POM 3 Geriatrics: chronic disease
1/60
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
61 Terms
what are the 4 Ms of age-friendly care?
what matters, medication, mind, mobility
incidence of hypertension
2/3+ of adults 65 and up
What are the 2 key geriatric groups at risk for HTN?
females and black patients
black patient's HTN characteristics
earlier onset, more severe cases, less controlled
leading etiology of HTN
arterial stiffness
lifestyle factors for HTN
smoking, ETOH, obesity
clinical presentation of HTN
most asymptomatic; dizziness, palpitations, headache, end organ damage, stroke, HF, renal failure, new onset A-fib
diagnostic workup of HTN
CBC, BMP, lipid panel, TSH, UA
ECG, home BP log, orthostatic readings
complications of HTN
CAD, CVA, CHF, LVH, arrhythmia, cognitive impairment, vascular dementia, CKD
risks of overtreating HTN in elderly
orthostatic hypotension, medication side effects
What BP is associated with increased mortality in elderly patients being treated for HTN?
<110/60
ACC/AHA guidelines for starting treatment for HTN in 65 years or older
start drug therapy for systolic >130; no diastolic threshold
incidence of T2DM
29% with DM in geriatric population
clinical presentation of T2DM
asymptomatic, hyperglycemia, increased adiposity, complications
What are the complications of T2DM in elderly?
micro/macrovascular issues, increased ASCVD, functional disability, depression, falls, incontinence, cognitive impairment, hypoglycemia
diagnosis of T2DM
A1C, fasting plasma glucose, random plasma glucose
What should be monitored in T2DM?
cholesterol, liver, BP, eyes, kidneys, feet
goals for T2DM management in elderly
AIC <7%, if multiple comorbidities <8%, fasting flucose 90-130, avoid hypoglycemia
A 76-year-old patient with PMH of CHF has an A1C of 8.5%. He currently takes metoprolol, spironolactone, and metformin. Which of the following would be the most appropriate to add on to their regimen to control his diabetes?
a. glyburide
b. empaglifozin
c. basal insulin
d. semaglutide
b.
What is the key risk factor of COPD?
smoking
clinical presentation of COPD in elderly
chronic cough, dyspnea, diminished or distant breath sounds, hyperresonance, prolonged expiratory phase, expiratory wheezing, increased AP diameter
complications of COPD
respiratory infections, cardiac involvement, deconditioning, depression
COPD work-up
spirometry - reduced FEV1/FVC ratio (<0.7); CXR
FEV1 values for mild, moderate, severe, and very severe COPD
mild: >80%
moderate: 50-80%
severe: 30-50%
very severe: <30% or <50% plus chronic respiratory failure
COPD management
smoking cessation, inhalers (LAMA +/- LABAs daily, PRN SABAs, +/- ICS if severe, supplemental oxygen, pulmonary rehab
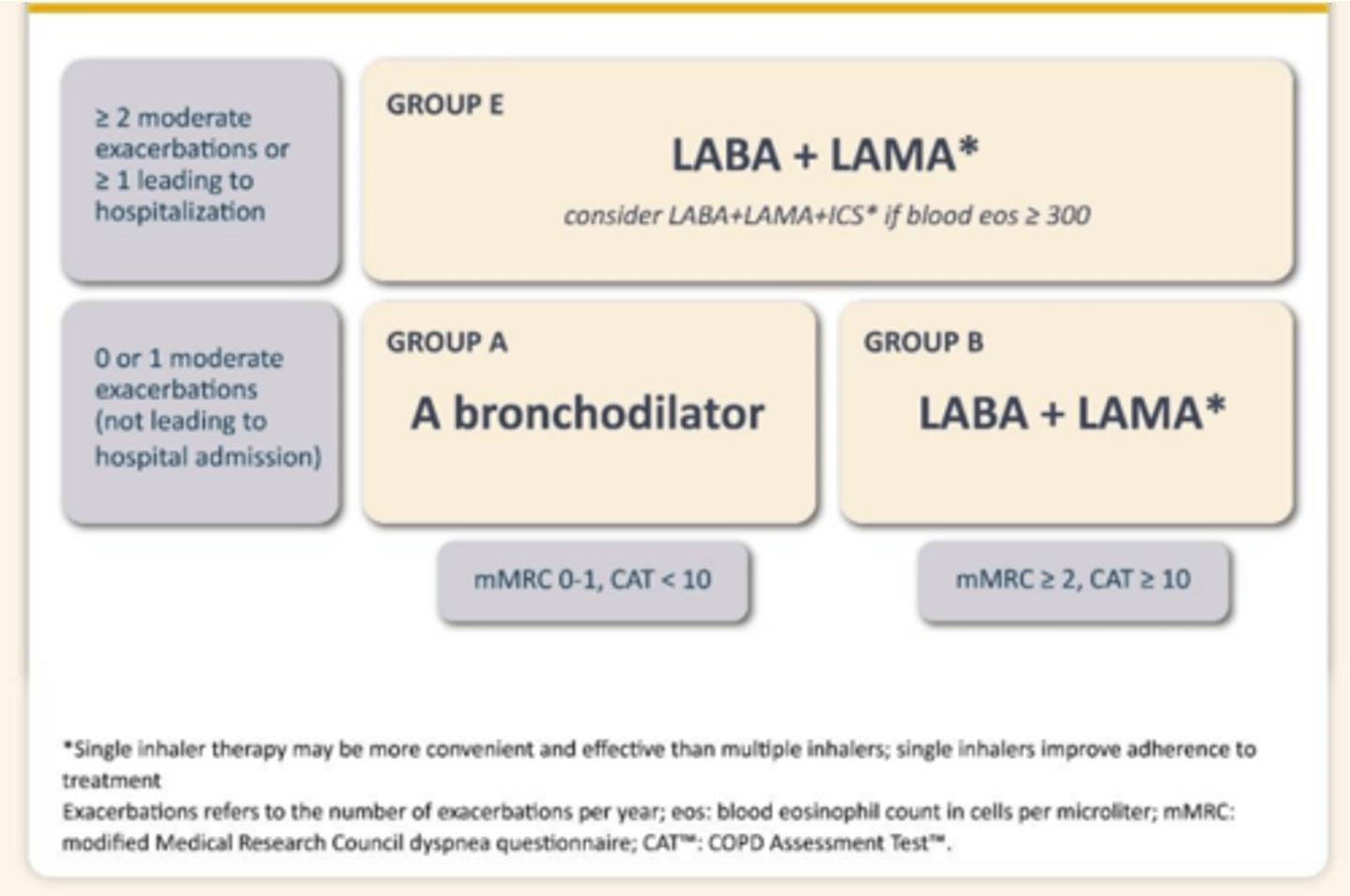
What is the alorithm for pharmacological treatment of COPD?
Group A (bronchodilator): 0-1 moderate exacerbations (not leading to hospitalization)
Group B (LABA + LAMA): mMRC 2 or more, CAT 10 or more; no hospitalizations
Group E (LABA + LAMA +/- ICS): if 2 or more exacerbations or 1 or more hospitalizations
CKD definition
reduced GFR or evidence of kidney damage for at least 3 months
risk factors for CKD
dibetes, HTN, ASCVD, CVA, obesity, family history, smoking, age, medications
clinical presentation of CKD
asymptomatic until advanced, then nonspecific
complications of CKD
fluid/electrolyet abnormalities, bone and mineral disease, anemia, poor nutrition
CKD workup
GFR < 60; UA/UACR, monitor BP, CBC, imaging
GFR categories for CKD
G1: >90
G2: 60-89
G3a: 45-59
G3b: 30-44
4: 15-29
5: <15
When should a patient be referred to nephrology?
stage 4
CKD management
advanced care planning, ACEI/ARB, SGLT2, dialysis, kidney transplant, palliative care for all patients
When is dialysis recommended?
GFR < 30
average age of patients with peripheral vascular disease
70
risks for carotid artery stenosis
male, age, smoking, family history
What is a AAA?
dilation of the abdominal aorta >50% (above 3.0 cm)
risk factors for AAA
smoking, male gender, age >65
What imaging is go to for AAA?
US first, CT
treatment of AAA
repair for large, observation if smaller
screening recommendations for AAA
patients 65 and up
complications of peripheral arterial disease
wound healing, disability, critical limb ischemia, critical limb threatening ischemia
Two main signs of peripheral arterial disesae
loss of hair, decreased temperature, discoloraiton of skin
PAD diagnostic workup
ABIs, imaging (US) then angiography for intervention, evaluate comorbidities
PVD management
local - minimally invasive - balloon, stenting
systemic: high dose statin, HTN management, smoking cessation, antiplatelet for more severe
70% of all cancer diagnoses will be in adults < age ______ by 2030.
65
most common cancer in US
breast cancer
risk factors for breast cancer
age, family history, genetics, dense breast tissue, diet, obesity, HRT
clinical presentation of breast cancer
lump, skin changes, nipple changes, LAD
incidence of colon cancer
4th most common, 4th leading cause of cancer mortality
risk factors for colon cancer
age, family history, weight, DMT2, red meat diet, smoking, alcohol, personal history of polyps
clinical presentation of colon cancer
change in bowel habits, rectal bleeding, blood in stool, abdominal pain
prognosis of colon cancer
individualized evaluation, prevention and early diagnosis key, surgical candidates have best prognosis
incidence of prostate cancer
2nd most common cancer, 3rd leading cuase of cancer mortality
risk factors for prostate cancer
age (men over 65), race/ethnicity (black patients with highest risk), family history, genetics
clinical presentation of prostate cancer
increased PSA, asymptomatic, urinary complaints, hematuria
incidence of lung cancer
3rd most common cancer, #1 leading cause of cancer mortality
risk factors of lung cancer
age (median age of diagnosis 70), smoking, secondhand smoke, exposure to radon or asbestos
clinical presentation of lung cancer
cough, dyspnea, chest pain, hemopytsis
prognosis of lung cancer
generally poor, worsens with age