PSYC 301: Psychiatric Disorders
1/84
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
85 Terms
Psychiatric Dysfunction
what are motivating factors for classifying psychiatric illnesses?
1) guide treatment choices
2) allow clinicians to communicate
3) serve parties who require diagnosis (insurance, CFA, legal)
4) permit research (causes, treatment, prognosis)
what are the three components that a condition must have to be included
in the DSM?
atheoretical
operationalist
categorical
what are criticisms of the DSM criteria?
heterogeneity of criteria
level of detail
overlap
authority
comparator (compare to self, norm, or none)
what are normative assumptions?
evaluation of right or wrong
ex: ought, should
what is deinstitutionalization?
movement to replace long-stay psychiatric facilities w/ community mental health services
what are historical examples & trends of normative assumptions?
homosexuality was classified as a disorder in DSM-I & -II & removed for DSM-III following gay activist protests at APA annual meetings & pressure from the gay PA
what are historical examples & trends of deinstitutionalization?
movement started in 1950s & 60s
w/out support, people w/ mental illness are at higher risk of incarceration (unhoused)
what is the relationship between mental illness and violence?
in absence of substance use disorder, people w/ mental illness are not more violent than other from their same neighbourhoods
controlling for poverty
Psychiatric Dysfunction: Schizophrenia
what is the main criteria that goes into a diagnosis of schizophrenia?
2+ of the following, present for a significant amount of time during a 1 month period
1 must be (1), (2), or (3):
1) delusions
2) hallucinations
3) disorganized speech (frequent derailment or incoherence)
4) grossly disorganized or catatonic behaviour
5) negative symptoms (diminished emotional expression or avolition)
what must the disturbance affect to qualify for the DSM-5 criteria?
level of functioning
ex: work, interpersonal relations, or selfcare
what must the disturbance show to qualify for the DSM-5 criteria?
continuous signs, persisting for at least 6 months
what must be ruled out to qualify for the DSM-5 criteria?
schizoaffective disorders
disturbance is not attributable to physiological effects of a substance or another medical condition
what are positive & negative symptoms of schizophrenia?
positive: hallucinations &/or delusions
negative: blunted emotional responses, impoverished content of thought & speech, reduced social motivation
what are hallucinations?
perceptions w/out sensory cause
often auditory - voices, noises, music
command hallucinations => high risk of harm (suicide)
what are delusions?
beliefs that are not realistic or culturally appropriate
variable
the world is full of hidden signs for me; i am being watched
what are symptoms of cognitive abnormalities?
impaired working memory & executive function
impaired source monitoring: tendency to misattribute own actions & thoughts to external causes
what are risk factors for schizophrenia?
genetics
urban environment
1st or 2nd trimester maternal infection or malnutrition
perinatal complications
cannabis or stimulant use
paternal age > 35 y/o
what are common structural brain changes in schizophrenia?
widespread decreased grey matter in frontal & temporal cortices
pronounced thinning of dlPFC (working memory)
what does this volume loss result in?
enlarged ventricles
what is the mechanism of volume loss?
reduction in cell processes (axons & dendrites)
what are structural changes in the prefrontal cortex?
loss of dendritic spine density
fewer GABAergic interneurons
what are structural changes in the hippocampus?
atypical layering structure
atypical neuron shape
what are functional brain changes in schizophrenia?
abnormal (often hypoactive) frontal & temporal lobes including hippocampus
what is the efficacy of nonpharmacological treatments for schizophrenia?
CBT shown promise for managing positive & negative symptoms when combined w/ medication
what is the efficacy for pharmacological treatments for schizophrenia?
antipsychotic drugs (positive symptoms)
less luck in treating negative symptoms
what is the dopamine theory of schizophrenia?
maybe it’s caused by too much activity at dopamine receptors
what are the 3 findings that the dopamine theory is based on?
1) brains w/ parkinson’s have marked dopamine depletion; & antipsychotics produce symptoms that are similar to parkinson’s
2) drugs known to increase dopamine levels (amphetamine, cocaine) produce symptoms of schizophrenia
3) efficacy of antipsychotics are correlated w/ the degree to which it blocks activity at dopamine D2 receptors
what are 3 major problems w/ the dopamine theory?
1) newer “atypical” antipsychotic drugs produce a wide variety of changes in the brain & were just as good as traditional antipsychotics
2) takes 2-3 weeks for antipsychotics to work, yet their effects on dopamine receptor activity are immediate
3) most patients show no significant improvement to the 1st antipsychotic they are given
what is the finding of glutamate hypofunction theory of schizophrenia?
PCP & ketamine can induce negative symptoms & psychosis & act antagonistically upon NDMA receptors
what happens if glutamate signaling becomes abnormal?
can lead to:
1) less GABAergic transmission
2) widespread pattern of too much activity
Bipolar Disorder
what is a depressive state?
new or worsened, daily, for 2 weeks in a row & 5+ of:
depressed mood
loss of interest or pleasure in almost all activities
weight or appetite changes
sleep changes
psychomotor changes (agitated or slowed)
tiredness, fatigue, low energy
sense of worthlessness or guilt
impaired ability to think
recurrent thoughts of death, suicidal ideation, or suicide attempts
what is a hypomanic state?
abnormal, persistent elevated, expansive, or irritable mood & increased goal-directed activity or energy, most of the time for at least 4 days
increased activity
persistent mild elevation of mood
marked feelings of well-being & both physical & mental efficiency
increased sociability & talkativeness (or increased irritability)
increased sexual energy
decreased need for sleep
to what degree does a hypomanic state affect ones functioning?
no severe disruptions of work or result in social rejection & no + symptoms (psychosis)
what is a manic state?
abnormal, persistent elevated or expansive mood & increased goal-directed activity or energy, most of the time, for at least 1 week
3 or more of:
inflated self-esteem or grandiosity
decreased need for sleep
more talkative than usual or pressure to keep talking
flight of ideas or subjective experience that thoughts are racing
distractibility
increase in goal-directed activity or psychomotor agitation
excessive involvement in activities that have a high potential for painful consequences
how do mood disturbances affect those in a manic state?
mood disturbance causes marked impairment in social or work life, needs hospitalization, or includes psychosis
what is bipolar I?
at least 1 major depressive episode
at 1 event of manic episode
what is bipolar II?
at least 1 major depressive episode
at least 1 hypomanic episode
what is the prevalence of BD?
.6% bipolar I & .4% bipolar II vs. 12.5% MDD
commonly begins in young adulthood
potential high impact
what is the life course of BD?
depressive episode is commonly the 1st mood event
pre-drome: smaller mood events outside of norm but not yet meet criteria
after both negative mood & mania has occurred then it’s possible to receive a diagnosis
what is the reward hypersensitivity model of BD?
according to this model, hypersensitive to reward is the trait that predisposes someone to developing BD
what does hypersensitive to rewards mean?
reward system responds very strongly when goals are attained or experiences a reward
according to the hypersensitivity model of BD, what can goal attainment can lead to?
loop: goal attainment => excessive reward state => behaviour or cognitive changes => ultimately (hypo)mania episodes
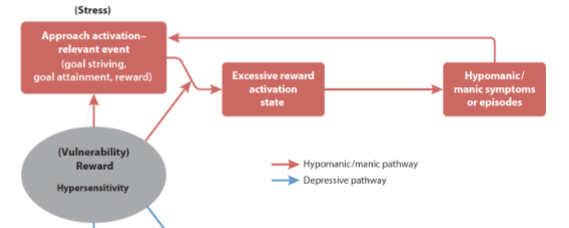
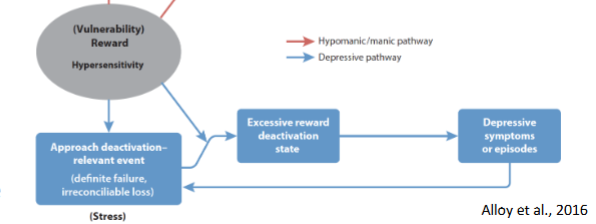
what happens if goal is not attained?
excessive deactivation of reward pathway => producing depressive state
what is the evidence of the reward hypersensitivity model of BD?
euthymic individuals w/ BD
prodromal features for hypomania, mania & depressive episodes
teens who score high on reward sensitivity are more likely to develop BD in a prospective study
what is the evidence for euthymic individuals?
excessive activity in frontal-striatal reward-related areas in responses to reward-related cues
make more risky choices than controls (gambling)
what is the evidence for prodromal features of hypomania & mania episodes?
excessive goal setting & increased success expectancies
what is the evidence for prodromal features of depressive episodes?
decreased motivation & goal setting & low self-confidence
what is a structural brain change associated w/ BD?
reductions in gray matter
what is this structural change driven by?
time spent in manic episodes, which are associated w/ neuroinflammation, stress hormones
what are functional brain changes associated w/ BD?
increased responsiveness in limbic & para-limbic areas
decreased responsiveness in areas associated w/ cognitive control
what are areas in the limbic & para-limbic system?
amygdala
ventrolateral prefrontal cortex (VLPFC)
ventral anterior cingulate cortex (ACC)
what are areas associated w/ cognitive control?
dorsal anterior cingulate cortex (ACC)
dorsomedial prefrontal cortex (DMPFC)
dorsolateral prefrontal cortex (DLPFC)
what are treatment options for BD?
mood stabilizers
atypical antipsychotics
psychotherapy
what psychotherapy have some evidence for treating BD?
CBT
health education
family-focused
Psychiatric Dysfunction: Executive (Dys)functions
what is the tripartite model of executive function?
cognitive control of behaviour
involving prefrontal cortex and/or associated projections
what tests are used to measure executive function?
judgment tests
verbal fluency
luria’s 3 step test
trail-making or drawing patterns
clock drawing “10 past 11”
what are the 3 components of the tripartite model of executive function?
1) working memory: holding & mental working w/ info in mind
2) inhibitory control: resisting temptations, not acting impulsively or prematurely, overriding automatic behaviour
3) cognitive flexibility: fluidly changing perspectives or approaches to solving a problem, adjusting to new demands switching between priorities or tasks
what test is used for working memory?
digit or pointing span
how many can you rememeber?
what are 2 tests used for inhibitory control?
stroop: blue, yellow, red, black, purple (words written in different colours)
flanker task: arrows are either congruent, incongruent or neutral (point in same, different direction or 1 arrow)
what are 2 tests used for cognitive flexibility?
wisconsin card sort (must adapt to changing rules)
trail-making w/ alternation (A, 1, B, 2, C, 3)
what are higher order “executive functions”?
3 core components depend on:
planning
organizing
multi-tasking
self-awareness
regulating emotions
inhibiting inappropriate behaviour
motivation
concentrating
what is neuropsychiatric syndrome of frontal lobe damage?
abulia
what is abulia?
lack of motivation
return to primitive reflexes
ultilization behaviour
ex: seeing glasses in front & putting them on even though they already have glasses on
what are 3 frontal-subcortical loops marking subcortical differences between the dorsolateral, orbitofrontal, & medial cortex?
executive dysfunction
apathy
disinihibition
which is area is linked w/ executive dysfunction?
dorsolateral prefrontal cortex
what sub-cortical regions are involved in executive dysfunction?
dorsolateral prefrontal cortex
caudate nucleus
globus pallidus
thalamus
which area is linked w/ apathy?
medial frontal cortex
what sub-cortical regions are involved in apathy?
medial frontal cortex
nucleus accumbens
globus pallidus
thalamus
which area is linked w/ disinhibition?
orbitofrontal cortex
what sub-cortical regions are involved in disinhibition?
orbitofrontal cortex
caudate nucleus
globus pallidus
thalamus
what does dysfunction in the orbitofrontal circuit lead to?
impulsivity
socially inappropriate
poor safety judgment ex: walking out into traffic w/out looking
difficulty evaluating anticipated rewards & punishments
don’t “learn from mistakes” due to diminished guilt & regret
what does dysfunction in the dorsolateral circuit lead to?
distractible
disorganized
perseverative: completing action using old rule even when it no longer applies
difficulty multitasking
poor time management & prioritization
what does dysfunction in the medial frontal circuit lead to?
emotion dysregulation: loss of empathy & blunted affect
apathy (loss of “get up & go”)
rigidity in thoughts & actions, poor ability to learn from mistakes
problems thinking ahead, sequencing steps for a task
what are major symptoms of ADHD?
extreme inattention
hyperactivity
impulsivity
how was ADHD previously characterized & how has it changed since then?
initially characterized as a problem of “moral control” => pathologizing not conformity
diagnosis intersects w/ societal norms (not just bio) => mismatch between environment & personality
shaped by culture & how society thinks we “should” behave, learn, perform
what are trends influencing ADHD diagnoses?
younger children in a classroom => more likely to get diagnosed (environmental mismatch)
rapid rise in adult diagnoses => changing social norms & diagnostics
symptom presentation vary w/ gender => girls underdiagnosed
externalizing behaviours (aggression) more likely to receive diagnosis => typically more common in boys
dysfunction is more severe in girls bc the point where they receive a diagnosis is when they are really struggling
what is the neurobiology of ADHD?
reduced activity & volume of PFC
what is the evidence supporting reduced activity of PFC?
those w/ ADHD don’t show orbitofrontal activity when withholding a response
planning & withholding task
what is the evidence supporting reduce volume of PFC?
slower maturation of PFC
normal cortical thinning is slower between ages 8-17
but in ADHD PFC is already thinner which is correlated w/ hyperactivity / impulsivity
what is the dual-pathway model of ADHD?
executive circuit (dysfunction: inattention)
dlPFC & caudate
reward circuit (dysfunction: lack of motivation)
OFC, ACC, & nucleus accumbens
explains differences in symptoms presentation bc people can have either 1 or 2 or both
what are treatments for ADHD?
evidence that those w/ ADHD have a hypoactive dopamine system
medication that act upon dopamine & norepinephrine systems in PFC & subcortical structures to inhibit reuptake