Medical Sociology Exam 4
1/147
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
148 Terms
Has the relationship between education and mortality increased or decreased?
Increase
The link between education and mortality is finely graded, meaning that every incremental year of schooling, not just the attainment of a degree, is associated with a significant mortality advantage
For which causes of death is the effect of education larger: high preventability or low preventability?
The effect of education is larger for high-preventability causes of death. This fits the Fundamental Cause Theory because people with more education can better use knowledge and resources to prevent disease when prevention is possible.
According to the logic of Fundamental Cause Theory, is stress itself a fundamental cause?
False. Stress is not a fundamental cause. It is better understood as a mechanism or pathway through which broader social conditions may affect health. Fundamental causes are upstream social conditions that affect multiple diseases through multiple risk factors and persist over time.
What is the relationship between SES and health?
There is a strong and consistent link: higher SES leads to better health outcomes. The relationship has grown stronger, meaning the health gap between high and low SES has increased over time. It continues even when diseases and risk factors change, suggesting deeper structural causes.
What does “all-cause mortality” mean in the context of SES?
It means SES influences the total likelihood of dying from any cause, not just a single specific disease.
What does “associations are gradual” mean in SES and health?
Health improves step by step with increases in SES; it is not just a rich vs. poor divide.
What is the health-wealth gradient?
Every increase in income, education, or status is linked to better health and lower mortality.
According to Grossman, what is the most important correlate of good health?
Formal education (years of schooling).
What is the “credentialing effect” in education?
The idea that having a degree itself improves outcomes, regardless of years of schooling. This theory suggests that the health benefits of education are tied to achieving specific milestones, such as a high school diploma or a college degree, rather than just the time spent in the classroom
Does evidence support the credentialing effect or cumulative benefits?
Evidence supports cumulative benefits: more years of education gradually improve health.
What was the Whitehall Study?
A study of British civil servants that examined the relationship between job status (SES) and health outcomes. Conducted by Michael Marmot, who followed over 18,000 male British civil servants, and is famous for establishing the "Status Syndrome," the finding that an individual’s rank in the social hierarchy is intimately related to their risk of illness and length of life
Why was the Whitehall Study unique in its population?
All participants were employed and had access to healthcare, meaning they were not in absolute poverty.
What is the “psychosocial revolution” from the Whitehall Study?
A shift toward explaining health differences through stress, status, and social hierarchy, not just material deprivation. The study was considered a "psychosocial revolution" because it looked at a population where everyone was employed, had decent housing, and enjoyed universal medical coverage through the British National Health Service. Because none of these men were living in absolute material deprivation, Marmot argued that material circumstances (like lack of food or shelter) could not explain the dramatic health differences between the grades
What key finding did the Whitehall Study reveal?
The central claim was that health is not just a binary between the "poor" and the "non-poor". Instead, the study found a finely graded health gradient: at every step up the employment ladder, mortality risk decreased. This means that even among people who are not poor and have "good stable jobs," those with slightly higher status jobs have lower mortality rates than those just below them
In the Whitehall Study, who had the highest mortality?
Those in the lowest job grades, The “Other” (least senior) group.
In the Whitehall Study, who had the lowest mortality?
Those in the highest job grades (administrators).
What does the Whitehall Study suggest about SES and health?
Relative status and position in hierarchy significantly impact health. Whitehall claimed that relative position in the "pecking order" is the primary driver of health outcomes. The theory suggests that being lower in the hierarchy is inherently stressful because individuals are sensitive to "feeling looked down on, being devalued, and being treated as second rate". This chronic stress triggers physiological pathways that lead to disease
What role does stress play according to the Whitehall Study?
Stress from lower status and less control contributes to worse health outcomes.
What does the Whitehall study say about lifestyle choices and the importance of control?
4. Limitations of Health Behaviors
Another major claim was that lifestyle choices (such as smoking, obesity, and lack of exercise) do not fully explain the gradient. Specifically, the Whitehall findings indicated that these standard risk factors accounted for no more than one-third of the observed differences in coronary heart disease mortality between employment grades.
5. The Importance of Control
Finally, the study highlighted that higher status confers more control over one's life, which acts as a buffer against stress. Conversely, being lower in the hierarchy often means having less autonomy and a lower "effort-to-reward" ratio, which contributes to the biological wear-and-tear that shortens lifespan
Does the SES gradient persist into older age?
Yes, though differences between top groups become less distinct in very old age.
What do “Marmot curves” show about neighborhoods and health?
Life expectancy increases as neighborhood income deprivation decreases.
What do geographic disparities in health suggest about SES?
SES affects health through where people live, not just individual factors. Through physical environments (housing, pollution, resources) and social environments (safety, stress, community).
The "Associations Have Grown" graph (Slide 10) illustrates how the mortality gap between socioeconomic groups widened significantly between 1960 and 1986. What does this pattern support in theory?
It supports fundamental cause theory—SES allows people to take advantage of new health innovations.(Link & Phelan)
Did mortality rates increase or decrease overall from 1960 to 1986?
They decreased overall, but not equally across SES groups.
Who had the most deaths in both 1960 and 1986 relative to their education? Men or Women?
Men with the least education
How does innovation affect inequality according to Fundamental Cause Theory?
New treatments increase inequality because high-SES individuals access and use them more effectively.
What is meant by the “reversal” in SES and health?
Lower-education groups are not just falling behind—they are losing years of life.
Between 2010–2017, who experienced the most decline in life expectancy?
Individuals with low education, especially white men and women.
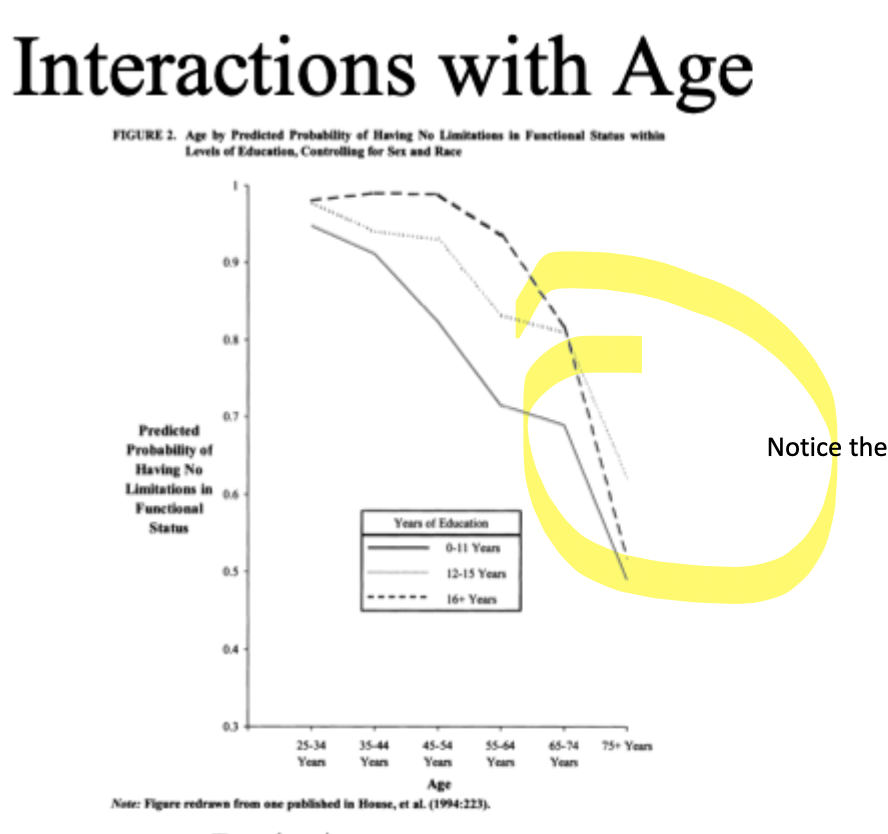
When does the health gap become the most pronounced?
During age 45-54, 55-64
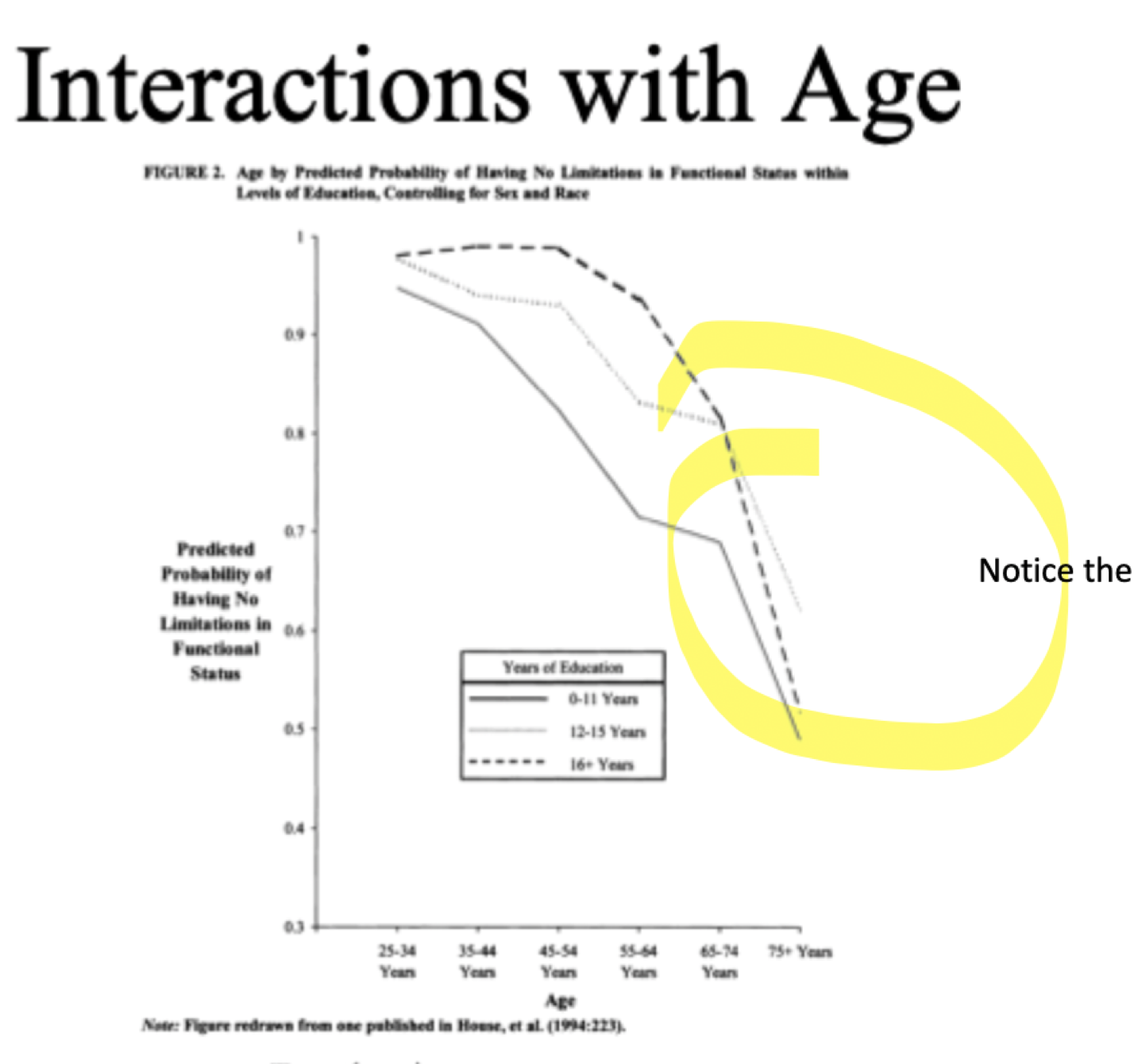
When is the health gap the smallest?
Young adulthood (25–34) and very old age (75+).
Define cumulative advantage.
Advantages and disadvantages accumulate over the life course, widening health gaps.
Cumulative Advantage Theory
This theory explains why the lines "fan out" as people age. It suggests that the benefits of high SES (like better healthcare, lower stress, and safer environments) and the harms of low SES (like physical labor or poor nutrition) accumulate over decades. By age 55, these accumulated differences result in a massive health divide.
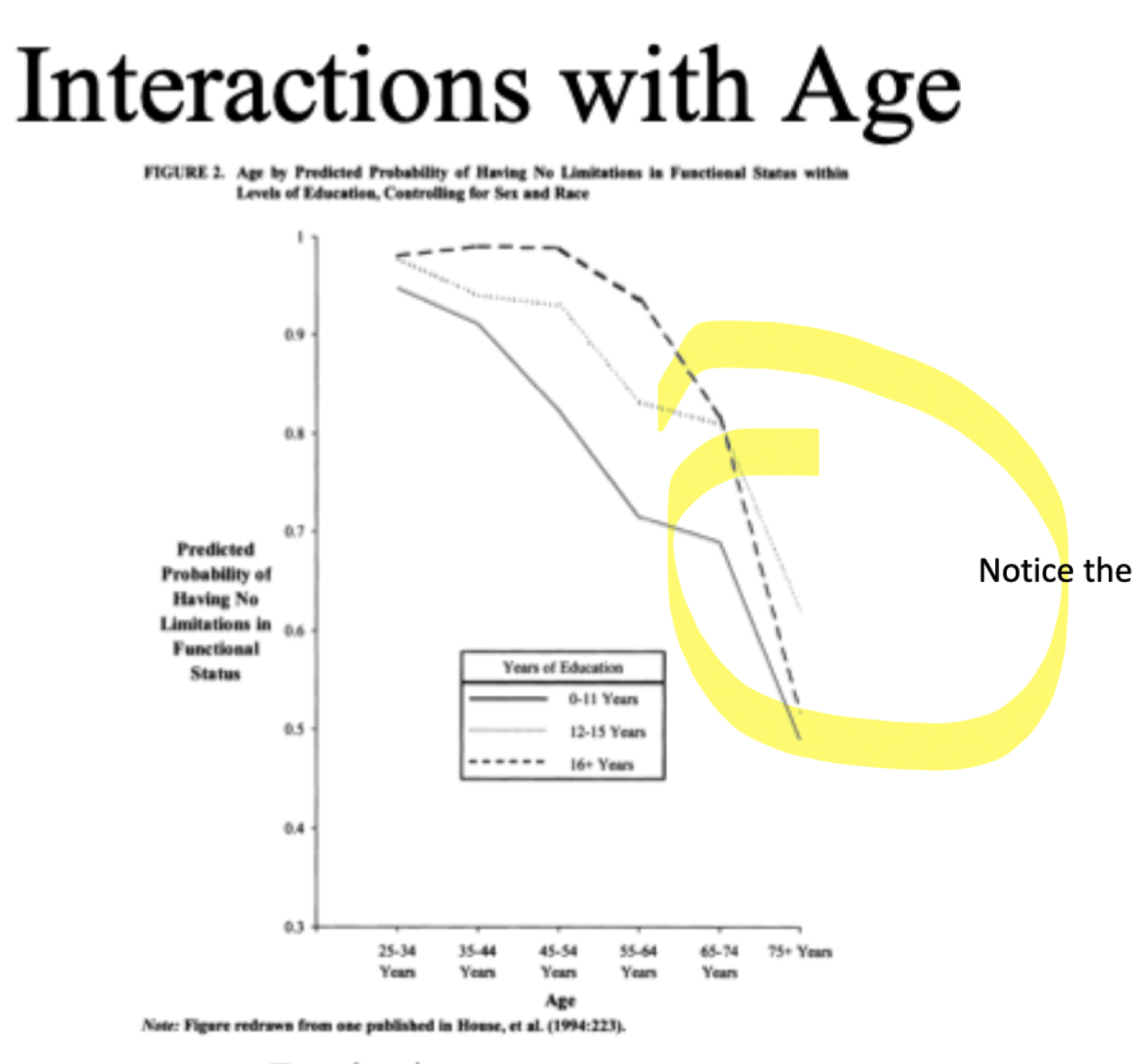
Age-as-Leveler Theory
This theory explains the convergence of the lines at the very end of the graph (age 75+). It suggests that in very old age, biological decline becomes a "universal leveler" that eventually affects everyone regardless of their previous social position. Additionally, social safety nets like Medicare may help to level the playing field by providing resources to those who previously lacked them.
What is Fundamental Cause Theory?
(Sociologist’s explanation) A theory by Bruce Link and Jo Phelan stating that SES is a root cause of health inequalities because it provides access to flexible resources.
Resources: These include money, knowledge, power, prestige, and social connections.
Mechanism: People use these resources to avoid risks (e.g., living in a safe neighborhood) and minimize the consequences of disease once it occurs (e.g., accessing the best specialists).
Persistence: Because these resources are flexible, they remain effective even as the specific diseases and risks in a society change over time
What does Psychosocial Theory argue?
Health is shaped by stress from social hierarchy, not just material resources. This perspective, heavily influenced by the Whitehall Study and the work of Michael Marmot, focuses on the "Status Syndrome".
Relative Deprivation: The argument is that being lower in the social hierarchy is inherently stressful because individuals feel "looked down on" or "devalued".
Biological Impact: This chronic stress triggers physiological responses (like elevated cortisol) that cause long-term wear-and-tear on the body, leading to disease.
Control: Higher status often confers more control over one's life, which acts as a buffer against stress
What is status syndrome?
A concept from Michael Marmot where lower status → more stress → worse health.
Why is control over life important for health?
More control → less stress → better health outcomes.
How do economists view health?
As human capital—something people invest in to increase productivity and lifespan.
What is Selection (social selection)?
This occurs when health causes social position. Specifically, childhood health conditions (like chronic asthma or malnutrition) can impede a child's education and future earning potential, leading to lower adult SES
What is reverse causation (health drift)
This happens in adulthood when a "health shock" (like a sudden disability or major illness) causes a person to lose their job or exhaust their savings, thereby lowering their SES
What is contamination?
A third variable (e.g., personality, genetics) influences both SES and health, making the relationship look causal.
This suggests the relationship is spurious because a third factor—such as genetics or personality traits (e.g., self-control)—underlies both an individual's ability to achieve high SES and their ability to maintain good health
What does newer research (Link et al., 2013) argue about status?
It’s not status itself, but the life conditions and exposures that come with status that affect health.
What example shows status can both help and harm health?
Emmy winners → more resources → better outcomes
Presidents → stress/risk → potentially worse outcomes
Why is the relationship between parents’ SES and children’s health considered causal rather than contaminated?
Children’s health is directly shaped by their parents’ SES through living conditions, nutrition, access to care, and environment, making it a strong causal relationship, not a spurious or contaminated one (since children’s SES is not independently determined).
What are distal causes of health?
Broad, upstream social factors (like SES, education, and neighborhood) shape exposure to risks and access to resources. They explain why health inequalities exist.
What are proximate causes of health?
Immediate, downstream mechanisms (behaviors and biological processes) that directly lead to disease. They explain how disease happens.
What is the key difference between distal and proximate causes?
Distal → root, structural causes (why inequality exists)
Proximate → immediate mechanisms (how disease occurs)
Why are distal causes considered “upstream”?
They set the context for health by shaping access to resources and exposure to risks before disease occurs.
What are examples of distal causes?
Socioeconomic status, education, social support, neighborhood conditions, race
What makes distal causes “fundamental”?
They involve flexible resources (money, knowledge, power, social ties) that can be used to avoid risks and manage disease.
What are proximate mechanisms in health?
Immediate, downstream pathways through which disease occurs, including behaviors and biological processes.
What are examples of proximate mechanisms?
Back:
Behaviors: smoking, diet, exercise
Biology: blood pressure, cholesterol, infections
What is the relationship between distal and proximate causes according to Bruce Link and Jo Phelan?
Distal causes → Proximate mechanisms → Health outcomes
Why do sociologists focus more on distal causes than proximate ones?
Because distal causes drive the entire system and explain why health inequalities persist over time.
Why is focusing only on proximate causes insufficient?
If one proximate risk is reduced, new risks will emerge unless the underlying distal cause is addressed.
Why does medicine tend to focus on proximate causes?
They are easier to measure, treat, and intervene on (e.g., prescribing medication).
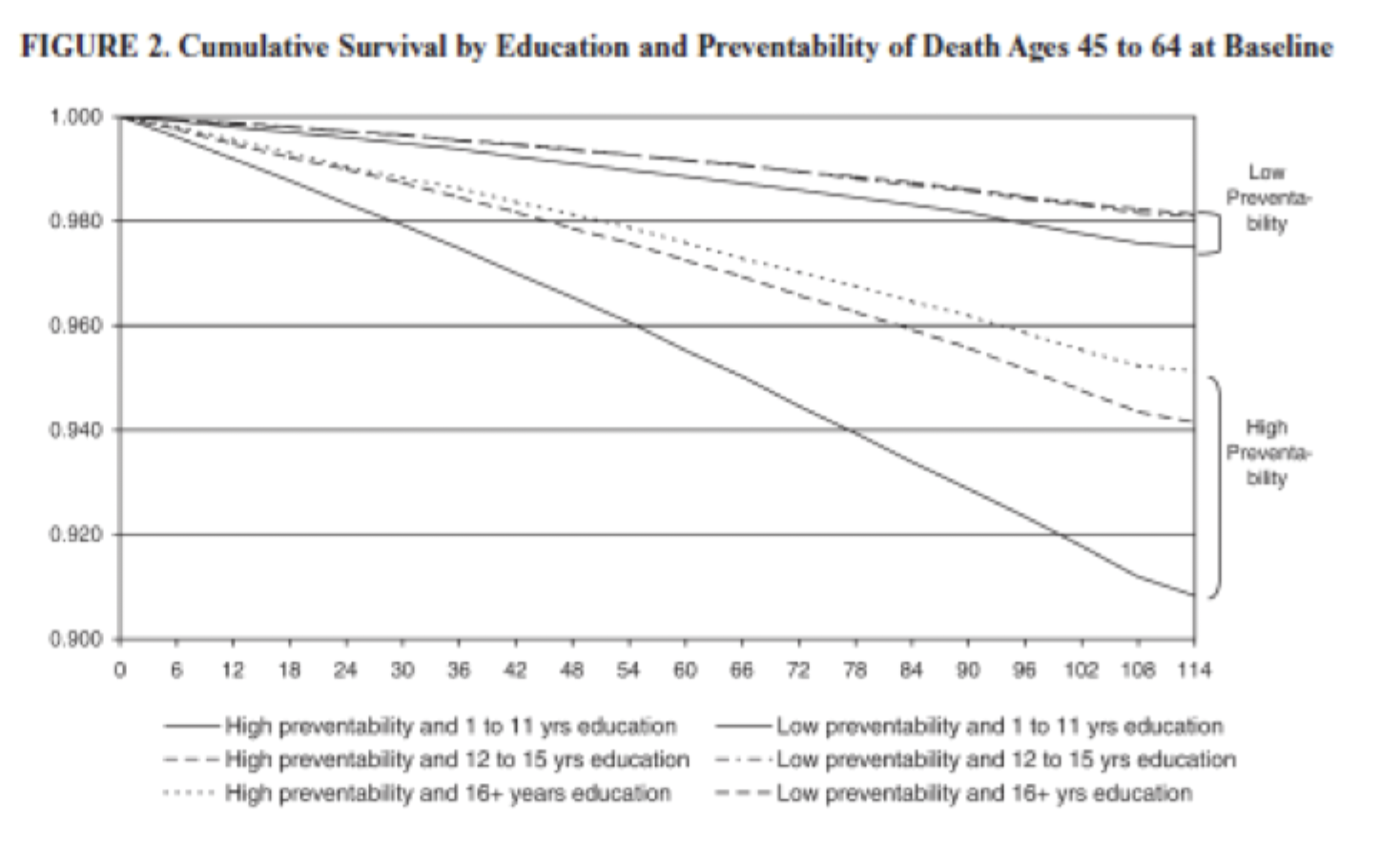
What does the “importance of preventability” show about SES and health?
When there are ways to prevent or treat a disease, people with higher SES can use their resources (money, knowledge, access) to stay healthier—so the gap between rich and poor gets bigger.
But when a disease can’t really be prevented or treated, no one has an advantage—so the gap gets smaller.
More control over disease → bigger inequality
Less control over disease → smaller inequality
When is the SES gap in survival the most extreme?
For diseases with high preventability or effective treatment.
When is the SES gap in survival the smallest?
For diseases with low preventability, where no effective interventions exist.
Why does preventability increase health inequality? (What happens to health inequality when medical innovation occurs?)
Because high-SES individuals can use flexible resources (money, knowledge, power) to avoid risks and access treatments. Inequality often increases because high-SES groups benefit first and most.
Who benefited the most from heart disease improvements? Who benefited the least from heart disease improvements?
Those with the most education (13+ years) / Those with the least education (0–7 years).
What changed after the Surgeon General’s report?
High-SES individuals were more likely to quit, creating a new inequality. Inequality can emerge after new knowledge becomes available, due to unequal resource use.
How does preventability support Fundamental Cause Theory?
It shows SES matters most when people can use resources to prevent or treat disease.
What explains recent declines in life expectancy among low-SES groups?
Drug use (deaths of despair) is the largest contributor to increased years of life lost (YLL).
Which group is the most impacted by drug-related mortality?
Individuals with low education (high school or less), especially white men and women.
In Fundamental Cause Theory, what are health behaviors considered?
Proximate (downstream) mechanisms, not root causes.
For example, once the "resource" of knowing smoking is harmful became available, the most educated used their flexible resources to quit, while the least educated remained stuck in social conditions that make health behaviors harder to change
Why are health behaviors not the main cause of health inequality?
Because they are shaped by upstream SES conditions, not independent drivers.
What is the true underlying cause of SES health inequalities?
Distal factors (SES) and access to flexible resources.
Why do sociologists argue that health behaviors do NOT fully explain SES-based health inequalities?
Limited explanatory power:
Behaviors explain only a small portion of health differences
Example: Whitehall → ≤ 1/3 of heart disease differences
Most inequality remains unexplained after controlling for behaviors
👉 Therefore, behavior is NOT the root cause
What is cultural health capital? (Gage-Bouchard)
Refers to the set of socially learned skills, knowledge, and communication styles that enable individuals to effectively interact with healthcare providers and navigate the healthcare system. Higher-SES individuals are more likely to possess CHC, allowing them to navigate the healthcare system more effectively and receive better care.
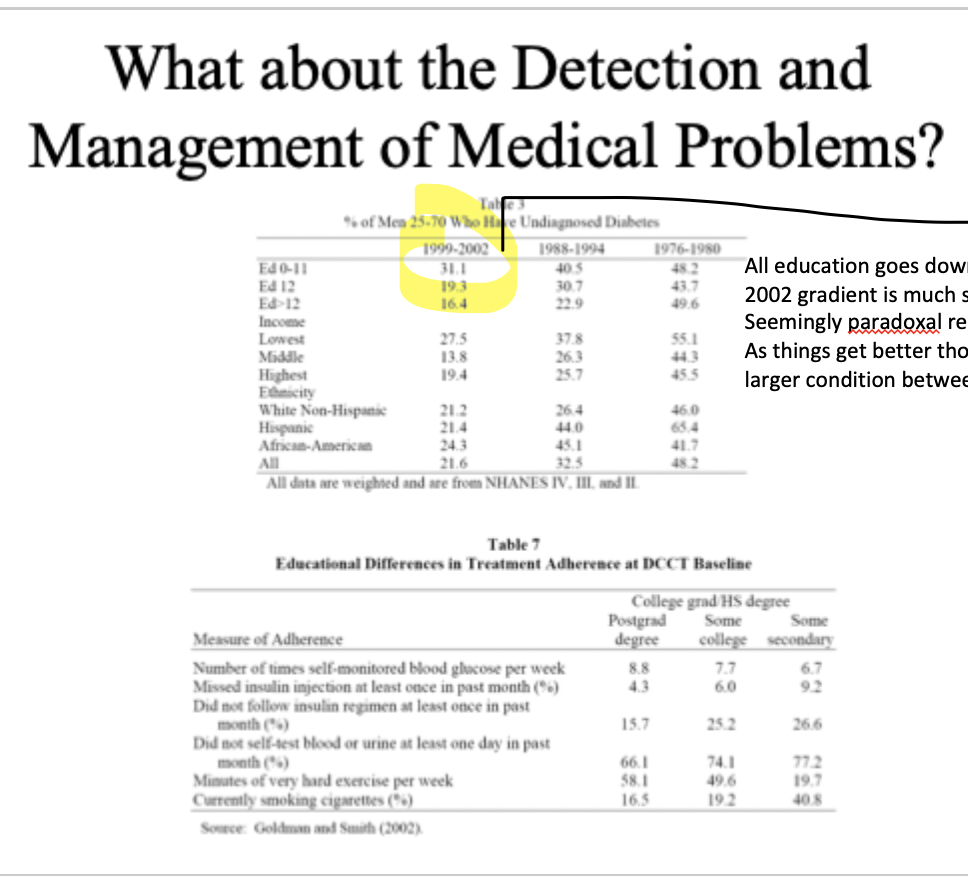
What do these tables prove about SES and health?
The key takeaway is that higher socioeconomic status improves both the detection and management of disease. People with lower education and income are more likely to have undiagnosed conditions (like diabetes), meaning problems are caught later, while higher-SES individuals are more likely to adhere to treatment (monitoring, medication, exercise). This shows that health inequality is not just about getting sick, but also about who gets diagnosed early and who is able to manage their condition effectively over time.
What did the pediatric cancer study reveal about healthcare inequality?
It revealed that even when families receive care in the same hospital with access to the same treatments, outcomes still differ based on social class. Differences persist because families vary in their ability to communicate with providers, understand medical information, and advocate for their children, which affects how care is delivered.
Why are higher-SES families more successful in navigating healthcare?
They are more familiar with these unwritten rules and can present their concerns in ways that physicians perceive as appropriate and legitimate, leading to better responses and care.
What is vigilant advocacy and who uses it?
Vigilant advocacy is a style used primarily by higher-SES parents (middle- and upper-class parents) in which they actively monitor care, ask informed questions, and engage with providers using medically appropriate language.
What is the outcome of vigilant advocacy?
Physicians tend to respond positively to this approach, often empathizing with the parents, taking their concerns seriously, and sometimes providing additional time or flexibility in care.
What is trusting advocacy?
Trusting advocacy is a style in which parents defer to the physician’s expertise and allow the doctor to make decisions without questioning or challenging recommendations.
What is the outcome of trusting advocacy?
Physicians generally find these patients easy to work with, but this approach may result in missed opportunities to question care or identify potential problems.
What is antagonistic advocacy?
Antagonistic advocacy involves challenging medical recommendations in a confrontational or blunt manner, often without the medical knowledge needed to support those challenges.
What is the outcome of antagonistic advocacy?
Physicians may perceive this style as inappropriate or ineffective, which can lead to defensive reactions, reduced communication, and poorer care outcomes.
What was the relationship between income and cholesterol in 1976–1980?
Higher income was associated with higher cholesterol levels. Wealthier individuals had worse cholesterol outcomes at that time. This is because higher-income individuals had greater access to expensive, high-fat, high-cholesterol foods, which were considered desirable at the time. The pattern was stronger in men, meaning high-income men had especially high cholesterol levels compared to others.
What changed in the relationship between income and cholesterol by 1999–2004? What explains the reversal in the income–cholesterol relationship?
The relationship reversed, so higher income was now associated with lower cholesterol levels. innovation, including new medical knowledge about diet and cholesterol, allowed high-SES individuals to change their behaviors and reduce risk.
What is the MacArthur Ladder and what does it measure?
A tool used to measure subjective social status (SSS) by asking individuals to place themselves on a ladder relative to others in society based on income, education, and occupational prestige. It captures how people perceive their own position in the social hierarchy rather than their objective SES.
Why is subjective social status important for health?
Subjective social status matters because individuals’ perceptions of their rank influence their stress levels, sense of control, and psychological well-being, all of which have direct effects on health outcomes.
What advantages are associated with moving up the social “ladder”?
Each increase in status is associated with greater access to resources, increased control over life circumstances, more respect and deference from others, and preferential treatment within institutions, all of which contribute to better health.
How does subjective social status affect adolescents’ daily experiences?
Adolescents with lower subjective social status experience higher levels of psychological distress in their daily lives, indicating that perceptions of status influence mental health even at a young age.
How does the Whitehall Study provide evidence for relative status affecting health?
The Whitehall Study showed that British civil servants with lower job ranks had worse health and higher mortality than those in higher ranks, even though all participants had stable jobs and access to healthcare. This demonstrates that relative position in a hierarchy, not just absolute poverty, affects health. It shows that health follows a gradient within a hierarchy, meaning that even among non-poor individuals, those lower in rank experience worse health outcomes due to factors like reduced control and increased stress.
How do ladder studies provide evidence for the role of relative status?
Ladder studies show that individuals who perceive themselves as lower on the social ladder report worse health outcomes, even after controlling for objective SES measures like income and education.
How does subjective social status affect adolescents’ daily experiences?
Adolescents with lower subjective social status experience higher levels of psychological distress in their daily lives, indicating that perceptions of status influence mental health even at a young age.
What did the original Academy Award study claim about longevity?
The original study claimed that Academy Award winners lived approximately four years longer than nominees who did not win, suggesting that higher status might directly increase lifespan.
What is immortality-time bias?
Occurs when individuals are incorrectly credited with survival time before an event that defines group membership, such as winning an award, even though they had to survive that period to be eligible.
What did the Emmy Award study find about status and longevity?
The study found that Emmy winners lived about 2.7 years longer than nominees, likely because winning led to increased income, better job opportunities, and improved life conditions.
Why did the Baseball Hall of Fame show no longevity difference?
Because induction occurs after a player’s career has ended, it does not significantly change their resources or life circumstances, so it does not affect health or lifespan.
What did the presidential election findings reveal about status and health?
Presidential winners lived about 5.3 years fewer than their opponents, likely due to the extreme stress and risks associated with holding high political office.
What overall conclusion can be drawn from these award studies?
Status does not consistently improve health; its effects depend on whether it changes life conditions in ways that either reduce or increase stress and risk.
How does social rank affect health in primates like baboons?
Higher-ranking individuals tend to have better health outcomes, including lower levels of cortisol, indicating lower chronic stress.
Why is the relationship between rank and health not universal across species?
Because the health effects of rank depend on the social structure; in some species, dominant individuals experience more stress, showing that rank alone is not inherently beneficial or harmful. They show that it is not rank itself that determines health, but the conditions and experiences associated with that rank.
What is ecological momentary assessment (EMA) and why is it important in this study?
Ecological momentary assessment is a method that collects real-time data through devices like cell phones, allowing researchers to measure individuals’ day-to-day experiences of stress and emotion, rather than relying on retrospective reports.
What does the lower graph (SSS vs psychological distress by age) demonstrate?
It shows a negative relationship between SSS and distress, meaning that as subjective status decreases, psychological distress increases, and this pattern is strongest in older adolescents.
Why is SES considered a “fundamental” cause of health?
SES is fundamental because it affects multiple diseases, operates through multiple pathways, and continues to influence health even as specific risks and diseases change over time.
How does Fundamental Cause Theory explain the cholesterol graph reversal?
When new knowledge about diet and cholesterol emerged, higher-SES individuals used their resources to change behavior first, leading to a reversal where they became healthier, while lower-SES groups lagged behind.