Motor Control Exam 3
1/156
Earn XP
Description and Tags
alliedaury
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
157 Terms
vestibular system roles
- sensory system w/ motor implications
- head position in relation to gravity
- head movement
- equilibrium/balance/postural control
- provides extra information beyond what proprioception provides
- allows for faster muscular adjustments
- helps us discern self motion vs environment motion
vision, vestibular, and proprioception
what are the 3 sensory afferents?
cortex, brainstem, cerebellum, and spinal cord
balance systems provide input to what 4 areas of the body?
true
T/F: if you lose 1/3 of your sensory systems you are able to adjust easily
true
T/F: if you lose 2/3 or all 3 of your sensory systems you will have major balance deficits and trouble with upright postural control
cortex, brainstem, and cerebellum
what 3 areas of the nervous system does the vestibulocochlear nerve synapse on?
outputs
____ in response to vestibular inputs
- oculomotor nerve
- cervical spine
- body
- conscious perception
- autonomic response
temporal
the vestibular apparatus is embedded in the ____ bone
bony; membranous
the vestibular apparatus is described as a ____ labyrinth with a ____ labyrinth lining
hair cells
nerve endings that when deflected transmit signals
otoliths
utricle and saccule
- responsible for recognizing linear acceleration or deceleration
- sensitive to relationship to gravity
utricle
detects horizontal linear acceleration (plane/train)
saccule
detects vertical linear acceleration (elevator)
hair; membrane; otoconia
these structures are within the macula (otoliths)
- ____ cells
- gelatinous _____
- _____ = pieces of calcium carbonate
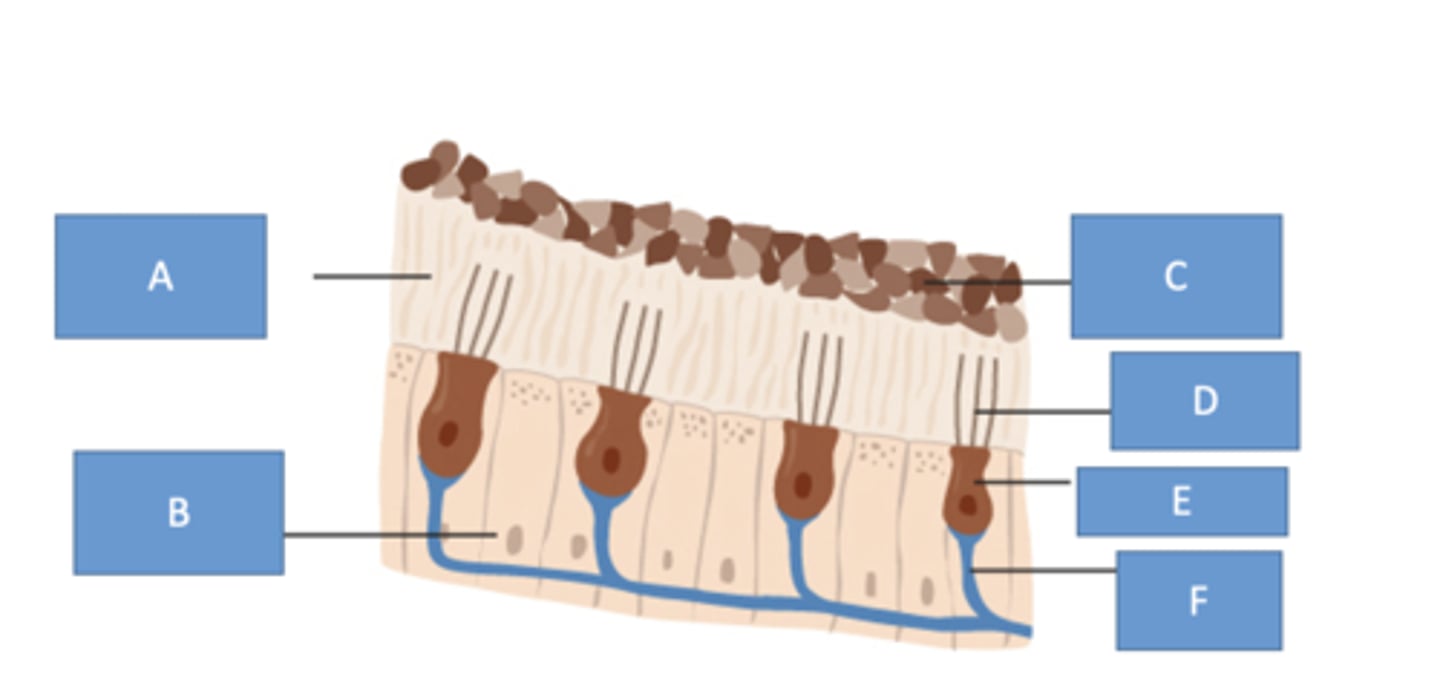
deflects
with movement, the otoconia weigh down the gel membrane which _____ hair cells
perpendicular
the utricle and saccule are ____ to each other
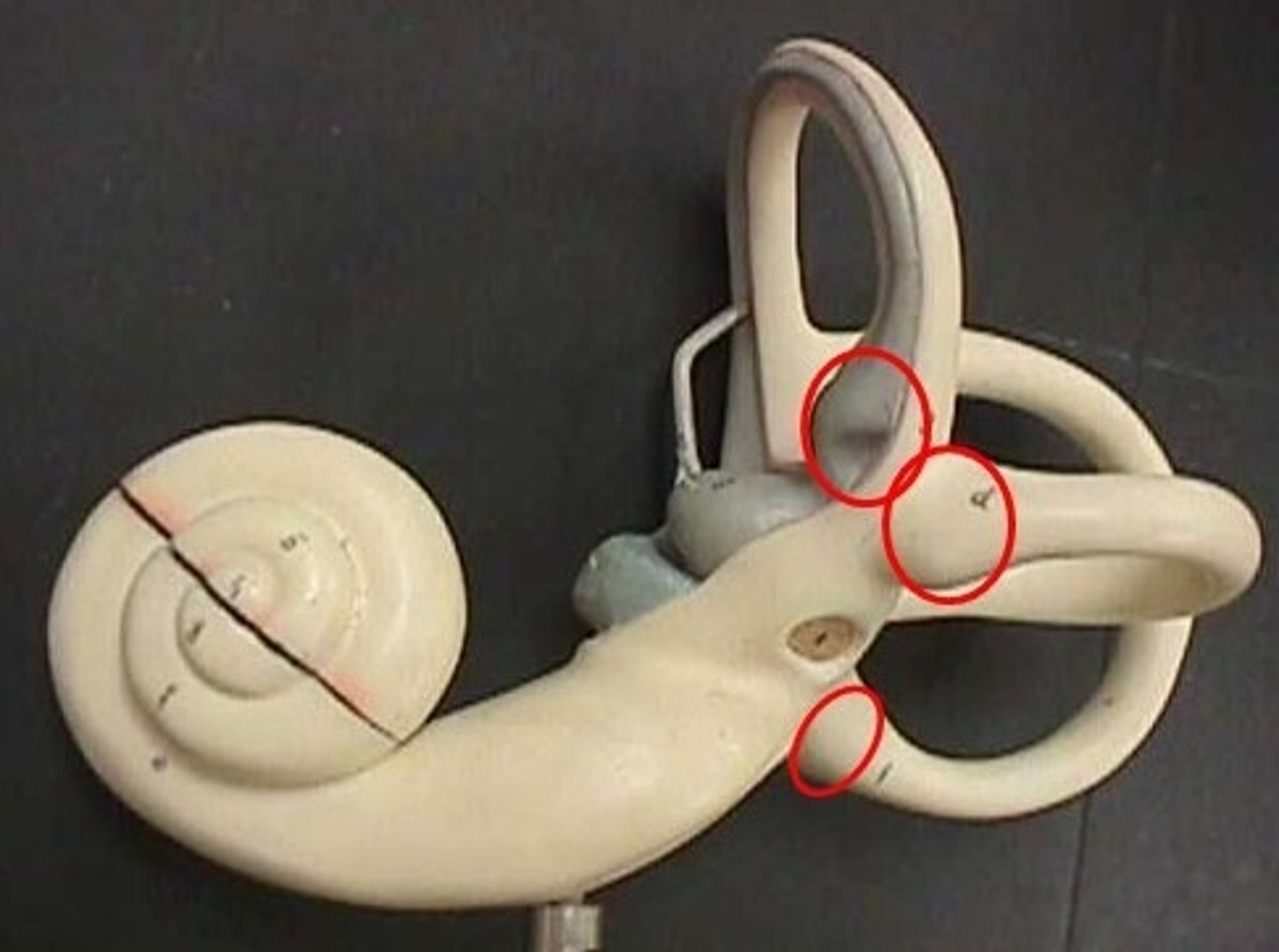
semi-circular canals
sense angular acceleration in 3 different planes
- posterior
- anterior (aka superior)
- horizontal (aka lateral)
90
semicircular canals are oriented ___ degrees to each other
- bilateral symmetry
- L and R horizontal canals work together
- Contralateral posterior and anterior canals work together
endolymph
the semi-circular canals are filled with ____ fluid
- moves opposite the direction of the head due to inertia (lag)
ampulla
interrupts semicircular canals
- crista (hair cells and supporting cells)
- cupula
- displaced by the endolymph ---> nerve firings
- deflection = excitatory or inhibitory effect
increased; decreased
with the horizontal canals, there should be ____ firing on the side you turn your head towards and ____ firing on the side opposite which you turn your head
push-pull relationship
head motion results in excitation on one side and inhibition on the other side
- brain interprets this firing asymmetry between sides as head movement
- this phenomenon provides sensory redundancy
dysfunction
vestibular _____
- pathology can cause changes in firing rates that are not due to head movement
- when those changes cause firing asymmetry, it leads to sensation of head spinning when it's actually still
- this stimulates VOR and causes reflexive eye movement, leading to nystagmus
MLF
ascends to nuclei for CN III, IV, and VI and the superior colliculus
- for eye movements/muscles
- oculomotor reflex, saccadic eye movements, smooth pursuit, and VOR
medial vestibulospinal tract
_____ _____ _____ MLF go to CN XI and cervical/upper thoracic SC
- for head/neck/upper body movements
lateral vestibulospinal tract
travels to the SC for upright posture and anti-gravity
- lower body movements/muscles
thalamus
synapses here to then go to the vestibular cortex
- cognition of spatial orientation, spatial memorym and perception of self motion
medial rectus
CN III controls the ___ ____ muscle
superior oblique
CN IV controls the _____ ____ muscle
lateral rectus
CN VI controls the _____ ____ muscle as well as the CL CN III nucleus
vestibulothalamocortical pathway
bilateral
- vestibular nucleus --> ventral posterior nucleus of thalamus --> vestibular cortex
- conscious awareness of head position and movement
- provides input to the CST to influence voluntary movement in response to head movement/balance challenge
vestibulo-colic reflex
head righting reflex
vestibulospinal reflex
for balance and upright posture
VOR
gaze stability when head moves quickly
- result of vestibular pathway to the extraocular muscles
- 1:1 ratio of head movement in one direction to eye movement in the opposite direction (head moves 15 degrees left, eyes move 15 degrees right to maintain object in focus)
vestibuloreticular pathway
information to the reticular formation (sleep/wake, habituation, pain modulation, muscle activity)
- autonomic response: nausea, vomiting
- altered consciousness (brain injury)
- influences reticulospinal tract (function of spinal reflex arcs and maintains muscle tone when standing and walking)
vestibulocerebellar pathway
influences coordination of postural muscles and head movement
- impacts magnitude of reflexive movements (body, head, eye)
- vestibular nerve routed to the fastigial nucleus which sends output to:
- vestibular nucleus --> MVST and LVST
- spinal cord: medial corticospinal tract
- reticular formation: medial reticulospinal tract
vestibular pathway
vestibular apparatus
vestibular nerve
cerebellar and vestibular nucleus
cerebellar output to fastigial nucleus then vestibular nucleus
vestib nucleus to 5 outputs
- reticular formation
- MLF ascends to CN III, IV, VI
- MVST in the descending MLF for head/neck for equilibrium
- LVST to spinal cord
- conscious pathway (cortex)
common vestibular symptoms
- dysequilibrium/imbalance
- ataxia of the trunk
- nystagmus: repetitive jerk and refixation of the eyes
- vertigo: subjective, conscious awareness of dizziness, true definition includes spinning but people often report different sensations
nerve; MLF
vestibular symptoms can occur with injury or lesion to:
- vestibular apparatus
- vestibular _____
- pons/medulla at level of nuclei
- disruption of _____ (eye movement issues)
- disruption of the LVST
- cerebellum
saccadic pursuit
abnormal smooth pursuit
saccadic intrusions
involuntary, rapid eye movements that interrupt steady fixation, causing the eyes to briefly jump off a target and usually return
esotropia

exotropia

strabismus
a common eye misalignment disorder where eyes point in different directions (crossed or turned) due to faulty neuromuscular control, poor muscle coordination, or high refractive errors
excited
vestibular nystagmus will always beat toward the relatively more _____ side
- named for the fast phase (from pt. perspective still)
remove
frenzel goggles are used to _____ visual fixation
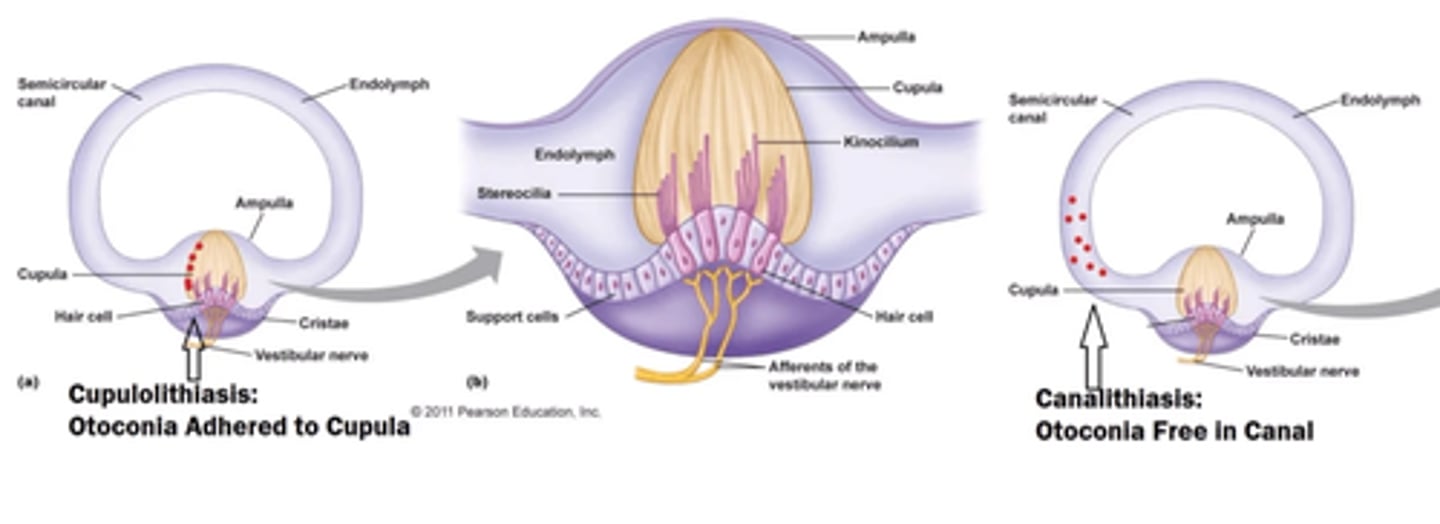
BPPV
most common peripheral vestibular disorder
- otoconia dislodge from the utricle and enter one or more of the semicircular canals
- causes: trauma, aging, viral, vitamin D deficiency, idiopathic
- episodes of dizziness triggered by head position changes
canalithiasis
episodes lasting < 1 min
- most common
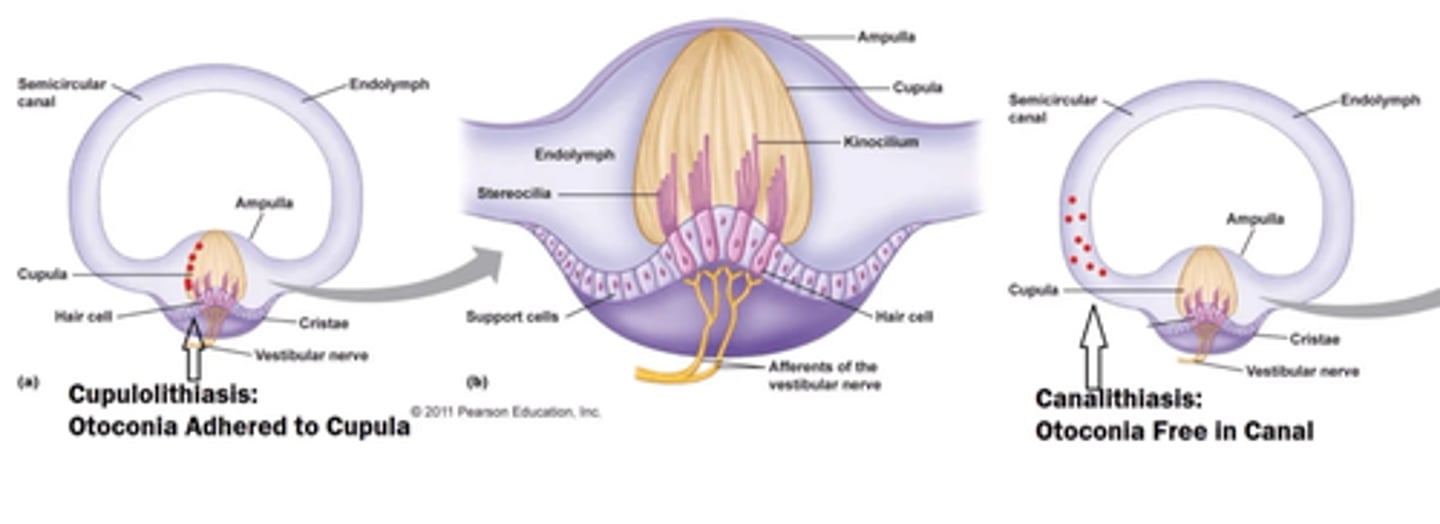
cupulolithiasis
episodes lasting > 1 min
right posterior SCC
which canal?
- rightward torsion
- upbeating nystagmus
left posterior SCC
which canal?
- leftward torsion
- upbeating nystagmus
right anterior SCC
which canal?
- rightward torsion (brief or not observed possibly)
- downbeating nystagmus
left anterior SCC
which canal?
- leftward torsion (brief or not observed possibly)
- downbeating nystagmus
posterior; anterior
the dix-hallpike checks for _____ or ______ canal involvement
BBQ/horizontal roll test
flex head to 30 degrees
roll head to right side and left side and observe
geotropic; worse
____ nystagmus in R and L sides of BBQ roll test:
- beats TOWARDS the ground usually < 60s (canalithiasis)
- affected side is the one with ____ symptoms
apogeotropic; less severe
_____ nystagmus in R and L sides of BBQ roll test:
- beats AWAY from the ground usually > 60s (cupulolithiasis)
- affected side is the one with ____ ____ symptoms
vestibular hypofunctions
inflammation of vestibular nerve causing a decrease in signal transmission on that affected side
- VOR impaired
- typically due to viral infection
- vestibular neuritis is most common
- vestibular labyrinthitis also possible (impacts hearing)
UVH
only one side is affected (decreased signal tranmission on one side)
vestibular neuritis
sudden onset or vertigo and nausea lasting approximately 1-4 days
- triggered by viral or bacterial infection
- dizziness and imbalance for weeks to months
vestibular labyrinthitis
sudden onset or vertigo and nausea lasting approximately 1-4 days
- triggered by viral or bacterial infection
- dizziness and imbalance for weeks to months
- hearing loss or reduction on one side
false
T/F: with hypofunctions it is common to have frequent reoccurnce or vertigo attacks
spontaneous
initially with a hypofunction a patient will exhibit a _____ nystagmus towards the healthy ear (other side is depressed)
alexander's law
amplitude of nystagmus increases when the eye moves in the direction of the fast phase (does not change directions)
- nystagmus lessens looking in the opposite direction
- nystagmus is greater with a fixation blocked (frenzel) and less with fixation
chronic
____ complaints of UVH
- blurred vision with head movement (things jump around)
- unsteadiness
- motion sensitivity
initial
____ complaints of UVH
- hx of present illness
- spontaneous or constant dizziness (can be spinning), usually with nausea, vomiting, unsteadiness, vision blurring esp with head movement ("couldn't get out of bed" "thought I was having a stroke")
- dizziness present even at rest but worsened with head movement, improves over a few days
- if seeks medical help may be put on vestibular suppressants
- may see this if being seen in ER
tests for hypofunction
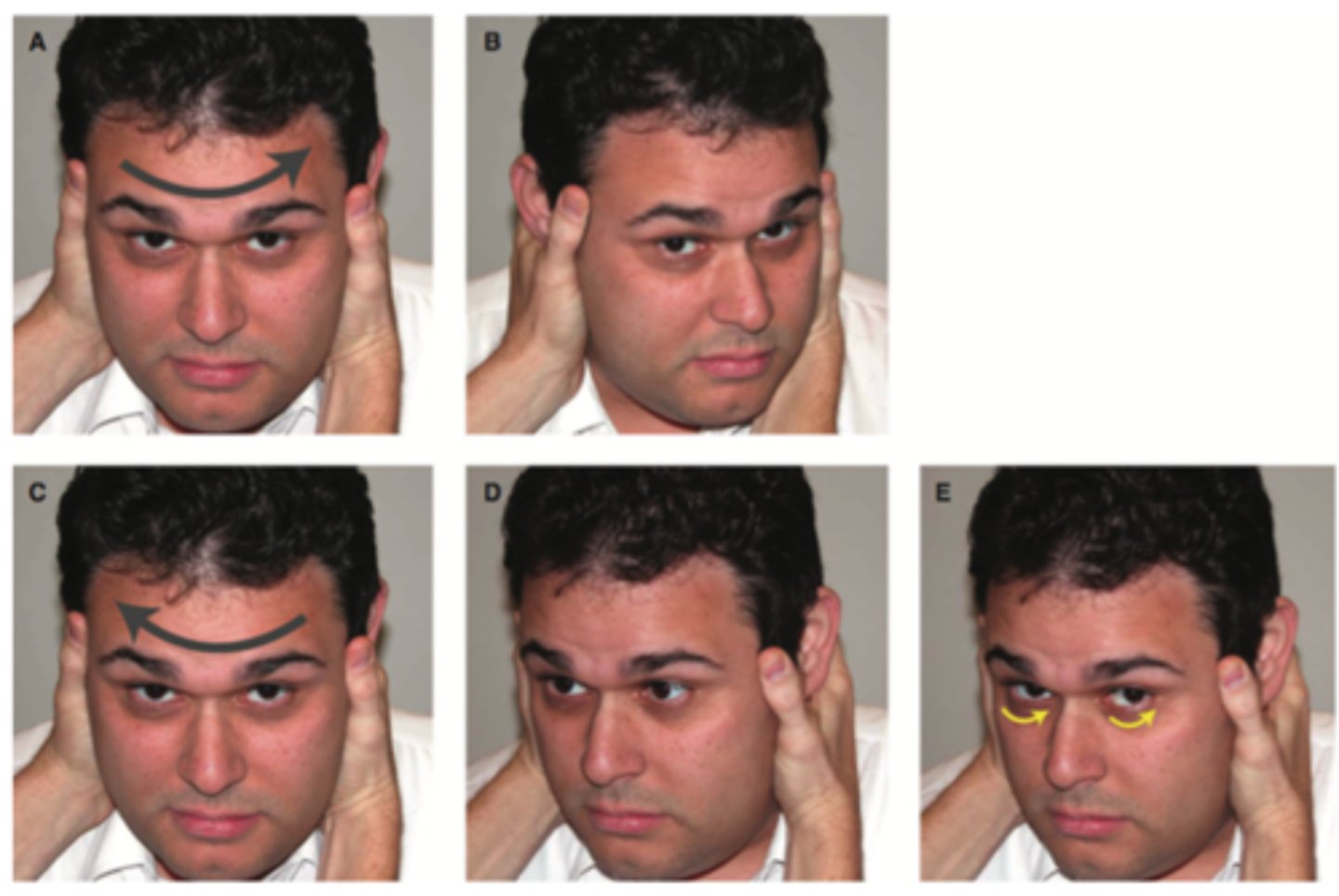
head shake test
head thrust/im[ulse
VOR
DVA
Balance (mCTSIB, CTSIB, FGA)
medical management of hypofunctions
acute: corticosteroids, vestibular suppressants/anti-nausea (not long term)
- if on suppressants (meclazine) findings will be altered, long term use interferes with recovery, recommend off 48 hours before exam
earlier
____ intervention improves outcomes in individuals with acute UVH
age; gender
outcomes for hypofunction are not affected by ____ or _____
false
T/F: saccades and smooth pursuit without head movement should be offered to improve gaze stability
2-3; 4-6; 5-7
duration of treatment for hypofunction:
- acute/subacute unilateral: ____- ____ weeks
- chronic unilateral: ____-____ weeks
- bilateral: ____-___ weeks
12; 20; 20-40
exercise dosage for hypofunction:
- acute/subacute: ____ min/day
- chronic unilateral: ___ min/day for 4-6 weeks
- bilateral: ___-___ min/day for 5-7 weeks
20; 4-6; 6-9
Balance (static & dynamic) exercise dosage for hypofunction:
- chronic unilateral: min of ____ min/day for at least ____-____ weeks
- bilateral: min of ____-____ weeks
normalization; goal; lack; unstable
indications to stop vestibular rehab:
- _____ of balance and/or gait
- symptom resolution
- _____ achievement
- plateau
- ____ of symptoms with exercise
- non-compliant/non-adherence
- fluctuating _____ vestibular symptoms
- medical/psych comorbidities preventing participation
BVH
damage to both vestibular nerves equally
- typically due to systemic causes
- ototoxicity (gentamycin, vancomycin, chemo)
- insidious onset or linked to medications
- no complaints when still/seated as long as symmetric
- oscillopsia large complaint along with unsteadiness
wobblers
people with BVD sometimes call themselves this
- they can have normal equilibrium as long as their eyes are open and all motions are performed slowly
- when moving rapidly or when eyes are closed, equilibrium is lost, resulting in a wobbly gait
no; positive
exam expectations for BVH
- ____ nystagmus or spinning sensation (as long as symmetric)
- ____ head thrust bilaterally
- severe imbalance
gaze stabilization; substitution
rehab for BVH
- oscillopsia: ____ ____ exercises
- imbalance: balance training, sensory ____, safety
central vestibular disorders
CNS dysfuction that interferes with transmission, processing, and/or integration of vestibular input
- often lesions w/in the brainstem or cerebellum
dysarthria, dysphagia, diplopia, dysdiadochokinesia, dysmetria
what are the 5 D's?
causes
___ of central vestibular dysfunction:
- stroke
- MS
- TBI
- Brain tumor
- TIA
- Cerebellar degeneration
- concussion
- vestibular migraine
spontaneous; direction; smooth
exam for central signs
- ____ nystagmus (esp downbeating or pure torsional)
- ____-changing nystagmus (does not follow alexander's law)
- impaired ocular motility (CN deficits)
- impaired ____ pursuits (jerky eye movements/saccadic intrusions)
- impaired saccades (hypo/hypermetric)
- complaints of motion sensitivity, imbalance, gaze instability
true
T/F: if PMH does not account for a central finding you need to refer to a medical provider
vestibular migraines
Dx requires: migraine with or w/o aura + vestibular sx. intense enough to interfere or prevent daily activities lasting between 5 min to 72 hrs
- can respond to regular migraine preventative treatment
- linked with other pain, inflammatory, autonomic and connective tissue comorbidities
- can be misdiagnosed as FND; different triggers (stress)
not
with vestibular migraines, an illness does ____ typically preceed a hypofunction
adaptation exercises
which exercises are best for UVH?
substitution exercises
which exercises are best for BVH?
substitution exercises
which exercises are usually best for central gaze stability issues?
DVA
how do you track progress for gaze instability?
habituation exercises
which exercises are best for motion sensitivity?
MSQ
how do you assess/track progress for motion sensitivity?
unsteadiness
treatment for _____
- balance training specific to deficits
- fall safety
- AD
CTSIB; FGA
assessments for unsteadiness
- ____, mCTSIB
- ____ > DGI
- ABC scale
hours; days
We perform the HINTS exam if someone has spontaneous nystagmus and has complaints of vertigo lasting ____ to _____
head impulse, nystagmus, and test of skew
what are the 3 tests of the HINTS exam?
true
T/F: a negative HINTS exam can r/o a stroke better than a negative MRI with difussion weighted imaging in the first 24-48 hours with specificity of 96%
head impulse test
patients with peripheral vertigo will have abnormal (positive) head impulse testing
patients with central vertigo typically have a normal (negative) head impulse test
- reassuring if abnormal (corrective saccades)
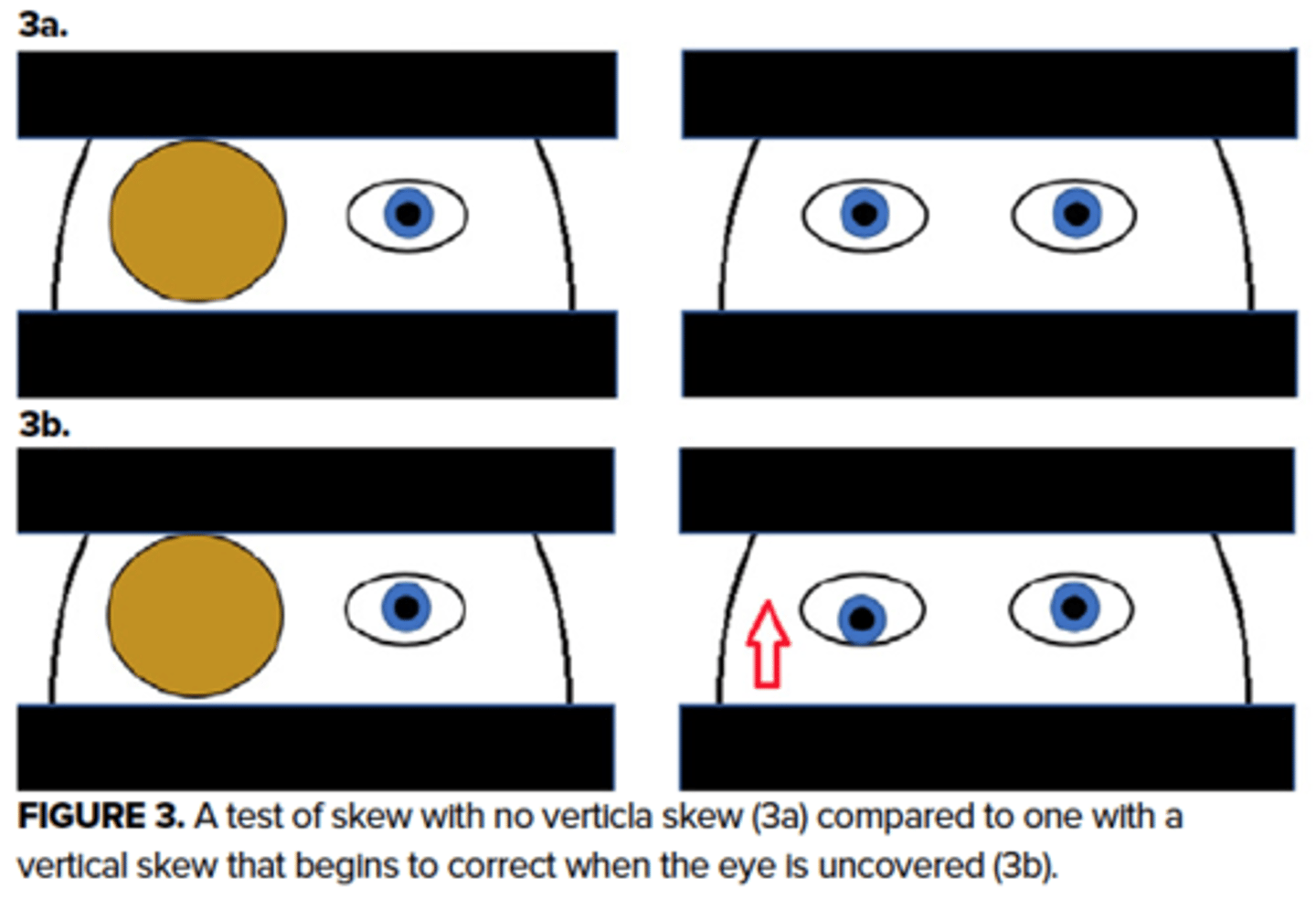
test of skew
alternative eye cover testing may reveal skew deviation in patients with central vertigo and should be absent in peripheral vertigo
- reassuring if no skew
CRM (modified epley)
used for canalithiasis for posterior BPPV