Exam 1
1/105
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
106 Terms
indicators of perfusion
level of consciousness
pulses
skin color/temperature
capillary refill time
urine output
preload
filling pressures/volume (end diastolic volume). right heart → central venous pressure (CVP); left heart → pulmonary artery occlusion pressure (PAOP/PAW(edge)P)
lumens of pulmonary artery catheter
proximal, distal, thermistor, balloon inflation
measurements from pulmonary artery catheter (PA line)
cardiac output
SvO2
pulmonary artery pressures - left heart preload (PAOP/PAWP)
measurements from central venous line
pulmonary artery pressures - right heart preload (CVP)
ScvO2
evaluating oxygenation
oxygen delivery - CO, arterial oxygen content (Hgb, SaO2, PaO2)
oxygen consumption/venous O2 saturation - normal is ~60-75%
SaO2
percentage of hemoglobin that are carrying oxygen
measured with pulse ox
normal range >94%
PaO2
partial pressure of oxygen dissolved in the blood (plasma)
ABG
normal range 80-100 mmHg
ScvO2 - central venous oxygen saturation
amount of O2 in blood returning to heart after tissues have taken O2; reflective of upper body only - more commonly used
measured with central venous catheter
normal range 70-80%
SvO2 - mixed venous oxygen saturation
amount of O2 in blood returning to heart after tissues have taken O2; true mixed-venous gas reflecting whole body
measured with swan-ganz (pulmonary artery) catheter
normal range 60-80%
P wave
impulse from SA node through the atria
atrial depolarization
atrial contraction takes place milliseconds after depolarization
P-R interval
time required for atrial depolarization
atrial contraction
.12-.20 sec
QRS complex
impulse from bundle of HIS → to bundle branches → to Purkinje fibers
ventricular depolarization
also atrial repolarization (but this is not visible on ECG)
<.10 sec
ST segment
ventricular contraction
T wave
ventricular repolarization
U wave
Purkinje fiber repolarization. rarely seen, may occur in cases of digoxin toxicity, hypokalemia
QT interval
normal is less than or equal to 0.44 sec, danger over .50 seconds
prolonged QT (ventricles take longer to recharge during beats) can cause dangerous arrhythmias
can be due to congenital heart problems, electrolyte imbalances, or medication side effects
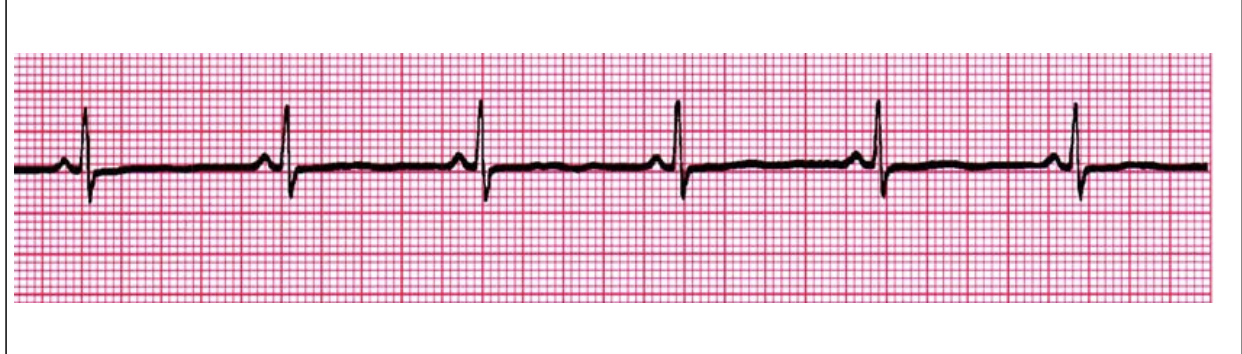
Regular Sinus Rhythm
Rate: 60-100 bpm
Rhythm: R - R =
P waves: Upright, similar
P-R: 0.12 - 0.20 sec & consistent
qRs: 0.04 - 0.10 sec
P:qRs: 1P:1qRs
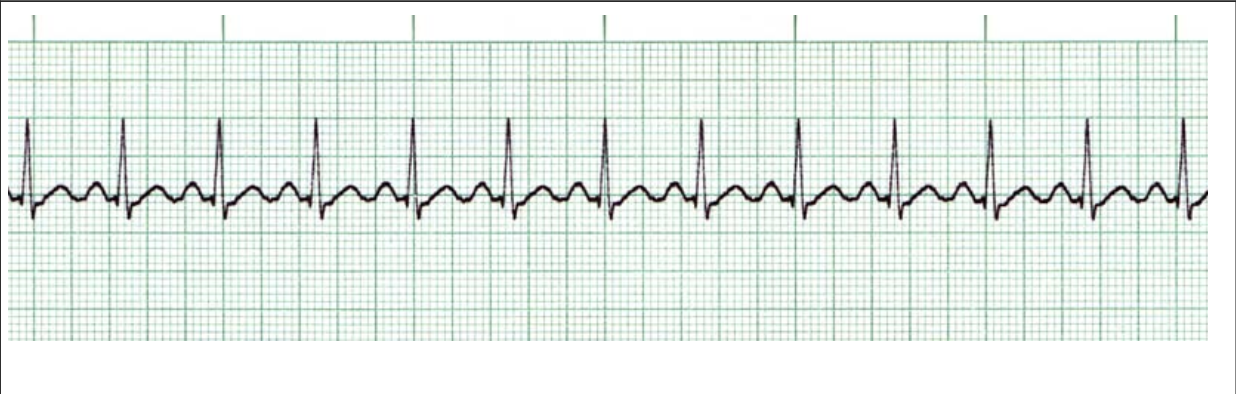
Sinus Tachycardia
Rate: >100
Rhythm: R- R =
P waves: Upright, similar
P-R: 0.12 - 0.20 sec and consistent
qRs: 0.04 - 0.10 sec
P:qRs: 1p:1qRs
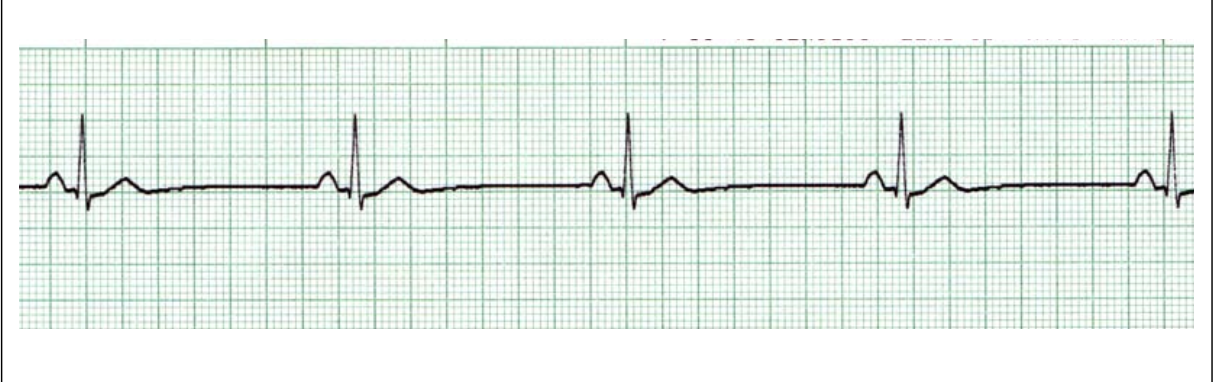
Sinus Bradycardia
Rate: <60
Rhythm: R- R =
P waves: Upright, similar
P-R: 0.12 - 0.20 sec and consistent
qRs: 0.04 - 0.10 sec
P:qRs: 1P:1qRs
symptoms: syncope, change in mental status, hypotension, SOB, diaphoresis, chest pain

Premature Atrial Contractions (PAC)
Rate: usually <100, dependent on underlying rhythm
Rhythm: irregular
P waves: early and upright, different from sinus
P-R: 0.12 - 0.20 sec, different from sinus
qRs: 0.04 - 0.10 sec
P:qRs: = 1:1
Causes: normal, excessive use of caffeine/tobacco/alcohol, CHF, myocardial ischemia or injury, hypokalemia, digoxin toxicity, COPD
Atrial Flutter
Rate: atrial rate 250-350, ventricular rate 150 common
Rhythm: atrial regular, ventricular regular or irregular
P waves: not identifiable
F waves: uniform (sawtooth or picket fence)
PRI: not measurable
qRs: 0.04-0.10 sec
Causes: ischemic heart disease, hypoxia, acute MI, digoxin toxicity, mitral or tricuspid valve disease, PE
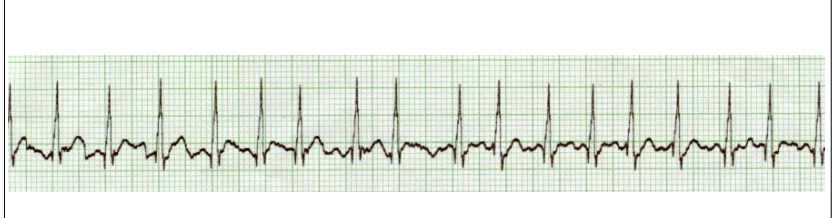
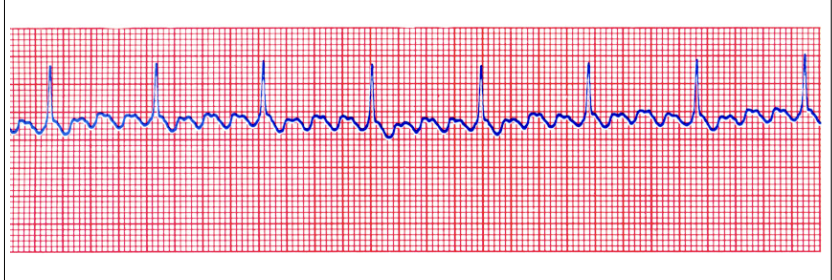
Atrial Fibrillation
Rate: atrial 400-700, ventricular 160-180 bpm
Rhythm: atrial and ventricular irregular
P waves: not identifiable
f waves: may be seen
P-R: unable to measure
qRs: usually normal
causes: ischemic heart disease, hypoxia, acute MI, digitalis toxicity, mitral or tricuspid disease
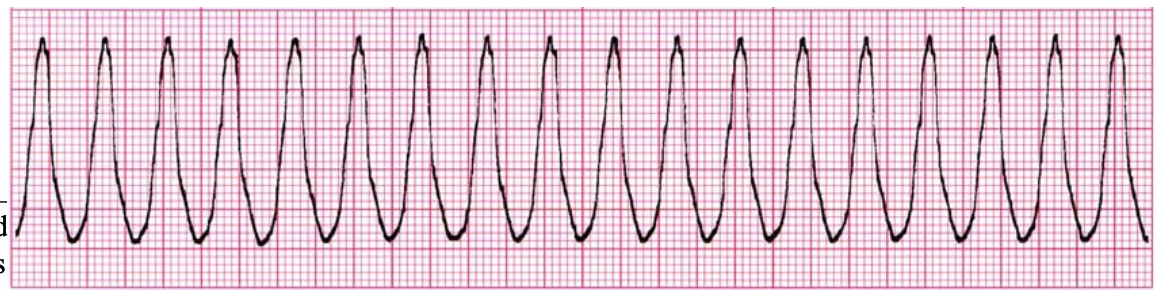
Ventricular Tachycardia (V-tach)
rate: 180
regularity: regular
P wave: no
P:QRS ratio and PR interval: n/a
QRS width: .26
causes: toxin, hypovolemia, hypoxia, hypothermia, toxins, cardiac tamponade, MI, PE, acidosis, K± issues
treatment for V-tach with a pulse
treat cause
anti-arryhthmic medications (amiodarone)
cardioversion
treatment for pulseless V-tach
initiate CPR
defibrillation
epinephrine, amiodarone
address the cause
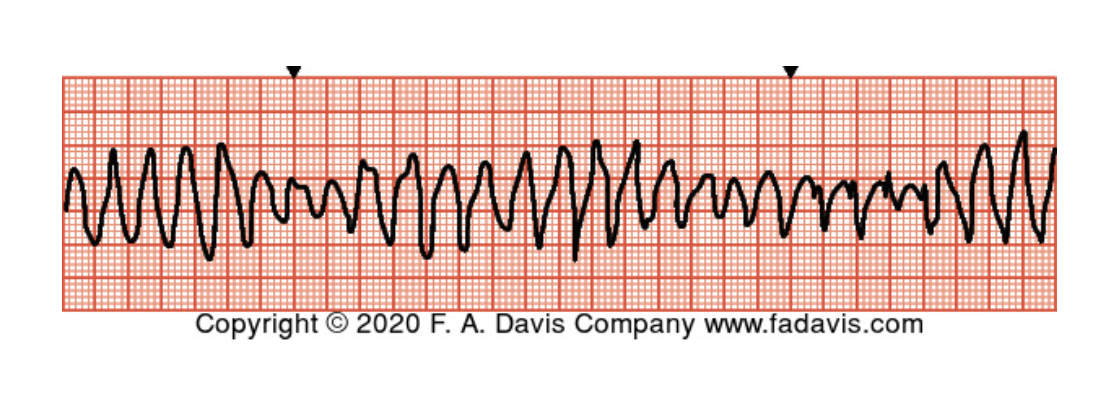
Polymorphic Ventricular Tachycardia (Torsade’s de Pointes)
Rate: 270
Regularity: Chaotic
No P wave (so P:QRs ratio and PR interval n/a)
QRS width: .20
treatments: v-tach tx, magnesium
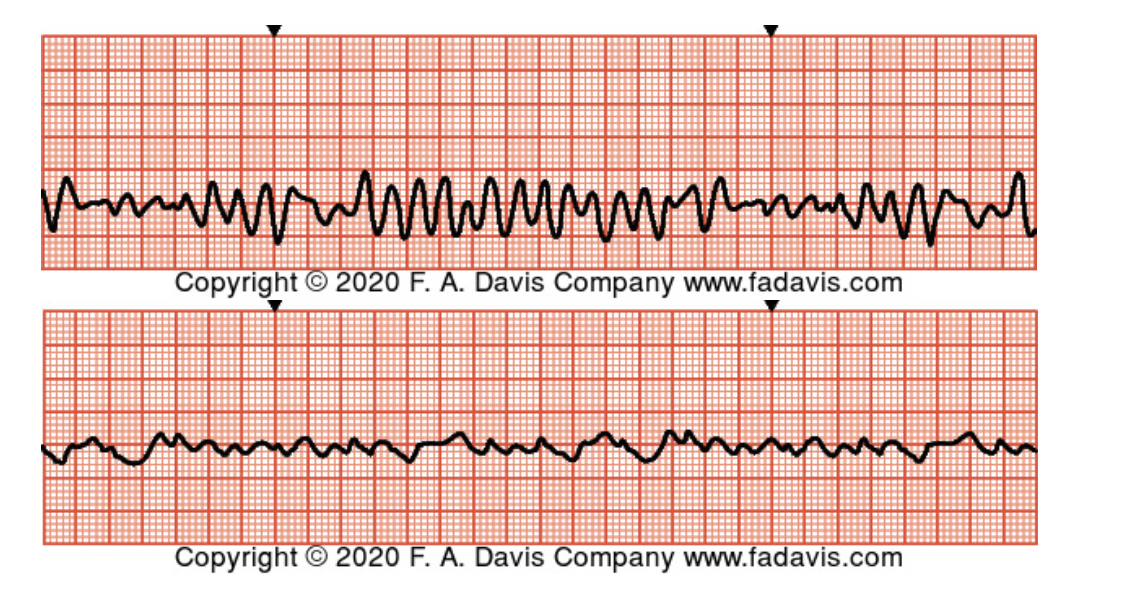
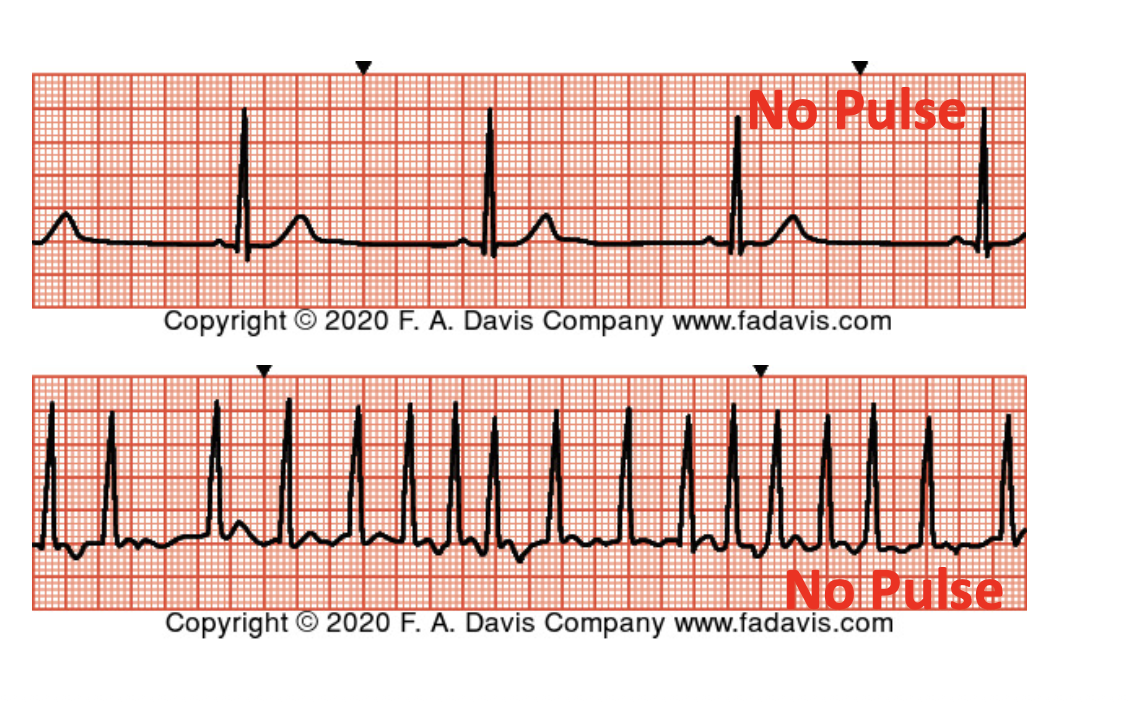
Ventricular Fibrillation
rate: n/a
regularity: chaotic
no P wave, P:QRS ratio, PR interval, identifiable QRS width
tx: initiate CPR, defibrillate immediately
causes: hypovolemia, hypoxia, acidosis, hypo/hyperkalemia, hypoglycemia, hypothermia, toxins, cardiac tamponade, MI, PE
pulseless electrical activity (PEA)
any viable rhythm without a pulse
tx: initiate high quality CPR, epinephrine, repeat
H’s and T’s
potential reversible causes of cardiac arrest or PEA
H’s: hypovolemia, hypoxia, hydrogen ion (acidosis), hypo/hyperkalemia, hypothermia
T’s: tension pneumothorax, tamponade (cardiac), toxins, thrombosis (pulmonary), thrombosis (cardiac)
defibrillation
not synchronized - delivered at any time in cardiac cycle
higher energy (electricity)
indications - ventricular fibrillation, pulseless v-tach
cardioversion
synchronized
delivered on R wave
lower energy (electricity)
indications: atrial fibrillation (after anticoagulation), unstable tachyarrhythmias
epinephrine
first line for pulseless rhythms
1mg q4min
amiodarone
antiarrhythmic
reduces heart rate
drip used in tachyarrhythmias
atropine
antimuscarinic anticholinergic
increases heart rate
used in bradycardias
1mg IVP
adenosine
converts, stops or slows rhythms
6mg IVP
prepare additional 12mg IVP if needed
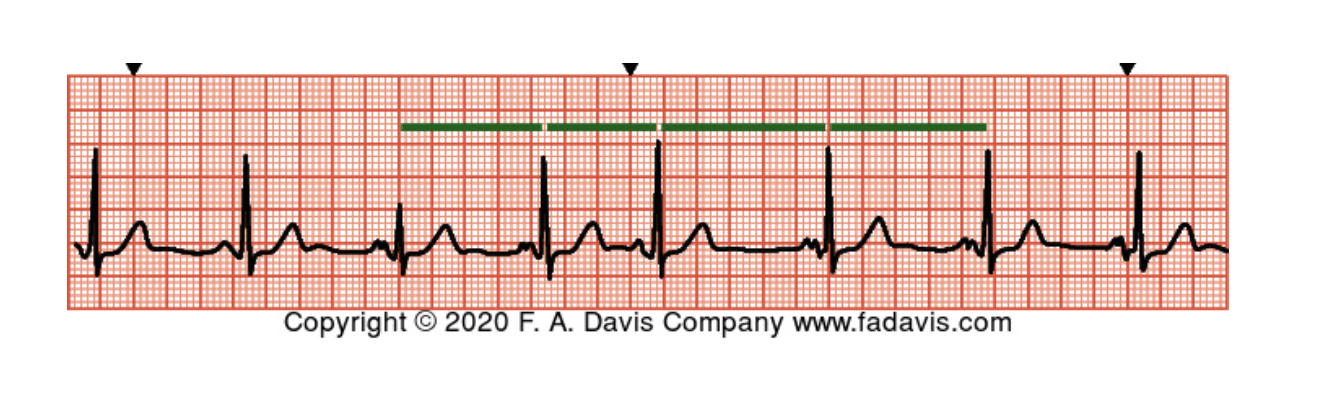
sinus arrhythmia - has to have a greater than 10% variation on P-P waveform max and min cardiac cycle
rate: 80
regularity: irregular
P-wave: yes
P:QRS ratio: 1:1
PR interval: 0.14
QRS width: 0.06
treatment of sinus tachycardia
distinguish whether symptomatic, compensating
treat cause
meds: beta blockers, CCBs
atrial fibrillation management
anticoagulation: heparin infusion, oral anticoagulants
rate control: sodium channel blockers, beta blockers, potassium channel blockers, nondihydropyridine CCBs, digoxin
rhythm control: meds, cardiac ablation, cardioversion, pulmonary vein isolation (PVI) an/or ICD/PPM
factors influencing organ perfusion
adequate oxygen availability - patent airway, adequate ventilation, adequate perfusion, respiratory assessment/ABG/SpO2
oxygen movement - sufficient Hgb, CBC, H&H, contractility
oxygen demand - is there an increased demand body is unable to meet, SvO2, ScvO2, lactate
oxygen exchange - vascular tone (dilation/constriction), blood/fluid status, blood pressure (MAP)
stages of shock
initial - initial insult, subtle changes in assessment/VS, beginning of cell damage
compensatory - compensatory mechanisms begin, tachypnea/tachycardia, decreasING BP and urine output
progressive - compensatory processes fail, blood shunted to vital organs
refractory - prolonged tissue hypoperfusion, multi-system organ failure, irreversible
DIC - disseminated intravascular coagulopathy
overwhelming inflammatory response leads to excessive clotting, which exhausts clotting factors and this depletion leads to excessive bleeding
DIC labs
elevated d-dimer r/t clots
decreasing clotting factors (platelets, fibrinogen)
increased clotting times (PTT, INR)
increased fibrin degradation products
DIC treatment
supportive care: optimize oxygenation, pH, electrolytes
treat cause
volume replacement and replacement of clotting factors
bleeding precautions
MODS: multiple organ dysfunction syndrome
decreased oxygen delivery to organs + increased oxygen demand + poor oxygen utilization
organ dysfunction leads to organ death
lungs and kidneys usually first
40% mortality w lung involvement, 80-90% mortality once 3 organs are involved
identification: depends on system failing, i.e. respiratory failure, anuria, absent bowel sounds
tx: supportive care, treatment of cause
assessment findings - initial stage of shock
subtle changes to baseline, or no change at all
may see lactate this early
assessment findings - compensatory stage of shock
subtle mental status change (restlessness, confusion)
tachycardia
weak pulses
decreasing BP, narrowing pulse pressure
tachypnea - respiratory alkalosis
decreasing urine output
cool, moist skin
assessment findings - progressive stage of shock
lethargy or coma
hypotension
dysrhythmias
anuria
absent bowel sounds
metabolic/respiratory acidosis (or both)
cold extremities
weak/absent pulses
assessment findings: refractory stage of shock
coma
hepatic, renal failure
peripheral ischemia and necrosis
obstructive shock
obstruction to ventricular filling and/or emptying, decreasing cardiac output. independent of other mechanisms
obstructive shock - causes that impair filling
tension pneumothorax: disruption in thoracic pressure presses on the heart. cardinal signs = decreased breath sounds on one side, tracheal deviation. tx with needle decompression
cardiac tamponade: fluid around the heart presses on the heart. cardinal signs = muffled heart sounds, JVD, hypotension with narrow pulse pressure (Beck’s triad). tx w pericardiocentesis
obstructive shock - causes that impair emptying
pulmonary embolism: clot in the lung blocking blood flow into pulmonary vasculature. cardinal signs: sudden shortness of breath, hemoptysis. tx w thrombolytic, thrombectomy
hemodynamic findings of obstructive shock
HR: ↑ r/t compensation
BP: ↓ r/t deficient CO
preload: ↑ OR ↓ (dependent on variables)
afterload/SVR: ↑ r/t compensation
contractility: no change
hypovolemic shock
inadequate vascular volume resulting in inadequate CO
hypovolemic shock causes
fluid loss dt vomiting/diarrhea, dehydration, blood loss, internal bleeding
clinical manifestations of hypovolemic shock
hypotension, tachycardia, change in mental status, pale/cool/clammy skin, weak pulses, prolonged capillary refill, decreased urine output
hemodynamic findings of hypovolemic shock
HR: ↑ r/t compensation
BP: ↓ r/t deficient intravascular volume
preload: ↓ r/t deficient intravascular volume
afterload/SVR: ↑ r/t compensation
contractility: ↑ r/t compensation
diagnostic findings for hypovolemic shock:
SpO2, PaO2, ScO2: Normal until late stages (pt still oxygenating, all hgb still carrying O2)
pH: High during compensatory stage (hyperventilation), low when body shifts to anaerobic metabolism
PaCO2: Low in compensatory stage (hyperventilation), high in late stages if pt develops respiratory distress
Lactate: Elevated when pt transitions to anaerobic metabolism
Hemoglobin: Low with blood loss
BUN: High in dehydration
Creatinine: High in kidney injury
anaphylactic shock
distributive shock caused by extreme hypersensitivity reaction to an allergen
anaphylactic shock pathophysiology
exposure to allergen → histamine response → venous dilation, increased capillary permeability, smooth muscle contraction → airway compromise, angioedema, profound hypotension
clinical manifestations of anaphylactic shock
airway compromise: SOB, tachypnea, wheezing, stridor, cyanosis, mental status change
vasodilation and capillary leak → “relative hypovolemia”: hypotension, tachycardia, cool/pale skin, weak pulses, peripheral edema
hypersensitivity reaction: angioedema, flushing, uticaria, rash
hemodynamic findings of anaphylactic shock
HR: ↑ r/t compensation
BP: ↓ r/t vasodilation, capillary leak
preload: ↓ r/t decreased venous return
afterload/SVR: ↓ r/t vasodilation
contractility: ↓ r/t coronary hypoperfusion, damage
treatment of anaphylactic shock
remove allergen first
administer epinephrine IM second
rescue: oxygenation - apply oxygen via NRB, prep for advanced airway) cardiovascular - IV fluids (need IV access)
ongoing: antihistamines, corticosteroids to shorten/calm anaphylactic rxn and decrease airway swelling, bronchodilators to relieve bronchoconstriction
neurogenic shock pathophysiology
injury to nervous system d/t by spinal cord or brain injury causes:
sympathetic disruption - loss of vascular tone (SVR) → vasodilation, decreased venous return, relative hypovolemia
unopposed parasympathetic response - bradycardia → low CO d/t low HR/SV, loss of compensatory tachycardia
hypotension, hypoperfsuion of tissues, anaerobic metabolism
neurogenic shock clinical manifestations
warm, dry, flushed skin r/t vasodilation
hypotension r/t decreased vascular tone (SVR)
bradycardia r/t unopposed parasympathetic activiy
↓ venous return - ↓ SV, CVP
↓ CO r/t bradycardia, ↓ SV
LOC changes r/t acidosis, hypoperfusion
elevated lactate, metabolic acidosis r/t anaerobic metabolism from ↓ perfusion
medical management of neurogenic shock
priority is maintain vital functions → rescue. tx hypotension = fluid administration, vasopressor infusion; tx bradycardia = atropine, pacing; tx respiratory compromise = intubation w mechanical ventilation
definitive: tx for cause
serial labs: lactate, ABG
septic shock
shock caused by body’s uncontrolled response to infection. insult (infection) → localized inflammation becomes systemic → distributive shock. leading cause of in-hospital deaths in the U.S.
septic shock pathophysiology
local response to infection = ↑ capillary permeability, mobilization of macrophages/neutrophils, formation of fibrin mesh
systemic (septic response) = systemic ↑ capillary permeability - vasodilation, capillary leak, relative hypovolemia, ↓ venous return and CO; hypercoagulation - septic emboli, DIC
clinical manifestations of early sepsis - hyperdynamic/”warm”
fever
tachycardia
bounding pulses
warm, flushed skin
decreasing BP and urine output
confusion/restlessness
increased CO
clinical manifestations of late sepsis - hypodynamic/”cold”
cool, pale skin
weak, thready pulses
hypothermia (very late)
decreased CO
hemodynamic findings for septic shock
HR: ↑ r/t compensation
BP: ↓ r/t decreased venous return
Preload: ↓ r/t decreased venous return
Afterload/SVR: ↓ r/t vasodilation
Contractility: ↑ in early/hyperdynamic stage r/t compensation
diagnostic findings for septic shock
ABG: respiratory alkalosis early, metabolic acidosis later
lactate: ↑ r/t anaerobic metabolism
leukocytes: ↑ r/t infectious process
cultures: + based on organism
clotting studies: ↓ in clotting factors (platelets, fibrin), ↑ clotting time (PTT, INR)
organ function: renal (creatinine), hepatic (AST/ALT) ↑ as organ dysfunction progresses
SCCM sepsis guidelines (hour-1 bundle)
measure lactate level
obtain blood cultures before administering antibiotics
administer broad spectrum antibiotics
begin rapid admin of 30mL/kg crystalloid for hypotension or lactate greater than or equal to 4 mmol/L
apply vasopressors if hypotensive during or after fluid resuscitation to maintain a mean arterial pressure greater than or equal to 65mmHg
cardiogenic shock pathophysiology
decreased oxygen supply to heart muscle, anaerobic metabolism → lactic acidosis
decreased heart contractility → decrease in CO
cardiogenic shock risk factors
co-morbidities: decompensated HF
trauma: blunt chest trauma
post-surgery: CABG
direct tissue injury: STEMI
cardiogenic shock clinical manifestations
hemodynamics: CO and SV ↓
↓ LOC/altered mental status
SOB
tachycardia, tachypnea
hypotension (narrowed pulse pressure - compensatory vasoconstriction maintains diastolic pressure while systolic pressure fails dt ↓ SV)
diaphoresis, pallor
N/V
cardiogenic shock diagnostics
diagnostic testing: CXR, echocardiogram, ECG, coronary angiography
laboratory testing: troponin, BNP; ABG/VBG, lactate, CMP
medications for cardiogenic shock
vasoactive (i.e. norepinephrine) - increase MAP and perfusion
inotropes (i.e. dobutamine) - increase contractility and CO
diuretics (i.e. furosemide) - decrease preload and fluid overload
surgical and supportive management for cardiogenic shock
mechanical circulatory support (MCS)
intra-aortic balloon pump (increases coronary perfusion by improving filling and decreasing afterload - balloon inflates during diastole and deflates during systole)
ventricular assist device - implantable
extracorporeal membrane oxygenation
heart transplant (rare)
pathophysiology of MI
vessel wall injury → atherosclerotic plaque build-up → obstruction of oxygen-rich blood flow through coronary vessels → plaque rupture and thrombosis
progression of vessel plaque build-up
plaque disruption and thrombus formation causes unstable angina → thrombus grows and causes partial occlusion (NSTEMI) → thrombus continues to grow and causes complete occlusion (STEMI)
typical clinical manifestations of MI
sternal chest pain
shoulder and arm pain
anxiety, impending doom
non-typical clinical manifestations of MI
dizziness, lightheadedness
N/V
indigestion
fatigue
radiation to neck/jaw/back
more common in women
diagnostic tests
lab tests: troponin I (highly sensitive to cardiac tissue), creatinine kinase, CK-MB/LDH (cardiac and tissue biomarkers used to detect damage), BMP/CBC/BNP/Lipid profile
diagnostic tests: 12 lead ECG, cardiac angiography (left heart catheterization)
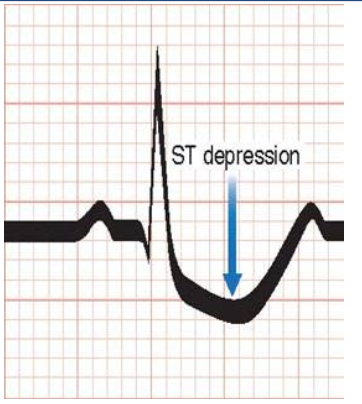
ischemic changes in MI ECG
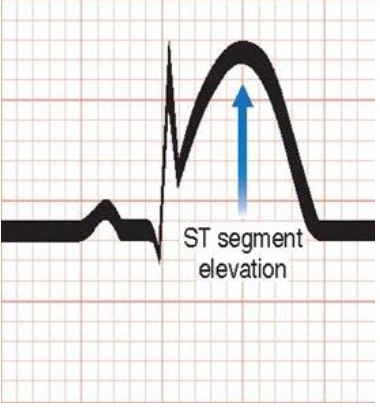
infarction - ST elevation in MI ECG. lasts mins to hours
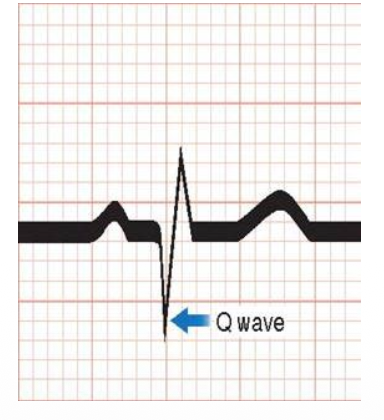
Q wave in MI ECG. up to 12 hours
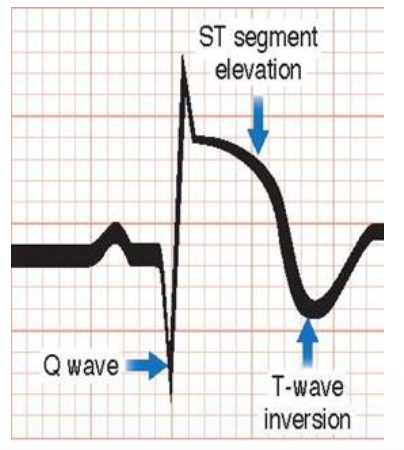
ST elevation with T wave inversion in MI ECG. can persist for 2-5 days
treatment goals of medical management of MI
maximize oxygenation
control pain
dilate coronary arteries
prevent clots
decrease myocardial workload
percutaneous coronary intervention
type of reperfusion therapy, performed in cath lab, minimally invasive procedure used to open clogged coronary arteries and restore blood flow to the heart
medications given during MI
morphine for pain
oxygen
nitroglycerin
aspirin - ASA (325mg)
medication given after MI
daily aspirin - ASA (81mg)
beta blockers
lipid lowering medications (i.e. Statins)
Antiplatelets (i.e. Clopidogrel)
ACE-Is or ARBs
coronary artery bypass graft (CABG)
surgical procedure used to treat severe coronary artery disease by creating new pathways (detours) for blood and oxygen to bypass blocked or narrowed arteries feeding the heart muscle.
single bypass = one artery or vein is used to bypass a single blocked vessel
double bypass = two grafts are placed to bypass two blocked vessels
…and so on to triple, quadruple, etc
complications of CABG
arrhythmias
bleeding
infection
organ failure
cardiac tamponade (Beck’s triad: JVD, muffled heart sounds, hypotension)
quadruple therapy for meds after MI
beta blocker
statin
ASA
ACE or ARB
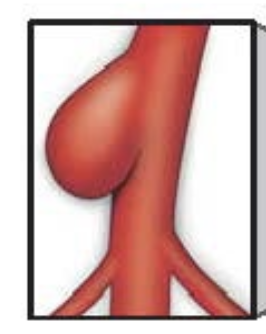
saccular aneurysm
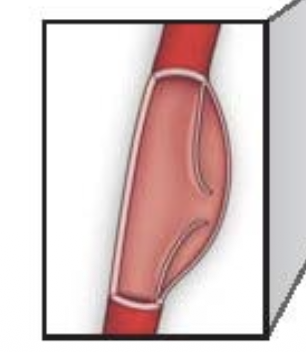
pseudoaneurysm - 1-2 layers involved
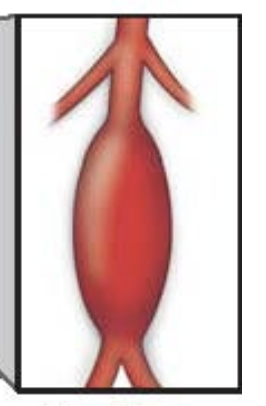
fusiform aneurysm - bulging of entire artery
aneurysm pathophysiology
media layer of artery is weakened → intima layer of artery is stretched → artery widens, tension increases, widening continues
50% widening is diagnostic, can stretch as wide as 2x diameter
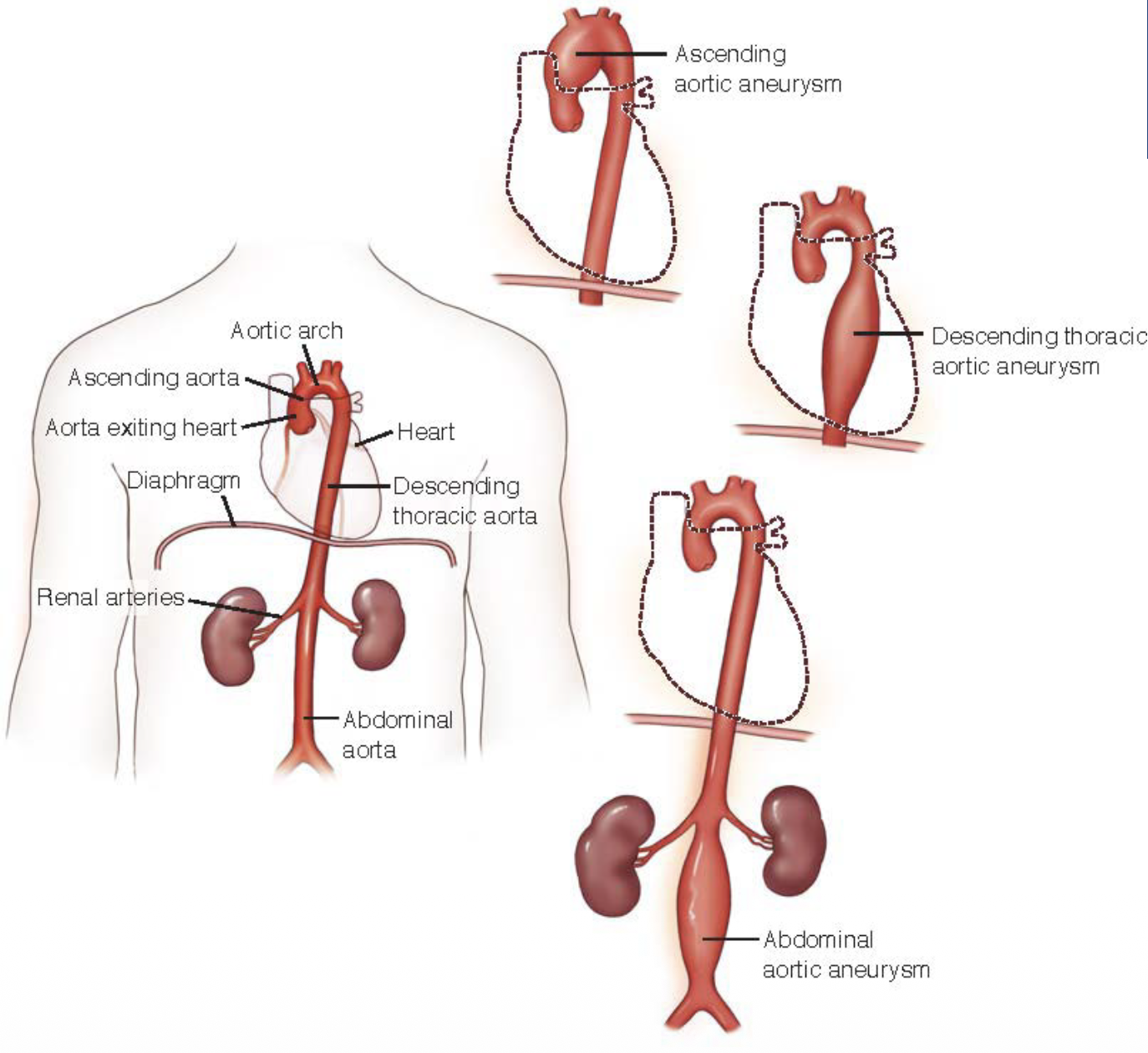
aneurysm types