Schizophrenia
1/20
Earn XP
Description and Tags
lecture 8
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
21 Terms
how many people does schizophrenia effect
1 in 300
24 million globally
m:f ratio is 1.4:1
age of schizophrenia onset
15-25 in males
25-25 in females
schizophrenia symptoms
Positive symptoms (gaining something)
hallucinations
delusions
disorganises speech
negative symptoms:
anhedonia → loss of pleasure
reduced motivation
reduced emotional state
cognitive symptoms
memory issues
inability to process social cues
impaired sensory perception
diagnosis of schizophrenia
DSM-5 criteria
2 or more symptims for a significant amount of time across a month period
must include one of:
delusions
hallucinations
disorganised speech
can also include:
disorganised/catatonic behaviour
negative symptoms
impaired function at work, interpersonal relations or self care
patients present differently
burden of schizophrenia
less common than depression, anxiety and BPD
high burden of diesase → many years with disability and around 20 years earlier death
genetic cause of schizophrenia
50% heritability in twins → not fully genetic
likely polygenetic and environmental factors
DISC1 gene is disrupted
expressed on post-synaptic excitatory synapses to regulate form and function
mutations identified and implicates a risk factor of psychiactric illness
Environmental risk factors for schiziphrenia
pre and preinatal
maternal infection
maternal nutrition → eg. famine
maternal stress
delivery complications
neglect
traffic-related air pollution
adolescence
migration → even higher in traumatic migration (eg, refuge, higher in men than women)
social isolation
stress
recreational drug use
highest for cannabis → onset in first few years of use
some link for alcohol and other substances
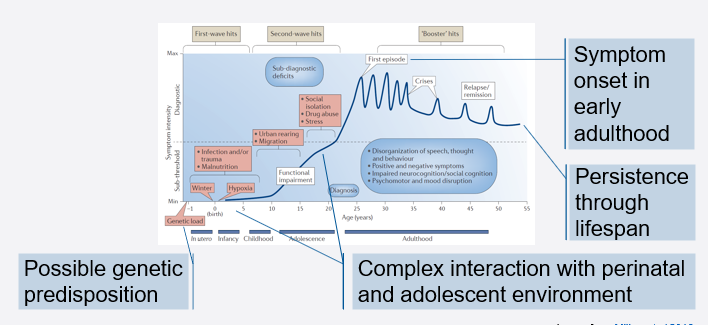
developmental timecourse of schizophrenia
possible genetic predisposition
complex interraction with perinatal and adolescent environment
symptems onset in early adulthood
persists through lifespan
possible higher risk of neurodegenerative diseases
dopamine hypothesis for schizophrenia
Positive symptoms → hyperactivity of D2 receptors in subcorticol and limbic regions
Negative and cognitive symptoms → hypofunction of d1 receptors in PFC
all current treatment uses this hypothesis except for xanomeline-tropsium (muscarinic agonist and peripheral antagonist)
dopamine pathways in schizophrenia
mesolimbic pathway
VTA → nucleus accumbens
reward
overactivity → positive symptoms
reduced by D2 antagonists
mesocortical pathway
VTA → PFC
underactivity → negative symptoms
exacerbated by D2 antagonisys, so use D1 positive allosteric modulators (PAM)
Niagrostriatal pathway
substantia nigra → striatum
movement
D2 antagonists cause extramyramidal parkinson-like movement disorder → bradykinesia, akinesia, termor
Tuberoinfundibular pathway
hypothalamus → anterior pitutiary
inhibits prolactin
D2 antagonists elevates prolactin and causes undesired lactation in women
Schizophrenia treatments based on the dopamine hypothesis
First generation antipsychotics (FGA)
haloperidol, chlorpromazine
D2 antagonists, reduce positive symptoms but not negative or cognitive symptoms
induce extrapyramidal side effects → poor patient compliance
Second generation antypsychotics (SGA)
clozapine, olanzaoine
D2 antagonists but also blocks D3, D4, mACh, 5-HT2A and 5-HT6
less extrapyramidal sife effects but weight gain and type 2 diabetes
no more effective than FGA (CATIE 2005 trial)
Third generation antipsychotics
aripiprazole, cariprazine
D2 and D3 partial agonists
slightly better
few extrapyramidal side effects
small effect on negative and cognitive symptoms
Brilaroxazine
D2-4, 5-HT1A,2A,6 and 7, nACha4 and b2, SERT
recent phase III trial
soon to seek approval
support for dopamine hypothesis of schizophrenia
Pharmacological:
amphetamines → inhibit DA uptake
cause psychosis in healthy induviduals
worsens symptoms in schizo patients
effective antyosychotic doses correlate with D2 occupancy
post-mortem
elevated dopamine, DA metabolites and D2 receptors in striatum
measures are in patients who have been treated → changes could be caused by this
PET
little change in transporters and receptors in treatment naive patients
increased basal dopamine in striatum
decreased basal dopamine in PFC
scanning using raclopride (binds to D2) and amphetamine shows increased mesolimbic dopamine release in schizo patients
genome wide association studies (GWAS)
single nucleotide polymorphisms (SNPs) at 287 genetic loci associated with schizo
impacts COMT gene → decreases dopamine metabolism
impacts D2 receptor locus
impacts postsynaptic kinases doenstream of DA receptors
limitations of dopamine hypothesis for schizophrenia
inconsistent findings for several risk factors → COMT, presynaptic DA regulators and vesicular storage
Risk genes like DISC1 are in DA and glutamatergic signalling
unclear mechanism of dopamine dysfunction
aound 30% of patients unresponsive to DA medication
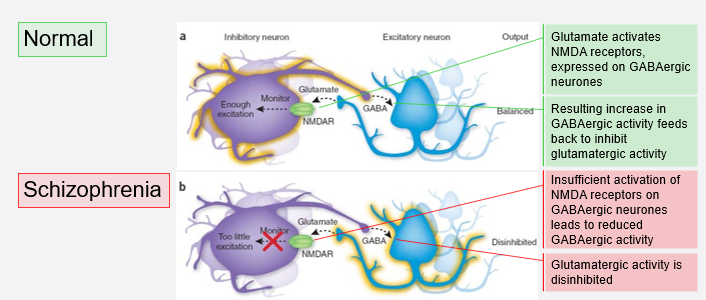
Glutamate or excitation/inhibition imbalance hypothesis
in a normal person:
glutamate activates NMDA receptors on GABAergic neurones
increases GABAergic activity
inhibits glutamatergic activity
in schizophrenia:
not enough NMDA activation on GABAergic neurones
decreased GABAergic activity
disinhibition of glutamatergic activity → more active, cytotoxicity
support for excitation/inhibition imbalance hypothesis of schizophrenia
Pharmacological
NMDA receptor antagonists (ketamine or PCP) causes psychosis on healthy individuals
Post-mortem
loss of GABAergic markers in PFC and hippocampus (inc GABA synthesis enzyme, uptake transporter and Ca2+ binding proteins)
increased endogenous NMDA receptor antagonist NAAG → binds to glycine site on NMDA
decreased inhibitory annd increased excitatory hippocampal synapses
Magnetic resonance spectroscopy (MRS)*
decreased glutamate, GABA and glutathione in anterior cingulate cortex
PET*
reduced NMDA receptors in hippocampus
* imaging studies on small cohorts not balanced for confounding variables or are stratified by a predominant symptom
clinical trials of drugs based on excitation/inhibition imbalance hypothesis of schizophrenia
none have been successfull yet
all work on glutamatergic mechanisms
eg. NMDA agonists and glutamate agonists
Evidence for the inflammatory hypothesis of schizophrenia
major histocompatability locus (chromosome 6) has highest association with schizo
encodes genes involved in immunity
patients have elevated cytokines in blood
envrionmental risks have links to inflammation → eg pollution
inflammatory comorbidity → 19% of schizo patients have IBS
stress and maternal immune activation increase risk by altering microglial function
can have autoantibodies against NMDA receptors
treatments based on the inflammatory hypothesis of schizophrenia
minocycline → antibiotic
inhibits microglial activation
Celecoxib → non-steroidal anti-inflammatory (NSAID)
some promising results
patient stratification needed for future trials → need to understand pateint genetics and history
plasma and imaging markers to identify likely responders
personalised medicine
Synaptic hypothesis of schizophrenia
version 1
fienberg, 1982
too many or too few or wrong synapses eliminated in adolescence
version 2
keshavan, 1994
excessive cortical pruning and insufficient subcortical pruning
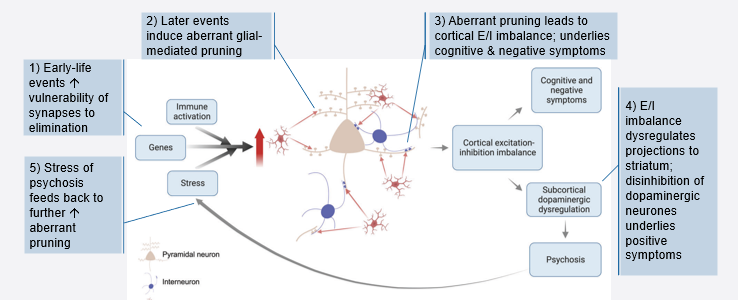
version 3 → intergrated hypothesis
howes and onwordi, 2023
genetic and environmental risks leading to abberant glial-mediated synaptic pruning
Intergrated hypothesis of schizophrenia
strengths, gaps and future directions of the integrated hypothesis of schizophrenia
strengths
basis to develop disease modifying agents not just symptom relief
gaps and future directions
synaptic loss alone doesnt account for all grey matter volume loss → also change in dendritic spine density, need imaging and marker studies
do synaptic alterations occur in the first episode of psychosis or earlier → need PET studies on high risk unmedicated individuals
does loss affect specific synapse types → need multimodal imaging ( eg. MRI and PET)
can SV2A (presynaptic protein) alterations be confirmed at a protein level post-mortem → relationship between SV2A and other synaptic markers