PSYC3102 [Final]
1/120
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
121 Terms
Aging Population Changes
Less kids
Better elderly care
Improved sanitation
More importance to care about invesitgating dementia
Cognitive functioning best viewed as….
function of lifespan
Most prevalent type of dementia
Alzheimer’s Disease
Protective and risk factors are in main…
modifiable, but not accessible for all
T/F Dementia is not automatically a cause for lacking capacity
TRUE
Dementia is extremely…
heterogenous; interventions best when coordinated among healthcare professionals; people often wait years for a diagnosis
Dementia [Umbrella Cateogry] definition
a term for broad class of neurological disorders associated with cognitive, personality, and behaivoural changes in later life; IS A DISEASE, NOT PART OF PRIMARY AGEING
Dementia Proper Definition
An acquired syndrome of intellectual impairment produced by brain dysfunction
Dementia Process
Neurons in brain accumulate plaques or tangles (tau proteins) that deposit on cells → leads to cell death , no way of slowing or stopping process atm
Heterogenous disease meaning
Condition that has diverse range of underlying causes and symptoms; people with same diagnosis may experience condition in different ways
Dementia Vs Normal Ageing
Memory loss that disrupts daily life vs sometimes forgetting but remembering later
Problems with words [aphasia] vs trouble finding right word
Changes in mood or personliaty vs irritation at having routine disrupted
Difficulty completing familiar tasks vs help needed with new tasks
Factors for Developing Dementia
Socioeconomic factors and resources matter, if big gaps → results in unhealthy ageing
When testing cognitive decline….
Motor Declines can precede cognitive decline
Dementia Prevalence and Frequency
Prevalence:
between 65-69 is around 1%
between 75-79 is around 6%
Over 90 years of age:
around 40% of people exhibit symptoms of moderate or severe dementia
Types of dementia
Huntington’s disease
Dementia with Lewy Bodies
Alcohol related dementia
Frontotemporal dementia
AD (Alzheimer’s disease)
VaD (Vascular dementia)
Other
Preclinical Phase of Dementia
Silent phase: brain changes without measurable symptoms
individual may notice changes, but not detectable on tests
MCI phase of Dementia
Cognitive changes are of concern to individual and family
one or more cognitive domains impaired significantly
preserved activities of daily living
Final Dementia Phase
Cognitive impairment Severe enough to interfere with everyday abilties
Not every single person end up in this phase, may only end on MCI and not face severe cognitive decline
Younger Onset Dementia
Can affect people in their 30s and 40s
No cure to slow down, but psychosocial interventions effective
Usually succumb to other illnesses such as stroke or pneumonia
due to neuron loss impacting memory, and then affecting other areas like breathing and swallowing
requires sensitive and individualised care
Alzheimer vs Vascular Dementia
Gradual/Insidious vs Abrupt/Stopwise
Early/Prominent vs Variable/Mild Early
Later in course vs Early/Prominent
Common in moderate/late stages vs present visuospatial deficits
Word-finding difficulty vs mild language impairment
Behaviour changes at any stagr vs apathy and depression
Late gait changes vs gait disturbances and motor failures
Uncommon to have hallucinations early vs uncommon to have hallucinations
Alzheimer’s Disease History
Alois Alzheimer (1964-1915)
Had 51-year old patient (August Dieter) with strange disease of cerebral cortex
Ahead of time by reccomending shift away from institutional practices such as isolation rooms or restrictions
Promoted individualised hands on care (“treatment next to bed of patient and into day room”)
Burdekin Report (Human Rights and Mental Illness)
Elderly more likely to receive drugs and less likely to receive psychotherapy
Worst images associated with old mental instituions is still the case for many elderly sick people (being physically restrained or sedated)
Prejudice that old people are disposable and not worth spending money or energy on - that natural parts of getting old
Dementia Diagnosis
Need to take good clinical history
Take a medical exam (by geriatrician/geropsychiatrists)
Neuropsychological testing (not just screening)
Neuroimaging (MRI)
Ruling out other causes (depression, anxiety, medication, vitamin deficiency, etc.)
Differential Diagnosis: Delirium
Altered state of consciousness that have underlying cause
Symptoms unclude waxing, limited attention span, behavioural/psychiatric changes
Seen in older adults with UTIs or infections from surgical procedures/placement of catheters; also from medicatin SE
When treated, cognitive faculties regained
But usually unrecognised and untreated, and fatal if person self-harms
Need to reduce excess stimulation and educating family about situation
Risk Factors for dementia
Vascular damage (diabteses, smoking, obesity, air pollution, head injury, etc.)
Dementia neuropathology (depression, physical activity, alcohol intake)
Stress and inflammation (visual loss, social contact, hearing loss)
Cognitive and brain reserve (continue cognitive activity consistently)
Protective factors for Dementia
Physical Activity: regular training to improve blood flow
Nutritious diet: mediterranean-style high in veggies, fruits, nuts, and healthy fats
Social connection: 3 good friends, maintain social interaction
Cognitive stimulation: consistently engage in mentally stimulating activities
Good sleep: consistent routine
Neuropsychological Assessment
Cognitive
Behaviour
Emotion
Social
Dementia in Indigeous Context
Over 45 years is 12.4% and 26.8% for those over 65 years old
5.2 times higher than overall Aussie population
Need to adapt Western methods to be culturally sensitive
correct language, notions of time/space, appropriateness of discussing family matters
KICA tool has cultural;ly suitable items (ex: what season is it vs what year is it)
Assessment of Capacity/Competence
Important to see if people is legally capable unless determined otherwise
Presence of neurologic or psychiatric diagnosis/disability does not mean person is incapable
Refusal to cooperate does not mean person is incapable
Why is diagnosis hard for many?
Hesitant to recognise decline
Can result in lengthy delay as time goes on from having to see sympton onset → family recognition → general physician → specialist evaluation
GPs reluctant refer/not well-trained
Functional things become challenging (ex: driving)
Misinformation on dementia online
Dementia Australia best contact point for all
Dementia Medication Treatment
Acetylcholine levels are reduced - medications target this
Donepezil (Aricept) treatment which modifies symptoms but does not interfere with progression
Medications usually most effective earlier in progression
Dementia Psychologcial Treatment
Early - psychotherapy, CBT if depression main focus
Boost physical/mental/social activity
Managging heart health helps manage dementia
Develop routines to scaffold daily activities
Caregivers
Most are females, especially daughters
around 450,000 people live with dementia in Australia
around 1.6 million care for person with dementia
Self-care critical
respite single out as most desired by caregivers
help with understanding evolving needs
address fears with unpredicable nature of psychosis or aggression
Assessment tools for family carers
Burden scale for caregivers (10 items)
Zarit Burden Interviews (22, 12, 4 items)
Psychosocial approaches for caregivers
ABC
activating event, behaviour, consequences
faciliating effective communication (less shouting, more giving space/non-verbals)
Environmental modificationss
all aspects + creative activity planning
Active coping strategies
Recruit more supporters
Changing appraisals of stressors
Develop new skills, revive oldones
Cultivate sense of humor/forgive self and others
Look for positive moments to share with person with dementia
Environmental manipulations for dementia patients
PUT
Gardens
Pets
Children
DONT PUT
Distracting stimuli (TV, radio…)
Rigid rules
Lack of structure
Practical things to do with Dementia person
Update will with enduring guardian
Appoint enduring power of attorney
Make plan to manage driving
Get info and connect to relevant orgs
Build formal + informal support team
Healthy Ageing
Functional ability compromises health-related attributes that enable people to be and do
Made up of intrinsic capacity of individual, relevant env characeristics and interactions between two
Factors for Succesful Ageing
Minimise risk of disease and disability
Continue engagement with life
Maintain physical and cognitive function
Six factors model of well-being
Environmental Mastery
Autonomy
Self Acceptance
Purpose in life
Personal growth
Positive relationships with others
Hierarchy of flourishing
Base: identity and connectedness
Security and autonomy
Meaning and growth
Top: Joy
increases wellbeing with every step
Externalising disorders meaning
create problems for external world
breaking age-appropriate social rules/disobeying authority
anger and aggression
impulsivity
Internalising disorders
create problems for internal world
anxiety
sadness
Attention-Deficit/Hyperactivity Disorder (ADHD) Criteria
Persistent pattern of inattention and/or hyperactivity impulsivity
inattention (6 or more symptoms for at least 6 months)
Hyperactiivty and impulsivity (6 or more symptoms for at least 6 months)
Several symptoms present before 12 years old
Symptoms present in two or more settings (home, school, etc.)
Interfere with quality of social, academic, occupational functioning
No other explanations
ADHD Inattentive symptoms
Often fails to give close attention to details
Often has difficulty sustaining attention
Often does not seem to listen when spoken to directly
Often does not follow through on instructions and fails to finish
Often has difficulty organising
Often avoids, dislikes, or is reluctant to engage in tasks that require sustained mental effort
Often loses necessary things
Often easily distracted by external stimuli
Often forgetful in ddaily activities
ADHD Hyperactivity/Impulsivity Symptoms
Often fidgit with hands/feet
Often leaves seat in classroom/seated situations
Often runs about/climbs excessively
Often has difficulty playing quietly
Often on the go
Often talks excessively
Often blurts out
Often has difficulty waiting turn
Often interrupts or intrudes
Types of ADHD
combined presentation (ADHD-C): if both inattention and hyperactivity-impulsitivty are met for past 6 months
Predominantly inattentive presentation (ADHD-PI): if inattention met, but not hyperactivity-impulsivity
Predominanly hyperactive-impulsive presentation (ADHD-HI): if hyperactivity-impulsivity met, but not inattention
Oppositional Defiant Disorder (ODD) Criteria
Pattern of angry mood, argumentative behaviour lasting at least 6 months, evidenced by at least 4 symptoms, exhibited during interaction with at least one individual who is not a sibling
Angry/Irritiable mood
losing temper, touchy/easily annoyed, resentful
Argumentative behaviour
arguing with authority, defying rules/requests, annoys others, blames others
Vindicativeness
spiteful at least twice within past 6 months
Behaviour associated with distress in individual/others in their immediate social context/impacts social, educational, occupational areas of functioning
Behaviour does not exlclusively occur during course of psychotic, substance use, deressive, or bipolar
Specify if mild (symptoms confined to one setting), moderate (at least in two settings), severe (three or more settings)
Conduct Disorder (CD) criteria
Repetitive and persistent pattern of behaviour which basic rights/societal norms are violated, manifested by presence of three of following 15 criteria in past 12 months, at least one criterion present in past 6 months
Aggression to people/animals
bullies others, physical fights, uses weapon, physically cruel, stolen things (confrontational), forced sexual activity
Destruction of property
engaged in fire setting, destroyed others’ property
Theft/Deceitfulness
broken into things, lies to obtain goods, stolen items (unconfrontational)
Serious violation of rules
stays out at night, run away from home, truant from school
Disturbance in behaviour causing impairment in social, academic, occupational functioning
If older 18, and criteria not met for antisocial personality disorder
Specify if with limited prosocial emotions, lack of remose, callous - lack of empathy, unconcerned about performance, shallow or deficient affect
Adolescent Disorder Prevalence
Most common disorder in children + adolescent
in australia, 7.4% of all children and adolescents
more common in boys (12.9% of boys, 5.6% of girls)
ratio of 4:1 in children (1:6:1 in adults)
not necesarilly that girls less susceptible, but symptoms present differently in girls
In Australia
5.1% diagnosed with ODD; 2.1% with CD
higher prevalence in males than females
Adolescent Disorder Course
For ADHD, prevalence declines in adolescence
ADHD persists from childhood to adulthood in 50-65% of individuals
ODD onset usually 2-3 years, CD late childhood or early adolescence
Half of children with ODD/CD continue into problematic adulthood
Aetiology of Externalising Disorders
Genetic risk
High heritability
Genes contribute less to ODD than ADHD, some indication in CD
Temperamental Risk
Difficult temperament (emotion regulation - high reactivity)
Neurobiological risk
ADHD
structure: delayed brain maturation, less activity
Function: selective deficiency in neurotransmitters
CD: structural and functional differences in areas associated with affect regulation and affect processing
Parenting factors
ADHD: smoking, neurotoxin, or alcohol exposure in utero
ODD: harsh, inconsistent, or neglectful parenting
CD: as above, maltreatment, lack of supervision, psychopathology
Psychological factors
Lack of self-control
Delay of gratification
Peers, neighbourhoods, and media
Treatment of ADHD (Per age group)
Preschool (4-5 years)
first line treatment = behavioural interventions
only prescribe stimulants if no significant improvements + moderate-severe impairment
Primary school (6-11 years)
apprroved medication and/or behavioural interventions - preferably both - stimulant medication usually tied first
Adolescence (12-18 years)
first line treatment = approved medication
may include behavioural interventions
Pharmocolgical Treatment of ADHD
Psychostimulants
increase norepinephrine and dopamine levels in brain
side effects: decreased appetite, increase HR, sleeping difficulties, unmask motor tics
Non-stimulants
SSRI - antidepressants
SNRI - slective norepinephrine reuptake inhibitor
Alpha-agonists
increase serotonin levels in brain
Behavioural Treatment of ADHD
Parent education, training and support to manage ADHD symptoms
Triple P - positive parenting program, PCIT, incredible years
streategies to strengthen relationship, improve communication, promote development
Classroom accomodations
Organisational supports
Personal Treatment of ADHD
Learn coping skills
make mental info physical bc of lack of working memory (reminders, to-do)
Make time physical (clocks, alarm, etc.)
break up lengthy tasks
Make motivation external (immediate reinforcements/consequences, rewards)
Moke problem solving manual (no mental manipulation, ex math tasks)
Refill self-regulation fuel task (rewards), self-statement, regular breaks, relaxation, meditation, physical exercise, sugar
Behavioural Treatment of ODD/CD
Evidence-based parenting support (triple P, incredible years, PCIT)
focus on family interactions
build parent-self regulations
develop relationships
clear expectation
increase appropriate prosocial behaviours
reduce inappropriate behaviours
Individual skills development (ex: anger management)
Multisystemic therapy (family, schools, peers, etc.)
Residential programs
Tailoring evidence-based parent support with First Nations communities
Pilot RCT
decrease in child behaviour concerns
improve parenting
reduction in barriers to mainstream services
National think tank
training to increase confidence via pre-accreditation workshops
dealing with logistical barriers + workplace support
peer networking
Practitioner support evluation
peer networking _ coaching → program sustainment 3 years later
implementaion consultants + first indigenous trainer
Remote community trial
38 local workers trained → positive training outcomes → positive family outcomes
Tailoring
community survey regarding parenting concerns → dvlp project scope
localise adaptations: names, images, delivery, locations, etc
Internalising Disorders Definition
Defines depressive and anxiety disorders same for children as adults
Depressive symptoms
show as irritability in children
in children/adolescents comorbid with externalising problems and anxiety
children have difficulty identifying anxiety, but aware of fears (age-appropriate usually)
Internalising Disorders Criteria [Depresive Symptoms]
Depressive Symptoms (5 or more during same 2-week period)
depressed mood (irritability)
diminished interest/pleasure
significant weight loss/gain
insomnia
psychomotor agitation/retardation
fatigue
feeling of worthlessness/inappropriate guilt
diminished ability to concentrate
recurrent thoughts of suicide
Internalising Disorders Criteria [Separation Anxiety Disorder]
Separation Anxiety Disorder
Developmentally inappropriate fear/anxiety concerning separation from home
Distress when anticipating seprations
Worry about losing/harm to attachment figure
Worry about experiencing untoward events (getting lost, being kidnapped, etc.)
Refusal to go out/sleep away from home/without attachment figure
Fear/reluctance about being alone
Nightmares with seperation themes
Internalising Disorders Criteria [Selective Mutism]
Selective Mutism
Consistent failure to speak in certain social situations
Speak to only a small number of people
Internalising Disorders Prevalence
In australia, among 6-17 year olds
3.2% diagnosed with MDD
6.9% diagnosed with anxiety disorders
Similar rates between males and females until age 12
Higher prevalence found in females than males between 12-17 years old
Internalising Disorders Course
Some internalising problems persist into adulthood
Linked to relationship difficulties, other anxiety disorders + mental health problems
Functional impairment in social and personal life
Childhood depression predicts six-fold increase in risk for suicide in young adults
Aetiology of interlising disorders
Biological Factors
few behavioural genetic studies conducted
some indication of heritability
predisposition to anxiousness
Social factors
experience of life stress, loss, or trauma / attachment issues
Parental overprotectiveness
maltreatment
Psychological factors
emotion regulation
rumination → future depression
caretaking children of depressed parents happy
Internalising Disorders Treatment
Depression
Psychotherapy
CBT
Family therapy
Antidepressent meds not effective as with adults
Anxiety
child focused CBT
family therapy interventions (ex: Fear-Less Triple P)
medication - SSRIs most common
CBT components - psychoeducation, emotion regulation, positive self-talk, in vivo exposure, contingency manegement
Neurodevelopmenta Disorder Definition
group of disorders with onset in developmental period, manifest early in development (before entering school); characteristics by developmnetal deficits in brain processes that produce impairments of personal, academic, or occupational functioning
Social Model Definition
Interaction between individual’s characteristics and an environment that creates physical, systemic, attitudinal, and social barriers for the individual
people disabled by environmnets not designed for them
shift towards changing systems, policies, and environments
Medical model definition
Deficit framing
Disability seen to be problem in indiivdual, not problem of society
that person needs to be fixed or cured
Social Model Definition
Group of neruodevelopmental differences that emerge during developmental period
differences typically become recognised early in development
characterised by diverse brain processes that may result in support needs, across personal, social, academic, or occupational contexts
particularly in environments that are not designed to accomodate the differences in the ways of thinking, learning, perceiving, and engaging with the world
Use of Language in Autism
Identify-first languge: autism is an integral part of their identity and who they are and consistently preferred by most autistic people
Shifts from medical model
supports should focus on environmnetal changes and on upskilling non-autistic, allistic, or neurotypical people
shift from terms like “disorder”, “imapirment”, “cure”, and “high/low functioning” pathologise autistic experiences
Neuroneutrality - Needs Focused Language
Moves away from deficit-based language on one end and superpower or romanticising language on other end
needs focused language allows meaningful conversations about access
Sharper Minds
has three SSPs (Student Staff partnerships) to co-produce and adapt components of the package
University simplified
co-designed with UQ neurodivergent student partners in 2025
Autism Criteria
Persistent deficits in social communication + social interaction across multiple contexts, manifested by all of the followig:
social-emotional reciprocity
nonverbal communicative behaviours
developing, maintaining, and understanding relationships
Restrictive, repetitive patterns of behaviour, interests or activities as manifested by at least two of the following:
stereotyped or repetitive motor movements
insistence on sameness (routines)
highly restricted, fixated interests
hyper or hypo-reactivity to sensory input
Must be present in early developmental period (may be masked/not fully manifested)
Symptoms cause clinically sig impairment on social, occupational, or important areas of current functioning
Not better explained by Intellectual disability or Global developmental delay
Specify if: with/without accompanying intellectual/language impairment, associated with known genetic/medical condition/severity of social commu impairments (requiring substantial support/substantial support/support)
Autism and Co-occuring neurodivergence
Most autistic people have one or more co-occuring conditions - these are not part of autism, but frequently present alongside it
Autism prevalence
Estimates 1 in 31 children aged 8 years are autistic
1 in 44 (2018) and 1 in 36 (2020)
Autism reported to occur in racial, ethnic, and socioeconomic groups
more prevalent among males, although debated
highest rates in 5-14 age group
20-24 age group more than doubled from 1.2% in 2015 and 2018 2.7% in 2022
youngest children are being identified
0-4 age group more than doubled from 0.4% in 2015 to 0.9% in 2022
Gender Differences in Autism
Autistic women more likely to be diagnosed at later stage
under-representation of autistic girls and women in research
interests towards topics relational in nature compared to males, who tend to be more mechanical in their interests
internalising difficulties (present as shy or anxious)
camouflaging
masking/double masking
Neurodiversity-affirming Pillars
Professional competency
three pillars:
social inclusion
economic inclusion
support services
ensure inclusion, safety, equitable access to opportunities, appropriate neurodiversity-affirming supports that recognise needs, strengths, and aspirations
Neurodiversity-addirming practices
Supports autistic identity
Adapts environment to suit their needs
incorporates autistic perspectives and therapeutic goals
aligns with their preferences and values
enhances autonomy
includes diagnostic assessment process
facilitates knowledge and self-acceptance
Neurodiversity-affirming Therapy
Emotion regulation is transdiagnostic → burnout prevention
modified CBT: big focus on affective education
energy banking: burnout management
withdrawal - energy depletion
deposit - energy boosters
Mindfulness-based therapy
Trauma-informed therapy
Parenting support and parents as co-therapists
Supports and/or medication for co-occuring mental health, medical health conditions, and disabilities
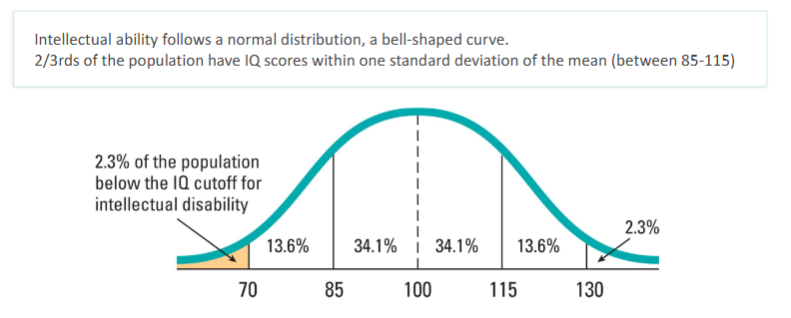
Intellectual Disability Criteria
Identified by significant limitations in both intellectual functioning and adaptive functioning
Intellectual and cognitive functioning required for diagnosis
Adaptive functioning required for classification
collection of conceptual, social, and practical skills
Age of onset is third element for diagnosis of ID
Explicit moved away from IQ scores alone to determine severity levels
Specify: severity in three domains based on behaviour (mild, moderate, severe, profund)
Intellectual Disability Specific Criteria
Intellectual functioning
IQ approximately 2 SD below mean (around 70), assessed using standardised tools
Adaptive behaviour
challenges in conceptual, social, and practical skills in everyday life
AB composite approximately 2 SD below mean
Developmental onset
Must originate before age 22
Intellectual Disability Prevalence
that about 450,000 people have an intellectual disability in Australia
Australian government released national roadmap for improving health of people with intellectual disability
Five assumptions (AAIDD)
Essential to applying the AAIDD definition in practice:
Limitations must be considered within context of community environments typical of the individual’s age peers and culture
Valid assessment considers cultural and linguistic diversity, and differences in communication, sensory, motor, and behavioural factors
Within an individual, limitations often coexist with strengths
Important purpose of describing limitations is to develop a profile of needed supports
With appropriated personalised supports over a sustained period, the life functioning of the person will generally improve
Intellectual Disability Aetiology
Chromosomal
Down syndrome - most common chromosomal cause
Genetic
Fragile X syndrome - commom inherited cause of ID
Phenylketonuria (PKU) - metabolic disorder, problems with eating high-protein, phenylalanine-rich foods
Prenatal infections
Rubella (German Measles)
HIV
Syphillis
Herpes simplex virus
Prenatal Toxin Exposure
Fetal alcohol syndrome - leading cause of ID
Environmental exposure: lead, mercury
Biological & Perinatal factors
Rh incompatibility between mother and infant
Premature birth
Low birth weight
anoxia/oxygen deprivation during birth
Pregnancy and birth complications
Postnatal infections
encephalitis - inflammation of brain
meningitis - inflammation of brain membranes
whooping cough
measles — cause brain damage if complicated
traumatic brain injury/neurological
head injuries
epilepsy and uncontrolled seizures
environmental toxin exposure
lead exposure
mercury expore
psychosocial and environmental
poverty + socioeconomic disadvantage
severe malnutrition in early infancy
environment lacking stimulation and responsiveness
early childhood neglect
limited access to intervention and healthcare
AAIIDD take on classifying ID (trad vs modern)
Traditional vs Modern approach
IQ score as primary classifier vs Support needs as primary focus
IQ: mild (50/55-70), moderate (35/40-50/55), severe (20/25-35/40), profound (<20-25)
deficit-focused and static, limited contextual consideration, heavily reliant on single test score
support: multidimensional - iq, adaptive behaviour, health, participation, context
adaptive behaviour composite score preferred for classification as it reflects real world functioning
purposeful and person-centred, aligned with social model of disability
ID Medical vs Social Model
Medical Model vs Social Model
Focus: deficit/impairment vs human functioning/env context
Language: disorder/cure/severity/impairment vs difference/support/needs/strengths
Classification: IQ Bands (mild, moderate, severe, profound) vs Support levels (requiring, substantial, very substantial support)
Goal: fix/normalise ind vs enhance QoL thru tailored supports
Env: individual adapt to env vs enc adapt to individual
AAIDD Five Dimensions
Intellectual Abilities: reasoning, problem-solving, learning, abstract thinking
Adaptive Behavior: conceptual, social, practical everyday skills
Health: physical, mental, and social well-being
Participation: involvement in home, work, school, leisure, community
Context: personal and env factors including culture and opportunities
AAIDD Systems of Supports
Resources and strategies that promote development and interests of person and enhance individual functioning and personal well0being
Person-centred, comprehensive, coordinated, outcome-oriented
Values and support relationships
Promote autonomy and choice (incorporate choice and inclusivity)
Align to personal goals and support needs (built aroundd individual goals, preferences)
Examples:
Family, friends, support workers
Professional support
Technological
Easy Read Info Guide
Adapt env to meet needs
Opportunities
Assessment process: intellectual functioning
Typically measured with individually administered and psychometrically valid, comprehensive, and culturally approrpiate tests of intelligence
Wechsler Intelligence Scale for Children Indices
Verbal Comprehension
Visual spatial
Fluid reasoning
Working memory
Processing speed
Testing identifies areas of relative strengths and weaknesses: ssist academic and vocational planning
IQ test scores, may be insufficient to assess reasoning in real-life situations and mastery of life skills
Factors affecting IQ scores
Practice effect (learning from repeated testing)
Flynn effect (overly high scores due to out of date norms)
Use of brief intelligence screening tests or group tests
Discrepant individual subtest score makes overall IQ score invalid
May not be normed for individual’s sociocultural background or native language
Co-occuring conditions that affect communication, language, and or motor function
Assessment process: Adaptive Functioning
Confirmed by both standardised measures (ABAS, VABS)
require additional sources of info
educational
dvlp
medical history
parent report
Factors affecting AD composite scores
Respondent related bias (who provides info)
Behavior may vary across home, school, community
Opportunity to perform the skills or level of support provided
Cultural context
Supportive and Effective engagement practices
Accessible communication (short, simple sentences, avoid jargon, one question at a time)
Respect & Dignity (speak directly, ensure inclusivity and respect)
Time & Patience (time for processing and responsing)
Visual Supports (use images, diagrams, etc)
Build Rapport (schedule consistent times for interaction)
Environmental Considerations (minimise distractions and noise)
Working with Adults with ID
Language needs to be adapted, reduce anxiety and put person at ease (humor)
provide more encouragement and more direct teaching of the tasks where needed
aim to facilitate person doing their best
Therapy
provide respect and listen well
common referral reasons (feeling sad and not being able to process that emotion)
important considerations (level of language that person hs both when talking to them and providing information/handouts)
Picture Exchange Communiation Systems (PECS)
Each card can be stuck on with velcro dots
Can create cards with FIRST and THEN
Eating Disorder Prevalence
Any ED
0.74-2.2% of males
2.58-8.4% of females
peak age of onet 15-17
Study found
Many ED risk factors present by early adolescence
Body dissatisfaction (13/15 → predict ED at 21)
Perceived pressure to be thin (14 → predict ED at 21)
Thin-ideal internalisation (14 → predict ED at 21)
Dieting (14 → predict ED at 21)
Negative Affect (14 → predict EF at 21)
suggests 14 as ideal age to do prevention
In austrlia, 4-16% of australian popul have eating disorder
by 14, 1.2% of males, 8.5% of females
by 20, 2.9% of males and 15.2% of females
binge eating disorder most common (esp with females)
anorexia typical onset 19-19 years more common with females
bulimia onset late adolescence/early 20s, more common with females
Eating Disorder Comorbidities
If have eating disorder, also have chances of
Anxiety disorders up to 62%
generalised anxiety - genetic link + excessive exercise/low BMI
social anxiety - highest BN, then BED, then AN-BP
OCD - rates are variable amongst ED
Mood disorders up to 54%
MDD has strong relationship
Bipolar has mixed reports from 1.9% up to 35.8%
Personality disorder sig higher in ED
Substance use or PTSD up to 27%
Substance use higher in ED
Psychosis + Schizophrenia has limited research
Body dysmophia have vairable prevalence
ADHD twice greater with ED
Autism higher prevalence
PTSD around 16-32% across all eating disorders
Suicide leading causes of death for those with ED
self-harm common with 1/3 of those with EDs