Teddy: First two lectures
1/115
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
116 Terms
what are the 2 sections of the stomach
corpus and antrum
what are the 4 sections of the corpus glands
pit (fovelus), isthmus, neck, and base
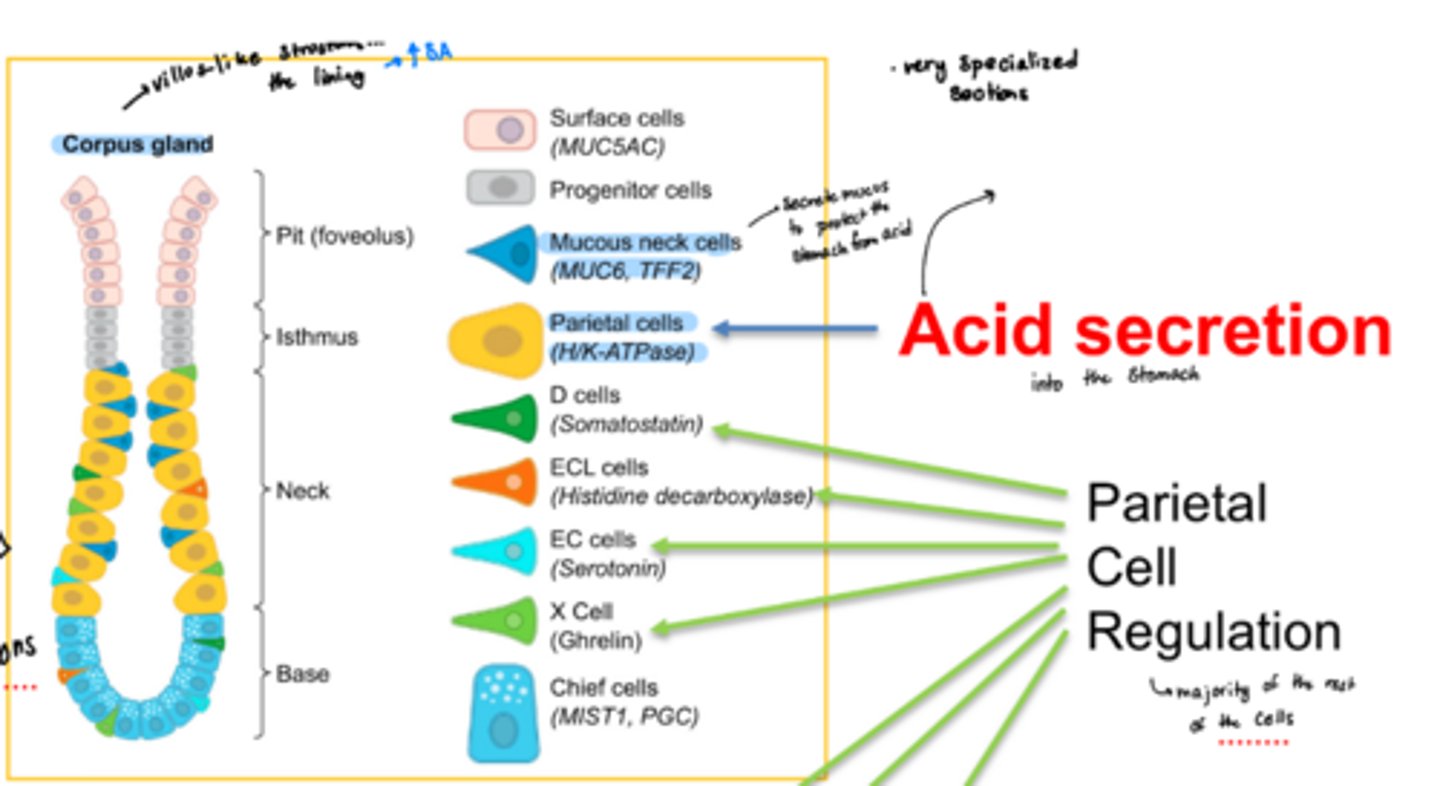
what are the 2 main types of cells unique to the corpus glands and what do they do
o Have mucus neck cells that secrete mucus to protect the stomach from acid (MUC6, TFF2)
o Have parietal cells that secrete acid (H/K-ATPase pump)
what do the "other" types of cells in the corpus and antrum glands do?
mainly play a role in parietal cell regulation
what are the 3 sections of the antral glands
pit, progenitor zone, and base
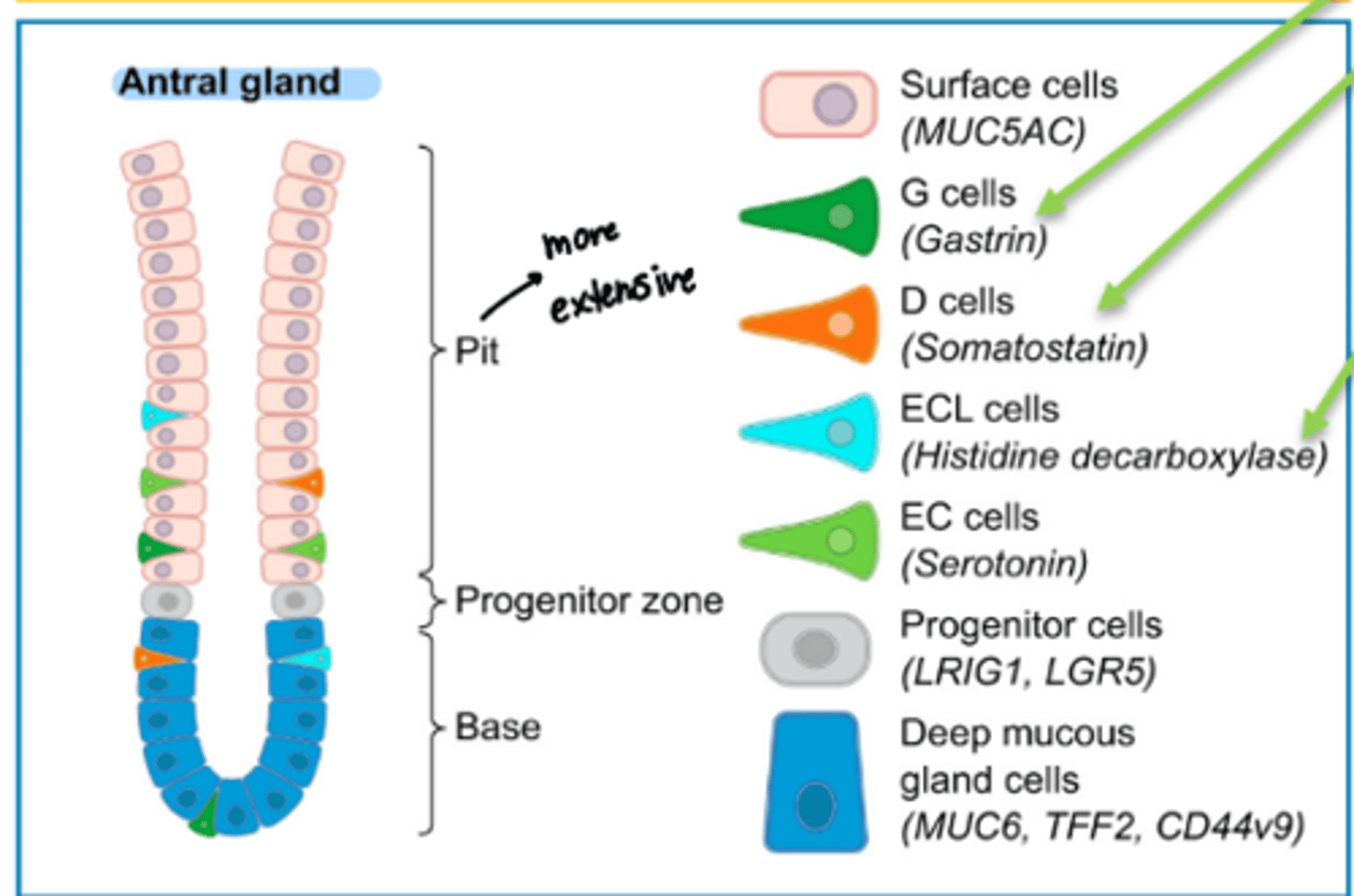
function of surface cells
produce mucus (protective)
D cell function
produce somatostatin which inhibits parietal cells
ECL cell function
produce histamine (positive regulation of paietal cells)
EC cells function
produce serotonin for mechanosensation
X cell function
produce ghrelin, the hunger hormone
chief cell function
produce pepsin (protease)
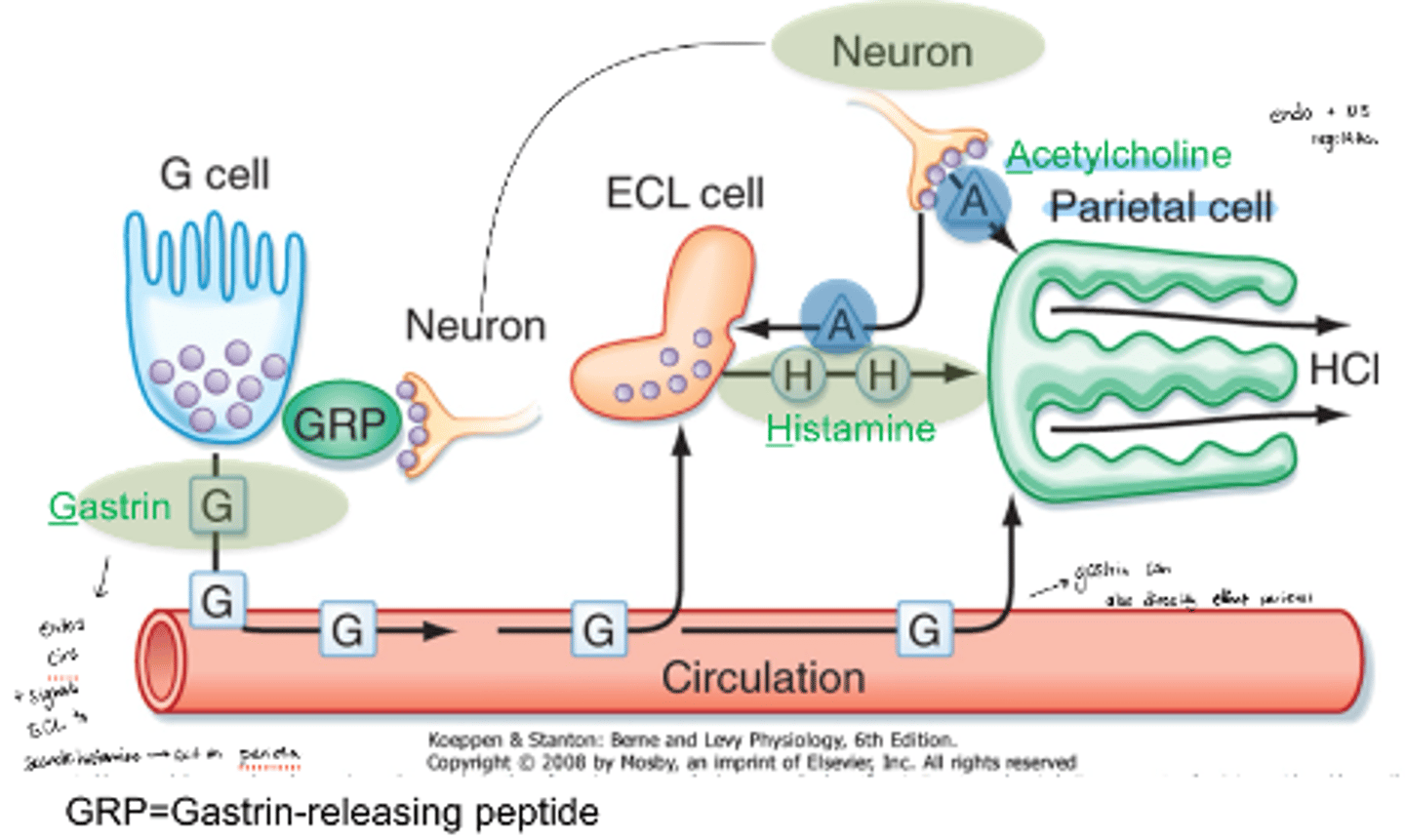
what are the 3 pathways and 3 cells that regulate parietal cells
neural, hormonal, and paracrine pathways
G, ECL, and parietal cells
neuron activation pathway of parietal cells
Neurons activate G cells using GRP. They then produce gastrin which goes into the bloodstream and can activate ECL cells to produce histamine or directly activate parietal cells
neuron secretion of ACh downstream effects
ACh secreted can activate parietal cells directly or activate ECL cells
ECL cells can then secrete histamine which activates parietal cells
what 4 molecules ca cause proton pump activation?
ACh, Histamine, Prostaglandin E2 inhibition, and gastrin can all cause proton pump activation by activating protein kinases
proton pump exchange (what comes in and what comes out?)
Proton pump in parietal cells causes H+ to come out of the cell in exchange for K+ going into the cell
histamine MOA in activation of the proton pump
Histamine binds to a Gs GPCR which converts ATP into cAMP using adenylyl cyclase
Protein kinases are then activated which then activate the proton pump
prostaglandin E2 MOA with proton pump
· Prostaglandin E2 can bind to a Gi GPCR which blocks protein kinase activation and doesn't allow the proton pump to be activated
what is the key cell type of the stomach wall that pumps proton into the lumen of the stomach to cerate an acid environment
parietal/oxyntic cells
which molecule is inhibitory of the proton pump (Gi)
PGE2
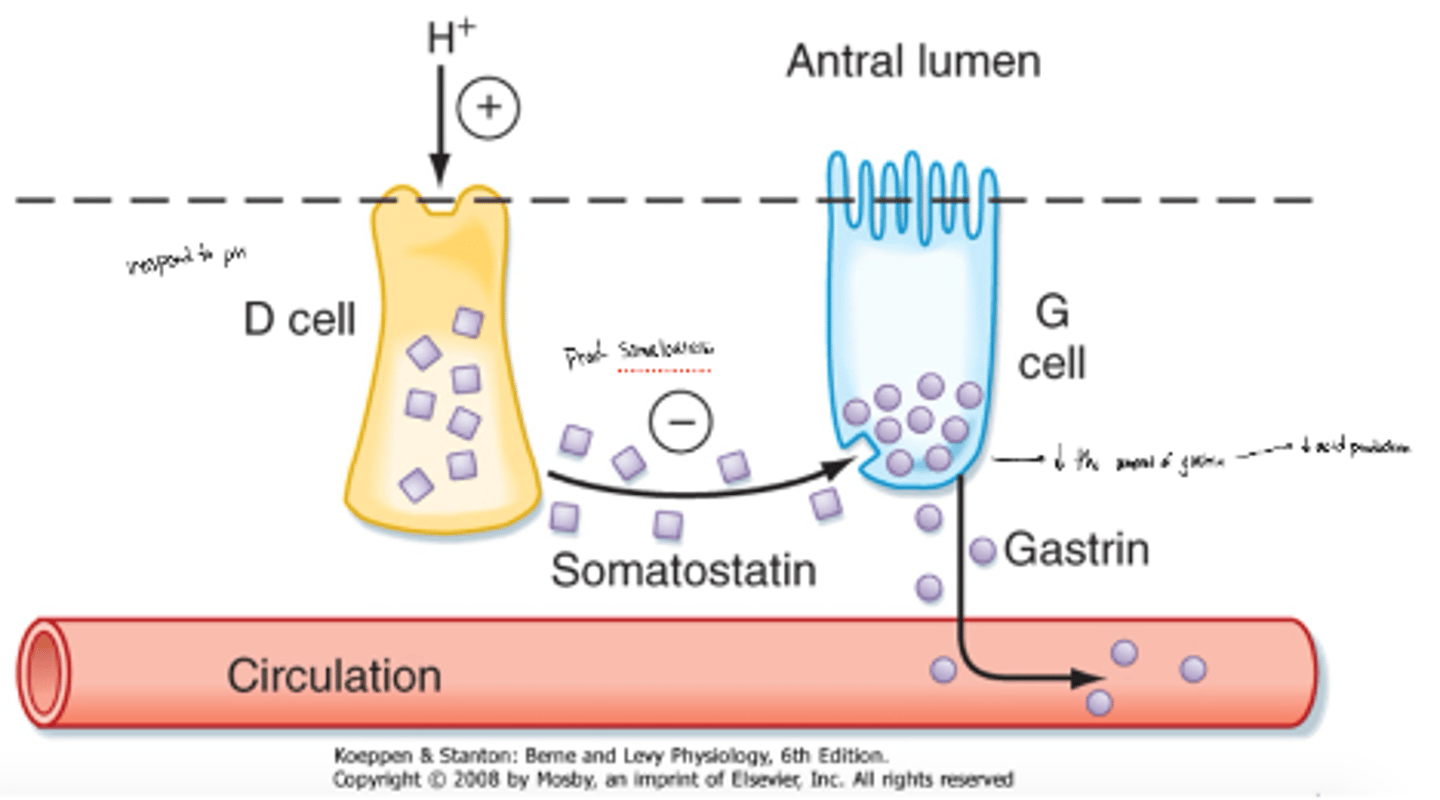
what happens if there is too much H+ (too acidic)
D cells secrete somatostatin which inhiibts the amount of gastrin released by G cells or directly inhibits parietal cells
The less gastrin being released, the less that parietal cells will be activated and secrete acid
what does PUD stand for?
peptic ulcer disease
acid peptic disorders
conditions that are the result of damage from acid and pepsin activity in the gastric mucosa
what are the 3 acid peptid diseases
o GERD
o Peptic ulcers (stomach and duodenal)
o Zollinger-Ellison syndrome
what 3 factors stimulate acid secretion
histamine, ACh, and gastrin
which 2 factors inhibit acid secretion
somatostatin and PGE2
whta are 3 reasons for GERD
o Weakened lower esophageal sphincter
o Hiatal hernia
o Pressure in the stomach
symptoms of GERD
heartburn, uncomfortable burning sensation behind the breastbone, MI can be mistaken for GERD episodes
severe: difficulty swallowing, chest pain
Complications of GERD
· esophageal erosions, esophageal ulcers and narrowing of the esophagus (esophageal stricture)
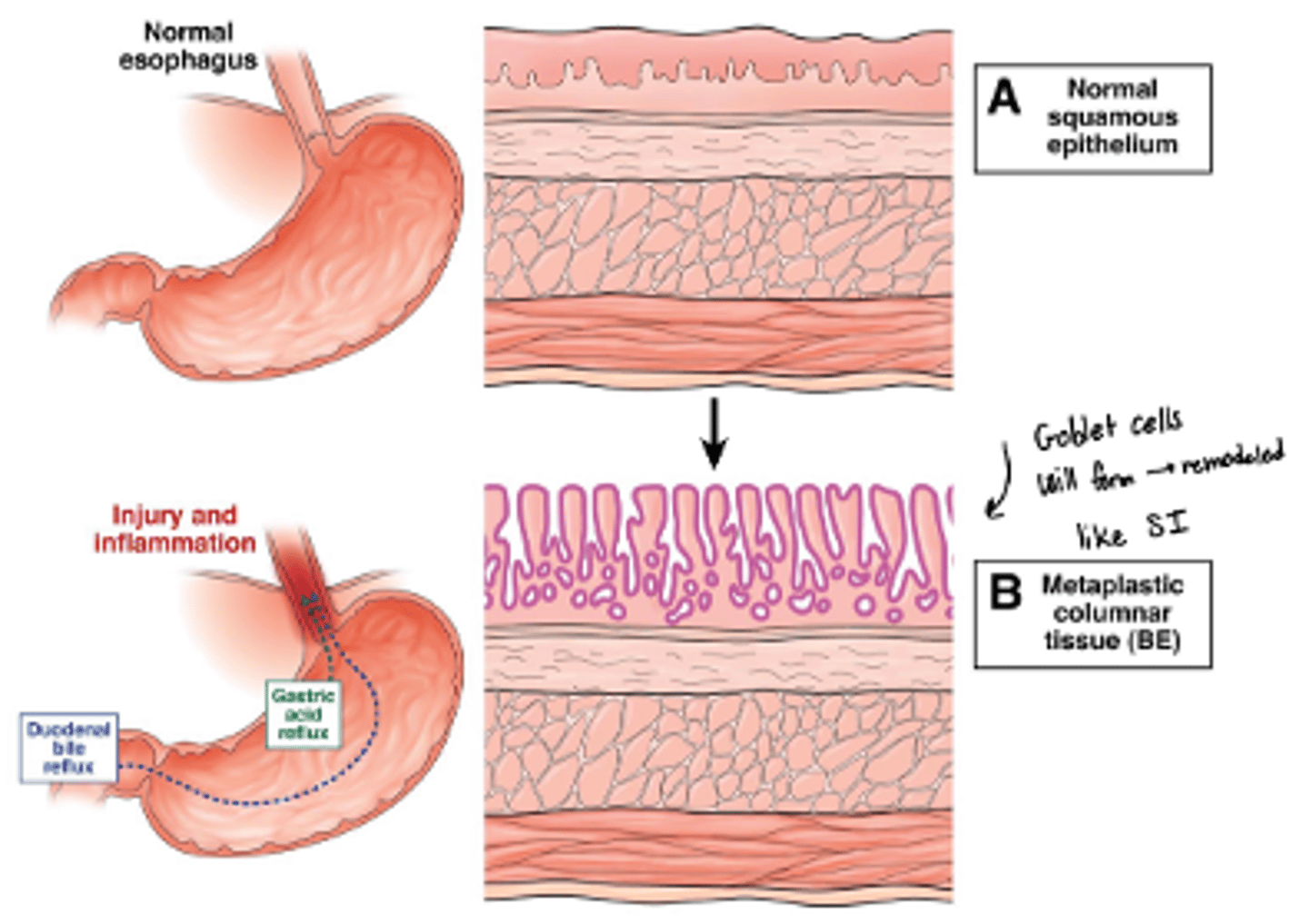
what is Barrett's epithelium
when normal esophageal lining or epithelium is replaced with abnormal epithelium
what things can cause ulcers?
o H/ pylori infection
o Excess inflammation
o Excess acid
o Infection
o NSAIDs
o Lifestyle
what are 3 protective features/mucosal defenses against ulcers?
o Prostaglandins
o Mucosal regeneration
o Mucus and bicarbonate production
what ultimately causes ulcers
an imbalance between defenses and aggressive factors
factors that defend the stomach and duodenum from self-digestion
o Mucus: continually secreted for protective effect
o Bicarbonate secreted from endothelial cells
o Blood flow: proper flow maintains mucosal integrity
o Prostaglandins: stimulate secretion of bicarbonate and mucus, promote blood flow, suppress secretion of gastric acid
what is H. pylori?
· gram negative bacteria that can live in the stomach and duodenum
what does H. pylori do to the stomach?
o Breakdown mucus layer due to inflammatory response by the presence of bacteria
o Produces urease which forms CO2 and ammonia which can damage the mucosal integrity
what must be present for an ulcer to form
gastric acid
gastric acid MOA in ulcers
Activates pepsin which acts with HCL in the injury of the mucosa (causes crater)
Decrease blood flow, causes decrease mucus production and bicarbonate synthesis and promotes gastric acid secretion
what does chronic use of NSAIDs cause
inhibits production of prostaglandins
what does smoking do to the GIT
nicotine stimulates gastric acid production
MOA of metaplastic transformation of esophageal lining
o Repeated injury and inflammation will break down the normal squamous epithelial layer of the esophagus
o Will grow back as columnar epithelium--> intestinal metaplasia (with goblet cells)
what is Zollinger-ellison syndrome (ZES)?
· Condition associated with one or more tumors in the duodenum or the pancreas
o Tumors are known as gastrinomas and secrete lots of Gastrin
what type of tumors are gastrinomas
neuroendocrine tumors
cause of Zollinger-ellison syndrome/gastrinomas
· Cause not fully understood but 25-30% of all gastrinomas are caused by inherited genetic disorder called multiple endocrine neoplasia type 1 (MEN1)
wermer syndrome (MEN1 mutation)
a rare disorder that causes tumors in the endocrine glands and parts of the small intestine and stomach
what levels should be tested if ZES is suspected?
blood gastrin levels
effect of excess gastrin production in ZES
· Excess gastrin production leads to extreme production of acid in the stomach eventually causing peptic ulcers. There are usually many ulcers in the affected area
symptoms other than ulcers seen with ZES
diarrhea, bloating, burping, nausea, vomiting, weight loss, poor appetite
prevalence of ZES
Extremely rare condition that can start at anytime but usually isn't diagnosed until ~50 years old
4 categories of action of drugs for peptic diseases
o Neutralizing gastric acid
o Reduce gastric acid secretion
o Enhance mucosal defenses/ "cytoprotectants"
o Antimicrobial activity
what are the 3 goals of treating peptic ulcer disease
-pain relief
-ulcer healing
-prevention of complications and ulcer recurrence
MOA of antacids
· Simply work by neutralizing hydrochloric acid
· They are weak bases that react with hydrochloric acid to form salts and water
· By increasing the pH of the stomach, antacids also inactivate pepsin (known to contribute to ulcer formation by digesting proteins in the stomach wall)
what pH level is pepsin activity significantly reduced?
pH>4
common antacid ingredients
o Aluminum hydroxide
o Magnesium hydroxide
o Calcium carbonate
o Sodium bicarbonate
3 parts of normal response to acid neutralization
o Increase gastrin release
o Increase acid output
o Increase volume of secretion
what is acid rebound
overproduction of HCl after stopping antacids
which ingredient in antacids are more likley to cause acid rebound
o Calcium carbonate is more likely to induce rebound vs Mg and Al-containing antacids
o Rapid vs slow acting antacids
what 2 factors determine the net buffering capacity of antacids
o Their ability to neutralize acid
o Time of residency in the stomach
aluminum hydroxide vs calcium carbonate antacids
aluminum hydroxide: act very gradually and their effects continue for several hours
calcium carbonate: act quickly and increase pH a lot so more likley to cause acid rebound
3 factors that affect how well a patient respond to antacids
o How much acid the patient secretes (hypersecretion)
o Rate at which antacids are emptied from the stomach
o Potency of the acid (ANC/ acid neutralizing capacity)
effect of aluminum-based antacids on GI motility
produce constipation
effect of Mg-containing antacids on GI motility
produce diarrhea
what is a possible consequence of absorption of un-neutralized sodium bicarbonate
can produce metabolic alkalosis
why should you be cautious with using antacids in patients with renal sufficiency
can cause some absorption of cations like Ca, Mg, Al, and Na
DDI of antacids
May chelate other drugs (avoid concomitant administration of other drugs such as tetracyclines, digoxin, propranolol)
what are the 3 histamine-2 receptor antagonists
famotidine, cimetidine, and nizatidine
MOA of histamine-2 receptor antagonists
· Are competitive inhibitors of H2 receptor in parietal cells
· H2 blockers also decrease (indirectly) gastrin and ACh-induced gastric acid secretion
3 effects of H2 antagonism
reduction in...
o Volume of gastric juices secreted
o Gastrin secretion
o H+ concentration
what are the 4 uses of histamine-2 receptor antagonists
o Duodenal ulcers, gastric ulcers, ZES, and GERD
adverse effects of H2RAs
usually well-tolerated
D, HA, muscle pain, constipation, fatigue
cimetidine DDI
inhibits CYP450-mediated drug metabolism
cimetidine effects other than on histamine
anti-androgenic effects by antagonizing the androgen receptor and increases estrogen levels by inhibiting its CYP-mediated metabolic inactivation
o gynecomastia in men
o galactorrhea in women
dicyclomine brand name
Bentyl
MOA of dicyclomine (lentil)
antagonizes the muscarinic ACh-R on parietal cells therby decreasing gastric acid secretion
why are anticholinergic agents rarely used?
because they're less effective and have less desirable side effects
ADEs of anticholinergic agents
o Dry mouth
o Blurred vision
o Cardiac arrythmias
o Urinary retention
what are PPIs
substituted benzimidazole prodrugs that block the activity of this transport protein for proton (H+) molecules
what cell type are proton pumps unique to?
parietal cells
what facilitates the MOA of PPIs
the pH of the stomach
PPI MOA
Irreversibly inhibit the H+/K+-ATPase in gastric parietal cells
o Produces dose-dependent inhibition of gastric acid secretion that persists even after the drug disappears from the plasma
what environemnt are PPIs active vs inactive
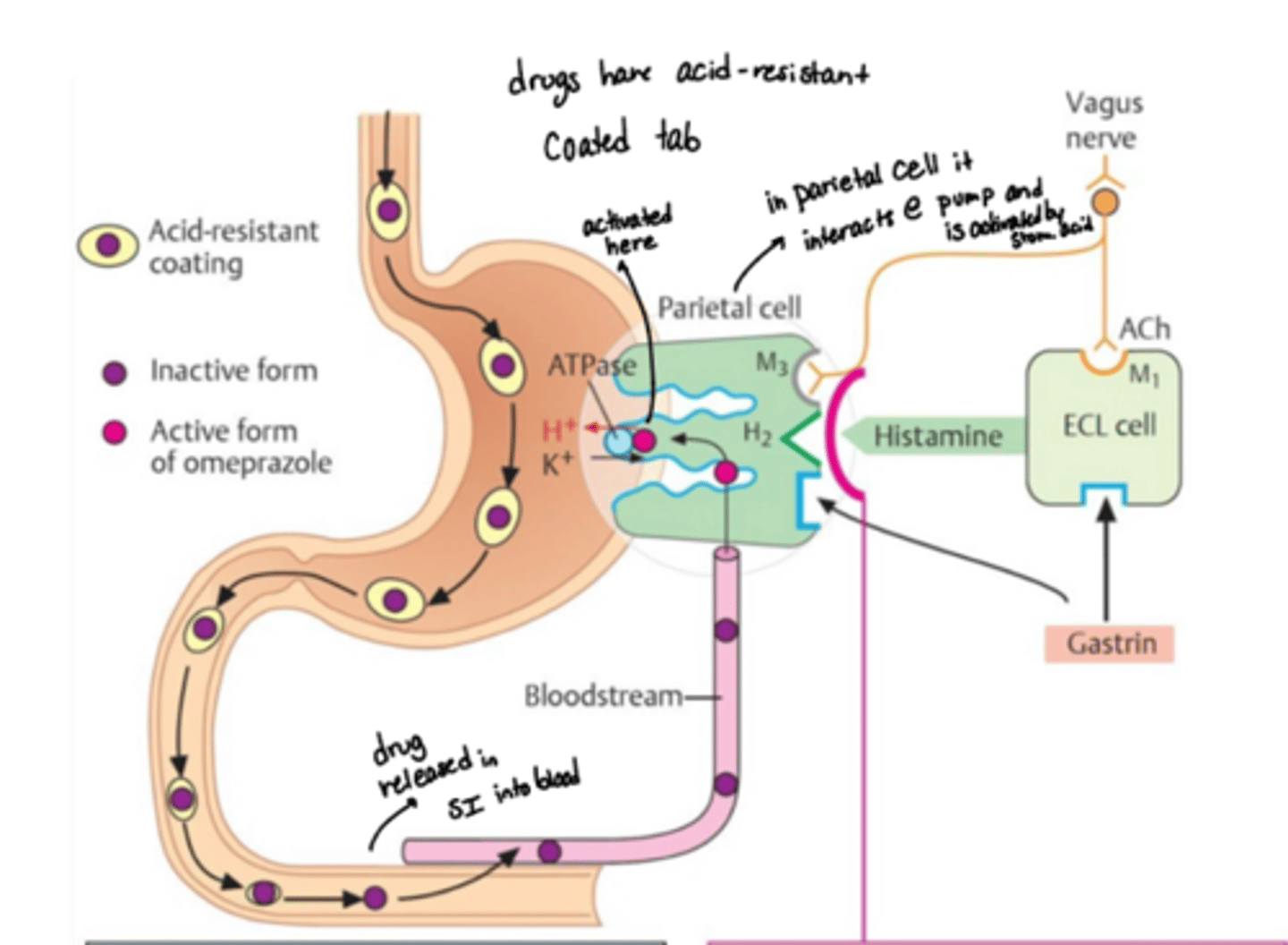
PPIs are inactive at neutral pH, but they are weak bases so in acidic stomach they’re activated
how are PPIs activated from their prodrug form?
require activation from the parietal cell canaliculus (side of cell that faces the acidic lumen of the stomach)
o PPIs are activated only when bound to the proton pump and exposed to the acid of the stomach
describe the release path of PPIs
· PPIs need to pass intact through the stomach into the intestines where the drug is released from its enteric coating formulation for absorption into the blood
· The pro-drug reaches the parietal cells via blood
· The pro-drug then diffuses into the canaliculi of parietal cels facing the lumen where the acidic environment converts the pro-drug into a sulfonamide reactive intermediate
· The active drug then binds to sulfhydryl groups of cysteine residues in the pump, leading to irreversible activation
PPI and infections
increase in pH may mean other bacteria may be able to tolerate the environment (C. diff, salmonella, E. coli)
DDI of PPIs
competition with clopidogrel for CYP2C19
both these drugs need to be activated by this enzyme
PPI possible side effects?
osteoporosis and bone fractures from decreased absorption of Ca in higher pH
kidney disease and dementia associations
how does mucosal erosion and ulceration occur in peptic acid diseases
pepsin-mediated hydrolysis of mucosal proteins
MOA of mucosal protective agents
create a barier in stomach and intestinal mucosa that prevents damaging effects of HCl and pepsin
they also bind pepsin and bile salts
misoprostol brand name
cytotec
what is mistoprostol and when is it used
o Prostaglandin E1 analog (PG stimulate mucus and bicarbonate production)
o Used when treatment with NSAIDs inhibits endogenous PG synthesis
when should mistoprostol not be used
in women of child-bearing potential
sulcralfate brand name
carafate
what is sucralfate made of
Complex of aluminum hydroxide and sulfated sucrose
MOA of sucralfate
o Undergoes polymerization and cross linking at low pH of stomach
o Binds tightly to the necrotic/ulcerated tissue
o Forms complex gel with mucus; mucus stabilized; diffusion of HCL and pepsin to mucosa is impaired
why does sucralfate have little side effects
not absorbed into the blood
duodenum and sucralfate
Although the pH of duodenum is >4, sucralfate retains its viscosity and binds tightly to the ulcerated intestine as well
colloidal bismuth compounds MOA
o Second coating agent (not mucus-like)
o Bismuth salts combine with mucus glycoproteins to form a barrier that protects the ulcer from further damage by acid and pepsin
o Bismuth is also known to stimulate secretion of bicarbonate, PG, and mucus
colloidal bismuth effect on H. pylori
o Colloidal bismuth has been shown to impede the growth of H. pylori
§ used in combination with antimicrobial agents and PPIs in patients that are H. pylori positive
what is H. pylori
gram-negative, spiral shaped bacterium that is flagellated
what is the most common cause of non-NSAID associated peptic ulcer disease?
H. pylori