CLPS 0450 Agnosia: Visual Perception Disorders
1/32
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
33 Terms
People with Object Recognition Agnosias have trouble with
object perception and object meaning
Patient GL
He could see (normal visual acuity) but not recognize things around him. Everything was unfamiliar. But he could draw objects that he couldn't recognize.
Apperceptive Agnosia (perception)
- Inability to differentiate between visually similar items (perceptual: shape, color, how do they fit together).
- They are unable to construct accurate 3-D perception
Associative Agnosia (meaning)
Inability to assign object significance or meaning. But they can still differentiate between visually similar items
if you can copy an object but can't identify what it is, what kind of agnosia is it?
Associative Agnosia
In unconventional views test, + means damage/no damage
damage
apperceptive agnosics have damage in _____ hemisphere
right
Associative agnosics have damage in _____ hemisphere
left
if the patient was bad at unconventional view test, they're most likely _______ agnosic.
apperceptive
De Renzi's Ghent Overlapping figures test is designed to test for _________ agnosia.
apperceptive! If you fail overlapping figures test -> apperceptive agnosia.
People with ______ agnosia will fail the object matching test.
associative
- being unable to match objects means they have trouble putting meanings onto objects -> associative.
- apperceptive agnosics struggle with unconventional views, not conventional views. They do NOT have semantic processing issues.
semantic = ______, perceptive = ______
associative; apperceptive
Warrington & Taylor developed a test that could test both perceptual and conceptual at the same time. People who failed the perceptual test failed at (both/one of) the tests, because they have _______ agnosia. They showed damage in _____ hemisphere. People who failed the conceptual test showed no predictor of doing well/failing the perceptual + conceptual test. They have _____ agnosa.
apperceptive; right; associative
For those with apperceptive agnosia, their performance in perceptual + conceptual task test was predicted by ______ task.
perceptual
For those with left hemisphere damage, no matter how well they did on ______ test, they sucked at ______ test. They have ______ agnosia.
perceptual; conceptual; associative
The 3-stage theory of object perception
A. Visual Analaysis -> B. perceptual categorization (apperceptive agnosia) -> C. semantic categorization (associative agnosia)
If you have damage in B, then you will have damage in C.
Patients with damage in C won't have anything wrong with B (they can still perceive the object pretty well, just can't describe what it is)
Marr's model of obejct recognition
Primal Sketch -> (line copying in clinical tests) -> 2 1/2 D sketch -> 3D Model representation -> semantic system
what is the difference between 2 1/2-D sketch and 3-D model representation?
2 1/2 sketch: data driven, so patients' sense of depth is dependent on the exact picture showing, in a single orientation.
3D model representation: not dependent on a single; inherent ability to imagine the object in any orientation (3D) without assistance.
what is line copying representing?
It shows that even patients with apperceptive agnosia can copy the drawing into 2 1/2D but slowly copying the lines. If patients draw fast, they have higher likelihood of having 3D representation ability intact.
If the patient is chance at unconventional views test, which stage of Marr's object recognition series is impaired?
3D representation, because they can't recognize the object in a different orientation.
Patient FRA had normal language capabilities but impaired object identification. In Marr's model, where did this impairment occur?
Associative agnosic; between 3D model representation and semantic system. (last stage);
Patient MS could name verbal description of function, and match identical stimuli. But he couldn't pass the unconventional views test. Where in Marr's model was he impaired?
perceptual agnosic;
Part 3-D model representation (lacks the ability to imagine the object in different orientations. dependent on a visual data)
where does principal axis/canonical view fall in Marr's model?
between 2 1/2D sketch and 3D model representation
what were the two unconventional views in Humphreys & Riddoch? Which one actually had an effect on the unconventional views test?
Foreshortened Principal Axis vs. Intact Principal Axis but with minimized distinctive features
Only patients tested on foreshortened principal axis performed poorly on the unconventional views test -> supported Marr.
BUT through Warrington's test where she showed a bunch of different orientations of an object, they found that all deficits that cloud the distinctive features (foreshortened, distorted, degraded, and obscured) can lead to poorer performance. What does this say about foreshortened principal axis ?
Foreshortened principal axis is not the only condition that can impair their performance
Three categories of agnosia in perceptual categorization
Form Agnosia, Transformational Agnosia, Integrative Agnosia
Patient HJA had integrative agnosia. This means he could recognize _____ parts, but unable to understand ______.
local; whole picture
ex) seeing a carrot's body and the bush area and calling it a carrot. Saw parts as unrelatable to each other
HJA could decide whether an oddly combined shape (ex. Kangaroo + foot) was real by looking at the silhouette. What does this say?
HJA could code the shape really fast, but is impaired at integration of parts into more complex representation & providing meaning to it.
how is patient HJA like an exception to Unconventional Views Test?
Out of the four stages, his impairment was at grouping of visual elements. But he did well on unconventional views test because he was good at identifying local, independent features, not because he could see the object as a whole. So, his earlier diagnosis of associative agnosia was wrong!
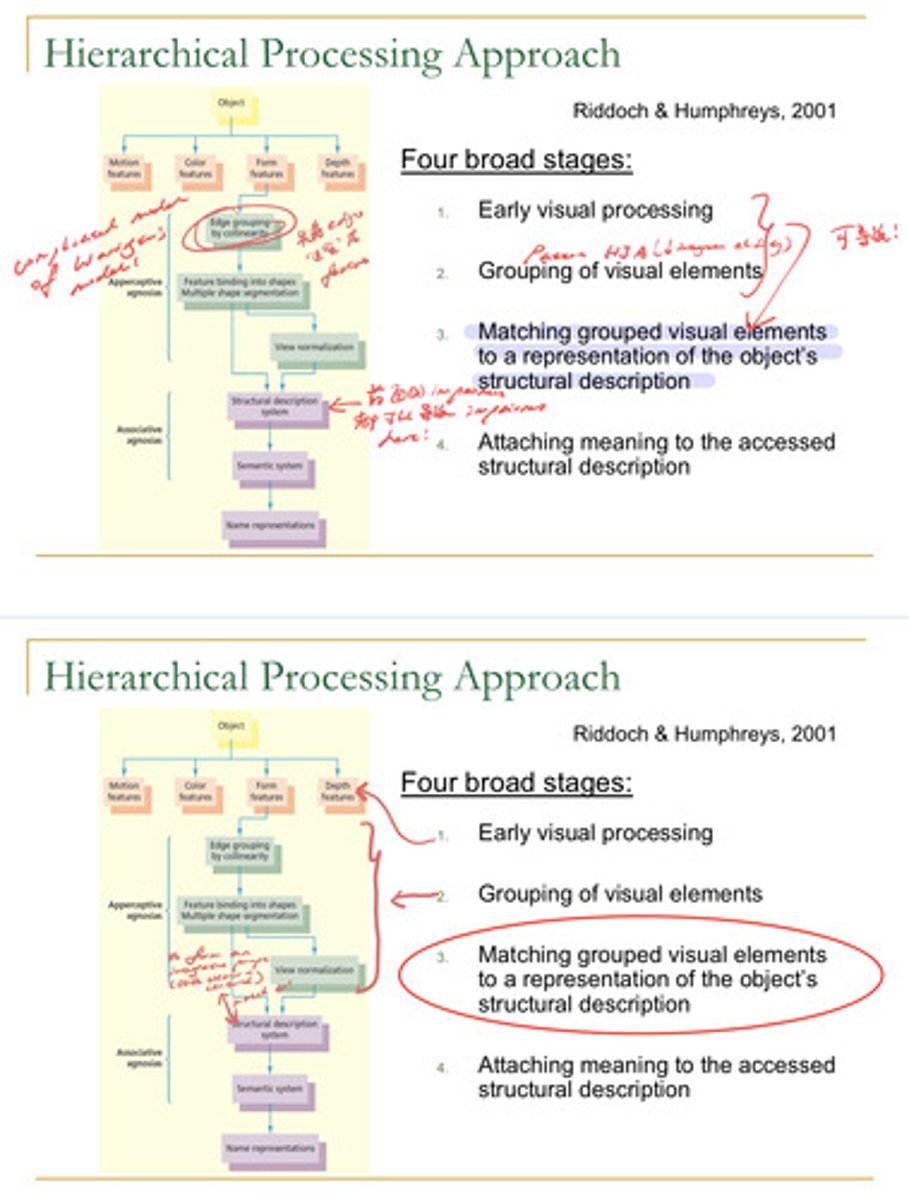
What are the four broad stages of hierarchical processing approach?
1. Early visual processing
2. Grouping of visual elements (patient HJA!)
3. matching grouped visual elements to a representation of the object's structure (applying the features to a real life object and recognizing the common features)
4. attaching meaning to the structure
similarity/difference between Marr and Warrington
Marr and Warrington both studied how we recognize objects, but in different ways.
Marr: used principle axis. foreshortened principle axis -> trouble recognizing objects
view normalization (view normalizing/mentally rotating an object so that it aligns with the principle axis and that's how we recognize objects)
Warrington: We use distinctive features to identify an object. Each object has pretty distinctive features that help us identify them.
Conclusion: you need both.
______ Stream focuses on feature matching (warrington); _____ stream focuses on object rotation (Marr)
Ventral; Dorsal
object orientation agnosia
Can recognize the object in all viewpoints, but cannot choose the correct orientation for an object.
Patient EL could name all the objects in every orientation , but could not determine whether the object was in correct orientation.
When drawings were in silhouettes, he couldn't name them since there were no more distinctive features! When they were not in silhouettes, he could name the objects.