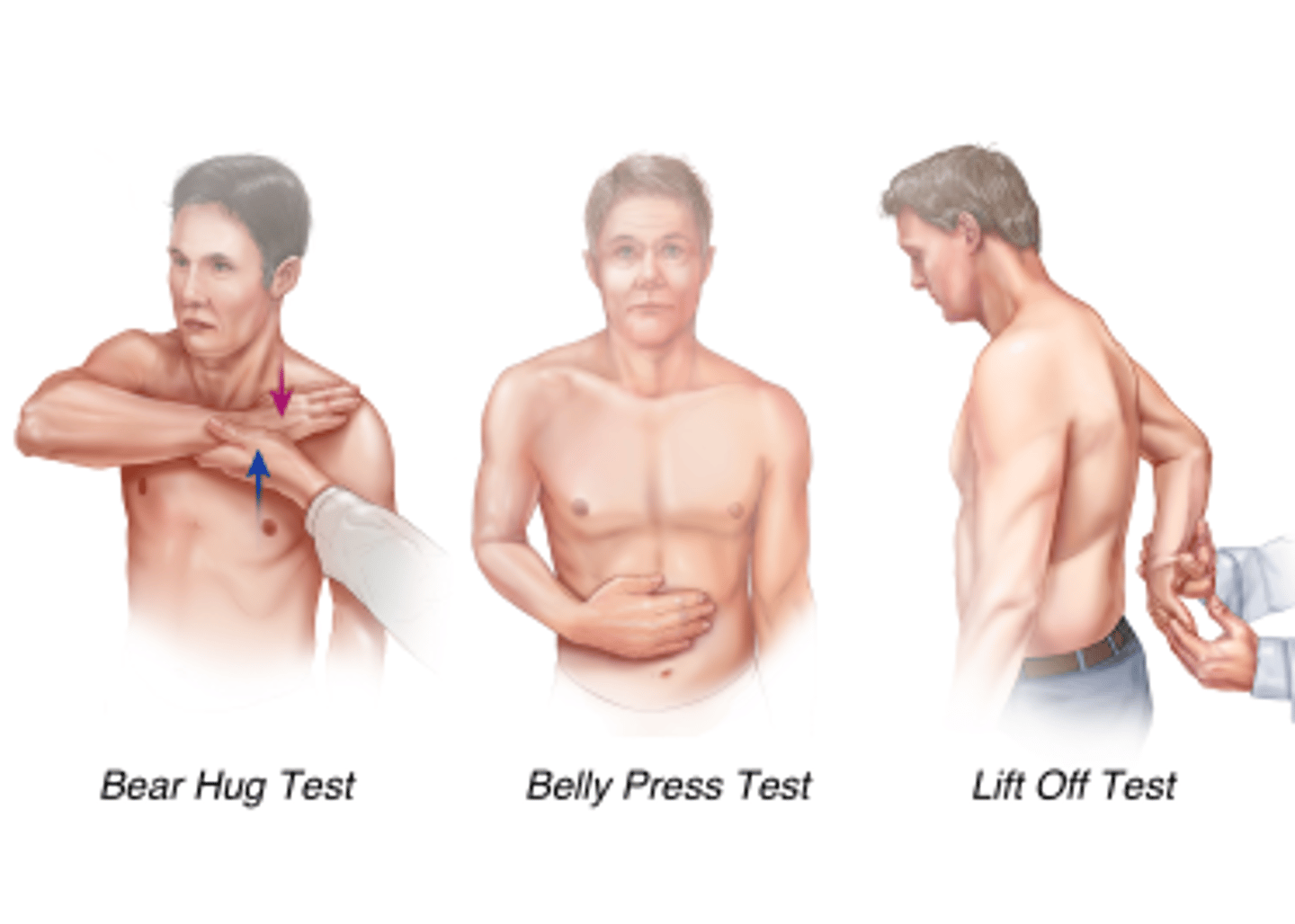
- Positive lift-off or belly press test indicates subscapularis tear

belly press test, bear hug test, lift off test pic
Imaging for rotator cuff tear
XRAY
MRI (gold standard)
Ultrasound

rotator cuff tear XRAY findings
Calcific tendonitis
Cystic changes in greater tuberosity
Proximal migration of humerus head seen with chronic cuff tears
MRI findings in rotator cuff tear
Able to accurately evaluate muscle quality (size, shape, degree of retraction of tear) and atrophy
Ultrasound findings in rotator cuff tear
inexpensive
user dependent
Rotator cuff tear treatment
•Tx determined by size of tear
•Initial tx may be the same as subacromial impingement (partial tears involving less than 60% of tendon)
Arthroscopic or mini-open rotator cuff repair is the treatment of choice for full thickness tears
What can advanced rotator cuff disease lead to
glenohumeral DJD
which leads to rotator cuff arthopathy and advanced shoulder osteoarthritis
how do anterior shoulder dislocation occur
Forceful traumatic injury that occurs when the shoulder is in an abducted and externally rotated position
epi/risk factors of anterior shoulder dislocation
•One of the m/c shoulder injuries
•Anterior dislocation >> posterior dislocation
•80-90% in teenagers
RF:
contact sport
military
collagen disorder (Ehlers-Danlos and marfan)
anterior shoulder dislocation can lead to secondary injuries such as
•Labrum & cartilage Injuries (Bankart)
•Bone defects or fractures (Hill-Sachs)
•Nerve injuries (axillary nerve)
•Rotator cuff tears
Important hx for anterior shoulder dislocation
loss of motion
arm feeling "dead"
history of traumatic event leading to sx
PE for anterior shoulder dislocation
Visible deformaties and LOM
Decreased sensation along deltoid (early finding)
Shoulder dislocation special tests
•Load and Shift test
https://youtu.be/txARar71h5E
•Apprehension sign
https://youtu.be/jZ29dAXKA5M
•Relocation sign
https://youtu.be/YX1uJhjhwWg
•Sulcus sign
https://youtu.be/vV7u2JtdYWI
Anterior shoulder dislocation imaging
XRAY - Gold standard for shoulder dislocations
MRI +/- arthrogram

MRI +/- arthogram
help diagnose shoulder pathology secondary to dislocation (labral, rotator cuff tears)
anterior shoulder dislocation treatment
conservative management
Reduction – May need to do this in the ER for conscious sedation
• Techniques: Kocher, Hippocratic, Stimson's
Short term immobilization less than 1 week
PT
anterior shoulder dislocation treatment
surgery
Arthroscopic/open shoulder surgery
posterior shoulder dislocation occurs when
trauma that occurs when the shoulder is in a flexed, adducted and internally rotated position
Which is more common an anterior or posterior dislocation and why?
Anterior bc there is more muscle and ligaments in the posterior side
epi/risk factors for posterior shoulder dislocation
•Posterior << anterior dislocations (but more commonly missed)
•50% are undiagnosed in ER
•Chronic microtrauma from overuse seen in football Lineman, weightlifters, and overhead athletes
RF:
seizures
electric shock
collagen disorders: Ehler's-Danlos and marphan
Important hx in posterior shoulder dislocstions
•Loss of motion
•History of repetitive pushing with the arm in forward flexed position
•History of traumatic event leading to symptoms
•Vague pain
PE findings with posterior shoulder dislocation
•Visible deformity and loss of motion
•Limited external rotation
•Shoulder locked in internal rotation
Posterior shoulder location special tests
•Jerk test
https://youtu.be/j_qG1MNOws8
•Kim test
https://youtu.be/-knsALCdv_A
•Posterior stress test
https://youtu.be/CHzJk5IeCkk
•Posterior load and shift test
https://youtu.be/txARar71h5E
Posterior shoulder dislocation imaging
XRAY (gold standard)
MRI+/- arthogram
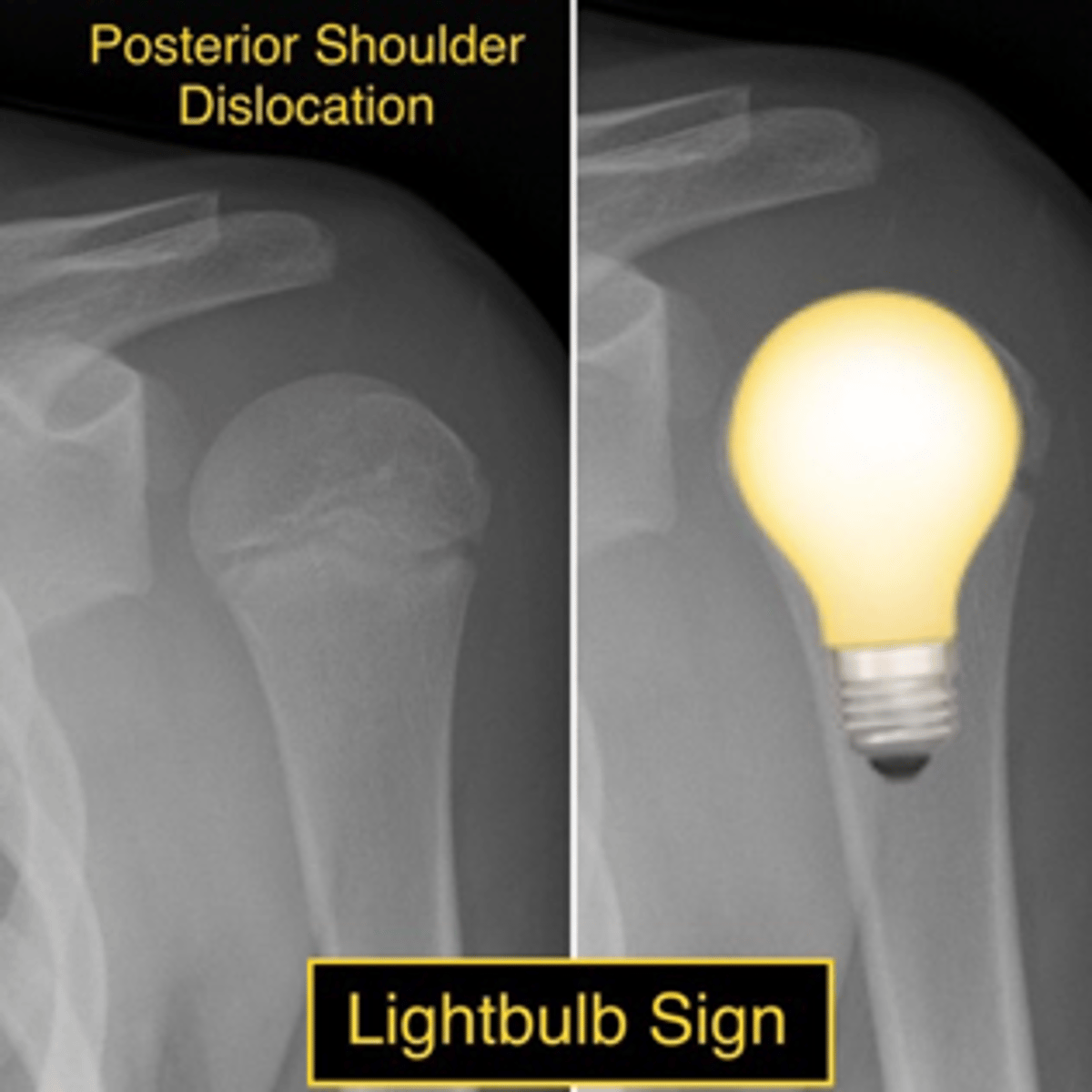
Xray findings in posterior shoulder dislocation
"Light bulb" sign
MRI+/- arthrogram in posterior shoulder dislocation
help diagnose shoulder pathology secondary to dislocation (labral, rotator cuff tears)
Posterior shoulder dislocation tx
Conservative management
•Reduction – May need to do this in the ER for conscious sedation
•Immobilization for 4-6 weeks in external rotation
•PT
Surgery
•Arthroscopic/open shoulder surgery
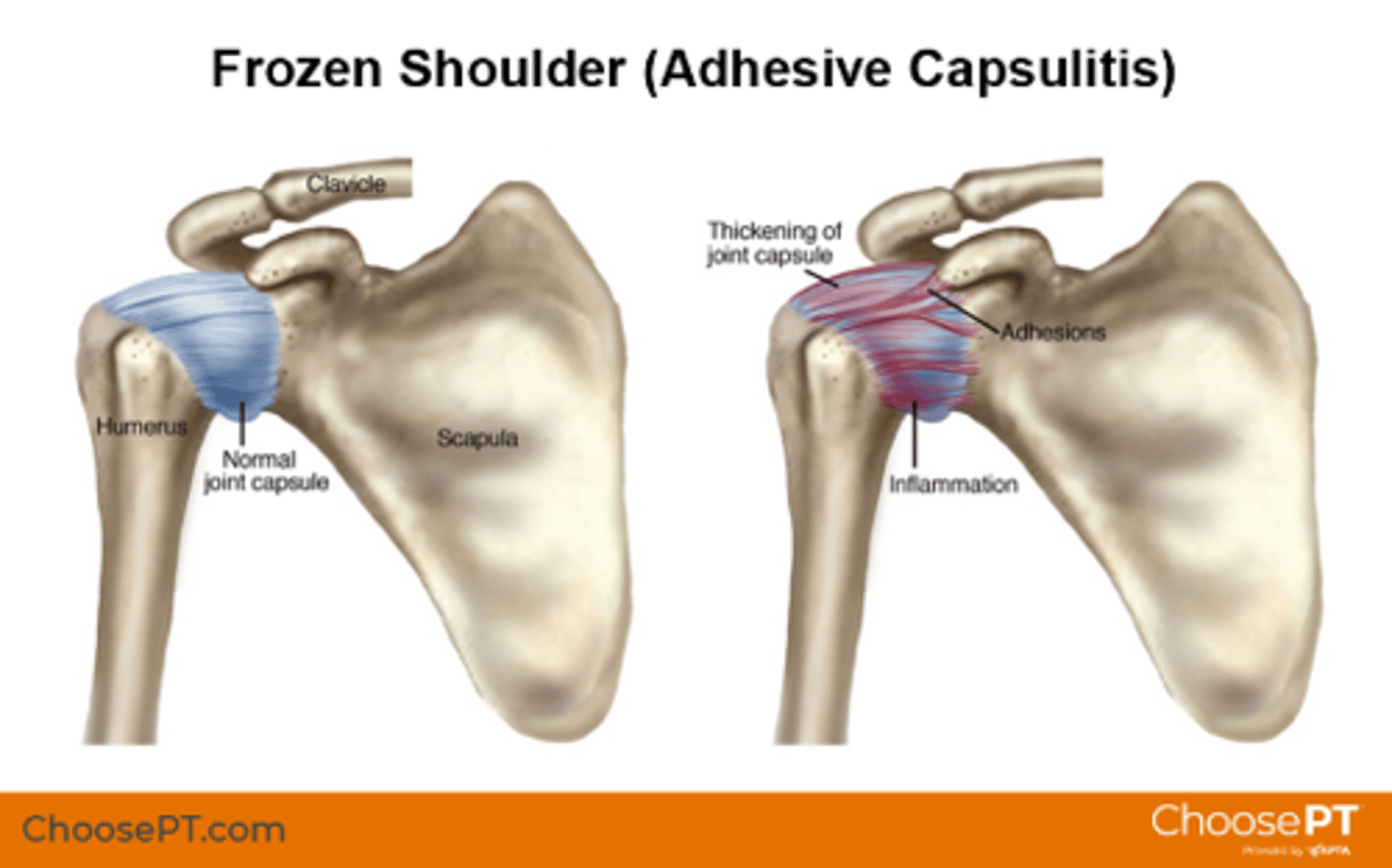
adhesive capsulitis
Inflammatory process causing fibroblastic proliferation of joint capsule leading to thickening, fibrosis, and adherence of the capsule to itself and humerus
Common age/gender for adhesive capsulitis
women ages 40-60
Factors associated w/ adhesive capsulitis
trauma- status post humerus fracture, long periods of immobilization, chest or breast surgery
idiopathic
Risk factors of adhesive capsulitis
•Diabetes #1 Risk factor
•Rheumatoid arthritis
•Thyroid disorders
•Cervical disc disease
PE of adhesive capsulitis
•Restricted passive and active ROM
•Pain intensifies with full ROM during exam
Dx of adhesive capsulitis
•Adhesive capsulitis is a clinical diagnoses
•Use imaging to rule out differential diagnosis
adhesive capsulitis tx
Conservative management
•Self limiting: 1-2 years
•Physical therapy 3-6 months
•NSAIDS vs. Steroids
•Cortisone injection
Operative management
•Manipulation under anesthesia
•Arthroscopic capsular release
lateral epicondylitis (tennis elbow)
overuse injury caused by repetitive overload at the origin of common extensor tendons which causes inflammation and microtears.
lateral epicondylitis (tennis elbow) epidemiology
-more common cause of elbow pain
-50% of tennis players
-Common in laborers who utilize heavy tools
-pt 35-60 years old
-workers who engage in repetitive gripping and lifting (can dx w grip strength + track progession)
Important hx of tennis elbow
-lateral side elbow pain
-hx of repetitive supination and pronation
-worse w lifting and gripping
-decreased grip strength
PE of tennis elbow
• +/- Edema over lateral epicondyle
• Point tenderness to palpation over lateral epicondyle
• Pain with resisted wrist extension with elbow extension
• Decreased grip strength

imaging findings in tennis elbow
X-ray: Most likely normal
MRI... No need for MRI
•MRI changes often present in sx patients
•Increased signal intensity at ECRB tendon may be seen (50% of cases)
imaging not great for tennis elbow
Tennis elbow tx
•80-90% resolve with or without tx w/in a year
•NSAIDS/Activity modifications
•Bracing: Counterforce brace, wrist brace
•PT
•Injection: Corticosteroid, platelet rich plasma (PRP)
Surgery
•Release and debridement of ECRB origin
•Reserved for those with persistent symptoms for over a year
•70% of patients with good to excellent outcomes

Medial epicondylitis (golfer's elbow)
Tendonitis/overuse of the common flexor-pronator tendon origin at the medial epicondyle
Golfer's elbow epidemiology
5-10x less likely than lateral epicondylitis
common in tennis, golfers and throwing athletes
Golfer's elbow important hx
•Medial sided elbow pain
•Possible reported history of injury or repetitive trauma of common flexor tendon
•Repetitive elbow use, repetitive gripping, repetitive valgus stress
•+/- Numbness or tingling in ulnar digits
Medial Epicondylitis (Golfer's Elbow) PE
•+/- Edema over medial epicondyle
•Point tenderness to palpation over medial epicondyle
•Pain with resisted wrist flexion
•Elbow stable to valgus stress to rule out UCL involvement
•Evaluate ulnar nerve to rule out cubital tunnel syndrome (can coexist)
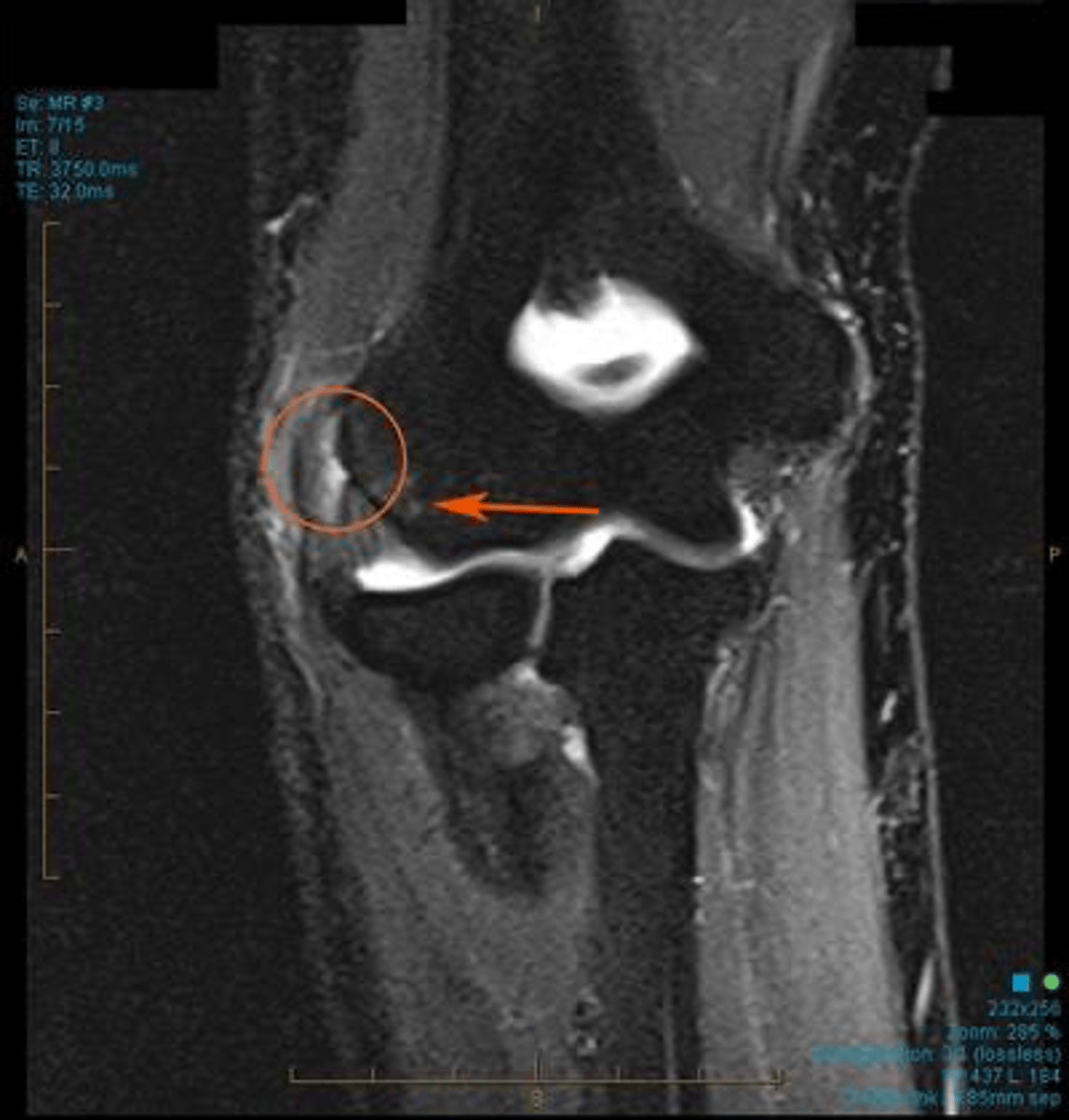
Golfer's elbow imaging findings
xray- normally unremarkable, used to r/o arthritic changes, UCL calcification or avulsion fracture in acute trauma
MRI- usually not needed, order to evaluate/r/o other caused of medial-sided elbow pain
Golfer's elbow tx
•NSAIDS/Activity modifications/ICE
•Bracing: Counterforce brace, wrist brace, elbow splint
•PT
•Injection: Corticosteroid, platelet rich plasma (PRP)
Surgery: Not typically recommended
•Open debridement of pronator teres/flexor carpi radialis, reattachment of flexor-pronator group
•Must rule out UCL pathology, cubital tunnel syndrome
*Must rule out UCL pathology, cubital tunnel syndrome
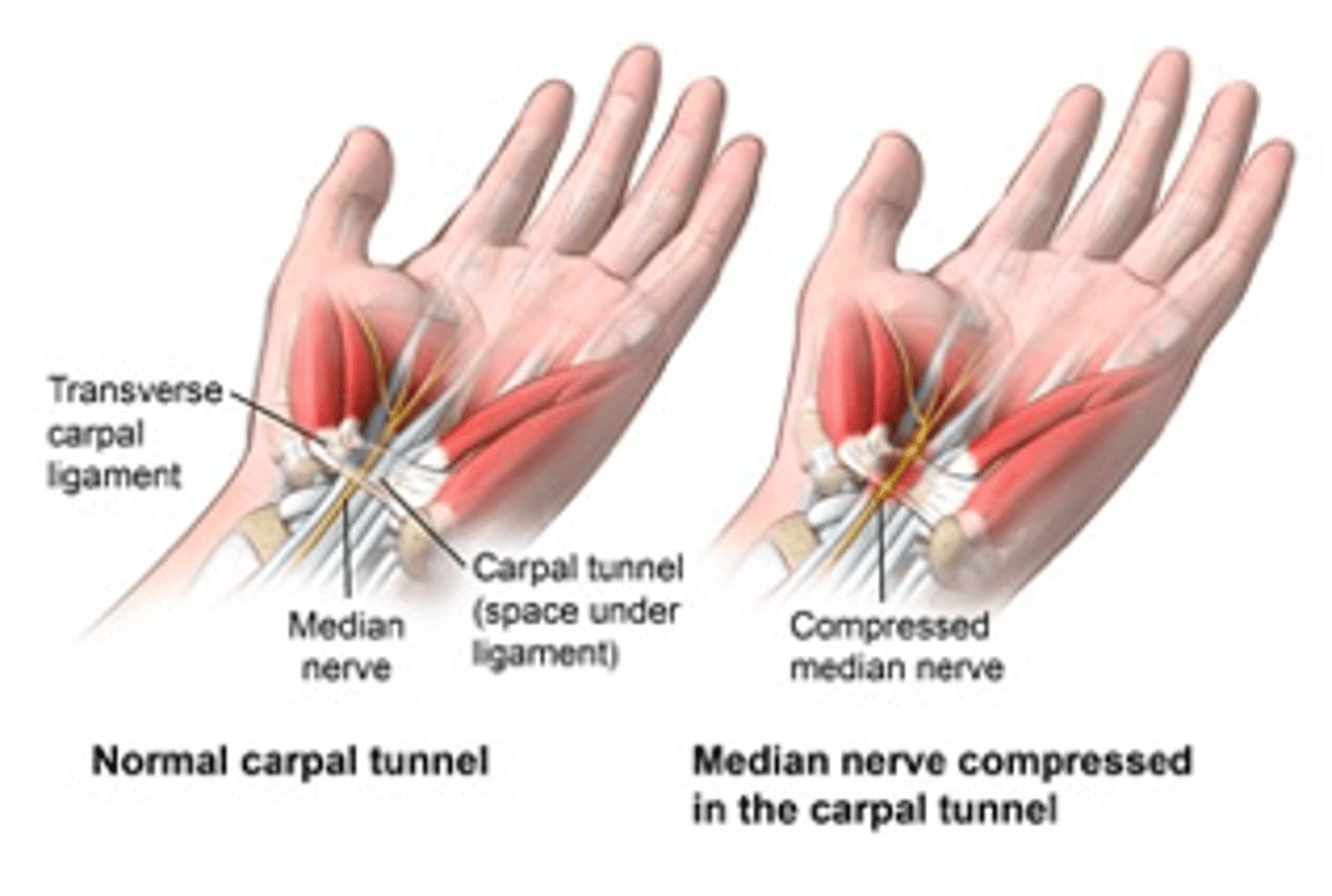
carpral tunnel syndrome
compressive neuropathy of the median nerve at the level of the wrist
Carpral tunnel syndrome epidemiology
most common compression neuropathy of the upper extremity
Carpral tunnel risk factors
female
obesity
pregnancy
hypothyroidism
rheumatoid arthritis
advanced age
chronic renal failure, alcoholism
smoking
Carpral tunnel important hx
•Numbness and tingling in the thumb, index finger, middle finger and radial aspect of the ring finger
•Sx worse at night w/ nocturnal awakening or when driving
•Patient reports needs to shake out the hand to get relief
•Weak grip or hand clumsiness
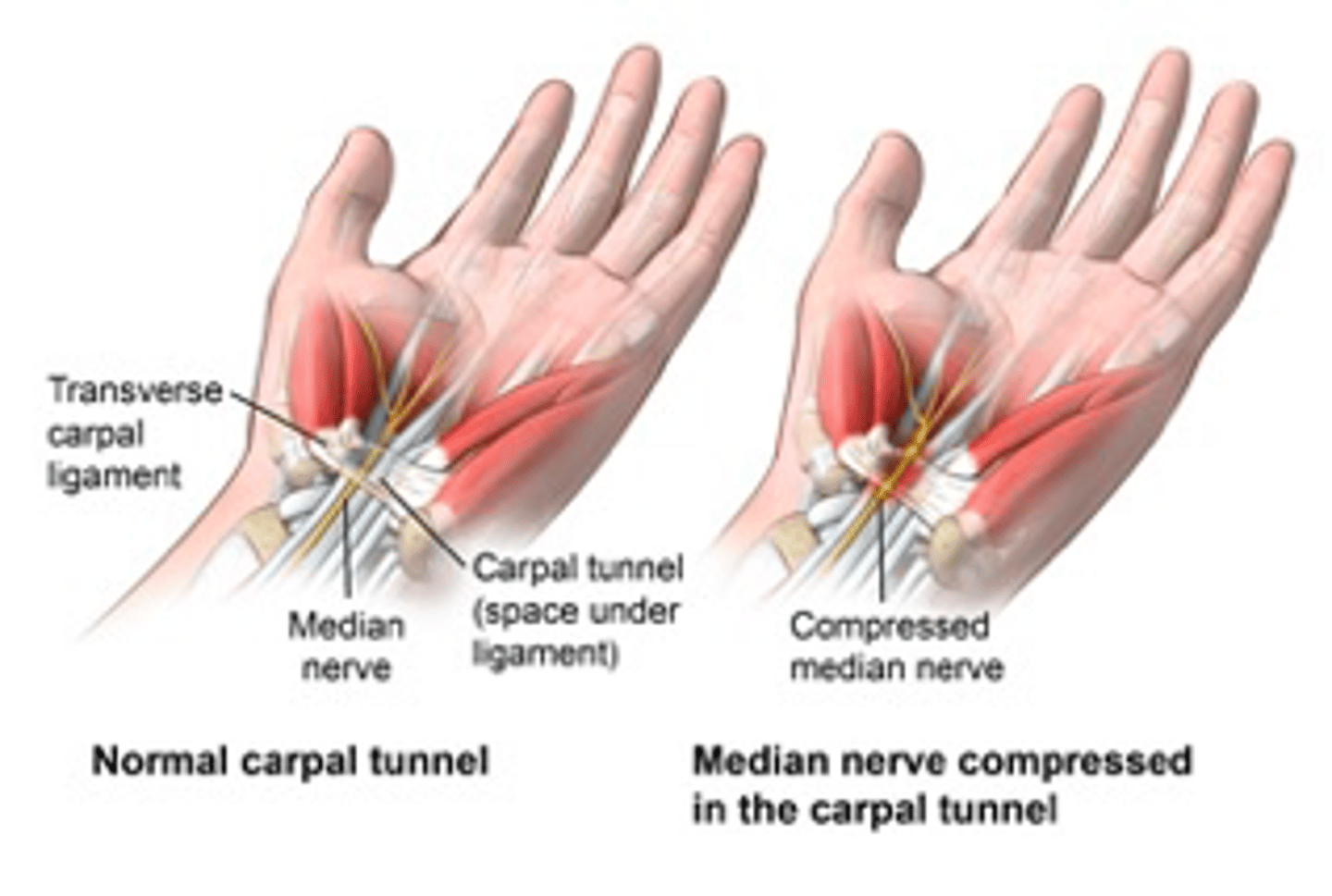
PE of Carpral Tunnel syndrome
•Inspect for thenar atrophy (severe involvement)
•Diminished 2 point discrimination, microfilament testing in median nerve distribution
•Weakness with resisted thumb abduction
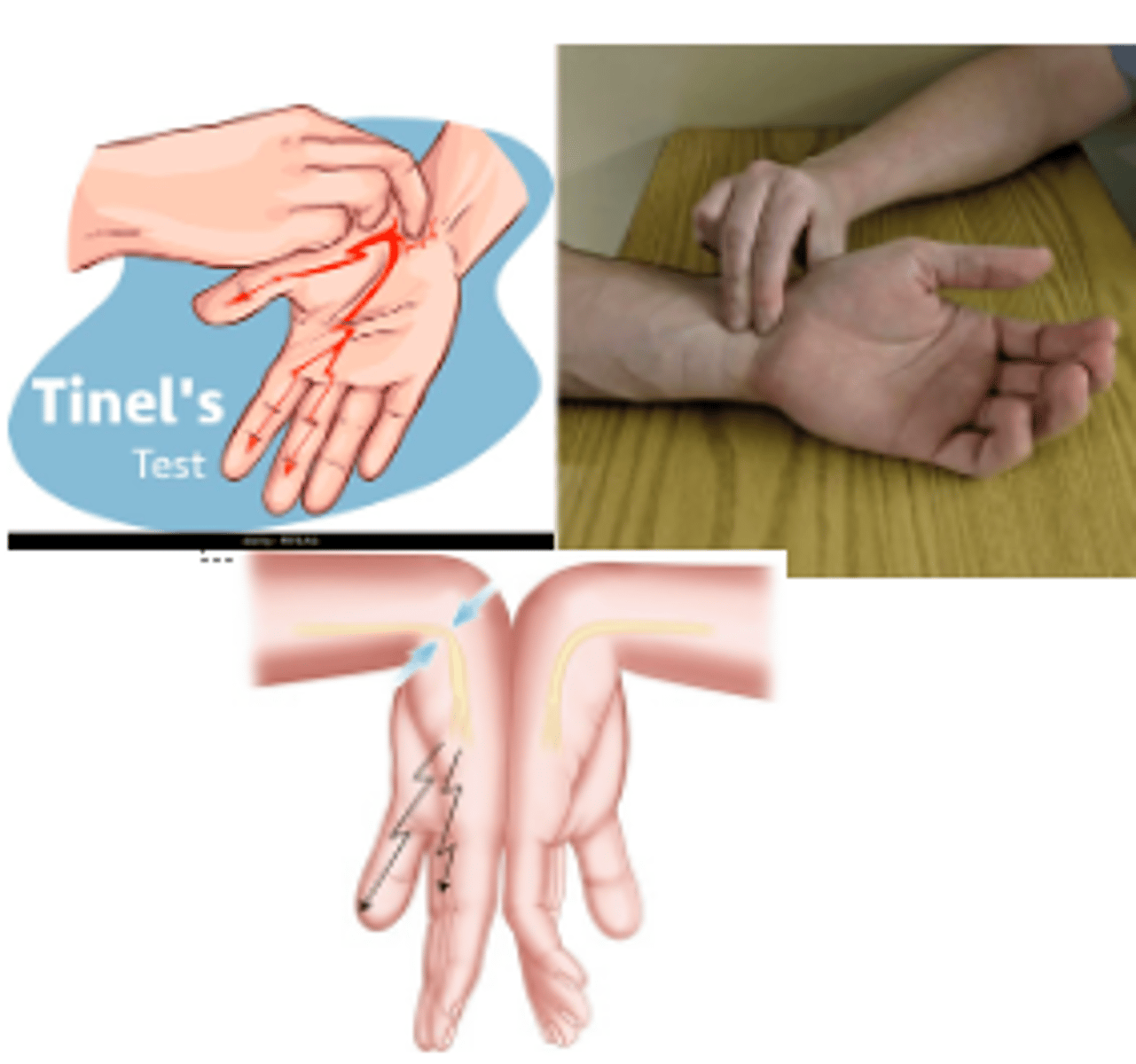
Carpral tunnel special tests
Phalen
Tinel
Pressure test
Carpral tunnel syndrome studies
EMG/NCS = GOLD STANDARD
•Can identify median nerve compression and determine severity.
•Make sure to also eval DDX such as cubital tunnel syndrome, cervical radiculopathy and peripheral neuropathy
Carpral tunnel syndrome tx
Nighttime bracing: Adjust wrist positioning when sleeping (avoid flexion)
Steroid injection
-Can be both diagnostic and therapeutic
-80% have transient improvement of symptoms (20% remain symptom-free at one year)
Surgery: Carpel tunnel release
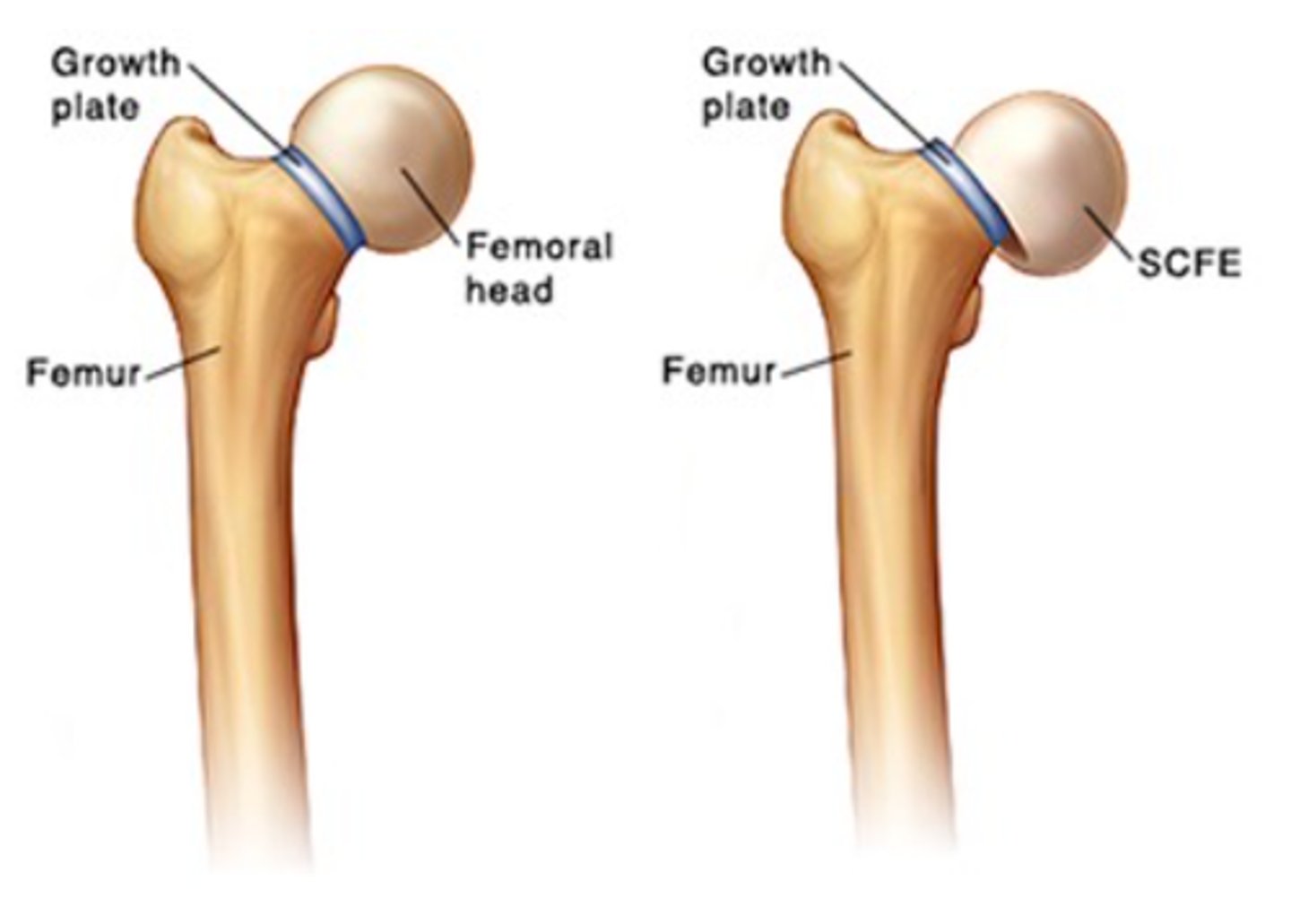
Slipped Capital Femoral Epiphysis (SCFE)
SCFE is a proximal femoral physis condition that involves slippage of the metaphysis relative to the epiphysis
Slipped Capital Femoral Epiphysis (SCFE) epidemiology
•Most common in adolescents 11-14 y/o (puberty)
•African Americans, Pacific islanders, Latinos
•More prevalent in males 2:1
•Left hip more common but could be bilateral
Slipped Capital Femoral Epiphysis (SCFE) etiology (risk factors)
Obesity #1 risk factor
(higher prevalence in obese male children)
important hx in Slipped Capital Femoral Epiphysis (SCFE)
•Chronic atraumatic hip pain (some may be traumatic)
•Hip pain radiates to thigh, groin or knee
•May only present with knee pain (lead to miss diagnosis)
•Limping
Slipped Capital Femoral Epiphysis PE
Inspection: antalgic gait, limp or waddling
Decrease ROM w hip internal rotation, abduction, and flexion
Weakness +/- thigh atrophy
Slipped capital femoral epiphysis Imaging/findings
XRAY
- ice cream falling off cone (L hip in image)
- growth plate widening or lucency
- blurring of proximal femoral metaphysis

Slipped Capital Femoral Epiphysis (SCFE) tx
Refer to ortho for surgery
Surgery: Percutaneous pin fixation
(+/- prophylactic pin fixation of contralateral hip in high-risk patients)

Avascular necrosis
Condition involving decreased blood along the epiphysis of a long bones
avascular necrosis epidemiology
•Most common location is the hip (femoral head) but may occur at the knee, talus, and humeral head
•More prevalent in males
avascular necrosis etiology risk factors
•Trauma- Femoral head fracture most common cause (effecting medial femoral circumflex artery)
•Alcoholism
•Chronic steroid use
•Sickle cell anemia
•Idiopathic
Avascular necrosis important hx
•Gradual onset of pain
•Pain worse with running, stairs or inclines
•Pain along anterior hip
•History similar like hip arthritis
avascular necrosis PE
•Early onset will have normal exam
•In advance stages will have exam like hip arthritis (pain and decrease ROM with hip internal and external rotation)
avascular necrosis imaging and findings
X-ray
•Sclerosis or cystic changes
•Flattening, subchondral radiolucent lines
•Subchondral collapse of the femoral head
MRI-GOLD STANDARD if x-ray is inconclusive and have a high suspicion. Highest sensitivity (99%) and specificity (99%)
•Bone marrow edema and chondral changes

avascular necrosis tx
conservative management
Bisphosphonates: Some studies show in early stages it may prevent femoral head collapse with subchondral lucency
avascular necrosis tx
surgery
Several different surgical interventions. Procedures:
•Total hip arthroplasty
•Decompression +/- bone grafting
•Rotational osteotomy
•Total hip resurfacing

anterior cruciate ligament tear
knee injury that leads to anterior and lateral rotatory instability of the knee
ACL tear epidemiology
•Half of all knee injuries
•More common in female athletes
ACL tear etiology
•Typically noncontact injury: tibia translates anteriorly while knee is in slight flexion while in valgus
•Common activities: soccer, basketball, skiing, and football
What other tear is common in an ACL tear
lateral meniscal tear (54%)
Important hx for ACL tear
•Patient reports feeling or hearing a "POP" at the time of injury
•Immediate pain and effusion/swelling
•Difficulty weightbearing
•Patient unable to continue activity or complete sporting event
•Acute trauma/blow to lateral aspect of the knee