Neuromuscular Diseases: Cerebral Palsy, UMN vs LMN, Guillain-Barre, Polio, and More
1/82
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
83 Terms
What is cerebral palsy?
A movement disorder caused by brain injury incurred near or at the time of birth, characterized by motor or postural abnormalities.
What does the term 'cerebral palsy' loosely translate to?
Brain paralysis.
What are the common accompanying impairments in cerebral palsy?
Speech, vision, hearing, and perceptual function impairments.
What type of paralysis is associated with cerebral palsy?
Spastic paralysis caused by loss of function of descending motor pathways.
What are the identified types of neurologic lesions in cerebral palsy?
Hemorrhage, hypoxia causing encephalopathy, malformations of the CNS, and persistence of immature layers of the primary motor cortex.
What are some prenatal risk factors for cerebral palsy?
Maternal infection with rubella or herpes, maternal diabetes or malnutrition, congenital brain anomalies.
What are some postnatal risk factors for cerebral palsy?
Meningitis, encephalitis, CVA, brain tumor, anoxia.
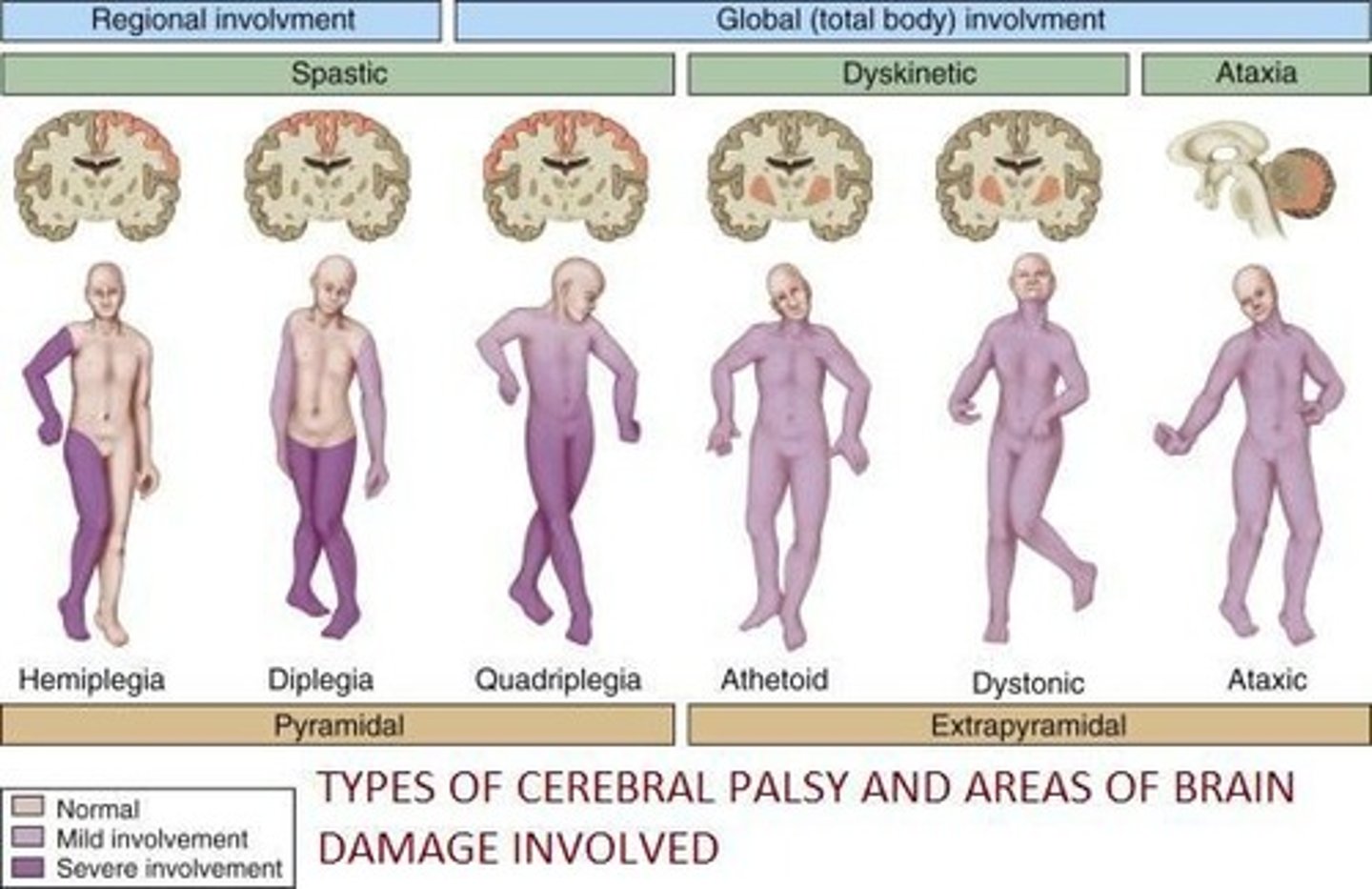
What are the classifications of cerebral palsy by muscle tone?
Hypotonia, hypertonia, ataxia, choreoathetosis, or dystonia.
What is spastic hemiplegia?
Cerebral palsy predominantly affecting one side of the body.
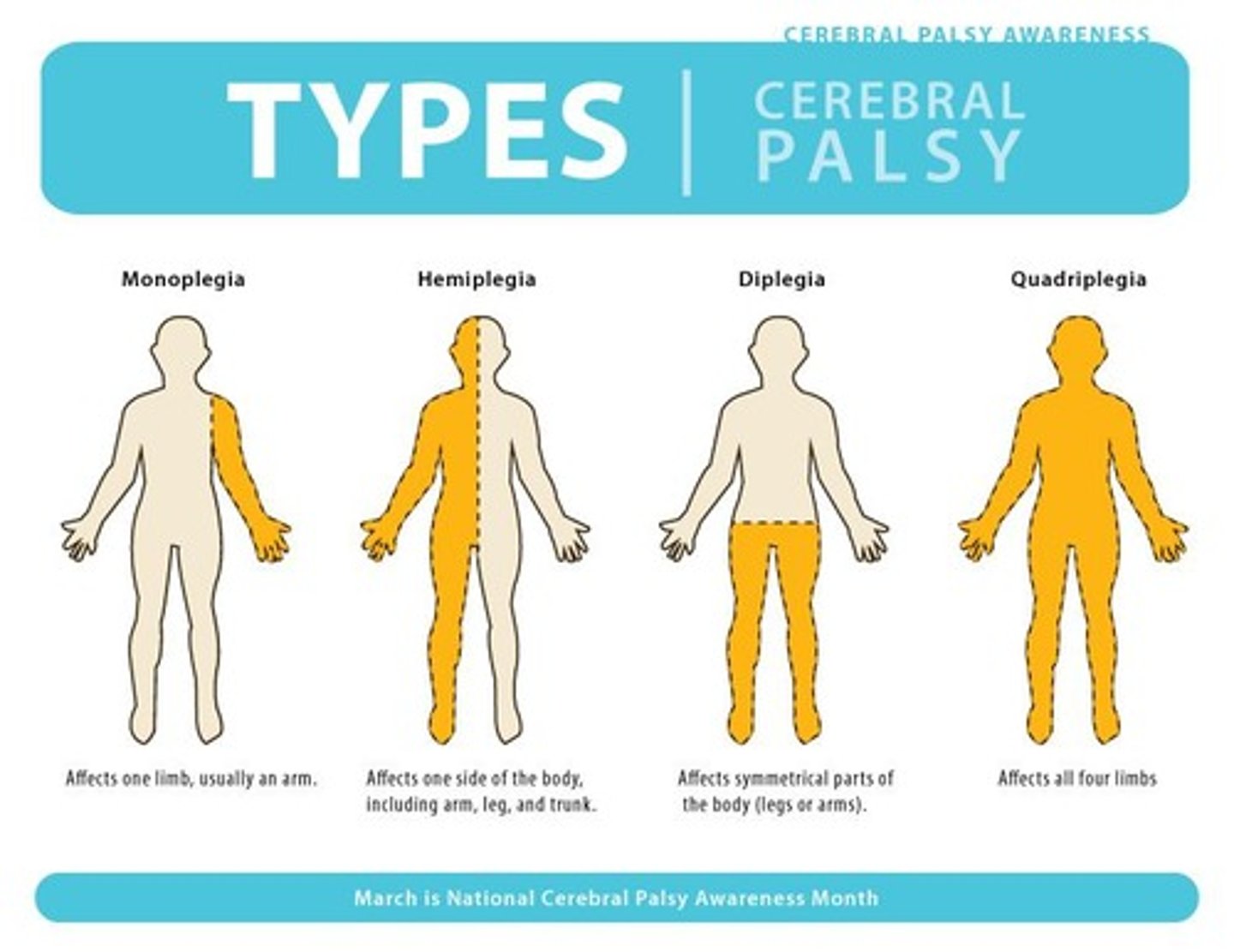
What is spastic diplegia?
Cerebral palsy affecting bilateral lower extremities more than upper extremities.
What is spastic quadriplegia?
Cerebral palsy affecting all four extremities.
What is dyskinetic cerebral palsy?
Cerebral palsy characterized by abnormal movements and hypertonicity.
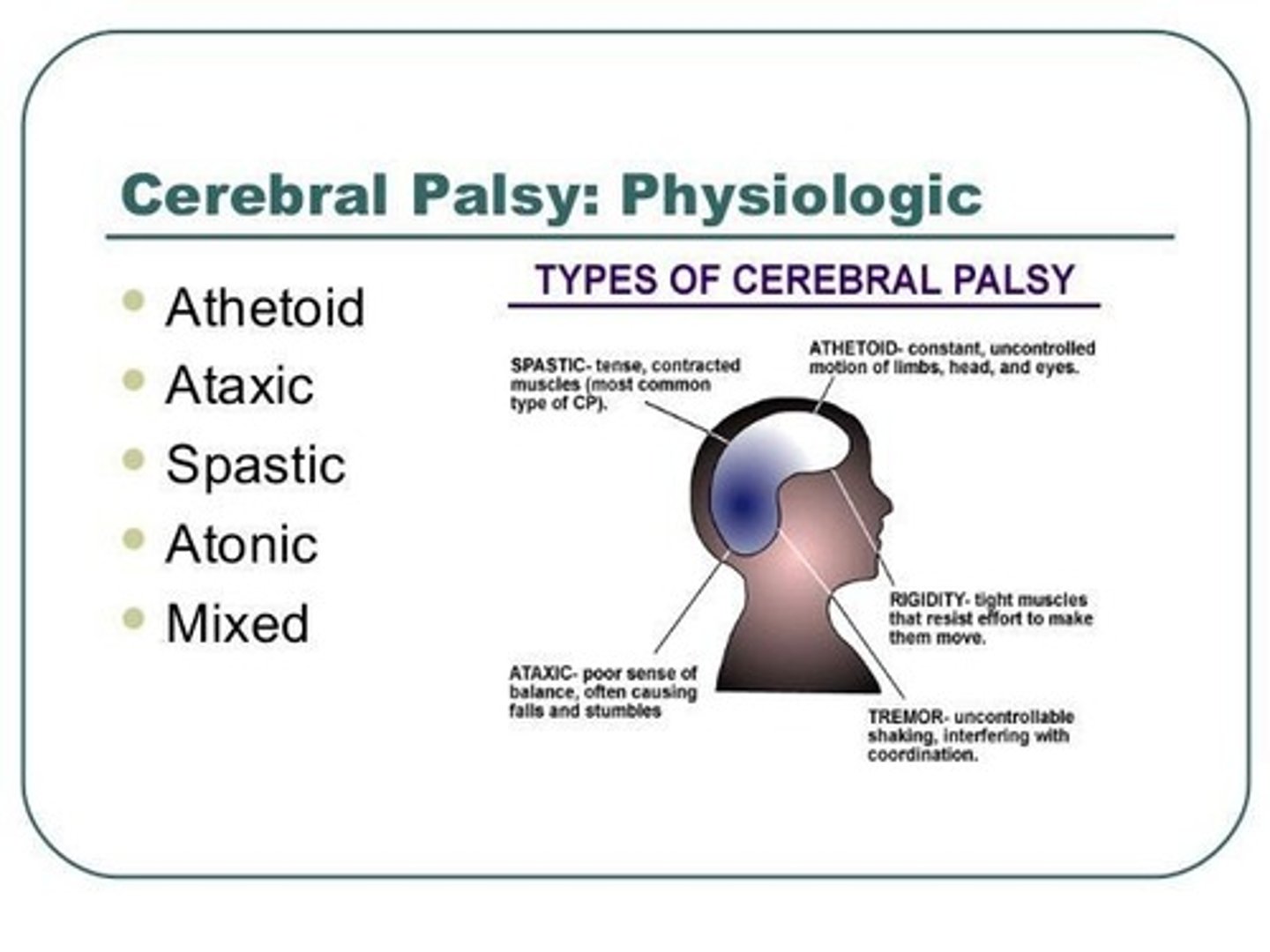
What is mixed cerebral palsy?
Cerebral palsy with no single specific tonal quality predominating, typically a mixture of spastic and dyskinetic components.
What are common clinical manifestations of cerebral palsy?
Alterations of muscle tone, delayed postural reactions, persistence of primitive reflexes, delayed motor development, abnormal motor performance.
What is the primary method for diagnosing cerebral palsy?
Observation, a good history, and a neurologic examination.
What are the components of an interdisciplinary team for treating cerebral palsy?
Physicians, therapists, nurses, special educators, psychologists, social workers, nutritionists, and family members.
What pharmacologic interventions are used for muscle spasticity?
Muscle relaxants such as baclofen, dantrolene, and diazepam.
What is the mechanism of action of baclofen?
It has an inhibitory effect on alpha motor neuron activity within the spinal cord, causing decreased firing of the alpha motor neuron.
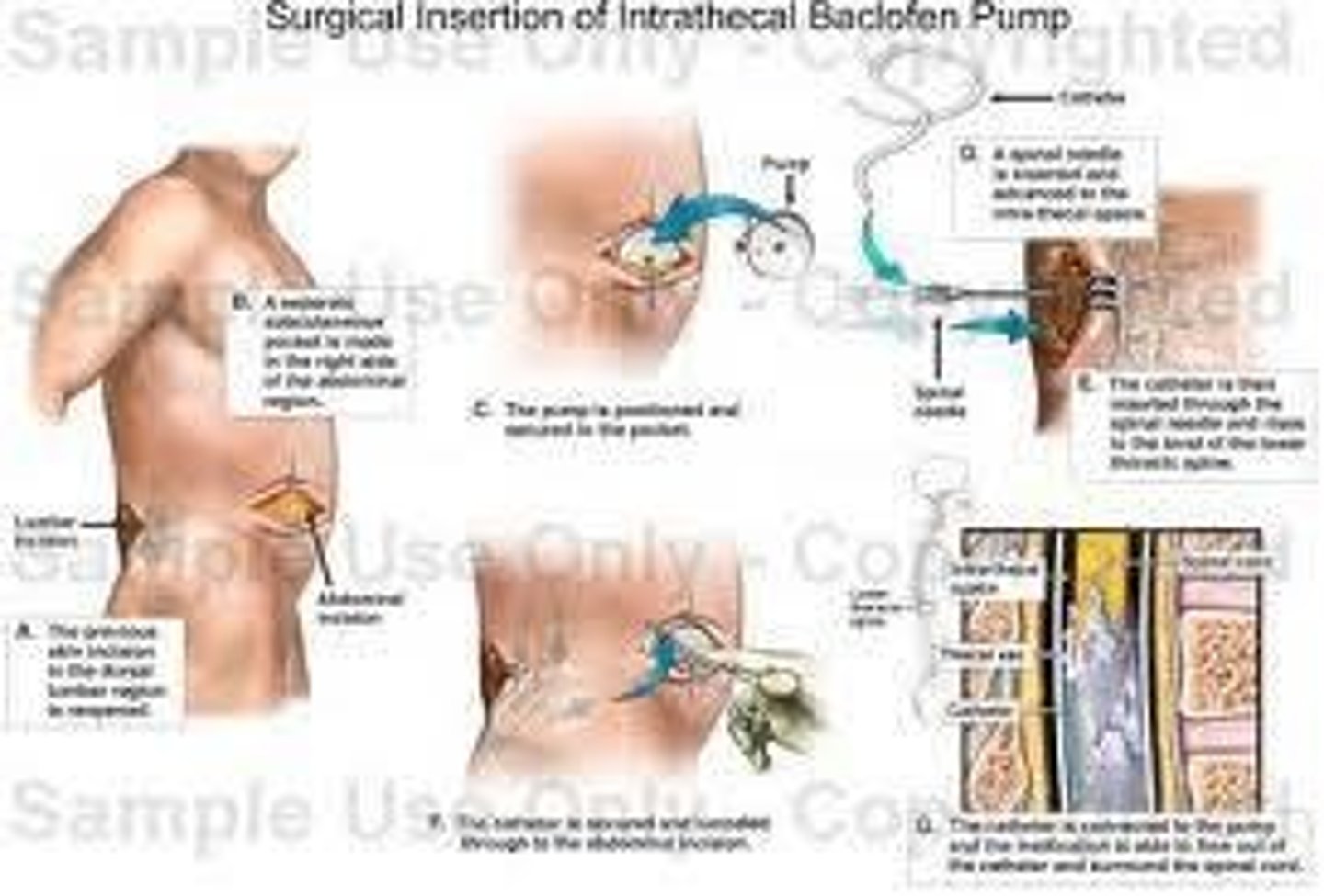
What is the purpose of a baclofen pump?
To deliver baclofen directly to the subarachnoid space surrounding a specific level of the spinal cord.
What is the role of dantrolene sodium in treating spasticity?
It impairs the release of calcium from the sarcoplasmic reticulum within the muscle cell, attenuating muscle contraction.
What are common side effects of polysynaptic inhibitors?
Drowsiness, confusion, and dizziness.
What is the expected prognosis for patients with cerebral palsy?
Motor impairments change with growth and maturation; limitations may become more apparent as a child ages.
What is the significance of primitive reflexes in cerebral palsy?
Their persistence indicates neurological impairment and may affect motor development.
What is the treatment approach for muscle lengthening in cerebral palsy?
Orthopedic surgeries such as muscle lengthening or releases, and bone procedures.
What is the function of orthotic interventions in cerebral palsy treatment?
To maintain flexibility, support or stabilize a joint, or improve alignment.
What is the role of assistive devices in physical therapy for cerebral palsy?
To aid in mobility and enhance functional independence.
What is the impact of cerebral palsy on cognitive function?
Associated disabilities may include cognitive impairments.
What is the primary action of Gabapentin?
Gabapentin raises the overall level of inhibition in the spinal cord, decreasing excitation of the alpha motor neuron and promoting skeletal muscle relaxation.
How does Tizanidine reduce spasticity?
Tizanidine inhibits spinal interneurons, resulting in decreased excitatory input onto the alpha motor neuron and subsequent reduction in spasticity.
What is the mechanism of action of Botulinum toxin?
Botulinum toxin inhibits the release of acetylcholine from presynaptic terminals at the skeletal neuromuscular junction, leading to temporary paralysis of the muscle fiber.
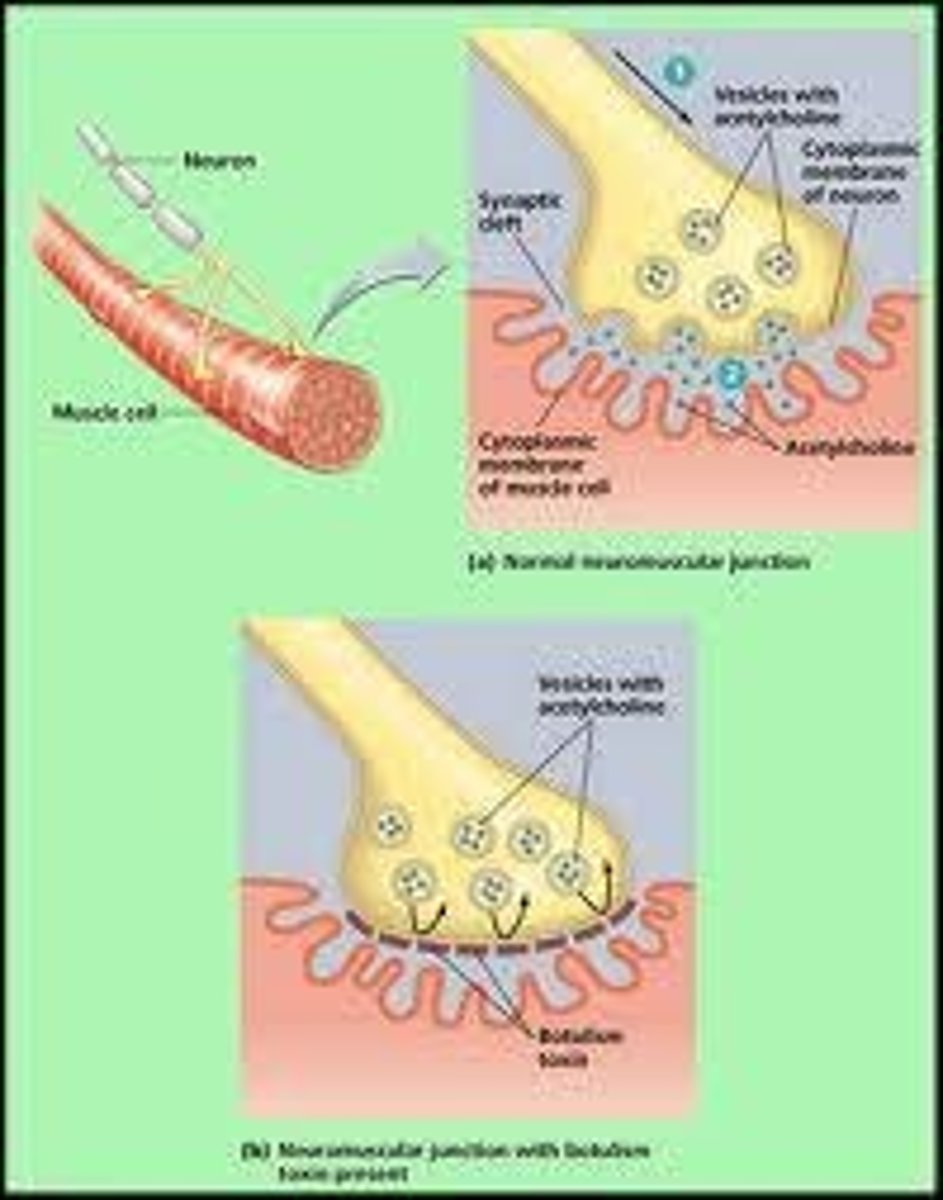
What are the clinical applications of Botulinum toxin?
Botulinum toxin is used for localized effects in certain forms of muscle hyperexcitability, such as in patients with cerebral palsy and stroke.
What distinguishes Upper Motor Neurons (UMN) from Lower Motor Neurons (LMN)?
UMN are located above the anterior horn cell, while LMN extend from the anterior horn cell to the muscle fibers.
What are acute signs of UMN lesions?
Acute signs include flaccid paralysis, areflexia, and hypotonia.
What are chronic signs of UMN lesions?
Chronic signs include spastic paresis, hypertonia, hyperreflexia, Babinski sign, clonus, and Hoffman's sign.
What are the symptoms of LMN lesions?
Symptoms include flaccid paralysis, hypotonia, muscle atrophy, areflexia, fasciculation, and fibrillation.
What is the difference in muscle tone between UMN and LMN weakness?
UMN weakness is characterized by increased tone, while LMN weakness shows decreased tone.
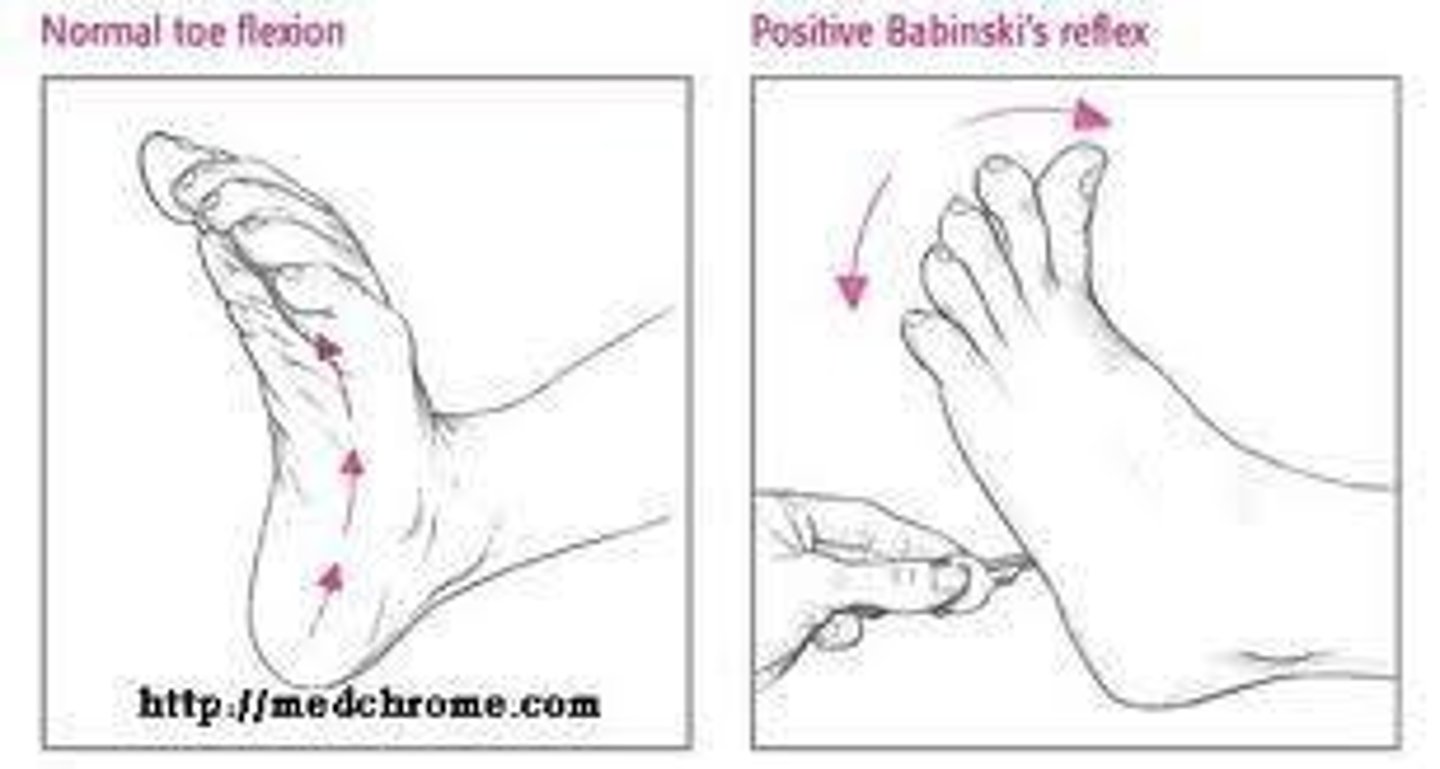
What does a positive Babinski sign indicate?
A positive Babinski sign indicates an Upper Motor Neuron lesion.
What is cervical spondylosis?
Cervical spondylosis is degenerative arthritis or osteoarthritis of the spinal vertebrae and related tissue, often leading to spinal cord root compression.
What are common symptoms of cervical spondylosis?
Symptoms include clumsy or weak hands, leg weakness or stiffness, neck stiffness, pain in shoulders or arms, and unsteady gait.
What are the signs of cervical spondylosis?
Signs include atrophy of hand musculature, hyperreflexia, sensory loss, and Lhermitte's sign.
What treatments are available for cervical spondylosis?
Treatments include anti-inflammatory drugs, muscle relaxants, mild analgesics, and decompressive laminectomy.
What is the most common cause of nerve root disorders?
A herniated intervertebral disk is the most common cause of nerve root disorders.
What are the symptoms of nerve root disorders?
Symptoms include sensory impairment in a dermatomal distribution, weakness, atrophy of muscles, and depressed or absent segmental deep tendon reflexes.
What is poliomyelitis?
Poliomyelitis is an acute inflammatory viral infection of Lower Motor Neurons caused by the poliovirus.
What percentage of poliovirus infections are asymptomatic?
95% of poliovirus infections are subclinical and often asymptomatic.
What are the potential outcomes for individuals who experience paralysis from poliomyelitis?
Outcomes include complete recovery, mild residual paralysis, or moderate to severe paralysis.
What is Post Polio Syndrome (PPS)?
Post Polio Syndrome refers to new symptoms that occur decades after the initial paralytic episode of poliomyelitis.
What precautions should be taken for patients with Post Polio Syndrome?
Patients should limit activity if it provokes or worsens symptoms.
What is the significance of the NYT article titled 'The Polio Generation'?
The article discusses the memories of polio survivors and the impact of vaccine rollout in the 1950s and 60s.
What is the role of assistive devices in the management of polio survivors?
Assistive devices and bracing are used to support mobility and function in polio survivors.
What is the importance of ongoing polio vaccination?
Ongoing polio vaccination is crucial to prevent outbreaks and protect unvaccinated individuals from infection.
What interventions are included in physical therapy for nerve root disorders?
Interventions include posture and body mechanics training, stretching and strengthening exercises, and pain management.
What is Spinal Muscular Atrophy (SMA)?
A fatal autosomal recessive disorder characterized by anterior horn cell degeneration leading to progressive weakness and skeletal muscle wasting.
What are the three types of Spinal Muscular Atrophy?
Type I (Werdnig-Hoffmann Disease), Type II (Intermediate), and Type III (Kugelberg-Welander Disease).
What is the most severe form of SMA?
Werdnig-Hoffmann Disease.
What are the symptoms of Werdnig-Hoffmann Disease?
Flaccid quadriplegia, difficulty breathing, poor feeding, and weak cry.
What is Kugelberg-Welander Disease?
A mild form of SMA that begins in proximal muscles and progresses to distal muscles, typically starting between ages 3-20.
What diagnostic methods confirm SMA?
Muscle biopsy and electromyography (EMG).
What is Herpes Zoster (Shingles)?
An acute inflammatory reaction caused by the herpes simplex virus, characterized by pain, itching, and vesicular eruptions limited to dermatomes.
What are the potential complications of Herpes Zoster?
Post-herpetic neuralgia, which includes pain and increased sensitivity to pressure.
What is Guillain-Barre Syndrome?
An autoimmune disease affecting the peripheral nervous system, often triggered by an acute infectious process, leading to flaccid paralysis and areflexia.
What are the initial symptoms of Guillain-Barre Syndrome?
Symmetric weakness that begins in the legs and ascends to the trunk and upper extremities.
What is the typical progression of weakness in Guillain-Barre Syndrome?
Maximal weakness usually occurs within 2-3 weeks, with recovery being a slower process.
What diagnostic tests are used for Guillain-Barre Syndrome?
EMG, nerve conduction velocity studies, and lumbar puncture showing increased protein without increased white blood cells.
What treatments are available for Guillain-Barre Syndrome?
Plasmapheresis and intravenous immunoglobulin (IVIG).
What is Neurofibromatosis?
An autosomal dominant disorder characterized by noncancerous tumors along nerves.
What are the two types of Neurofibromatosis?
Type 1 (NF1) and Type 2 (NF2).
What are the diagnostic criteria for Type 1 Neurofibromatosis?
Presence of 6 or more café-au-lait spots, freckling in certain areas, 2 or more neurofibromas, optic gliomas, or a first-degree relative with NF1.
What is Amyotrophic Lateral Sclerosis (ALS)?
A progressive neurodegenerative disease affecting motor neurons, leading to muscle weakness and wasting without sensory deficits.
What are the common symptoms of ALS?
Slurred speech, difficulty swallowing, muscle weakness, and frequent falls.
What is the typical age of onset for ALS?
Between ages 50 and 70, more common in men.
What are the two FDA-approved drugs for ALS?
Riluzole and Edaravone.
What is the prognosis for ALS?
The disease is relentlessly progressive, typically leading to death from respiratory failure within 3 to 5 years.
What is the role of physical therapy in managing ALS?
To assist with respiratory strategies, skin care, mobility, and maintaining the highest level of function.
What is the connection between Guillain-Barre Syndrome and Zika virus?
Cases related to Zika seem to progress faster than typical Guillain-Barre Syndrome.
What are the signs of respiratory failure in Guillain-Barre Syndrome?
Weakness reaching respiratory musculature may require ventilation for breathing support.
What is the significance of café-au-lait spots in Neurofibromatosis?
Presence of more than 5 spots larger than 5mm can be a diagnostic criterion for NF1.
What are the common interventions for SMA?
Respiratory care, pulmonary hygiene, mobility training, and assistive device instruction.
What is the expected recovery rate for Guillain-Barre Syndrome?
Approximately 85% of patients achieve full recovery, but relapses are possible.
What is the role of macrophages in Guillain-Barre Syndrome?
Macrophages strip myelin from nerves, leading to degeneration.
What are the common symptoms of post-herpetic neuralgia?
Pain and increased sensitivity to pressure following a shingles outbreak.
What is the typical age range for Kugelberg-Welander Disease onset?
Between ages 3 and 20.
What is the main characteristic of Type 2 Neurofibromatosis?
Bilateral vestibular schwannomas and multiple meningiomas.