Basics of Suturing
1/31
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
32 Terms
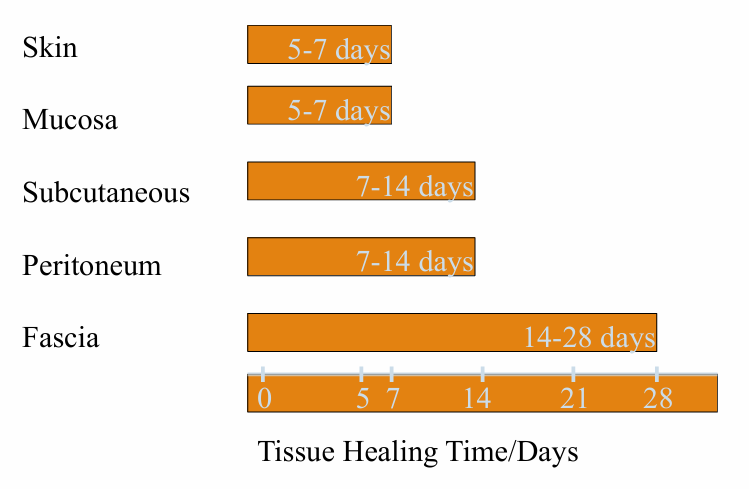
critical wound healing period
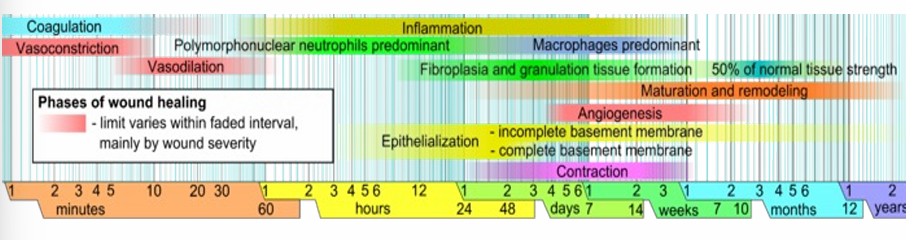
model of wound healing
1) hemostasis: within minutes post-injury, platelets aggregate at the injury site to form a fibrin clot
2) inflammatory: bacteria and debris are phagocytosed and removed, and factors are released that cause the migration and division of cells involved in the proliferative phase
3) proliferative: angiogenesis, collagen deposition, granulation tissue formation, epithelialization, and wound contraction
4) remodeling: collagen is remodeled and realigned along tension lines and cells that are no longer needed are removed by apoptosis
surgical wound classification- clean
-1-5% risk of infection
-operative incisional without penetrating infectious organs
surgical wound classification- clean-contaminated
-3-11% risk
-operative wounds in which the respiratory, alimentary, genital, or urinary tract is entered under controlled conditions and without unusual contamination
-biliary tract, appendix, vagina, and oropharynx
surgical wound classification- contaminated
-10-17% risk
-open, fresh, accidental wounds, operations with gross spillage from GI tract
surgical wound classification- dirty or infected
->27% risk
-old traumatic wounds, necrotic tissue, perforated viscera
-postoperative infection predicted
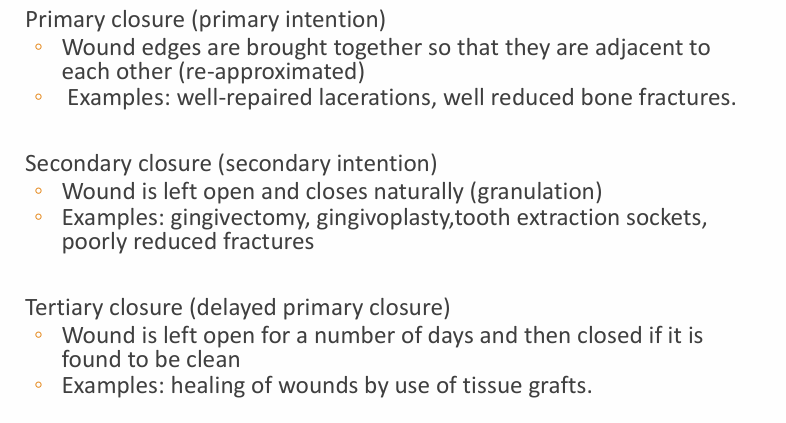
closure types
sutures
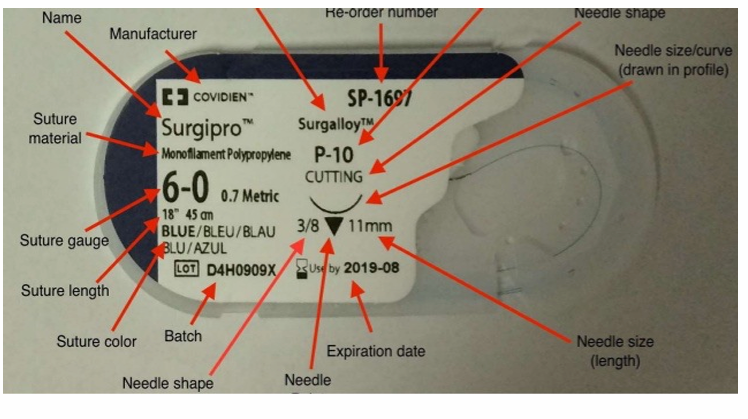
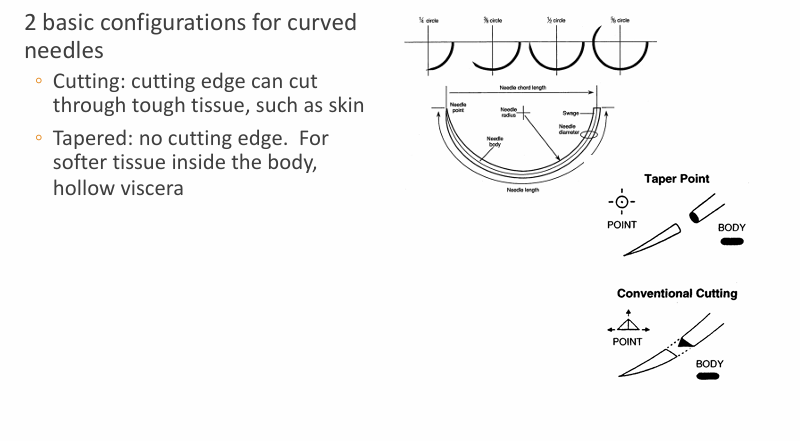
suture needles
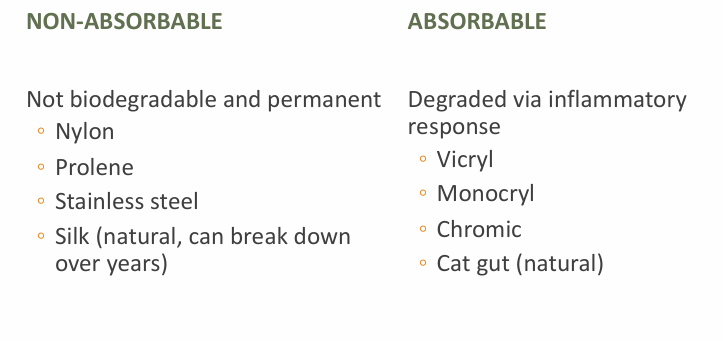
types of sutures- non-absorbable v. absorbable
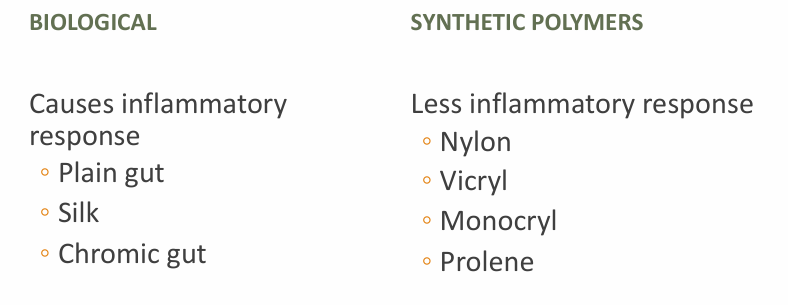
types of sutures- biological v synthetic polymers
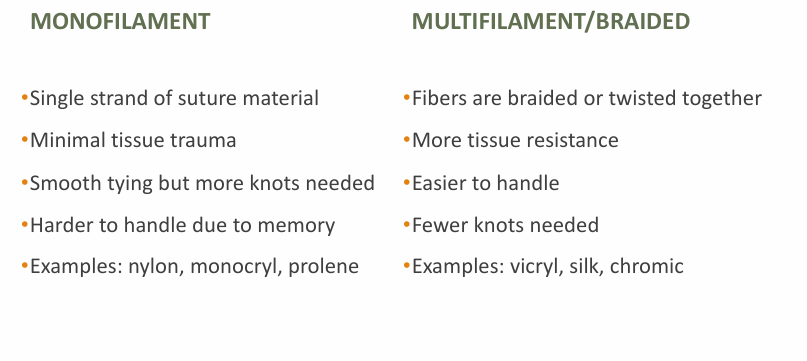
types of sutures- monofilament v multifilament/braided

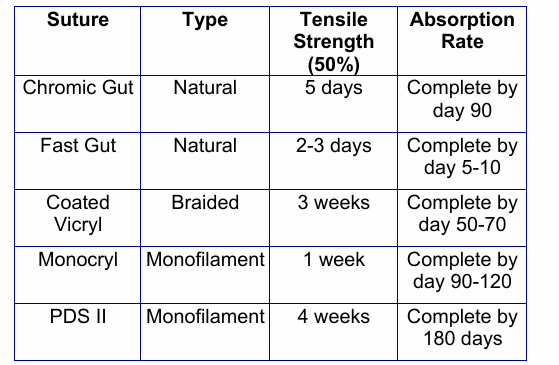
chromic gut, fast gut, coated vicryl, monocryl, PDS II
suture selection
-do not use dyed sutures on the skin
-use monofilament on the skin as multifilament harbor bacteria
-non-absorbable cause less scarring but must be removed
-absorbable for mucosa, GI, biliary, GU
-non-absorbable for skin, tendons, fascia
-cosmetics = monofilament, subcuticular
-location and layer, patient factors, strength, healing, site, availability
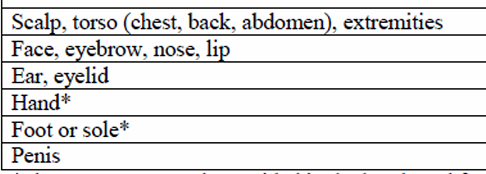
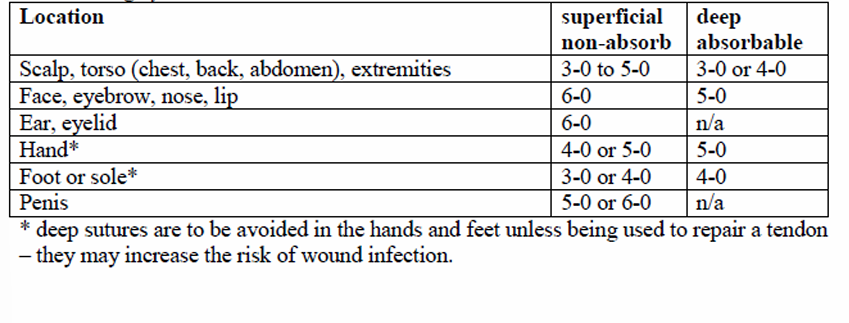
suture sizes- location, superficial non-absorb, deep absorb
general guidelines- face (except eyelids)
-deep dermal: 4-0 vicryl
-superficial: 6-0 nylon/prolene OR 5-0 fast gut
general guidelines- intraoral/tongue
-deep/muscle: 3-0/4-0 vicryl
-superficial: 3-0 chromic gut
general guidelines- scalp
-deep dermal/galea: 3-0 vicryl
-superficial: 4-0 nylon/prolene OR 3-0 chromic gut OR staples
anesthetic solutions- lido and lido with epi
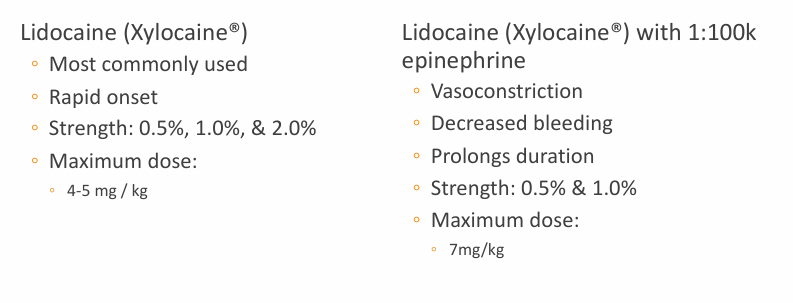
anesthetic solutions- cautions
-due to its vasoconstriction properties, avoid using lidocaine with epinephrine on:
-ears, nose
-fingers, toes
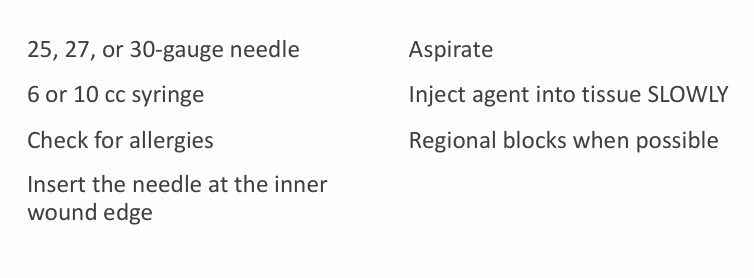
injection techniques
types of closures
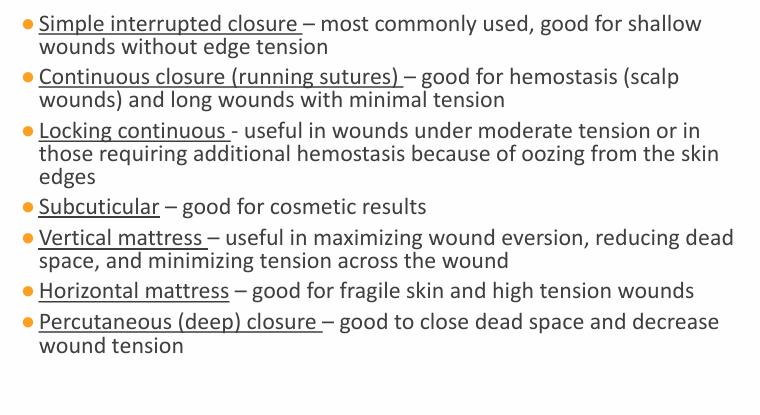
simple interrupted suturing
-stitch is tied separately
-used in skin or underlying tissue layers
-more exact approximation of wound edges can be achieved with this technique than with the running stitch
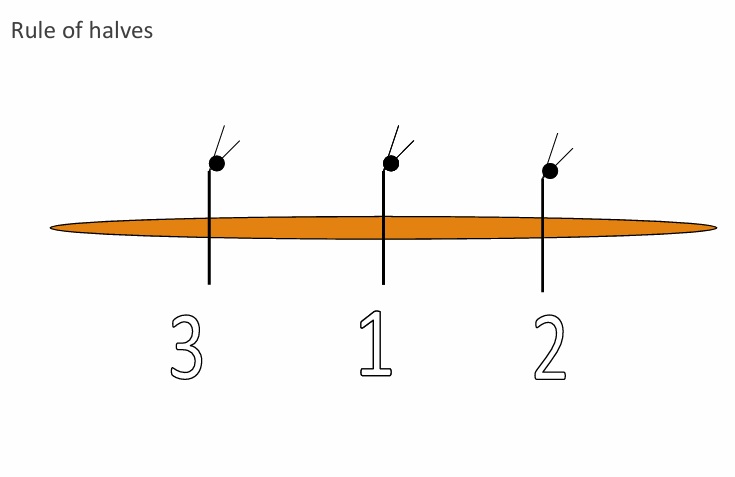
-rule of halves: matches wound edges better, avoids dog ears, vary from rule when too much tension across wound
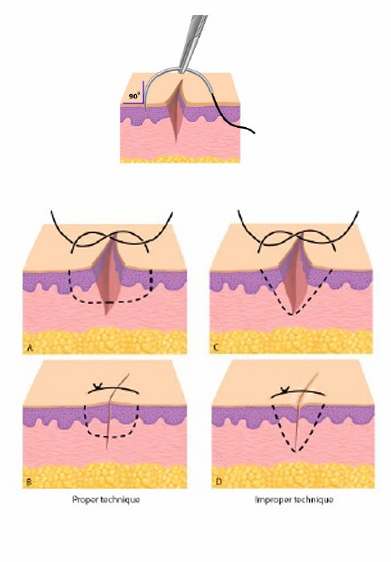
suturing technique
-needle enters skin with a 1/4-inch bite from the wound edge at 90 degrees
-use the forceps and lightly grasp the skin edge and arc the needle through the opposite edge inside the wound edge taking equal bites
-rotate writs to follow arc of the needle
-principle: minimize trauma to the skin, don’t bend the needle, follow path of least resistance
-evert wound edges, scars contract over time
finishing the simple interrupted suture
-do not position knot directly over wound edge
-number of throws depends on size of suture: 3-0 = 3 throws, 6-0 = 6 throws
-on each throw, reverse the order of wrap
-cut the ends of the suture 1/4-inch from knot
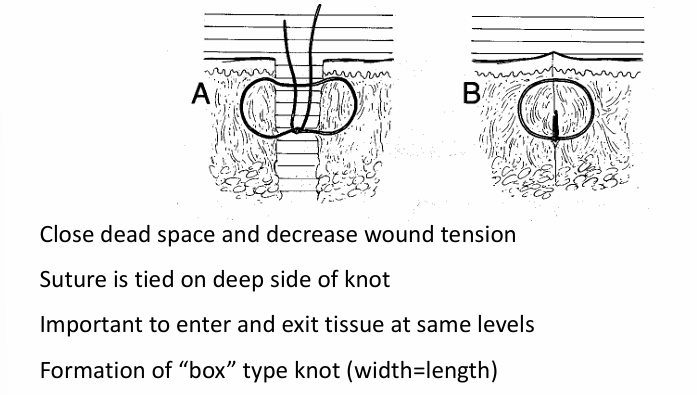
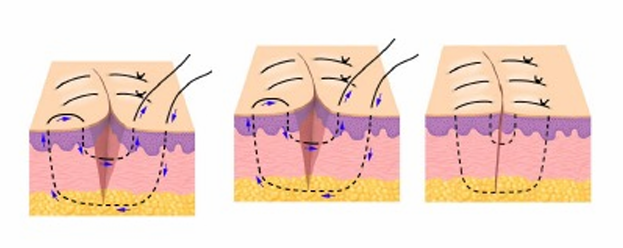
deep suture technique
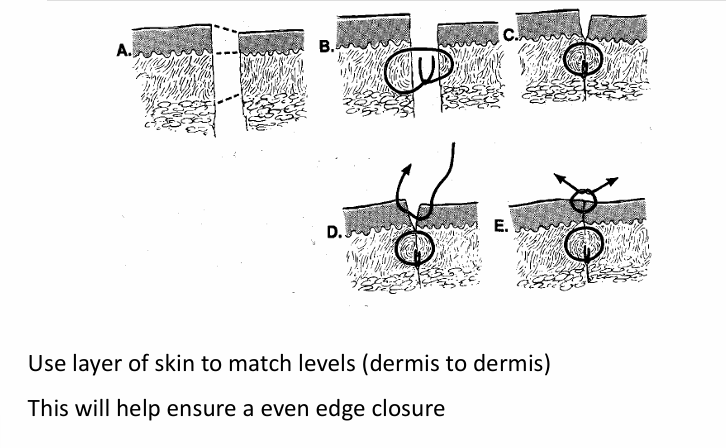
matching uneven skin edges
continuous locking and non-locking sutures
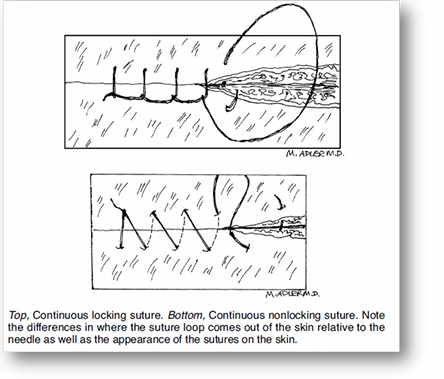
running or continuous stitch
-made with one continuous length of suture material
-close tissue layers which require close approximation
-speed of execution, and accommodation of edema during the wound healing process
-greater potential for mal-approximation of wound edges with the running stitch than with the interrupted stitch
-needle at a 90 degree angle to the skin within 1-2mm of the wound edge and in the superficial layer
-exit through the opposite side equidistant to the wound edge and directly opposite the initial insertion
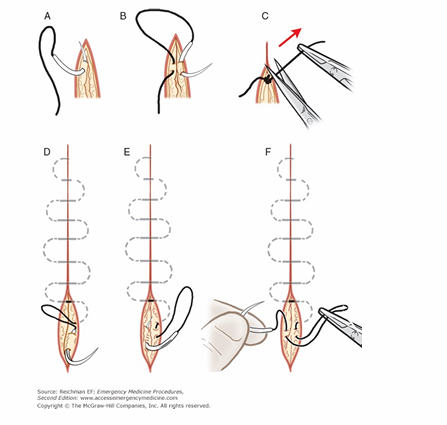
subcuticular suture
-usually for closing surgical incisions
-require clean wound edges
-best cosmetic result
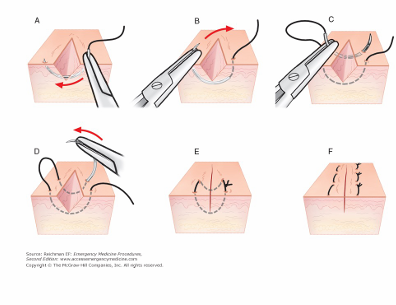
vertical mattress
-good for everting wound edges and areas with high tension (over joints, chest, back)
horizontal mattress
-good for wounds under high tension (back, chest, over joints)
-good for hemostasis