CMS exam 1
1/41
Earn XP
Description and Tags
testing on: concept, patient SE, treatment. all select-alls have at least 2 answers. often all 5.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
42 Terms
pH
normal for humans: 7.35-7.45
acidosis: many H ions, <7,35
alkalosis: few H ions, >7.45
acid: compound that allows H ions to break free (low pH)
base: compound that binds w H ions (high pH)
lungs control CO2 (acid potential). kidneys control bicarb by reabsorbing or not (alkalotic potential)
buffer systems
chemical buffer system keeps pH constant
phosphate buffer system
protein buffer system
chemical buffer system
carbonic acid - bicarbonate buffer system
carbonic acid (acid) - H2CO3 (CO2 + H2O).
bicarbonate (base) - HCO3
increases w CO2. eating many carbs. high metabolic action (like fever)
resp control (CO2 changes)
changes quickly, seconds-minutes
if acidic (many H), resp rate and depth increase to release CO2
if alkaline (few H), RR and depth decrease to hold onto CO2
renal control (metabolic HCO3 changes)
slower
if acidic, H+ excreted in urine
if alkaline, HCO3 excreted in urine
if resp broken, renal compensates and vise versa
acid base disturbances
resp acidosis, metabolic acidosis, resp alkalosis, metabolic alkalosis
resp have root cause in ventilation or alveoli gas exchange
metabolic causes by metabolism issue (not resp), by acids other than CO2, like lactic acidosis (caused by anaerobic resp), DKA, sulfuric acid
acidosis: abnormal increase in H due to excess acid or loss of bicarbonate (thru diarrhea)
metabolic: due to excess metabolic acids or lost bicarbonate
due to salicylate (aspirin) intoxication
hypoxia, shock, sepsis → lactic acid
DKA → ketoacidosis
kussmauls resps SE of prev 3
renal failure
loss of bicarbonate
SE: hyperkalemia, dysrhythmias, confusion
intervention: treat cause, O2, fluids, K, sodium bicarb (if IV, pH <7.1 or coding; PO), dialysis, antidiarrheal meds (stop bicarb loss), diuretics (increase H+ loss)
respiratory: excess of carbonic acid due to low RR or alveoli gas exchange
due to shallow breathing (weak resp muscles), resp depress (brain issue or sedation), obstruction of resp, blocked alveoli gas exchange
SE: CO2 causes vasodilation → cerebral edema → visual disturbance, headache, restlessness, agitation, confusion, drowsiness, coma
intervention: fix cause, positioning, O2, meds, IS, mechanical ventilation (increase CO2 loss), ambulation
alkalosis: abnormal decrease in H ions, due to excess bicarb or loss of acid
SE (same for both): hypokalemia, hypocalcemia (alkaolosis makes Ca bind to albumin, trousseaus + chvosteks signs +), anxiety, irritability, dizziness, hypotension, mental confusion, numbness and tingling of digits, muscle twitching, tetany, seizures
metabolic: excess bicarb due to high PO or IV bicarb
due to ingesting lots of bicarb or antacids, excess bicarb admin, loss of hydrochloric acid from stomach, diuretics (H loss)
intervention: treat cause, stop bicarb intake, give antiemetic, stop loop or thiazide diuretic, E/F replacement
resp: carbonic acid deficit due to high RR or alveoli gas exchange (releasing too much CO2)
due to anxiety, pain, fever
intervention: reduce CO2 loss
anxiety: meditation, benzo, propanolol
pain: meditation, positioning, tylenol, narcotic
fever: antipyretic
acid base imbalances
metabolic acidosis, resp acidosis, metabolic alkalosis, resp alkalosis
resp have root cause in ventilation or alveoli gas exchange
metabolic causes by metabolism issue (not resp), by acids other than CO2, like lactic acidosis (caused by anaerobic resp), DKA, sulfuric acid
table
blood gasses
arterial blood gas sample taken by resp therapist. results in 15 min. thru A-line if needed often.
ABG interpreted using pH, PaCO2, and HCO3, and optionally PaO2
PCO2: measurement of partial pressure of CO2 in blood, reflects resp component.
normal 34-45 mm Hg.
> 45, excess CO2, pH acidosis
<35 less CO2, pH alkalosis
HCO3: bicarbonate. measurement of bicarb in blood. reflects metabolic component of kidneys
normal 22-26 mm Hg.
>26 excess bicarb, alkalosis
<22 less bicarb, acidosis
math:
see pH, identify if acidosis (<7.35) or alkalosis (>7,45)
see PCO2 and HCO3, identify
example:
pH 7.20, acidosis (result of imbalance)
PCO2 56, acidosis
HCO3 (bicarb) 25, normal
resp acidosis (caused by PCO2) with no compensation bcos HCO3 is normal and kidneys haven’t reacted yet. acute because of short timing (kidneys havent responded yet)
compensation only if normal pH
arterial blood gas (ABG) compensation
signs of compensation:
pH normal but PCO2 and/or HCO3 are imbalanced
if one is acidosis, the other is alkalosis to balance pH
lungs compensate if issue is metabolic, and kidneys compensate if issue if resp.
metabolic acidosis:
low pH and low HCO3
SE kussmal resps (rapid, deep resps to blow off CO2)
resp acidosis:
low pH and high PCO2
SE kidneys absorb bicarb
metabolic alkalosis:
high pH and high HCO3
SE low RR to retain CO2
resp alkalosis:
high pH and low PCO2
SE kidneys excrete bicarb
math
pH 7.38, PCO2 49, HCO3 30
PCO2 high acidosis, HCO3 high alkalosis
pH is normal but closer to acid (from 7.4), showing that the issue is acidosis.
PCO2 is the acidosis one, so resp primary issue. renal compensated. compensated rep acidosis
math
pH 7.44, PCO2 49, HCO3 33
pH normal but on alkalosis side (from 7.4), showing alkalosis is the issue
PCO2 normal, acidosis and HCO3 high, alkalosis.
renal primary cause, resp compensation
compensated metabolic alkalosis
pH 7.51, PCO2 25, HCO3 24
pH alkalosis, PCO2 alk, HCO3 normal
pH is alk, showing alk problem. PCO2 is alk, showing that resp is cause
uncompensated resp alkalosis
pH 7.2 (acidosis), PCO2 40 (normal), HCO3 12 (acidosis)
acidosis is the issue. HCO3 kidneys caused issue.
uncompensated metabolic acidosis
SE/cause of kussmauls, hypoxia, salicylate, sepsis, toxic, etc
acute respiratory failure
hypoxemic: PaO2 < 60 mm Hg
low O2 in blood
hypercapnic: PaCO2 > 45 mm Hg, pH <7.35
cannot remove CO2 from blood
due to failure of oxygenation or failure of ventilation
initial SE: dyspnea, tachypnea, restlessness, confusion
progressive SE: worsening acidosis, cardiac dysrhythmias, increased ICP, coma, death
oxygenation failure (primary hypoxia cause):
decreased or absent blood flow, decreased O2 exchange at alveoli, not enough O2
ventilatory failure (primary hypercapnia cause):
extrapulmonary:
muscular disorder → diaphragm use issue
brain dysfunction, spinal cord injury
external pressure → hypoventilation
intrapulmonary:
airway resistance or obstruction
lung compliance
treat: treat cause, support ventilation & gas exchange
O2 therapy, minimize O2 demand, meds, positioning, mechanical ventilation
ventilation perfusion ratio
ventilation (V) / perfusion (Q)
physiologic shunting: area is ventilated but alveoli has limited gas exchange
non-invasive positive pressure ventilation
continuous positive airway pressure (CPAP):
positive pressure during entire inspriation and expiration. must have spontaneous respirations and proper mask seal
bilevel positive airway pressure (BPAP):
higher positive pressure during inspiration and lower positive pressure durign expiration. must have spontaneous respirations & proper mask seal
IPAP - inspiratory PAP
EPAP - expiratory PAP
indication:
CPAP: sleep apnea
BIPAP: resp exacerbations (COPD, CHF), palliative, post-extubation
contraindications:
altered LOC, inability to protect airway, resp distress, need for PO access (meds, food), N/V, cannot control oral secretions, facial trauma, inability to establish mask seal
complications:
gastric distension, aspiration, nasal/facial skin breakdown, nasal dryness/congestion, eye irritation, anxiety
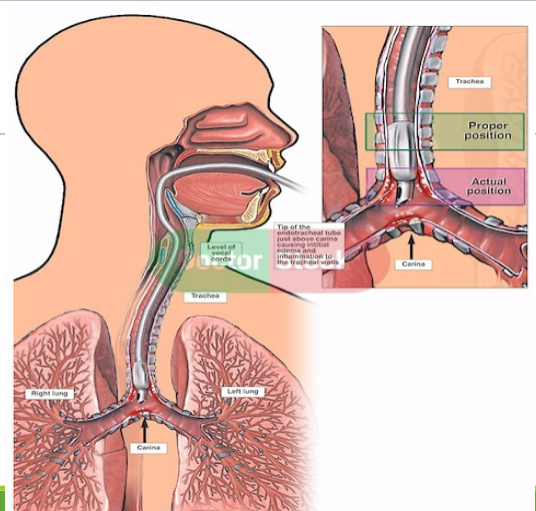
endotracheal intubation & mechanical ventilator
indications:
compromised airway, resp exacerbations, ABG imbalances, cardiac arrest, low LOC, resp support during & post surgery, life-long use for progressive neuromusc diseases
complications:
anxiety, delirium, hypotension (due to less room for heart due to big lungs), barotrauma (too much air), ulcer, malnutrition, RF infection, muscle atrophy
nurse role: stabilize airway, gather equipment, inform patient, IV meds, monitoring + assessment, stabilize tube + suction PRN, verify placement, LF gastric distension
confirm placement:
LF exhaled CO2 level
auscultate bilateral breath sounds
symmetry of chest expansion
chest x-ray (2-3 cm above carina)
goal: short term (2-3 wks), patent airway, low WOB, remove secretions, provide ventilation + O2, prevent complications
ventilator-associated events (VAE):
infectious lung injury: ventilator-associated pneumonia (VAP)
non-infectious lung injury: ventilator-caused injury, atelectasis
VAP BUNDLE interventions:
HOB 30-45
oral care q2-4 hr (6x daily)
q12h CHG
sedation assessment (stop sedation daily, readiness to wean)
peptic ulcer disease prophylaxis (pepsid to stop malnourishment issues)
DVT prophylaxis (SCDs, heparin, PT)
turn q2
intubation pic
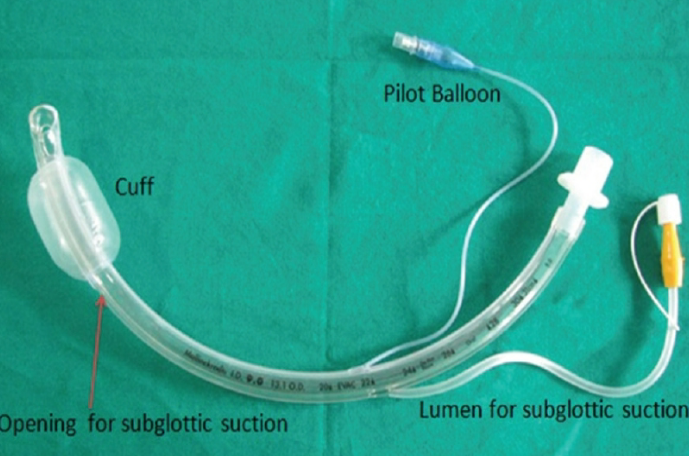
in-line suction (closed unit)
closed unit vs normal suctioning (see trach)
adaptor at the ETT-vent circuit interface that allows suctioning of airway without disconnecting ventilator
pros: stability of PEEP, lower RF infection
cons: hypoxia, trauma

ventilator alarms
high pressure: alarms when peak inspiratory pressure (PIP) is high. means that it requires too much pressure to oxygenate the patient. AMBU bag at bedside (for manual ventilation)
nurse job: assess patient
cause: coughing, gagging, tube biting
anxious, fighting ventilator
airway displaced or obstructed
decreased compliance of lung or collapse
low pressure: alarms when PIP is too low.
cause: leak in circuit preventing breath from being delivered
cuff leaks in ET or trach tube
patient extubated self
ventilator settings
ventilator settings:
FiO2 (fraction of inspired O2): O2 concentration. 21% (room air conc) to 100%
rate: bpm
tidal volume (VT): set of volume of air delivered on inspiration
peak inspiratory pressure (PIP): pressure applied on inspiration to deliver set tidal volume.
positive end expiratory pressure (PEEP; range of 5-20): air pressure maintained thru expiration. prevent alveoli collapse, good for if need more lung surface area to increase gas exchange.
goal: treat persistent hypoxemia. keep alveoli open longer. improve gas exchange. lower WOB
complications: hypotension, barotrauma, pneumothorax
modes:
pressure/volume modes:
volume-targeted
pressure-targeted (preset airway pressure)
ventilator trigger mode:
assist control (AC mode; first choice)
controls breathing more than patient
vent assists with breath to the set tidal volume, ensures the breath occurs regardless of patient desire
pt can initiate breath, but the vent inserts exact volume of air into lungs
decreases patient WOB
cons: potential resp alkalosis. pt can breathe faster then set RR
synchronized intermittent mandatory ventilation (SIMV)
used after AC. vent assists with set tidal volume on some programmed breaths.
increases patient WOB on unassisted breaths. pt can breathe faster than the set RR
cons: potential resp alkalosis
weaning: re-establish spontaneous independent breathing, minimize sedation
AC → SIMV → positive pressure support
extubation: O2, high fowlers, DB & C/suction, monitor
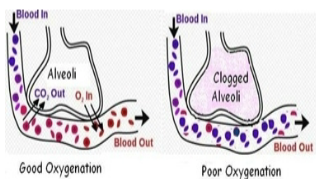
acute respiratory distress syndrome (ARDS)
caused by direct or indirect lung injury. 35-45% mortalityn
injury → low bloodflow → RBC accumulation → inflammation → damage to alveolar membrane → increased capillary permeability → proteins + fluid leave into interstitial space → pulm edema
fluid in alveoli + low blood flow → alveoli damage → difficulty to produce surfactant → alveolar collapse → impaired gas exchange
RR raises but O2 can’t cross membrane. CO2 crosses easier → blood O2 and CO2 both drop
pulm edema worsens → inflammation causes ambrosia → worsened gas exchange → hypoxemia → resp acidosis
SE:
sudden and progressive pulm edema from inflammatory cascade (non-cardiac)
severe hypoxemia that is unresponsive (refractory) to O2 therapy
decreased lung compliance
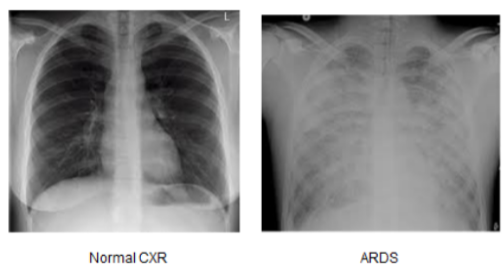
dense pulm infiltrates with ground-glass appearance on chest x-ray (turning to fibrosis
common comorbidities (don’t study)
direct: severe thoracic trauma, diffuse pulm infection. toxic gas, aspiration, prolonged mech vent use
indirect: severe sepsis, shock, or anaphylaxis. severe nonthoracic trauma, pulm emboli, metabolic disorders, hematologic disorders, drug overdose/ingestion
phases:
Phase 0 Acute Lung Injury 3ish days
expected SE: initial sever dyspnea, labored WOB, low PaO2 + SpO2, tachycardia, disorientation, anxiety
possible SE: fever, diaphoresis, hypotension, crackles
Phase 1 ARDS - Exudative, 7-10 days
SE: low surfactant, crackles,
diagnose:
chest x-ray → diffuse bilateral infiltrates
ABGs → resp acid
hypocapnea, PaO2 <60
cardiac tests to rule out cardiac origin
Phase 2 - Fibroproliferative, weeks to months
repair: dead cells removed → fluids dissipate → alveoli repaired → surfactant produced
Phase 3 - Fibrotic, weeks to months
50% mortality
resolution
SE: ventilator, long-term care facility, barotrauma
fibrosis: irreversible, higher mortality
SE: multi-organ dysfunction, vent dependent, barotrauma,
mgmt:
vent support - high peep/FiO2 (to keep lungs open), small tidal volumes (prevent barotrauma in alveoli)
positioning - HOB elevated, or prone (allows the fluid to enter diff alveoli so the wet alveoli get a break, + taking heart weight off lungs helps w breathing)
nutrition - enteral or TPN
circ support - conservative fluids + monitor UOP
drugs - diuretics, antibiotics
sedation to help patient accept the high WOB from ventilator
ECMO (extracorporeal membrane oxygenation; removes blood, adds O2 and removes CO2, puts it back in), oxygenation
critical care
environment: for life-threatening situations. supplies are highly sophisticated and readily accessible
patients: many complex + interrelated issues, frequent priority reorganization, time limits due to rapid condition changes. acquire complete and detailed history + physical exam
monitoring
cardiac telemetry
hemodynamic: arterial line + MAP, cardiac output + input, pre-load + CVP, swan Ganz (PA pressure + PCWP)
stressors: sleep cycle interruption, sleep deprivation, mental altering drugs, fear. new environment, new faces, noise, light levels, inaccessibility to friends and family, lack of privacy, lack of info, anticipation of pain, impaired communication, excess alarms
arterial line (A-line)
BP and blood samples can be taken. includes a fluid bag connection to ensure clots don’t form (clotted artery creates surgical emergency)
mean arterial pressure (MAP):
(SBP + [2 x DBP]) / 3
if >65, organs are perfused. 65-110 good
always calculate MAP
![<p>BP and blood samples can be taken. includes a fluid bag connection to ensure clots don’t form (clotted artery creates surgical emergency)</p><p><strong>mean arterial pressure (MAP):</strong></p><ul><li><p>(SBP + [2 x DBP]) / 3</p></li><li><p>if >65, organs are perfused. 65-110 good</p></li><li><p>always calculate MAP</p></li></ul><p></p>](https://assets.knowt.com/user-attachments/6b91651e-8c1a-4437-a173-343bcba62311.png)
hemodynamics
cardiac output: amount of blood ejected by heart in 60 seconds, average 4-8L
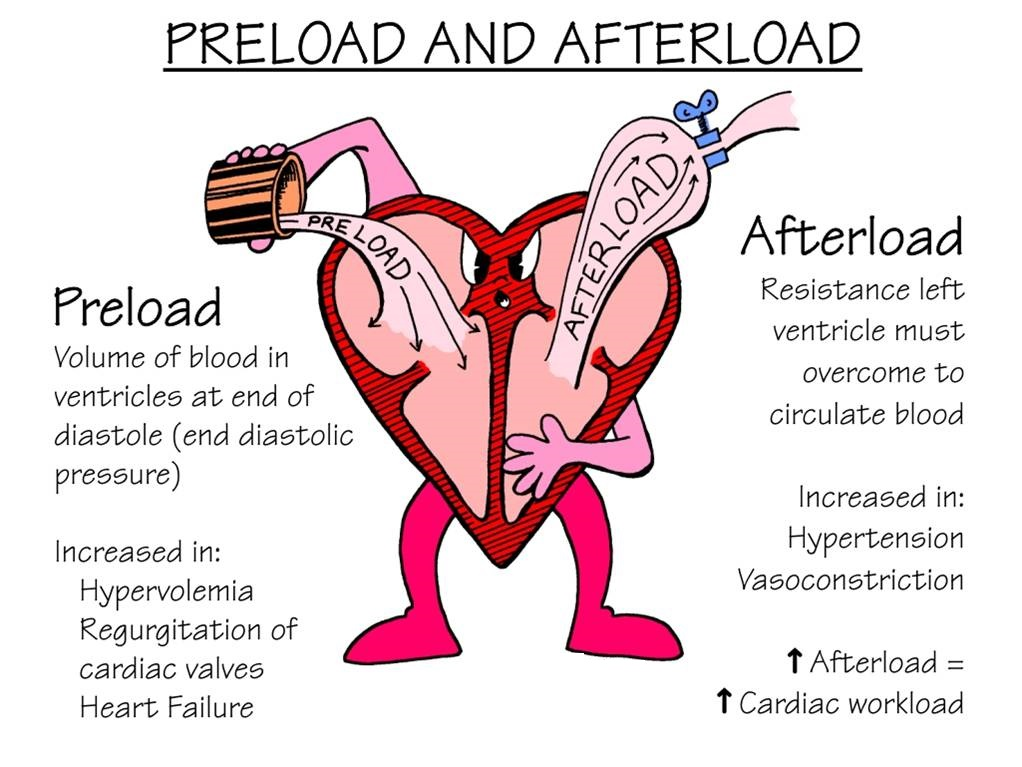
preload: volume of blood
afterload (systemic vascular resistance SVR): how much resistance heart is beating against
contractility: how strong each contraction is
control of peripheral circ: dilation/constriction of vesselscentr
central venous pressure (CVP) line
measurement of the right atrium, the blood returning the preload
can be measured with regular centra line cath or PIC line, or with Swan Ganz
normal: CVP 2-6 mm Hg
if high, too much preload, fluid overload, probs heart failure
if low, fluid deficit, small preload, hypovolemia
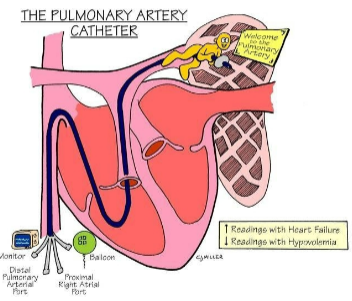
Swan Ganz catheter
put into right IJ, goes thru right atrium, right ventricle, ends in pulm artery
also measures pressure in blood flow
normal: 15-26 mm Hg / 5-15 mm Hg
if high: heart failure
if low: hypovolemia
pulm capillary wedge pressure (PCWP): estimates pressure of left atria
can’t inflate balloon more than 1.5mL
normal: 6-12 mm Hg
if high: heart failure
if low: hypovolemia
intracranial pressure monitoring
normal: 10-15 mm Hg
neuron death: sustained >20
shock
widespread abnormal cellular metabolism that occurs when oxygenation and tissue perfusion needs are not met to the necessary level to maintain cell function. identified thru perfusion and oxygenation.
aerobic metabolisms turn anaerobic → increased lactic acid → metabolic acidosis
types:
hypovolemic: inadequate volume
cardiogenic: inadequate pump
distributive: ineffective vasculature
neurogenic, chemical (anaphylaxis, sepsis, capillary leak), obstructive
stages (need to know all info):
initial: box 31.3 pg 764
MAP drops 5-10 mm Hg from baseline; vasoconstriction
raise in HR or tachycardia for no reason
slight raise in RR
slight vasoconstriction, paler skin
normal UOP
sense of impending doom
normal acid base
nonprogressive/compensatory
MAP drops 10-15 mm Hg from baseline
raise in HR, possibly tachycardic, continued sympathetic stimulation
raise in RR, SpO2 drops 2-5% from baseline
skin is pale and cool, blood shunts away from extremities and more toward organs
UOP decreases slightly, increased thirst
anxiety, fear, sense of urgency
mild metabolic acidosis
progressive
MAP >20 mm Hg from baseline
HR tachycardic but pulses weak due to shunting
tachypneic, resp distress
O2 drops 5-20% from baseline
skin is pale, cool, and diaphoretic (anoxia to non-essential organs, no skin perfusion). possible cyanosis in nail beds and oral mucosa
UOP little to none. dark and concentrated. increased BUN/Cr
confusion, agitation, brain is less perfused
metabolic acidosis + hyperkalemia
refractory (irreversible)
MAP <65 mm Hg. cannot be maintained via fluids, vasopressors, etc.
HR is messed up. tachy, brady, dysrhythmia, vtach, etc. severe hyperkalemia. acidic blood.
resp failure, intubated.
no peripheral pulses, maybe carotids. SpO2 not measurable due to constriction + coldness. skin is mottled, dusky, grey, cold.
no UOP
unresponsive, coma, seizure activity
resp (due to no CO2 release) and metabolic (mixed) acidosis. severe hyperkalemia.
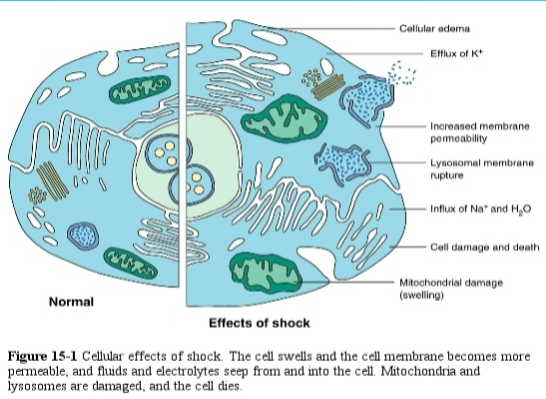
cellular (pic):
walls more permeable, efflux of K, influx of Na and H2O, cell membrane + organelles swell
blood hyperkalemia and blood hyponatremia
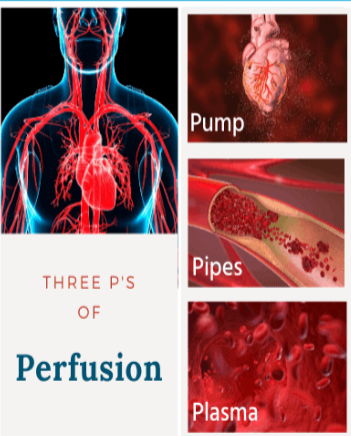
perfusion
working pump, working vessels that dilate and constrict, plasma with appropriate mobility and nutrients
needs:
adequate volume of blood (preload)
effective pumping by heart (CO)
constriction and dilation of vasculature SVR)
unobstructed pathway for blood flow
oxygenation
needs:
blood flow (CO)
amount of hemoglobin to carry O2
% of arterial O2 hemoglobin saturation
O2 consumption (not tested):
body’s demand for O2, reflecting body’s metabolism
magnitude of O2 consumption deficit correlated with mortality rates
low O2 consumption is common in shock
due to reduction in blood flow
hypovolemic: not enough blood flow
cardiogenic: not pumping 4-8L/min
obstructive: clots
uneven distribution of blood
septic
anaphylactic
neurogenic: spinal, brain
O2 delivery wiggle room (not tested): body normally provides 3-4x more O2 than needed for the metabolism
causes of hypoperfusion and hypoxia
volume: not enough volume, wrong type of volume
pump ineffective
vasculature ineffective: volume isn’t where it needs to be
obstruction in pathway
hypovolemic shock
loss of whole blood, plasma, or interstitial fluids in quantities that the body’s metabolic needs are not met. not enough volume or wrong volume perfusion (saline vs blood)
decrease in blood volume or plasma → decrease in venous return (preload) → low SV → low CO → low tissue perfusion → anaerobic metabolism → lactic acid production → myocardial depression
low CO → low coronary artery perfusion + inadequate cellular perfusion → RF infection + hemorrhage → organ damage
causes: GI bleed, GSW, hemorrhage, bowel perforation, dehydration, MVA, trauma, diabetes insipidus (too much diuresis)
SE:
skin: longer cap refill time. cool, pale skin due to vasoconstriction. clammy moist skin due to epinephrine + norepinephrine
thirst: thirsty due to increased serum osmolality
UOP: low due to vasoconstriction, low GFR, and ADH release
LOC: hyper-alert then decreases
HR: tachycardia. SV decreases → HR increases to maintain CO
RR: high RR and depth to improve O2, blow off Co2, compensate for impending acidosis, increase right heart filling volume
hyperkalemia, hyponatremia
diagnosis: H/H, electrolytes
hemodynamics:
CVP (central venous pressure) preload 2-6 mm Hg
MAP 65-110 mm Hg
(SBP + 2DBP) / 3
treat:
airway: O2, HOB up
breathing
circulation: stop blood loss, restore lost volume, add fluids to improve UOP
crystalloid solutions (LR, .9% NS): to provide intravasc expansion
albumin: effective volume expander, may increase mortality sometimes. (also used in ascites)
hetastarch: plasma volume expander. no danger of hepatitis. cheaper than blood. doesnt replace hemoglobin
FFP: give if fluid loss is due to plasma loss (burns). also for clotting disorders
blood: for major blood loss (whole blood, packed RBCs, etc)
raise foot of bed to push blood to core, helps with oxygenation and increases CO
dobutamine, milrinone, digoxin: inotropic agents to improve left ventricular function and give cardio support
norepinephrine and neo-synephrine: improve preload by giving fluids or vasoconstrictors after volume has been replaced
dopamine
secondary treat (fix stuff caused by our meds)
correct acid-base issues
monitor fluid overload rebound
meet nutritional needs. thru guts if bowel sounds. thru TPN if no bowel sounds
cardiogenic shock
caused when the heart’s pumping ability becomes impaired → low cardiac output (CO). 40% mortality
cause: conditions that cause dysfunction of left ventricular, right ventricle, or both due to ischemia, structural issues, or ischemia
low cardiac contractility → low SV and CO → pulm congestion + low tissue perfusion + low coronary artery perfusion
low coronary artery perfusion → low cardiac contractility again
SE: very similar to HF but patient also can’t perfuse or oxygenate
crackles, fluid overload, pulm edema, JVD, pitting edema, peripheral edema, scrotal edema (this is the diff between cardio shock and hypovol shock)
low BP
weak pulses
cool and clammy skin
low UOP, low bowel sounds, low everything
altered LOC
HF
treat:
give inotrope, diuretic, vasopressor, vasodilator
norepinephrine: vasopressor to fix low BP
inotrope: to increase heart contractility and improve organ perfusion
diuretic: allows body to pee off extra fluid overload
dobutamine, milrinone: increase CO
nitroglycerin, nitroprusside: vasodilator to decrease afterload and lower left ventricular workload. hypothetically lowers BP but reduces resistance.
only if systolic BP > 110
if <110, vasoconstrictor instead
O2, raise HOB
increase CO by fixing dysrhythmias, hypo or hypervolemia
distributive/circulatory shock finish anaphylactic patho
heart works, volume is fine. problem is vasculature
anaphylactic: hypersensitivity allergic reaction to antigen → massive vasodilation → low CO + increased capillary permeability → bronchoconstriction → inflammation → increased coronary permeability → misdistribution of blood → blood doesn’t return to heart → low preload → low CO → bad perfusion
SE: hives, angioedema, stridor, periorbital edema, flushed skin, rash
goes from anaphylaxis to anaphylactic shock due to low O2 and perfusion
low BP
low CO
high HR (compensation)
low UOP
skin is rashed, flushed and warm → cold and cool
treat: epinephrine, vasoconstrictor, fluids, O2, raise HOB, diphenhydramine (benadryl), steroids
neurogenic:
cause: spinal cord injury (T6 and up), spinal anesthesia, brain medulla damage, drugs (ganglionic blocking agents, barbiturates), etc.
SE: massive vasodilation → low vascular tone → low systemic vascular resistance → low CO → low perfusion → impaired cell metabolism
massive BP + MAP drop (normal good MAP: 65) (for neuro: MAP >85-90 to improve spinal cord perfusion)
HR decreases (no more sympathetic NS stimulation to compensate bcos sympathetic NS is the issue)
initial pink, warm, flushed skin (blood pooling in extremities). then quickly becomes cold due to lack of circulation
neuro patients have very poor temp reg
treat: O2 + raise HOB for oxygenation.
fluids to replace the fluids that are in the wrong place
vasoconstrictors (norep, epine) to fix the massive vasodilation and get blood back to heart
septic: chemically induced → triggered sepsis → anaphylaxis → capillary leak
shock complications: (don’t memorize)
brain: low O2, hypoxia, seizures, LOC, lethargy, coma, etc
kidneys: vasoconstriction, necrosis, oliguria, high BUN/Cr
myocardium: low CO and low coronary perfusion, myocardial failure, increases dysrhythmias, low CO
fluid shifts: water moves into cells w Na, lowering blood volume, cellular edema, lower metabolic activity
peripheral circ: vasoconstriction to increase blood volume, fluid moves from interstitial to intravascular to increase BV, compensation fails and blood shunts away from organs and to brain and heart
bowels: vasoconstriction, ischemia, ulcers, death
liver: low blood flow, hypoxia, infection, met acidosis, DIC, hard to get rid of toxins
glucose: hyperglycemia due to needing more energy
ARDS: low lung bloodflow → low surfactant → atelectasis. high cap permeability → fluid leaks from capillaries into lung → pulm edema
disseminated intravascular coagulation (DIC)
global inappropriate microcirculation clotting.
RF: pregnant people, amniotic embolus, abrupto placentae, trauma, any shock, septic shock, cancer, toxins
cause: infllammatory response → coagulation activation → clots capillaries → clotting factors run out → paradoxical bleeding.
SE:
treat: O2 for hypoxemia, fluid for volume, RBC, FFP, clotting factors
if caught during clotting phase (before bleeding), give heparin to break down clots to stop using all clotting factors
multiple organ dysfunction syndrome (MODS)
multiple (more than 2) organs affected by shock
signs of organ dysfunction: bad LOC, no bowel sounds, low UOP, etc
sepsis thinking
low UOP due to low perfusion to kidneys
drop in O2 due to global response to infection → low perfusion to all organs
sepsis
#1 cause of death
infection → overwhelming inflammatory process → systemic response → coagulation → impairment of fibrinolysis → RF DIC → bad blood flow → low perfusion → cells shut down → organs fail → death
#1: systemic inflammatory response syndrome (SIRS) signs
temp > 100.4 or <96.8
HR >90
RR >20
WBC >12 or <4
10% increase in neutrophil bands
#2: sepsis (>2 SIRS criteria + suspected or confirmed infection
#3: severe sepsis (organ dysfunction)
SE: infection, organ dysfunction, hypotension, hypoperfusion, SBP <90 or MAP <65
hypoperfusion: tachypnea, oliguria, alteration in LOC, lactate > 4 mmol/L (shows lactic acid in blood due to anaerobic due to bad perfusion; normal 2.2 or less)
#4: septic shock + multiple organ dysfunction syndrome (MODS)
RF: age <1 or >65, malnutrition, hypothermia, central venous catheters, endotracheal intubation or ventilation, aspiration, infection with resistant microorganisms, any chronic illnesses, immunodeficiency (HIV, alcoholism, chemo, transplant), invasive procedures
SE: fluids + treatments not working. severe sepsis + hypotension
MODS:>2 organ dysfunctions without homeostasis even if treatment
hypotension: SBP <90 or reduction of 44 mm Hg from baseline or MAP <65
WBC changes
increased % of neutrophil bands
temp changes, chills
low skin perfusion, low cap refill
low UOP
low PLT, skin mottling
hyperglycemia
petechiae or purpura
tachypnea, tachycardia, LOC
labs:
cultures of urine, blood, sputum, wounds
polymerase chain reaction system (PCRS) to LF what type of infection
WBC left shift, PLT
lactate > 4 mmol/L (norm 2.2 or less)
procalcitonin >2 mcg/L (norm <0.5)
coag profile PT/INR & PTT
d-dimer
activated protein C
cytokines
treat: vasopressor (norepinephrine + levo??)
1 hr sepsis bundle:
measure lactate level
give fluids at 30mL/kg for hypotension or for lactate > 4 mmol/L (give first if unstable/hypotensive)
get cultures before giving antibiotics (do first if stable)
give broad-spectrum antibiotics within 1 hr of sepsis
volume replacement (fix)
fluid intervention: crystalloids (NS or LR) 30mL/kg or low volume. colloids or albumin. blood replacement if HGB <7
antimicrobial: early therapy + eliminate source of infection
glucose:
hyperglycemia: pro-inflammatory, pro-coagulant, interferes with immune by impairing neutrophils + wound healing and increasing RF infection.
keep BG 140-180 to reduce mortality
vasopressor: hypotensive → add fluids + norep. A-line. dobutamine if myocardium depressed. no dopamine bcos it can promote tachydysrhythmias
lung ventilation:if ventilation, prevent barotrauma, avoid high pressures to tidal volume, use low tidal volume, use PEEP, HOB 30-45
antibiotics
prevention: handwashing, infection control, oral care, turn patients, catheter care, wound care, identify RF, get quick cultures if febrile, assess well
nursing (do not study):
fix fever/hypothermia, tachycardia, tachypnea, hypotension
monitor heart (rhythm, CO, SVR)
monitor ventilation (ABGs, pulse ox, lung sounds, RR)
renal: UOP <5 mL/kg/hr, BUN/Cr, Na
hemat: bruising, bleeding, PLT, PT/INR, aPTT, fibrin
nutrition: feed bowels if they are on, maintain protein, normalize glucose
GI: N/V, abd distention, bowel sounds, high enteral residuals >200mL (not digesting food), hyperbilirubinemia, high liver enzymes
neuro: restlessness, LOC, GCS
skin: temp, color
skin function
protective barrier, thermoreg, fluid retention, sensation, vitamin D absorption,
burns
SE: loss of skin function caused by source, heat intensity, exposure duration, skin thickness, plasma loss (55% of blood volume, 90% water)
major burns (>20% total body surface area TBSA):
fluid imbalance: inflammation, edema, redness, turns systemic ASAP, vasodilation, capillary permeability, fluid loss
hemodynamic changes: cardiac output decreases, SNS response (stress) → hypermetabolism (up to 1 yr) + hyperglycemia
types:
thermal (common): contact, steam, flame, scalding liquids
chemical: contact, fumes, ingestion, injection. depends on chemical concentration + volume
household cleaners
electrical (high vs low volt): entry + exit points, cardiac + renal concerns. dysrhythmias due to electricity.
electrical wires, poles, lightning
inhalation: from thermal or chemical agents
environment, work
radiation:
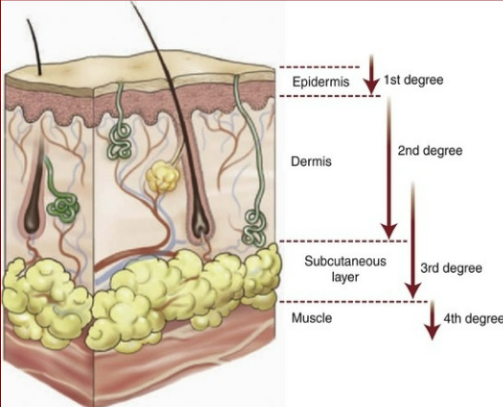
burn depth: (11th, p 467 table 21.8)
superficial thickness (1st degree): thru epidermis.
SE: nerve damage, feels pain when burnt, redness, blanchable
partial thickness (2nd degree): past epidermis and into dermis.
superficial partial thickness: halfway thru dermis
deep partial thickness: fully thru dermis
SE: nerve damage, feels pain when burnt, blistered, moist
full thickness (3rd degree): thru epidermis, dermis, and SQ tissue. difficulty healing, needs grafts.
SE: pain cannot be felt in this layer because nerves are not in SQ. pain only felt in less burnt areas, dry, discolored. leathery or charred.
deep full-thickness (4th degree): thru epidermis, dermis, SQ, and muscle, sometimes to bone. cannot heal, grafts don’t help, needs amputation
SE: same as full thickness
burn care
total body surface area (TBSA)
decided by TBSA, type of burn, depth, what body parts (if dependent or independent), age, and past medical history
circumferential: all the way around. circumferential burns on a leg would be 18
RF: diabetes, cardiac issues, renal function + liver function (for meds), pulm function, mobility
TBSA determines how much fluid is needed to fix the patient.
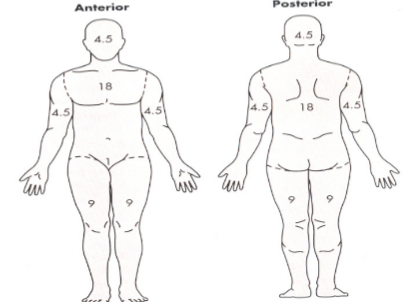
rule of nines (pic): estimates TBSA in 9% increments. does not measure 1st degree. done before hospital/ED. even if only half of a part is burnt, count the whole part.
18%: front abd, back abd
9%: front L leg, front R leg, back L leg, back R leg
4.5%: front R arm, front L arm, back R arm, back L arm, face, back of head
1%: groin
phases of burn care
#1 resuscitative: hemodynamic stabilization thru fluid status + UOP (foley)
onset of injury → 48 hrs
SE before treatment: high serum K (burnt out of cells), high BG (stress), low Na (fluids gone), high HGB/HCT (lost plasma dehydrated), possible metabolic acidosis (due to hypovolemia). RF hypovolemic + distributive shock (capillary leak)
primary survey:
airway/breathing: patent, LF inhalation injury. give bronchodilators or O2. intubate if too edematous
circulation: replace fluids using resuscitative formula
disability: stabilize injuries
expose + examine: temp reg
NG tube for nutrition if poor gut perfusion. burns gotta be washed + debrided. give tetanus shot.
inhalation injury: RF smoke heat or toxic chemicals in smoke
in upper airway (above glottis) or lower airway (below glottis; alveoli damage, RF ARDS)
SE: edema in airway, LOC, facial burns, sooty sputum, singed face nose hairs, blistered mucosa + lips, vocal hoarseness, stridor, wheezing, dyspnea, tachypnea
treat: if suspected, intubate. baseline chest x-ray, 100% O2 w tight-fitting mask, raise HOB, ABGs + carboxyhemoglobin levels, bronchodilators
carbon monoxide poisoning:
tasteless, odorless gas due to incomplete combustion of carbon-containing fuels.
binds to O2 receptors on HCG molecules → low O2 carrying capacity
affects cardiac muscle
makes SpO2 unreliable due to being unable to properly sense O2 in skin
normal carboxyhemoglobin: <10%
coma + death carboxyhemoglobin: >60%
cardio issues: plasma shifts from intravasc to interstitial within 30 min, lasting 48 hrs.
SE low CO due to hypovolemia → vasoconstriction → tachycardia, cardiac dysrhythmias
GI: low gut perfusion → peristalsis → RF duodenal ulcer (Curling’s ulcer) + RF translocation of intestinal bacteria (if gut is hungry and can’t eat, it finds bacteria to eat)
renal: low kidney perfusion → RAAS triggers → oliguria → rhabdomyolysis → RF acute tubular necrosis
#2 acute: prevent infection + UOP
48 hrs → wound closure
survey:
lung sounds (LF fluid overload)
GI + renal function (UOP)
address hypermetabolism + nutritional needs
wound + infection care
pain mgmt
positioning + mobility
pulm: RF pulm edema RF fluid resus, RF bronchial pneumonia, RF ARDS, RF infection with intubation
cardio: fix capillary leakage (fluids), maintain UOP, titrate IV fluids (no more huge boluses), strict I/O, E/F balance
GI + renal: RF gastric ulcer, paralytic ileus RF narcotics, AKI. increased metabolic rate. (NG tube, high protein)
nutrition: high calorie + protein diet needed. hypermetabolism 100-200% above baseline. manage stress (from fluid loss), inflammation, heat loss, muscle atrophy, daily weights, vitamins
pain + mobility: hella pain + anxiety meds. account for drug tolerance. medicate before dressing change. early ambulation. specialty beds + positioning (prevent hands + feet contracting and getting stuck).
immune: wound closure. early surgical debridement. infection control (PPE, cultures asap, barrier techniques for changes)
primary bacteria source is hair
no fresh flowers or plants
#3 rehabilitative: increase mobility and reduce contractures. most wounds closed → closest to baseline. may take 2-5 yrs.
maintain or improve mobility: positioning, specialty beds, splinting to prevent contractures, PT, OT
cosmetics: minimize scarring, protect skin integrity, sunscreen, compression garments 23 hrs/day 6-24 mo.
give resources + support for discharge: grief, PTSD, chronic pain
IV fluid resuscitation formula
during phase 1 resuscitative burn phase
done in 1st 24 hrs, for major burns (>20% TBSA). LR because it is isotonic and also has electrolytes + lactate, making it similar to plasma. warm the fluids to maintain temp reg.
IV LR (Parkland formula; for all burn types)
4 mL x TBSA (whole number) x kg
calculates for 24 hrs of fluid
first 50% of fluids given within first 8 hrs of injury (not arrival)
second 50% over next 16 hrs
successful if UOP > 30mL/hr
injury 5:30pm, TBSA 30%, weight 100kg
4 mL x 30 × 100 → 120 × 100 → 12,000mL LR
1st 6,000mL ends by 1:30am
2nd 6,000mL ends by 5:30pm
working if:
fixed LOC
HR <120
SBP >100, MAP >65
UOP >30mL/hr
blood pH 7.35-7.45
wound care
for phase 2 acute burn phase
PPE + remove dressings as often as ordered
gentle cleaning + debridement. encourage granulation
maintain room temp, pain control, communication
monitor sedation, airway, + VS
prevent cross-contamination (change gloves between wounds)
non-surg debridement: mechanical, enzymatic, wound vac
surgical excision: wound grafting, escharotomy (to remove eschar; incision down to superfiical fat)
compartment syndrome: occurs in burns of chest or limbs.
SE: pulse, paresthesia, palor, paralysis, pain
treat:
escharotomy: cutting in and allowing expansion of skin to accommodate for edema and bloodflow
fasciotomy: deep incision thru fascia (above muscle)
grafts
autograft/allograft: taking patient’s own skin from an unburnt area to cover granulated wound. best option
split thickness wound (epidermis + half wound at donor site. sheet or meshed graft.
aftercare: no debridement or cleaning. only change dressings if ordered (surgeons picky)
donor site heals within 1-2 wks. graft adherence within a few days.
biological skin substitutes: from allograft or xenograft. temporary. removed or rejected by body before a more perm solution.
allograft: living related donor or cadaver
xenograft: animal skin donor
donor site: often anterior thigh. less painful than og site. multiple dressing options like polyurethane, hydrocolloids, hydrogel.
shock and sepsis jeopardy notes
stages of shock
initial shock: patient HR increased from baseline, mild vasoconstriction, compensates UOP (WDL)
refractory shock: HR tachy, brady, complete heart block, or dysrhythmia
progressive shock: HR rapid but weak, UOP anuric, tachypneic
non-progressive shock: MAP decrease of 10-15 from baseline + O2 decreases 2-5%
progressive shock: MAP decreased > 20 from baseline
type of shock
septic shock: severe sepsis w hypotension despite fluid replacement. needs vasopressor support
anaphylactic shock: sudden life-threatening hypersensitive reaction to antigen
hypovolemic shock? caused by loss of whole blood, plasma, or interstitial fluids in high quantities and metabolic needs cant be met
neurogenic shock: caused by spinal cord injury or spinal anesthesia
cardiogenic shock: dysfunction of L ventricle, R ventricle or both due to ischemia, structure, or dysrhythmias
signs of shock
septic shock: fever, bounding pulse, high lactate
hypovolemic shock: hypotension, low UOP, flat neck veins
neurogenic shock: bradycardia, poor temp reg
cardiogenic shock: crackles, HTN, JVD
anaphylactic shock: flushed skin, angioedema, hives
concepts
multiple organ dysfunction syndrome: high liver enzymes, neuro change, low UOP, hypotension
treat underlying cause: how to fix any shock
tachycardia: first signs of shock requiring investigation
what are the 2 core concepts of shock: oxygenation and perfusion
3 Ps of perfusion: pipes, pumps, plasma
treatments:
inotropes: increases cardiac contractility
epinephrine: med IV, SQ, nasally, and ET
.9% NS, LR: isotonic fluids for volume replacement
norep: most commonly used vasopressor for all shocks
nitroglycerin: low afterload/SVR during cardiogenic shock
sepsis:
sepsis: SIRS criteria + infection
septic shock: in severe sepsis, fluids arent effective for MAP, vasopressors must be added
SIRS criteria: tachycardia, increased RR, 10% increase in bands, fever, or hypothermia
lactate: 2.2 normal, >4 mmol is concerning
sepsis bundle: IV fluids, lactate level, blood cultures, antibiotics
q&a
ABGs: SE, body’s compensation, treatment
know lab values + SE, Na, K, Ca
resp failure: indications, complications, contraindications, vent settings, pH, hypercapnia, PO2. bipap vs cpap indications, complications. ARDS SE, RF. ARF RF. AC vs SIMV. confirmation of ET tube: chest xray, bilat lung rise, bilat lung sounds, exhaled CO2. VAP bundle: CHG oral care 2/day, HOB up, sedation vacation, DVT, PUD prophylaxis. high vs low vent alarms.
pulm artery pressure high vs low, MAP, CVP?,