AQA A Level Psychology - Psychopathology
1/64
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
65 Terms
Statistical infrequency
Occurs when an individual has a less common characteristic
Example of statistical infrequency
-Lower than average IQ, <70
-May be diagnosed with intellectual disability disorder
Statistical deviation evaluation
-Real life application - diagnosis of mental disorders
-Unusual characteristics may be positive - e.g. higher than average IQ
-Not everyone benefits from a label - lower than average IQ might be able to live normal life but label could negatively impact self esteem
Deviation from social norms
Concerns behaviour that is different from the accepted standards of behaviour in a community or society, specific to the culture we live in
Example of deviation from social norms
-Antisocial personality disorder
-Failure to conform to lawful or culturally normative ethical behaviour
-Person is abnormal because they do not conform
Deviation from social norms evaluation
-Real life application - diagnosis of disorders
-Never the sole reason - antisocial personality disorder also categorised by distress (failure to function)
-Cultural relativity - social norms depend on culture, can't apply to people from other groups
-Human rights abuses - defining people as abnormal to control them e.g. slaves who ran away
Failure to function adequately
When an individual is unable to cope with ordinary demands of day to day living, e.g. intellectual disability disorder
Rosenhan and Seligman's signs of not coping
-Lack of conformity to standard interpersonal rules - maintaining eye contact, respecting personal space
-Severe personal distres
-Dangerous and irrational behaviour to self and others
Failure to function evaluation
-Patient's perspective - considers individual's subjective experience, useful criteria
-May just be deviation from social norms - e.g. extreme sports, religion
Subjective judgement - difficult to judge distress
Deviation from ideal mental health
Occurs when an individual does not meet a set of criteria for good mental health
Jahoda's criteria for ideal mental health
-No symptoms or distress
-Rational behaviour, accurate self perception
-Self actualisation (reaching potential)
-Coping with stress
-Realistic world view
-Good self esteem, lack of guilt
-Independence
-Successful work, love and leisure
Deviation from ideal mental health evaluation
-Comprehensive - covers wide range of criteria
-Cultural relativity - self actualisation may not be as normal in other countries
-Unrealistically high standard for mental health - would see us all as deviant
Behavioural characteristics of OCD
-Compulsions
-Avoidance
OCD Compulsions
Repetitive behaviours motivated by obsession that reduce anxiety
Avoidance
Individual actively keeps away from triggering situations
Emotional characteristics of OCD
-Anxiety and distress
-Depression
-Guilt and disgust
Cognitive characteristics of OCD
-Obsessive thoughts - recurring unpleasant thoughts
-Cognitive strategies to cope - meditation, praying
-Excessive anxiety - hypervigilance
Genetic explanations for OCD
Genes made up of DNA make up chromosomes and code for the physical and psychological features of an organism. Genes are inherited from parents.
Lewis (1936)
37% of OCD patients shared it with their parents, 21% shared it with their siblings
Candidate genes
Genes identified that create vulnerability for OCD, e.g. 5HT1-D beta involved in transport of serotonin across synapses
Polygenic
OCD is caused by more than one gene
Taylor (2013) identified 230 that could be involved
Genetic explanations evaluation
-Twin studies - Nestadt (2010) 68% of identical twins share OCD as opposed to 31% of non-identical
-Too many candidate genes - little predictive value, difficult to pin down
-Environmental faote - Cromer (2007) found over half of patients had past trauma, those w/ multiple traumas had more severe OCD
Neural explanations for OCD
Physical and psychological characteristics are determined by the nervous system, in particular the brain and surrounding neurons
Serotonin
Neurotransmitter serotonin regulates mood
Low levels of serotonin = mood-relevant info not transmitted, mood is affected
Decision-making systems (where in the brain?)
-Decision-making associated w/ frontal lobe
-OCD associated w/ impaired frontal lobes
-Also associated w/ parahippocampal gyrus (processes unpleasant emotions)
Neural explanations evaluation
-Antidepressants reduce OCD - serotonin involved
-Associated w/ neurological disease Parkinson's
-No one system always causes it - can't claim neural systems are innvolved
-Abnormal functioning could be because of the OCD, not a cause of it
SSRIs + OCD
-Prevents re-absorption and breakdown, levels increase therefore post-synaptic neuron is stimulated
-e.g. Fluoxetine, typical dose 20mg a day
Combined OCD treatment
-Drugs used alongside CBT
-Drugs reduce anxiety etc, patient can engage w/ CBT effectively
Alternatives to SSRIs
-Tricyclics - same effect on serotonin system with more severe side effects
-SNRIs - serotonin-noradrenaline reuptake inhibitor, also increase noradrenaline levels
Drug therapy evaluation
-Effective - Soomro (2009) 17 studies comparing SSRIs and placebos all found that SSRIs improved symptoms
-Cost-effective and non-disruptive
-Side-effects - patients stop taking them
-Unreliable evidence from drug companies
-OCD can be caused by trauma - not biological
Behavioural characteristics of phobias
-Panic - crying, screaming
-Avoidance - conscious effort to keep away from stimulus
-Endurance - remaining in presence of stimulus while experiencing extreme anxiety
Emotional characteristics of phobias
-Anxiety - inability to relax or feel positive emotion, can be long term
-Unreasonable emotional responses that are disproportionate to the danger posed
Cognitive characteristics of phobias
-Selective attention - inability to focus on much else apart from stimulus
-Irrational beliefs - what could happen etc
-Cognitive distortions - irrational perceptions of stimulus
Two-process model
Mowrer's (1960) model to explain phobias stating that phobias are acquired by classical conditioning then maintained by operant conditioning
Acquisition by classical conditioning
e.g. Little Albert
US = UR
NS = NR
NS + US = UR
CS = CR
Conditioning generalises to similar objects
Maintenance by operant conditioning
-Negative reinforcement - avoidance of situation removes unpleasant anxiety
-Therefore avoidance likely to be repeated
Two-process model evaluation
-Good explanatory power - cause = treatment
-Avoidance behaviour - motivated by positive feelings of safety, person sticks with safety factor (e.g. agorophobe may feel less anxiety going outside with someone)
-Incomplete - disregards biological evolutionary factors e.g. Seligman (1971) biological preparedness where we have phobias associated with innate knowledge of danger (dark, snakes)
-Phobias may not follow trauma
-Doesn't explain cognitive aspects
Systematic desesitisation
Behavioural therapy designed to reduce an unwanted response to a stimulus where a patient is taught to relax in the presence of a phobic stimulus
Counterconditioning
The learning of a different response to a stimulus
Reciprocal inhibition
The idea that two opposite emotions cannot be felt at the same time so one cancels out the other
Systematic desensitisation
-Anxiety hierarchy - list of phobic situations in order of level of anxiety induced
-Relaxation - deep breathing, drugs, imagining themselves on a beach etc
-Exposure - patient exposed to stimulus whilst in relaxed state, moves up anxiety hierarchy until patient remains relaxed in high anxiety situations
Systematic desensitisation evaluation
-Effective - Gilroy (2003) follows up 42 patients who had three 45 minute sessions, at both 3 and 33 months they had less anxiety than control group
-Suitable for diverse range of patients - can be understood and engaged with by those w/ learning difficulties
-Acceptable - not traumatic, lower refusal and attrition rates
Flooding
-Behavioural therapy in which a patient is exposed to an extreme form of phobic stimulus in order to reduce the anxiety stimulated by it by process of extinction
-Patient must give fully informed consent
Extinction
Learned response is extinguished when conditioned response is encountered without the unconditioned stimulus so the conditioned stimulus no longer produces the conditioned response
Flooding evaluation
-Cost-effective - fewer sessions needed
-Less effective - complex phobias like social phobia wouldn't apply
-Traumatic treatment - high refusal and attrition rates, wasted time and money
Behavioural characteristics of depression
-Activity levels - reduced energy levels leading to withdrawal from work, education and social life
-Disruption to sleep + eating - insomnia and hypersomnia, increase or decrease in appetite leading to weight gain/loss
-Aggression and self harm - irritability, verbal aggression, physical aggression directed at themself
Emotional characteristics of depression
-Lowered mood - feelings of worthlessness and emptiness
-Anger - can be extreme, can lead to aggressive behaviour directed at the self or others
-Lowered self-esteem - dislike of the self, self-loathing
Cognitive characteristics of depression
-Poor concentration - difficulty finishing tasks or making decisions that previously wouldn't have been an issue
-Attending to/dwelling on the negative - ignoring the positives of a situation, biased recall of unhappy events over happy ones
-Absolutist thinking - all good/all bad, see bad situations as an absolute disaster
Beck's cognitive theory of depression
-Faulty information processing - focussing on the negative, ignoring the positives, blowing small problems out of proportion
-Negative self schemas - interpreting information about ourselves negatively
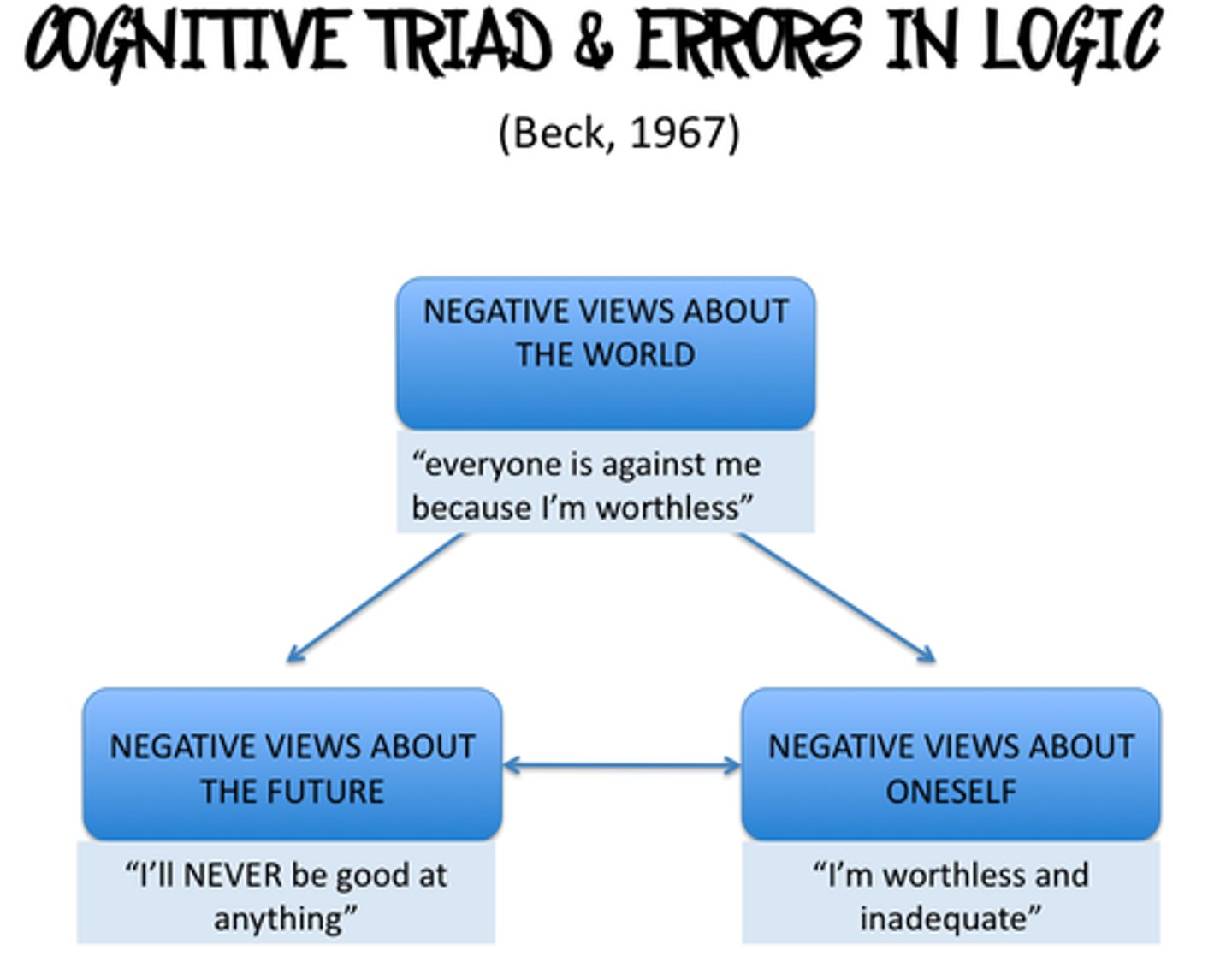
-The negative cognitive triad
Beck's negative triad
Three kinds of negative thinking that lead to depression
1. negative view of the world - cold, hard place
2. negative view of the future - things will always be this way
3. negative view of the self - failure
Beck's theory evaluation
-Good supporting evidence - Grazioli and Terry
-Practical application - CBT can challenge components of triad and encourage patient to think about their sensibility
-Doesn't explain all aspects - Cotard syndrome, hallucinations, bizarre beliefs
Grazioli and Terry (2000)
-Assessed 65 pregnant women for cognitive vulnerability and depression before and after birth
-Cognitively vulnerable women more likely to develop post-natal depression
Ellis
Good metal health is the result of rational thinking that allows people to be free of pain
Ellis' ABC model
-Activating event - negative events trigger irrational beliefs
-Beliefs - irrational beliefs such as need for perfection, success, fairness
-Consequences - emotional and behavioural consequences of irrational beliefs
Ellis' ABC model evaluation
-Practical application - CBT can challenge irrational beliefs
-Doesn't explain all aspects - Cotard syndrome, hallucinations, bizarre beliefs
-Partial explanation - only applies to reactive depression (following unpleasant events ) and not post-natal depression etc
Cognitive behavioural therapy (CBT)
Method for treating mental disorders based on both cognitive and behavioural techniques where negative thoughts are challenged and enjoyable behaviour is encouraged
Irrational/dysfunctional thoughts (Ellis)
Thoughts that are likely to interfere with a person's happiness, leading to depression
CBT process
-Assessment - establishment of patient's problems + goals, plan conceived to achieve goals
-Irrational thoughts identified
Beck's cognitive therapy
-Identification of negative thoughts about world, self and future
-Reality of these beliefs is tested - recording when they enjoyed something or someone was nice to them
-'Patient as scientist' - investigation into beliefs to give therapist evidence against them
Ellis' rational emotive behavioural therapy (REBT)
-Extends ABC model to ABCDE - dispute and effect
-REBT therapist identifies irrational beliefs + challenges them in order to change belief and break link between negative life events and depression
-Empirical argument and logical argument to dispute beliefs
Empirical argument
Used in REBT - disputing whether there is actual evidence to support an irrational belief
Logical argument
Used in REBT - disputing whether the negative thought logically follows from the facts
Behavioural activation
Therapist encourages patient to engage in enjoyable activities or exercise to provide more evidence for irrational nature of beliefs
Evaluation of treatments of depression
-Effective - March (2007)
-May not work in severe cases - drugs required to give patient motivation/ability to engage w/ therapy
-Overemphasis on cognition - circumstances (poverty, abuse) may influence depression
March
-327 adolescents diagnosed w/ depression
-After 36 weeks 81% of CBT and antidepressants groups showed significant improvement, 86% in combination group
-CBT is just as effective as drug therapy