Lecture 13: High risk neonates
1/110
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
111 Terms
Level 1 care: Well newborn nursery
Care for infants ≥ 35 weeks and stabilize infants < 35 weeks for who are ill for transport to a higher level facility
Level 2 care: Special care nursery
Care for infants ≥ 32 weeks and ≥ 1500 g
Transitional care after NICU
Provide ventilation/CPAP for < 24 hrs
Stabilize infants who are ill for transport
Level 3: NICU
Provide sustained life support for infants < 32 weeks for <1500 g
full range of respiratory support, including high-frequency ventilation and inhaled NO
readily accessible to many specialists
Level 4: Regional NICU
Located within institution able to perform complex surgical care
Full range of specialists
Facilitate transport
Activation of stress response cascade (7 steps)
HPA axis activated
Cortisol
Inflammatory cascade
Free radicals
Oxidative stress
Cellular injury
Disease
When is the most important time for brain development?
3rd trimester
Late preterm
34-37 weeks gestation
Moderately preterm
32-34 weeks gestation
Very preterm
28-32 weeks gestation
Extremely preterm
< 28 weeks gestation
Periviable birth
Somewhat viable birth
20 0/7 weeks to 25 6/7 weeks
Prematurity primary concerns
Poor Thermoregulation
RDS
Intraventricular hemorrhage
Patent Ductus Arteriosus
Necrotizing enterocolitis (NEC)
Nutrition, growth, and feeding
Preterm babies: Thermoregulation
Thin epithelium + large SA = more loss of heat
hypothermia increases mortality in preterm infants
How can we prevent hypothermia is preterm babies? (4)
Hats
Polyethylene bags (helps with insensible water loss)
Radiant warmer
Increase room temp
Preterm babies: Respiratory Distress Syndrome
development of the bronchi and terminal bronchips occurs by 17 weeks, but 17-26 weeks is a critical time for alvioli development
Surfactant
substance that reduces the surface tension of an air/liquid interface within the alveoli in the lung — keeps lungs from collapsing
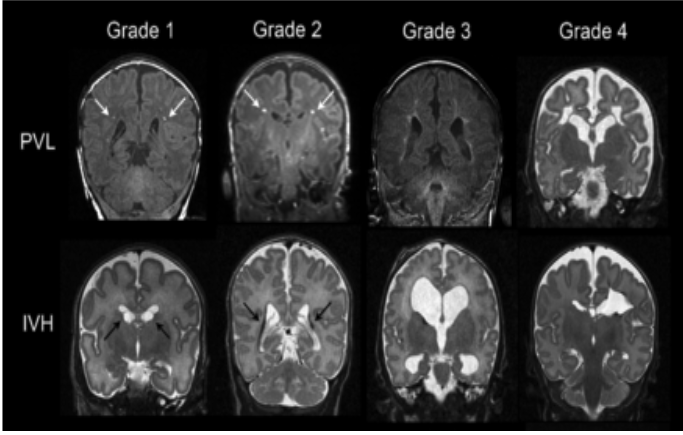
Intraventricular hemorrhage (IVH)
geminal maxtric is a highly vascularized area of the brain that is prone to bleeding, especially in premies
Grades of IVH (4)
Grade 1: isolated germinal matrix
Grade 2: bleeding into ventricle without dilation
Grade 3: bleeding into ventricle with dilation
Grade 4: Involves the parenchyma of brain
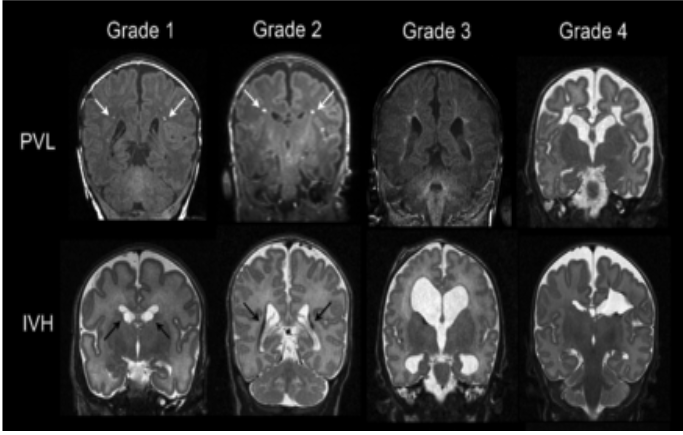
Periventricular leukomalacia (PVL)
necrosis and softening of white matter near the brain's ventricles, which can contribute to neurodevelopmental delays and other brain complications
most common in premies
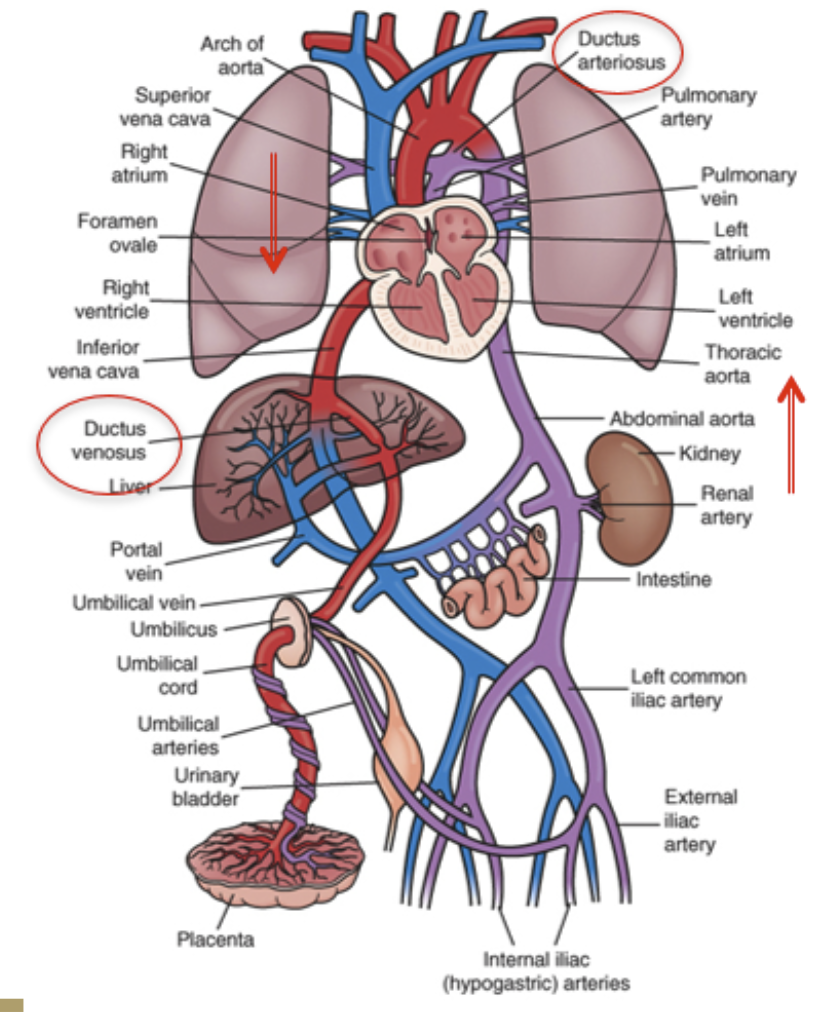
Ductus venosus transitional circulation
Birth
Umbilical cord clamped
SVR rises
ductus venosus closes from lack of BF from placenta
PVR falls
Functional closure of PFO bc left side pressure > right
Functional closure of PDA bc removal of prostaglandins (produced by placenta) and increased O2 levels
What is the result of exposure of O2 to the lungs?
Functional closure of PFO bc left side pressure > right
Functional closure of PDA bc removal of prostaglandins (produced by placenta) and increased O2 levels
PVR falls
Functional closure of PFO bc left side pressure > right
Functional closure of PDA bc removal of prostaglandins (produced by placenta) and increased O2 levels
Patent ductus arteriosis
congenital heart defect where the ductus arteriosus doesn’t close after birth
Why are infants in respiratory distress (esp. preterm) at risk for PDA not closing?
due to the infant not being able to fully use lungs and intake O2
Necrotizing Enterocolitis
where intestinal tissue becomes inflamed, dies, and can lead to perforations, severe infection, and high mortality rates
most common in premies
Factors predisposing to NEC
Genetic
Characteristics of the immature fetal intestine
altered microbiota
inadequate intestinal barrier function
excessive inflammatory response
NEC signs and symptoms
Abd distension d/t intestinal pneumatosis and pneumoperitoneum
Loopy bowel
Signs of infant lethargy
Feeding intolerance
Hematologic: low platelets
Metabolic: hyponatremia, hyperkalemia, acidemia
NEC etiology (5)
Hypoxic insult
Enteral feedings
Sepsis
Microbiome
Inflammatory mediators
NEC prevention (3)
BM feeding
Prevent preterm birth
Infection prevention
NEC treatment
Bowel resection
Triple abx
NPO
Wall suction to decompress bowel
Serial xrays to track bowel progression/health
Slow reintroduction of PO
When does coordination of suck, swallow, and breath develop?
32 weeks gestation
What is the goal of feeding for a premie?
Feeding is can exercise — goal is to expend as little energy as possible
How can we help premies expend as little energy as possible when feeding?
Cue-based feeding
Slow flow bottle nipple
Side-lying position
Late preterm infant
34-37 weeks gestation
When can late preterm infants often be discharged (early side)?
2-5 days after birth
What are late preterm infants are at risk for? (5)
Poor feeding
Hyperbilirubinemia (can’t break down RBCs yet)
Hypoglycemia
Hypothermia
Infection
Post-maturity
>42 weeks gestation
Post-maturity risks
Uteroplacental insufficiency
Meconium aspiration
Post-maturity placental insufficiency
this occurs because placental is really only supposed to last 40 weeks
causes hypoxia before and/or during labor, leading to:
poor resp. effort after birth
hypoglycemia
mec aspiration
hypoxic ischemic encephalopathy
Post-maturity meconium aspiration
with perinatal stress or post-maturity, there is often the passage of meconium before/during/immediatley after delivery and can be aspirated into lungs
This is our biggest concern with post-mature babies bc it can cause respiratory distress!
Pulmonary HTN
BVs of baby’s lungs don’t open, leading to a hypertensive state in pulmonary vasculature — too much blood bypasses the lungs so O2 can’t get into blood, leading to a low O2 state for brain and body
most common cause is meconium aspiration
Small for gestational age (SGA)
defined as weight <10th percentile for weeks of gestation
Symmetric SGA
both head circumference and weight are below threshold
Asymmetric SGA
weight below threshold, but head circumference WNL
better outcomes bc brain is fully developed
What may SGA indicate?
Poor placental function
Inherent abnormality of fetus (e.g., genetic disorders)
What are SGA infants at risk for?
Asphyxia
Cold stress
Hypoglycemia
Polycythemia
What are SGA infant at risk for long-term?
poor neurodevelopmental outcomes
Large for Gestational Age (LGA)
>90rh percentile for gestational age
Risk factors for LGA
Diabetic mothers
Large parents
What are LGA infants at increased risk for? (3)
Birth trauma
Asphyxia
Hypoglycemia
Neonatal hypoglycemia treatment (3)
Feeding
Glucose gel
IV glucose
Most common type of birth injury
clavicular fracture
bc of shoulder dystocia
Types of birth trauma: skeletal injuries (4)
Skull
Clavicular
Humerus
Femur
Types of birth trauma: peripheral NS injuries (2)
Brachial plexus injuries
Facial palsies
Types of birth trauma: CNS (4)
Intracranial hemorrhage
Hypoxic ischemic encephalopathy
Spinal cord injuries
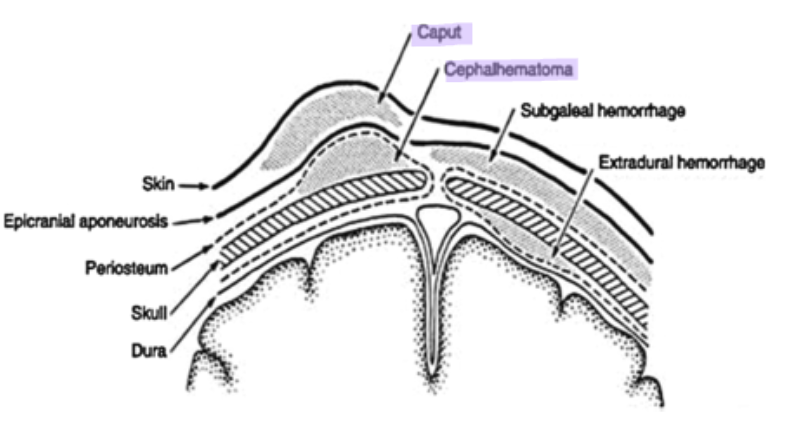
Cephalohematoma vs Caput Succedaneum
Cephalohematoma: collection of blood below the periosteum and does not cross the periosteum
dewveops over 24 hrs
Caput: collection of blood above periosteum and crosses suture lines
present at birth
What types of vaccines can be given during pregnancy?
only inactivated vaccines
TORCH infections
group of infectious diseases transmitted from a pregnant person to a fetus or newborn, causing severe congenital anomalies, stillbirth, or developmental issues
Toxoplasmosis
Other (syphilis)
Rubella
Cytomegalovirus
Herpes
If mom is Group B Strep (GBS) positive, how long after contraction will the baby show the illness?
1 week
GBS s/s in mother
Fever
GBS bacteruria
Preterm delivery
Prolonged ROM (>18 hrs)
GBC s/s in infants (7)
Lethargy
Poor feeding
Resp difficulties
Tachypnea
Grunting
Hypoxia
Possible fever
GBS late onset in an infant
7-89 days of life and typically presents with meningitis
needs a sepsis work-up
Toxoplasmosis transmission (2)
Undercooked or raw meat/shellfish
Cat feces
Congenital toxoplasmosis fetal complications
Visual and hearing impairment
Learning disabilities
Intellectual disabilities
Syphilis transmission
skin and mucocutaneous exposure
Syphilis fetal complications
Still birth
Hydrops fetalis
Preterm birth
Syphilis complications at birth up to 8 weeks after birth
Hepatosplenomegaly
Mucocutaneoius lesions
Pneumonia
Osteochondritis
Hemolytic anemia
Thrombocytopenia
Late infant manifestations of syphilis (2)
Vision impairment
Abnormalities in bone, joints, teeth, and skin
Syphilis treatment
penicillin
Rubella transmission
transmitted through direct or droplet contamination from nasopharyngeal secretions
Congenital Rubella syndrome may result in… (4)
Fetal death
Congenital anomolies with eyes or heart
Hearing loss
Neurological abnormalities
Rubella vaccine and pregnancy
Rubella vaccine is a LIVE vaccine, so it CANNOT be given during pregnancy
must be given before or immediately after delivery
Cytomegalovirus (CMV) transmission
Transplacental (most concerning)
During birth (contact with secretions)
Postnatally via breast milk or saliva/urine
*Women at highest risk for transmission are those exposed to saliva or urine of young children
CMV infant risks
Hearing loss
Vision loss
Intellectual disability
Microcephaly
Seizures
Herpes Simplex Virus (HSV) neonatal consequences
Presents with:
cutaneous lesions
Opthalamic involvement
Neurological involvement
High mortality with infection
HSV transmission prevention
avoidance of vag delivery with an active infection
How can HIV be transmitted from mother to infant?
During pregnancy, intrapartum (labor/delivery), and postpartum (breastfeeding)
How does HIV transmission occur during pregnancy?
Transplacental (hematogenous) or ascending infection from genital tract to amniotic fluid/membranes
How does intrapartum HIV transmission occur?
Mucocutaneous contact with maternal blood, amniotic fluid, or genital secretions
What medication reduces transmission during labor in high viral load?
IV Zidovudine intrapartum
What is given to the infant after being born to a mother with HIV?
Antiretroviral prophylaxis for 4–6 weeks
Neonatal Abstinence Syndrome (NAS)
is withdrawal in a newborn after in-utero exposure to opioids
When is NAS present?
2-3 days after birth
NAS s/s (3)
Tremors
Hypertonic
Inability to eat, sleep, or be consoled
NAs treatment
Weaned off over days to weeks of these drugs:
Methadone
Morphine
Nuprenorphine
Clonidine
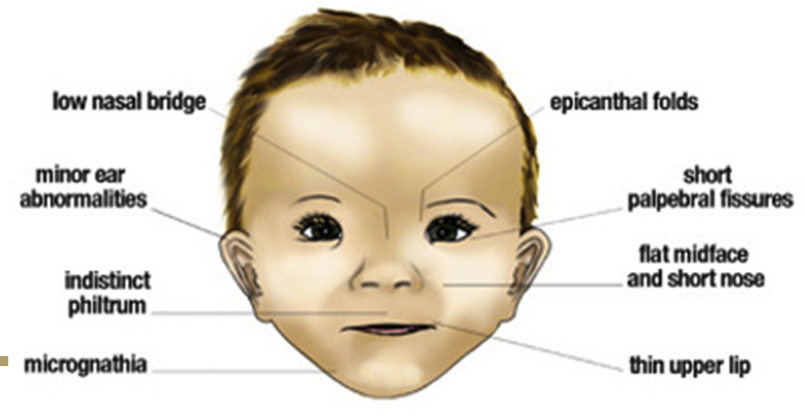
Fetal Alcohol Syndrome
caused by alcohol exposure during pregnancy, leading to permanent physical, neurologic, and developmental abnormalities
dose-dependent
Hemolytic Disorders: Rh/ABO incombatability (mom Rh- and baby Rh+)
Fetal RBCs are destroyed by maternal antibpodies
anemia and hydrops (extreme edema)
Erythroblastosis fetalis (hemolytic disease of newborn)
Rhogam
prevents mom from developing anti-Rh antibodies
needs to be given anytime risk for maternal-fetal transfusion
Hyperbilirubinemia
elevated bilirubin level in the blood leading to jaundice in newborns
Hyperbilirubinemia causes
Anything that increases rate of RBC breakdown (infection, prematurity, caput, cephalohematoma)
Liver dysfunction
Hypoalbuminemia
Poor GI function
G6PD deficiency — causes hemolytic anemia
Kernicterus
a severe, permanent brain injury caused by very high levels of unconjugated bilirubin crossing the blood–brain barrier in a newborn
preventable and considered a “never event”
Vetricular septal defect (VSD)
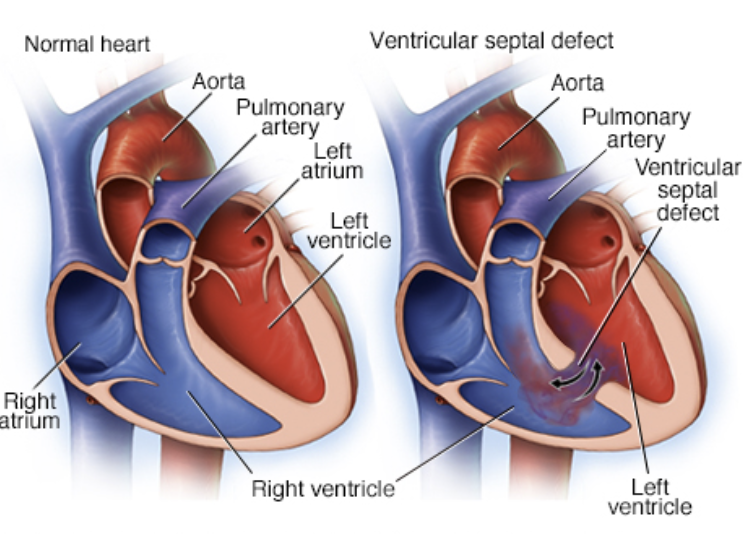
Is blood flow to lungs increased or decreased in VSD?
decreased bc bypassing defect in ventricle
O2 stats will be lower
Coartation of the Aorta
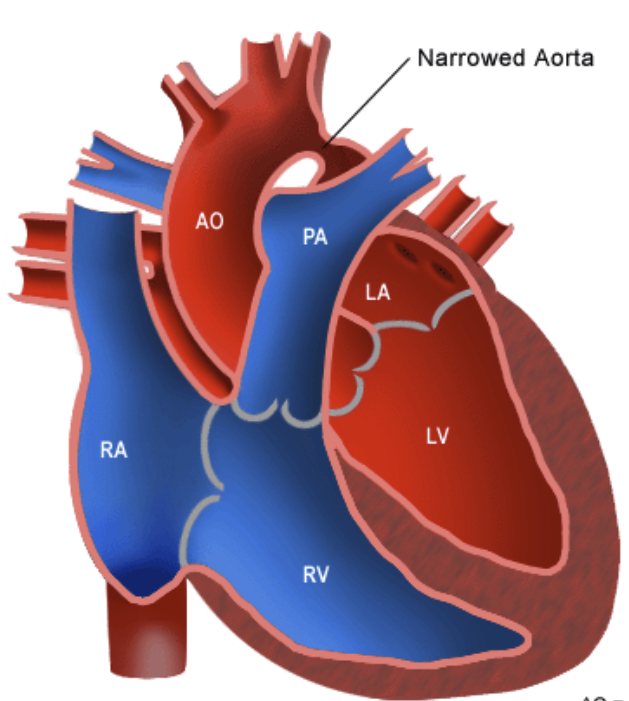
If a baby has a severe coarctation, they will be…
very blue
Tetralogy of Fallot
4 defects:
Large VSD
Overriding aorta that straddles VSD
Pulmonary stenosis
RV hypertrophy
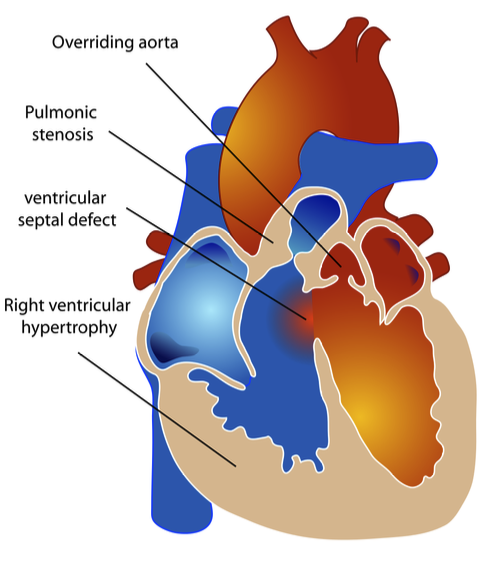
Tet spell and treatment
Acute cynaotic event that can be semi-treated by bringing knees ti chest to increased systemic vascular resistance
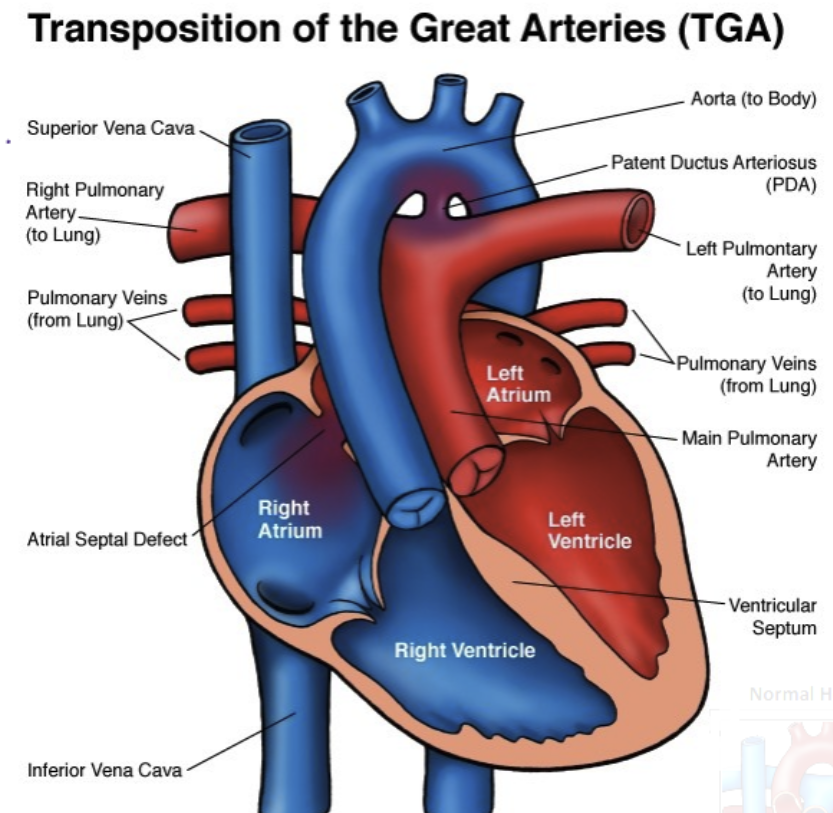
Transposition of the Great Arteries
Aorta and pulmonary arteries are switched
Cleft lip and palate risk factors
Alc
Smoking
Diabetes
Epilepsy meds
Primary concern of cleft lip/palate
feeding bc baby cannot create a seal
nasopharyngeal reflux (milk will come out of nose)
Cleft lip/palate special bottle
long nipple to get past cleft palate