12. Drop installation & Dilated fundus exam
1/29
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
30 Terms
How often should a pt be dilated?
AOA says every 2 years if everything is fine (except for 65+ y/o requires every year)
What is cycloplegia?
The temporary paralysis of eye’s ciliary muscle, prohibiting accommodation & causing pupil to dilate)
Do all dilation drops cause cycloplegia?
No, tropicamide does not cause full cycloplegia but cyclopentolate does.
Do we need to use both dilation drops?
no
Why is dilation important?
It tells us more about the body & a pt’s blood vessels without having to cut them open.
What is PH to confirm before dilation?
allergic or had adverse reactions from previous dilation
pregnant or nursing (some drops have systemic absorption ex. phenylephrine)
current drops used
make sure you have finished all preliminary test that require accommodation!
if pt has increased BP or HTN (side effect of drop is vasoconstriction)
What’re the things we must do & document before dilating a pt?
check angles
IOP
BP (no HTN crisis)
pupils
any test requiring accommodation!
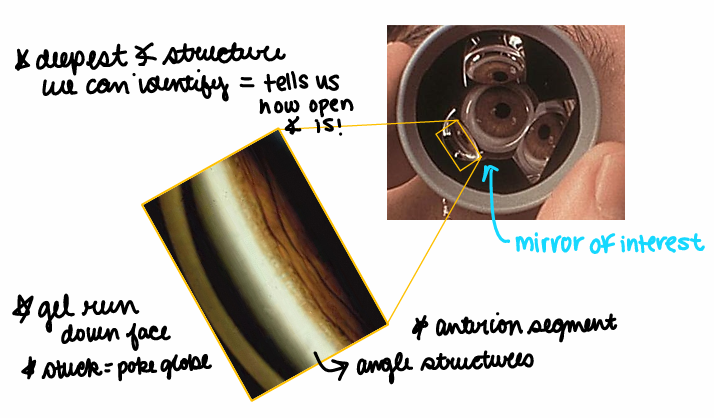
What should you do instead of dilation if the angles are narrow?
Gonioscopy! 3-mirror or 4-mirror that suction cup to the eye so we’re able to look at the 4 quadrants! This is uncomfortable & we must numb the pt beforehand!
The 3 mirror gonioscopy lens must be rotated but the 4 mirrors does not need to be. This is also done behind the slit lamp. Gel might run down the pt’s face & if it gets stuck poke the globe!
The deepest angle structure we can identify tells us how open the angle is.
Which drops are commonly used for adults?
Anesthetic (which would go 1st):
Tetracaine 0.5% (cheaper & burns a lot)
Proparacaine 0.5% (some people are allergic too)
You would NOT use both
White bottle/cap for both bottles
PAINFUL if you forget to add these 1st
Dilation drops:
Tropicamide 0.5% or 1%
Phenylephrine 2.5%
Combo of the two above to control parasympathetic & sympathetic NS
Red caps on both bottles
Dilation drops mechanism of actions?
Parasympathetic (rest/digest/calm):
Circular (sphincter) muscle of the eye constricts
Tropicamide is a cholinergic antagonist
This is what mainly used in clinic (easy dilation for light blue eye or hyperopes)
Sympathetic (fight/flight):
Radial (dilator iris) muscles constrict
Phenylephrine is an adrenergic agonist
Rarely only use this one (b/c sphincter muscle work well & the eye will still constrict partially in reaction to light)
To get maximal dilation use both! Tropicamide will create no opposing reaction from sphincter muscle!
What should you note about the cap colors of dilation drops?
Cap colors mean things!! Don’t need to know specifics for the exam just know cap colors matter!
What should you do before installing drops? (Besides PH & previous preliminary exams)
CHECK THE LABEL & EXPIRATION DATE OF THE DROPS
What instruction should you give the pt to avoid systemic absorption?
Punctal occlusion! Especially for pregnant ladies or pt’s with HTN.
What’re the side effects of phenylephrine?
May reduce inflammation of the eye that was caused by tropicamide. So, you should ass in the drops in this order: anesthetic → phenylephrine → tropicamide
Phenyl might be able to dx a ptosis as well. This drop constricts mullers muscle & open the eye (so when we add phenyl & the ptosis is resolved we know that ptosis is NOT caused by the levator muscle & is caused by mullers muscle b/c phenyl constricts mullers muscles)
When would you use 10% phenylephrine drop?
For something like asnika (pupil looks like a flower in the iris & is caused by a sticky iris)
You would use a single drop of 10% phenylephrine & many drops of cyclopenolate (to reduce inflammation & spasm of the ciliary body) & when you do this it will take several hours for the eyes to return to normal.
Does drop order really matter?
No but it is suggested to use tropicamide last.
How long should you wait between drops?
Anesthetic will work right away & then tropicamide you should wait for 5 minutes until adding in the next drop phenylephrine (do not add back-to-back)
How long does tropicamide last?
4 hours
What drops should you use on kids?
cyclopenelate (will take about 30 minuets for full effects)
Can drops bounce off the conjunctiva?
YES, you could use a dilation spray or put drops in the corner of the pts eye.
How many drops can the eye hold?
less than 1
How many drops are in a 1 mL?
20 drops/mL (know for Rx & dosage)
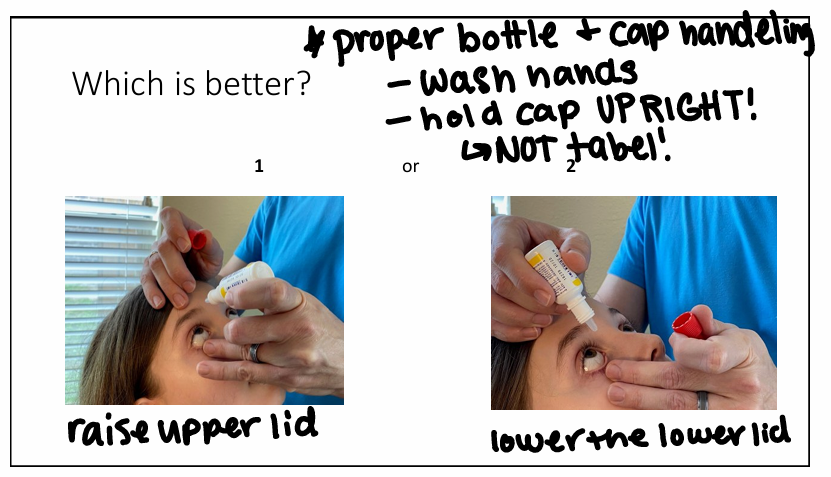
What is the proper bottle & cap handling of drops?
The pt should look down (not up b/c they can see the drop coming & will flinch - can’t control upper lid) & then you can contract the upper lid. The bottle should never touch the lashes & the drop should not bounce off the cornea.
Proper drop installation?
The pt should look down (not up b/c they can see the drop coming & will flinch - can’t control upper lid) & then you can contract the upper lid. The bottle should never touch the lashes & the drop should not bounce off the cornea.
offer a pt a tissue before you put in the drops
always brace your hand
head back on the head rest (when available)
drop one eye, then the other & do not pause between drops
What happen after dilation?
There is a “reversal drop” called Dapiprazole but it is not commonly used.
It can induce HA, redness, itching & light sensitivity.
alpha blocker (stops phenylephrine activity)
induces miosis
Give the pt shades
Advantages of BIO?
bright illumination of fundus
stereoscopic view (see elevation)
larger field of view (see more retina)
greater working distance
view is INDEPENDENT of pt’s refractive error
Disadvantages of BIO?
difficult to learn
requires the use of a lens
low magnification (-3X)
image reversal & inversion
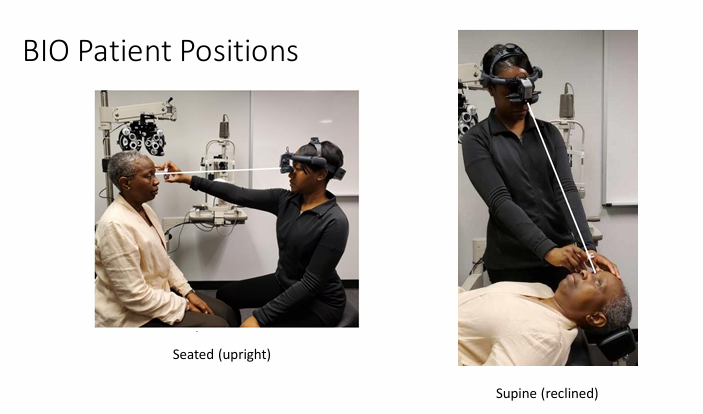
What’re the pt positions for BIO?
How many views of the retina are there with BIO?
8 views & then posterior pole (best to do posterior pole last for optimal pt cooperation)
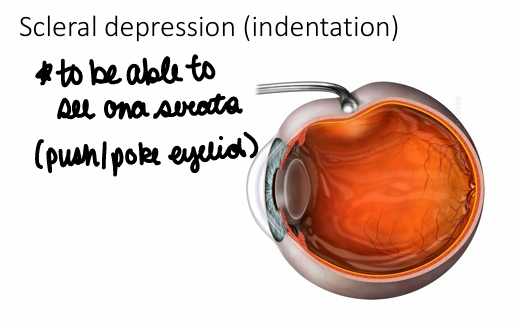
What is the outermost layer of the retina? How might we be able to see this with BIO?
Ora serrata; could do a scleral depression (indentation) this is when you push/poke the eyeball