Pathophysiology Exam 1 Study Materials - Inflammation and Healing
1/241
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
242 Terms
Leading cause of death (all)
heart disease
leading cause of death - 18-30 y/o
accidents
acute disease
short term, high intensity
chronic disease
long term, low intensity
etiology
cause of disease/pathology
pathogenesis
cellular mechanism that lead to dysfunction
pathophysiology
symptoms
sensitivity
ability for a test to be positive
specificity
ability of a test to be negative in the absence of disease
highly sensitive tests tend to have more false (negatives/positives)
positives
PSA test
not specific (high PSA does not tell you if the pt has prostate cancer)
LDH test
not specific (better for monitoring, not for diagnosis)
Troponins
very sensitive and specific (heart cells with damage/death)
continuously dividing cells
skin, GI, salivary glands, epithelial cells, etc
quiescent cells
halted division: liver, kidney, pancreas, smooth muscle
non-dividing cells
cardiac, neural, skeletal muscle
ischemia
decreased blood flow to a body part --> decreased oxygen
#1 cause of cell damage
ischemia
anoxia
good blood flow but oxygen not getting there
reperfusion injury
injury to tissue that occurs after blood flow is restored due to anaerobic metabolism and free radicals
what kind(s) of toxicant is lead?
neuro: ADHD and mental retardation
nephro: inhibits vitamin D activation
bone: can interfere with bone development and growth
blood: RBC production
what kind of toxicant is carbon monoxide?
blood
what kind of toxicant is cyanide?
blood (can't use O2 despite having it)
what kind of toxicant is ethanol?
hepatic
what kind of toxicant is elemental mercury?
neuro (vaporized and inhaled)
Organic mercury
ingested from fish (takes a lot), dermal absorption: very potent
thimerosal
antifungal, controversial paper with vaccines x autism
contusion vs hematoma
contusion = bruise
hematoma = swelling/lump
exotoxin
antibiotics work, secreted by viable living bacteria
endotoxin
fever spikes with antibiotics, ruptured cell wall --> release more endotoxin = increases sickness
ionized calcium
problems with accumulated Ca, cell works hard to maintain stores (mitochondria, ER, Ca binding proteins)
dystrophic calcification
RUPTURING
malignant calcification
high intensity, short period of time, increased in PTH abnormalities
saponification
lipases --> calcium soaps --> gritty
pyknosis
clumping of the nucleus (necrosis)
karyorrhexis
fragmentation of nucleus (necrosis)
karyolysis
nuclear dissolution and chromatin lysis
coagulative necrosis
protein denaturation (aerosol chemicals/huffing = cardiotoxins --> necrosis/pallor of cardiac muscle)
liquefactive necrosis
Neurons and glial cells of the brain
caseous necrosis
only TB infections
fat necrosis
activation of lipases ex: small dense breasts
Example of small dense breasts: dystrophic cells
could be cancer --> destroys cells --> dystrophic calcification precipitation
Example of small dense breasts: saponification
BENIGN: exercising/dieting (change of microenvironment) --> increases lipases
Common condition where gangrenous necrosis may occur?
diabetes (poor circulation --> abundance of glucose --> infection)
apoptosis
programmed cell death
energy to free radical ratio in young patients
energy > free radicals
energy to free radical ratio in aging patients
energy < free radicals
algor mortis
temperature decreases in death
livor mortis
blood pools after death (helpful to see if the body was moved)
rigor mortis
rigidity, at death = limp, 24 hours = ridgid, >24 hours = limp again
postmortem autolysis
bacteria in body breaks down
hypertrophy
increase in cell size
metaplasia
changing from one type of normal cell to another type of normal cell
atrophy
decrease in cell size
hyperplasia
increase in number of cells (never in permanent cells)
dysplasia
abnormal cell growth, NOT CANCER/PRECANCER
physiologic response
expected
pathologic response
unexpected/harmful response
innate resistance
first line of defense
second line of defense
inflammation
vascular response to inflammation
blood cells dilate, increased vascular permeability and leakage, WBC adhere to inner walls of vessels and migrate through the vessels
third line of defense
adaptive (acquired) immunity
goals of inflammation
limits and controls the inflammatory process, prevent and limit infection + further damage, interact with components of the adaptive immune system, prepare the areas of injury for healing
role of chemical mediators
increased vascular permeability
effect of emigration of leukocytes
margination, pavementing, diapedesis
role of neutrophil and macrophage activation
antigen destruction and phagocytosis
T or F: different parts of the body will have different inflammation steps
FALSE: will have the same pathogenic path, inflammation is inflammation
intracellular players of inflammation
WBC, PMN/neutrophils, lymphocyte, monocyte, eosinophil, basophil, platelets, plasma proteins (compliment, clotting, kinin)
extracellular players in inflammation
mast cells (first responder), macrophages, fibroblasts
Mast cells: (does/does not) migrate; located (inside/outside) the vessel
DOES NOT, OUTSIDE
role of macrophage
garbage pick up outside the cell
role of fibroblasts
secrete collagen
vascular factors players
histamine, serotonin, nitric oxide, kinin, complement, and coagulation factors
vascular factor effect
vasodilation and increased vascular permeability
acute inflammation players
neutrophils, platelets, mast cells
chronic inflammation players
macrophages, lymphocytes (B and T)
role of cytotoxic T cells
kill infected cells
role of helper T cells
secrete cytokines (B cells, macrophages, and neutrophils) and regulate inflammation (pro or anti)
role of B lymphocytes
produce antibodies (the studiers)
Pattern recognition receptors (PRRs)
receptor on the cell membrane, recognizes patterns (lactate dehydrogenase) in our own damaged cells
pathogen-associated molecular patterns (PAMPs)
recognize specific pathogen proteins
PRR vs PAMP
PRR: tissue damage, PAMP: pathogen detected
complement receptors
communicate to cells
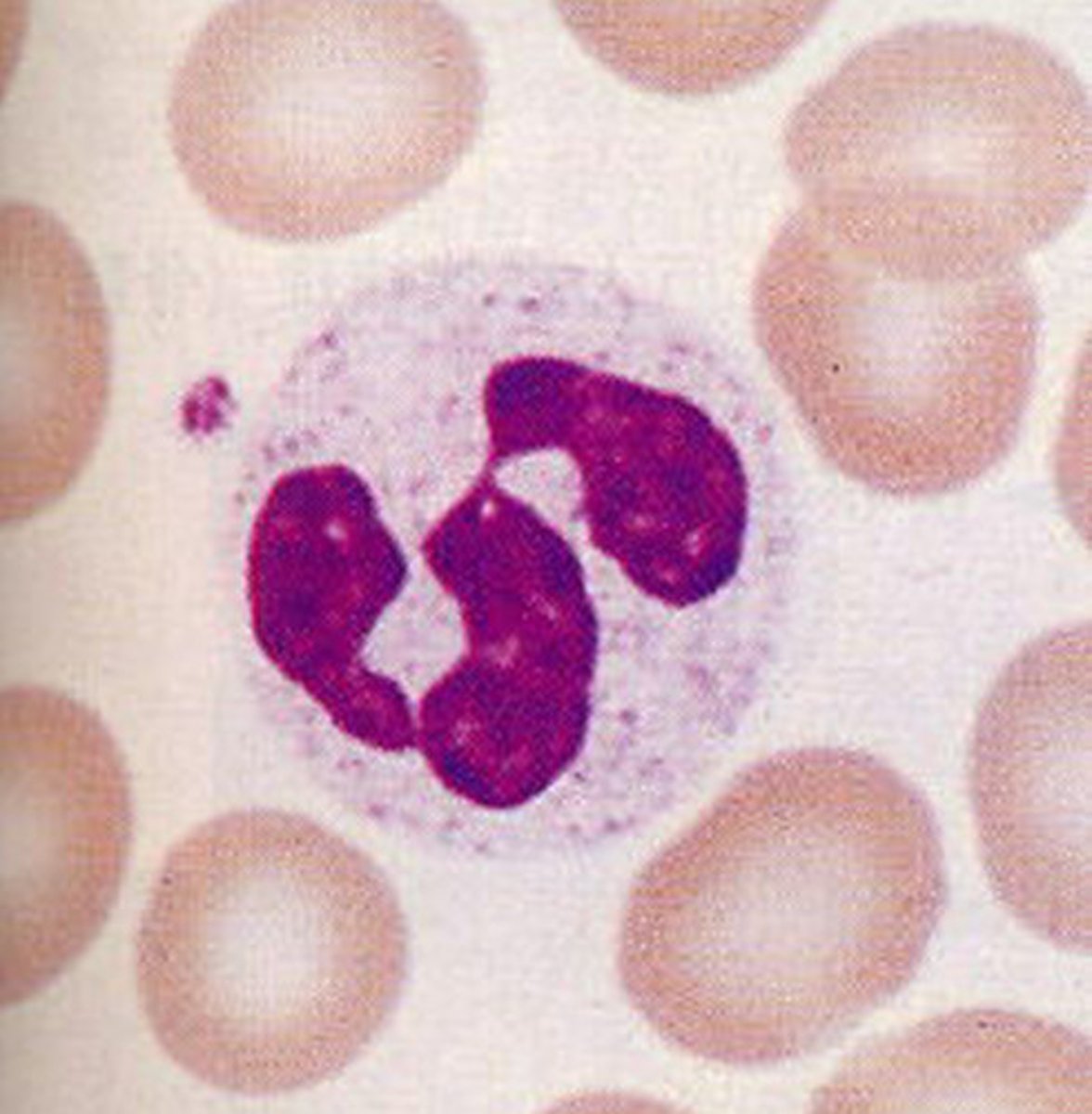
neutrophils (granule status)
granules, 3 nuclei
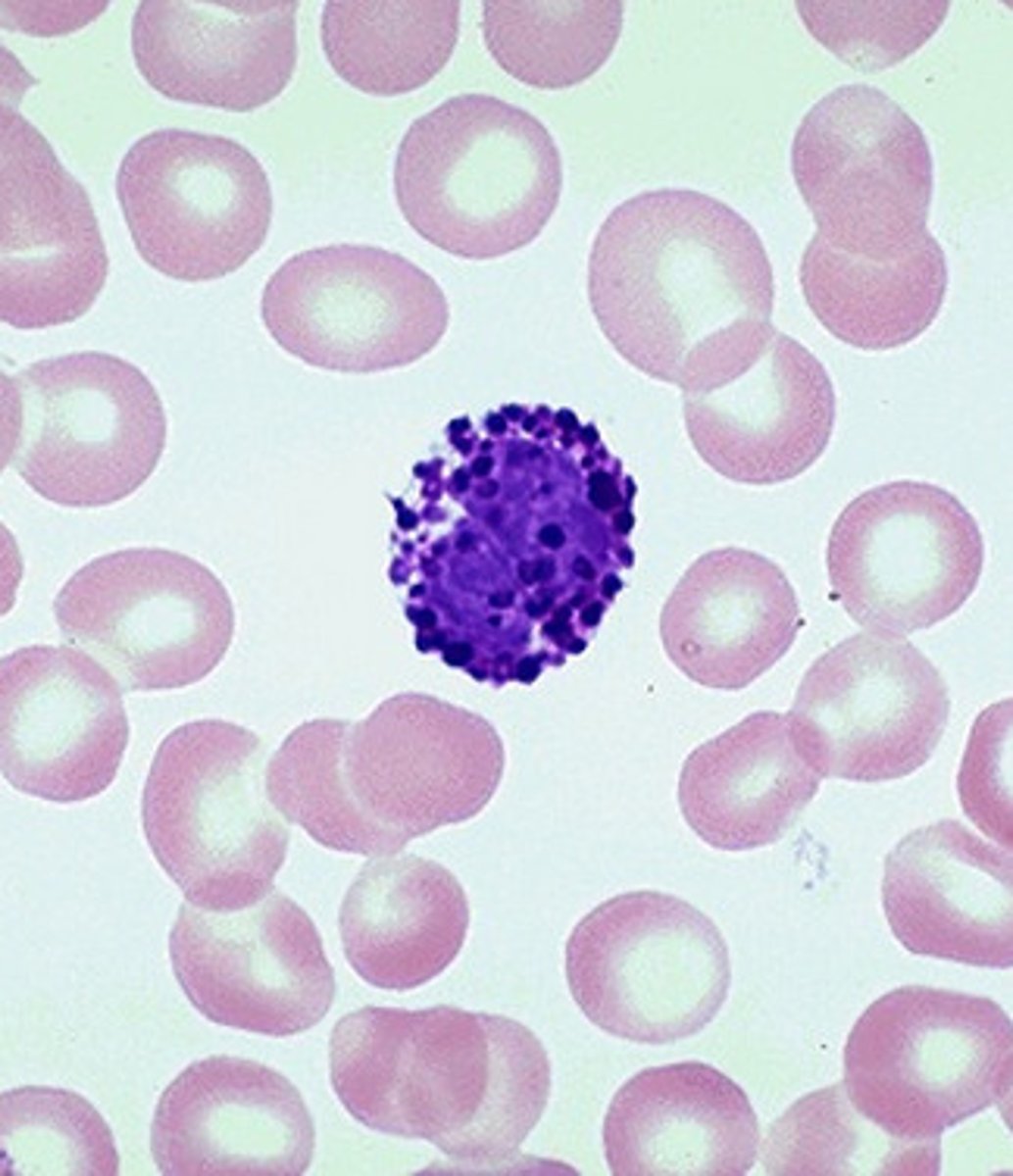
eosinophils (granule status)
granules, red/orange

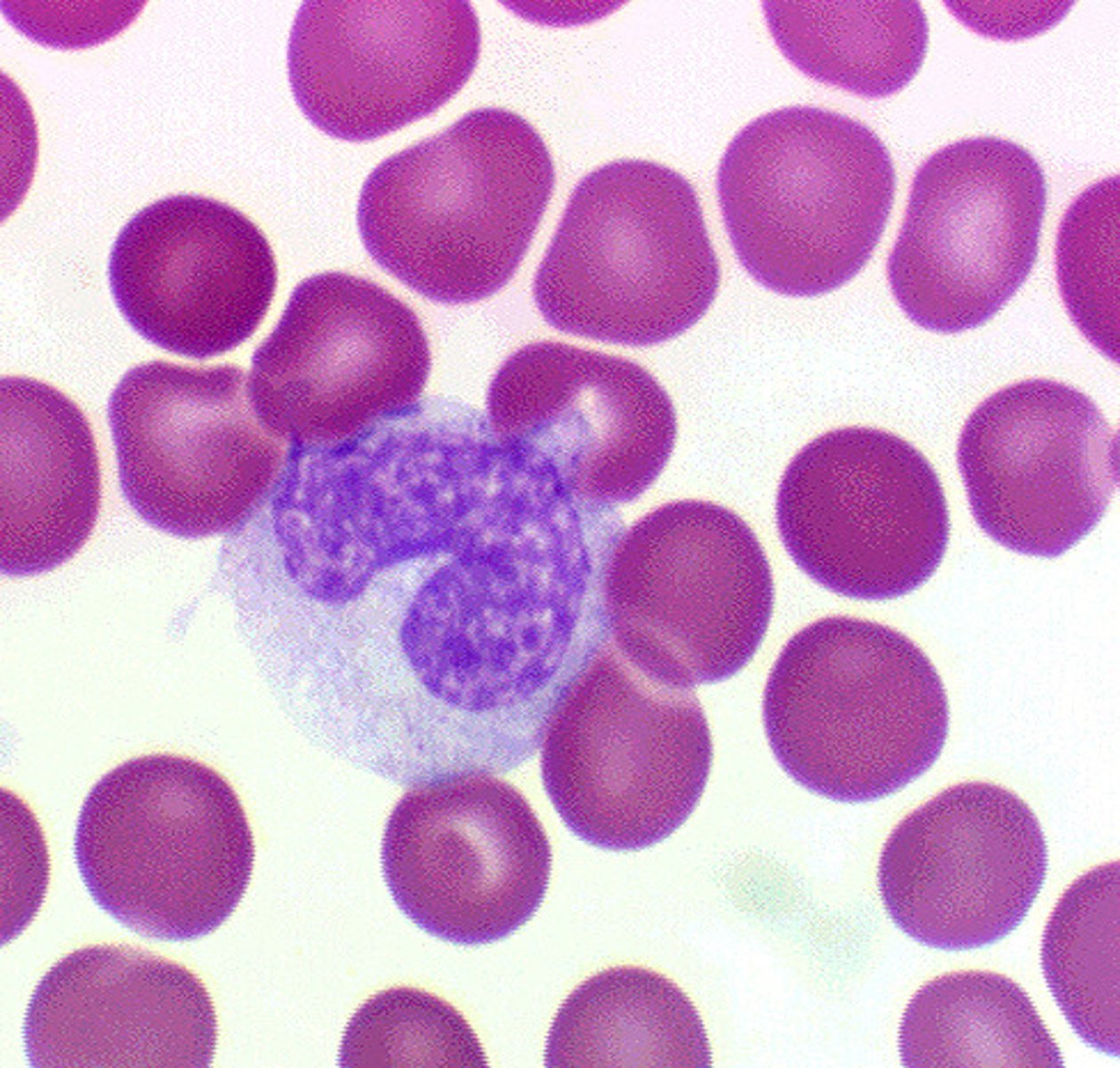
basophils (granule status)
granules, blue/purple
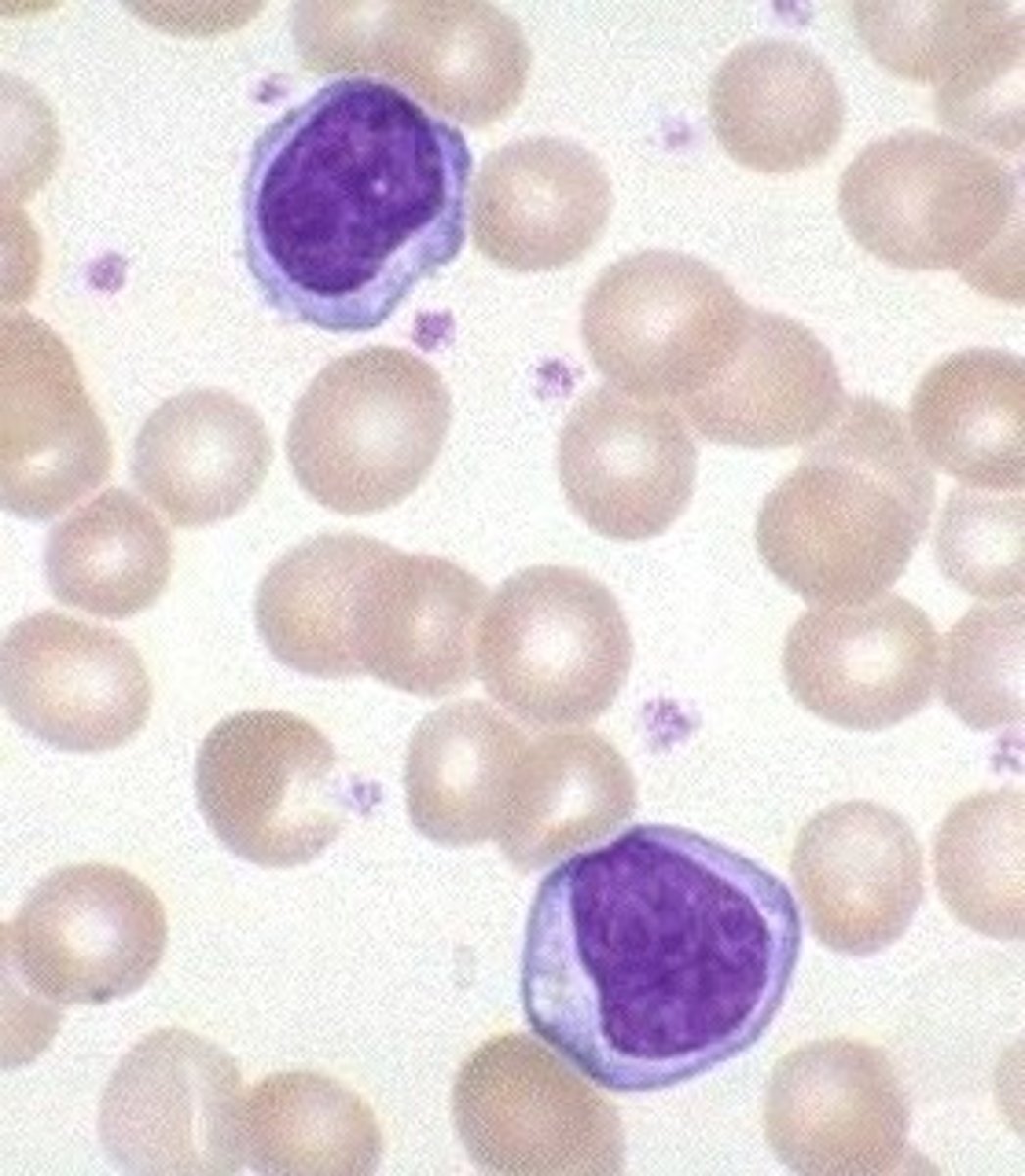
lymphocytes (granule status)
no granules, large nucleus
monocytes (granule status)
no granules, largest/rarest in blood
leukocyte mobility
very mobile, can squeeze between cells lining blood vessels by diapedesis and attack bacteria/debris
phagocytic WBCs
neutrophils, monocytes, and macrophages
role of eosinophils
allergic reactions and parasitic infections (also GERD, mono)
role of basophils
severe allergic reactions releasing histamine (promote inflammation) and heparin (blood clotting)
chronic inflammatory cells
lymphocytes, monocytes, macrophages, plasma cells (LyMMP)
acute inflammatory cells
neutrophils (PMNs, eosinophils for parasite)
where can mast cells be found?
loose connective tissue close to blood vessels --> everywhere
how are mast cells activated?
physical injury, chemical agents, immunologic processes, and receptor triggers
histamine degranulation
expels contents, exocytosis
histamine: synthesis of lipid-derived chemical mediators
takes time, not immediate response, the reason inflammation can last for days
Histamine
vasoactive amine that causes temporary, rapid dilation of blood vessels and postcapillary venules, binds to receptors
H1 receptors in blood vessels mechanism
receptors found on tunica media of blood vessels, when histamine is released from the mast cell (outside the vessel) → diffuse down towards blood vessel → binds to a receptor on the smooth muscle cells in the tunica media → relaxation → vasodilation and increased vascular permeability