The Gastrointestinal System: Gastrin/Paracrine/Enzyme Secretion in the Gastric Phase and the Intestinal Phase
1/64
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai | Chat |
|---|
No analytics yet
Send a link to your students to track their progress
65 Terms
G cells
secrete gastrin, does NOT respond to ACh like other cells (triggered by GRP and more strongly by AAs)
found deep in the pits of the stomach
inhibited by SST
gastrin
hormone in the stomach secreted by G cells with 2 major functions: indirectly secreting more H+ ions (stimulate acid release) and stimulate mucosa growth in stomach and small/large intestine (innermost layer renewal is important)
works on top of parietal cells (trigger their release of more H+) and ECL cells to stimulate acid release and mucosa growth in stomach/SI/LI
triggered by GRP (long loop) and amino acids (short loop, favored over GRP) from digested food
inhibited by too acidic environment (ulcer risk) and SST
what triggers and inhibits gastrin secretion from G cells?
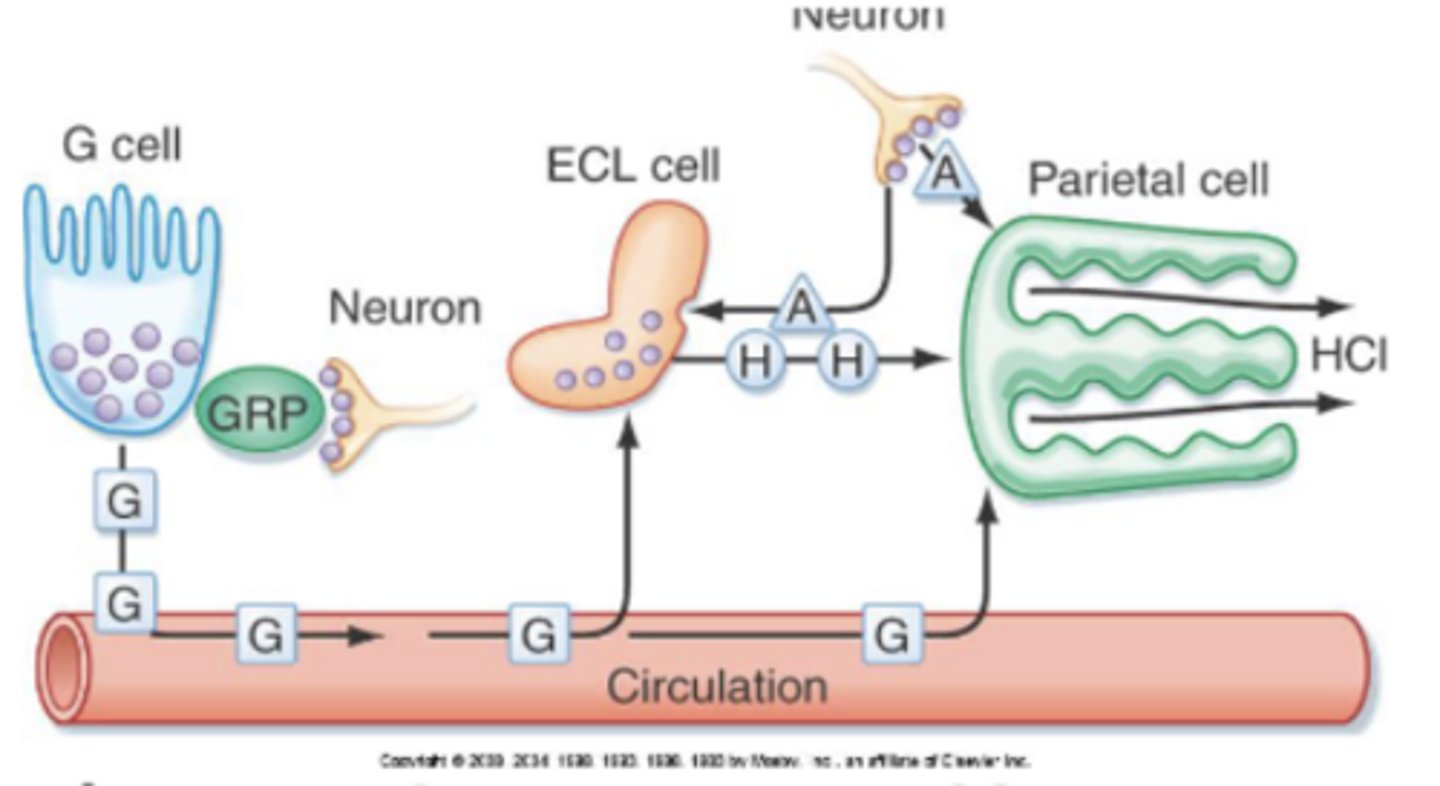
vagus nerve stimulation via nervous input (seeing/smelling/thinking of food) → releases the NT gastrin-releasing polypeptide (GRP) to activate G cells
long loop
what triggers the release of GRP?
gastrin into blood from G cells → reaches ECL cells and parietal cells
reach ECL cells → secrete histamine → bind to H2 receptor on parietal cell (strong stimulus) → HCl production
reach parietal cells → bind to CCK-B receptor → HCl production
***bc there are 2 ways to stimulate HCl production, this is a strong method of stimulation on parietal cells
describe the pathway of gastrin acting on other stomach cells
D cells
secrete somatostatin when activated by high acidity
somatostatin (SST)
hormone secreted by D cells that is the major "breaker" in the stomach bc it inhibits most other cells (primary feedback signal)
to reach homeostasis, D cells respond to H+ ions where high acidity activates D cells to make SST and inhibit the activity of other cells
this inhibits meal-stimulated gastrin secretion
what triggers and inhibits SST secretion from D cells?
paracrine secretion
local-acting secretion (secreted directly into tissue to affect neighbor cells)
histamine, intrinsic factor, and SST
intrinsic factor
protein produced by parietal cells critical for B12 absorption (and thus RBC production/ileum absorption); similar mechanism stimulates secretion of this as HCl
most important secretion in the stomach bc vitamin B12 is vital for absorption of nutrients in ileum and RBC production → issues with this can cause pernicious anemia, and its function allows you to still survive (as long as you take care of B12 intake and eat small meals) if large parts of stomach are removed/parietal cells are damaged
pepsin
enzyme secreted by chief cells in its inactive form, which is only activated into this in acidic environment (triggered by H+ or presence of itself)
function of breaking down proteins (ex. collagen), but when pH get more basic when it moves into SI it no longer functions (i.e. only works in stomach)
gastric lipase
co-secreted with pepsin, important for fat digestion (which mainly does not occur in the stomach though)
vagus nerve activation (visual stimulation, smell of food, etc.) releases NTs that stimulate cells to secrete
uses ACh to stimulate chief cells (enzyme secretion), parietal cells (HCl and intrinsic factor secretion), and ECL cells (strong stimulation of parietal cells)
uses GRP to stimulate G cells
describe long loop activation as a control mechanism of gastric secretion
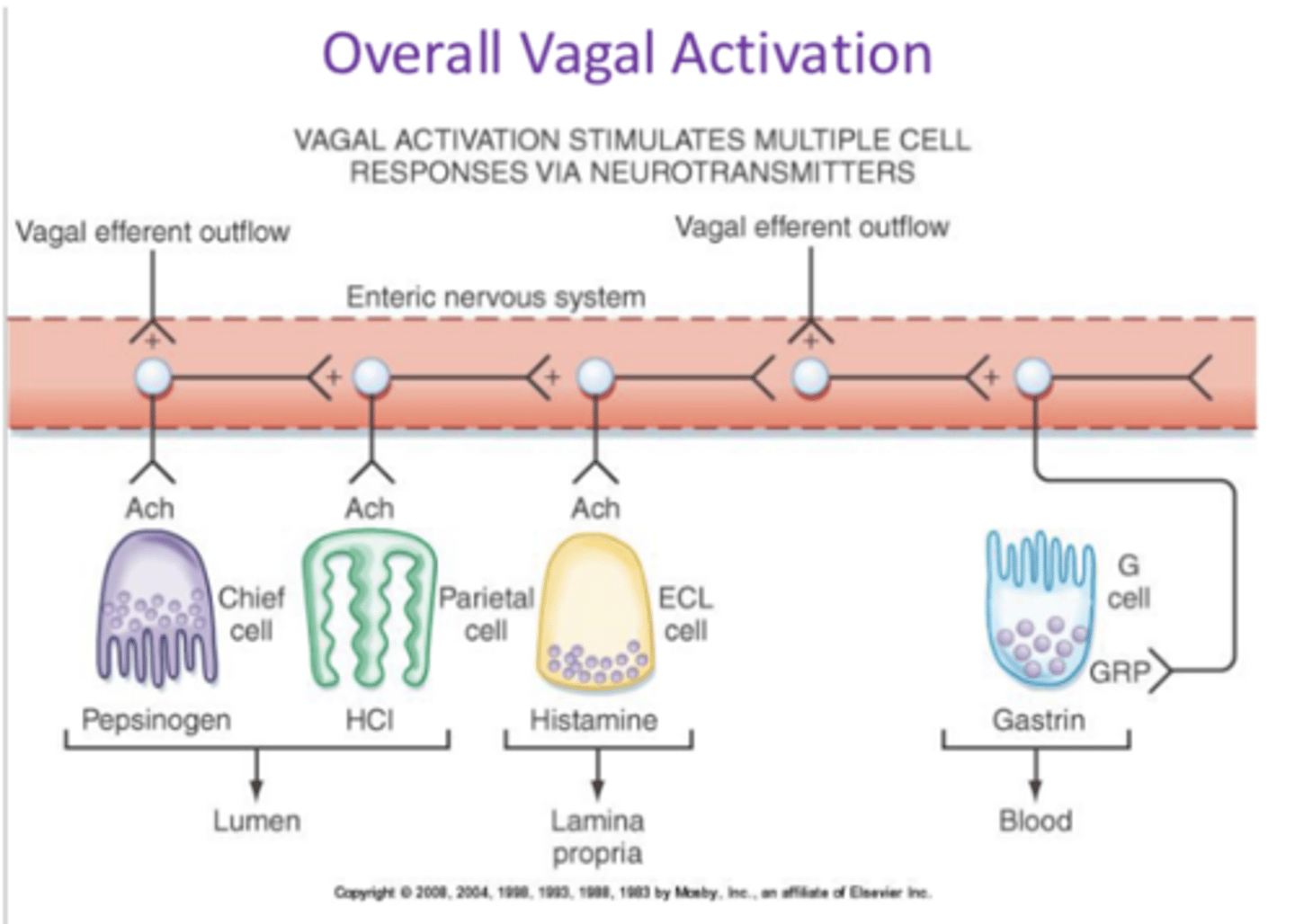
ACh (in gastric secretion)
neurotransmitter of the parasympathetic NS that activates chief, parietal, and ECL cells
food arrives in stomach → enteric nervous system activated → activate G cell via AAs (ex. from collagen breakdown in acidic enviro)→ gastrin
describe short loop activation as a control mechanism of gastric secretion
ECL cells
secrete histamine when activated by ACh and gastrin
inhibited by SST
histamine
secreted by ECL cells (stimulated by gastrin and ACh) very strong activator of parietal cells via Gs pathway to secrete acid
parietal cells
secrete HCl (gastric acid) and intrinsic factor when stimulated by ACh, gastrin, and histamine
inhibited by SST
HCl/H+ (in gastric secretion)
triggers D cells and chief cells, inhibits G cells
secreted by parietal cells
chief cells
secrete pepsinogen (pepsin when active) and gastric lipase when stimulated by ACh and H+
inhibited by SST
the nervous system → vasovagal activation (enteric NS)
content and volume, enteric NS
Motility is mostly conducted through ___. The ___ and ___ of food you eat activates ___, which modulates motility in the stomach
vasovagal activation (of motility)
causes stomach to contract → diff regions of stomach and phases of digestion have diff patterns of contraction
neurons can be activated by mechanical stimulation (e.g., distention)
enomechanical stretch receptor (mechanoreceptor): when you eat a lot stomach walls stretch
how does volume modulate motility in the stomach?
neurons also can be activated by chemical stimulation (e.g., presence of products of protein digestion)
when you eat, proteins are detected by chemical receptors
how does content modulate motility in the stomach?
proximal = reservoir/storage (fundus, body); where relaxation (receptive/adaptive) occurs
distal = pump/grinder (antrum, pyloric sphincter) where mixing/peristalsis occurs
proximal vs distal portion of stomach
receptive relaxation
relaxation of stomach muscles as food moves through esophagus and enters stomach
vagus activation (anticipation of food → neural activity), presence of food → nervous activity relaxes upper portion of stomach in anticipation of food arrival
adaptive relaxation
relaxation of stomach muscles when filled; when food does arrive and stretches stomach walls, mechano/chemo receptors activate short loop and cause stomach to react even further
VIP and NO trigger relaxation of smooth muscle
no, it's limited bc its walls are not specialized for absorption and instead are specialized for protection (only aspirin/other weak acids and alcohol (EtOH) can be absorbed and enter blood)
protection mechanisms: thick basic mucus and HCO3 layer, tight junctions bw epithelial cells (limited paracellular transport), and rapid replacement of lining (every 5 days) by GI stem cells
is there lots of absorption in the stomach, and what is its walls specialized for?
gastric ulcers
destruction (necrosis) of the stomach lining of the gastric mucosa (irritation) caused mainly by bacteria (H. Pylori)
taking antacids can provide relief (since it temporarily limits acidity), but only taking antibiotics addresses the root of the problem/cure it (bc it kills the bacteria that cause it)
can also be caused by oversecretion of G cells/acid (Zollinger-Ellison syndrome) and NSAID (inhibited mucus production)
the intestinal phase
series of responses after chyme enters the SI, and the rate of this relies on stomach function
includes control of gastric emptying, motility/secretion of SI, secretion of accessory organs, and digestion/absorption of fat/carbs/proteins
duodenum
first segment of SI; common bile duct (secrete bile) and pancreatic duct (pancreatic secretions)
jejunum
middle segment of SI; profound villi and microvilli to increase SA, most absorption happens here
ileum
final segment of SI; peyer's patch and lymph nodes (immune response), ileocecal valve (connect to LI)
circular folds/plicae
permanent (don't disappear when SI expands), deep folds of the mucosa and submucosa in the SI that enhance absorption by increasing surface area and slowing the passage of the partly digested food
gastric emptying
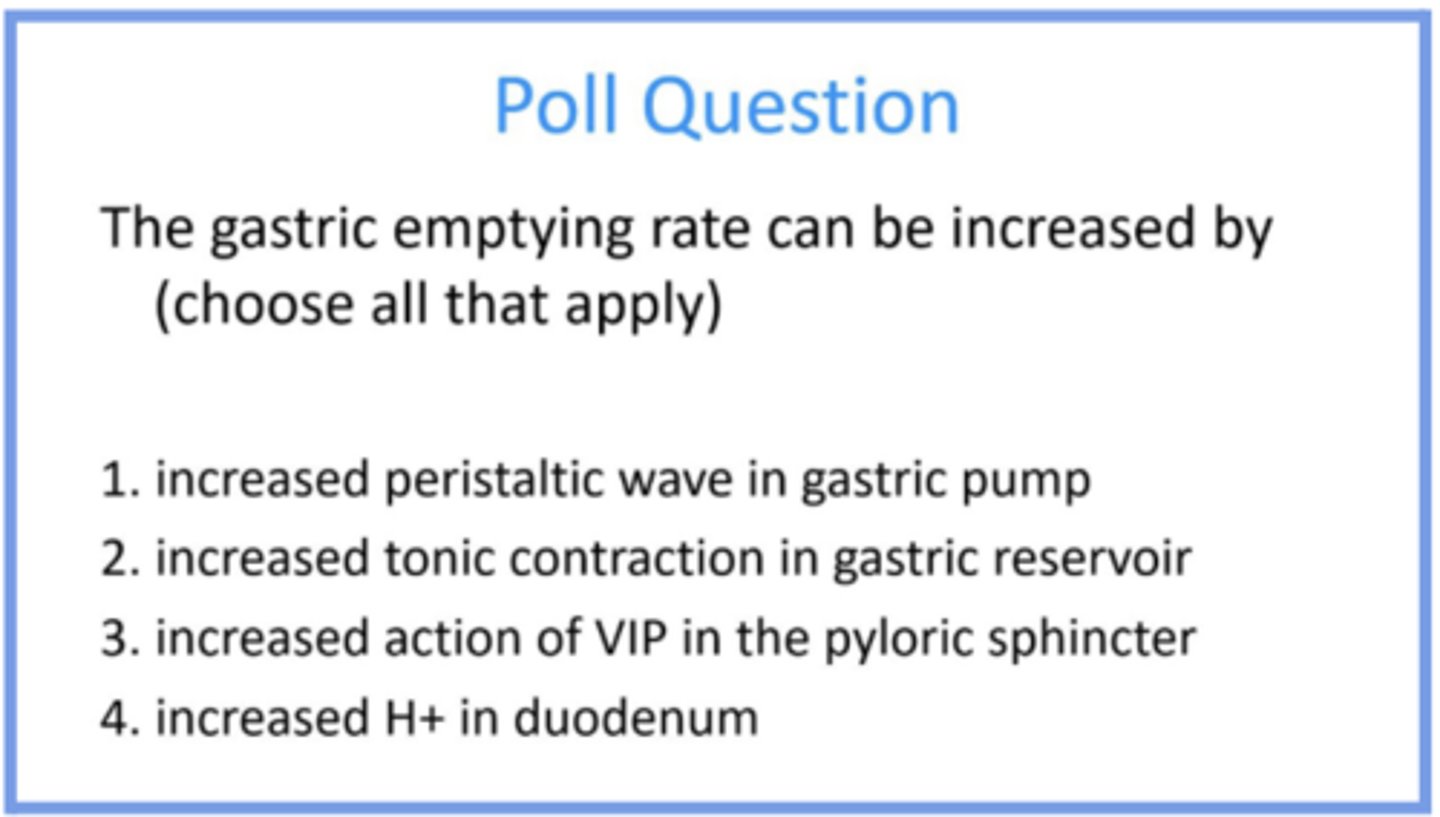
food from stomach's controlled movement into SI; strong peristaltic waves in gastric pump (antrum/distal stomach) coupled with increased muscle tone in reservoir (instead of typical relaxation → tonic pressure) and opening of pylorus (NO and VIP)
duodenum also has to be relaxed to let food through → inhibition of duodenal segmental contractions
pylorus/pyloric sphincter
muscular sphincter between stomach and duodenum that controls gastric emptying
promoted by gastric volume, neural (stretching signal), and gastrin (amount of hormone)
inhibited by distension and acid in the duodenum (enterogastric reflex) and hormones (GIP, CCK, secretin)
what promotes and inhibits gastric emptying?
mechano and chemo receptors → integrate signals to communicate if more should be sent into SI (avoid damage from acid)
distension = processed by mechanoreceptors
acidity from contents in SI (not protected from acid) = chemoreceptors
what kind of receptors are present in the SI that impact gastric emptying?
GIP
digested glucose detected by SI triggers secretion of this hormone, which tells stomach to slow down and travels all over the body
CCK (cholecystokinin)
secreted by I cells (mucosa of the upper small intestine) and stimulates pancreatic enzyme secretion (augment secretin functions), contraction of gallbladder, relaxation of sphincter of Oddi, and inhibits gastric emptying and gastric secretion
"gallbladder mover" bc contracts gallbladder walls to secrete bile
secretin
secreted by S cells (mucosa of the upper small intestine) and stimulates pancreatic bicarbonate secretion (augment CCK functions) in response to acid, and inhibit/slow gastric emptying and gastric secretion
bicarb secretion opposes increase in acid
increasing pumping increases rate its contents are pushed out
increased pressure in reservoir = decrease volume and push more food down towards pump area, and increased contraction there pushes it towards pyloric sphincter
want less resistance in pyloric sphincter when more food is pushed through it (use VIP or NO)
more H+ (more acidic) in duodenum is bad in the SI because it creates ulcers, so if there is more H+ in it it signals less to be sent to it (decrease gastric emptying) and also triggers secretin
answer the question and provide reasoning for each answer option
dumping syndrome
gastrectomy (surgical removal of part of stomach/SI) may lead to loss of feedback control of emptying bc the reservoir is removed, causing undigested, sugary food to "dump" directly into the SI which draws in fluid and causes rapid, symptomatic digestion
symptoms include hyper/hypo glycemia (which cause most of the other symptoms), malabsorption, fast HR, sweating, nausea, diarrhea, and vomiting
can be controlled by altering diet (limiting amount of food/type food)
normally before you eat, your body prepares for you to release insulin from the pancreas → then when you eat you do not have a "shock" of glucose
in dumping syndrome you don't have anticipation/preparation to increase insulin when stomach/SI is smaller bc food moves through it so quickly → when you do eat, you get a rapid spike in glucose (hyperglycemia) and a spike in insulin (drives glucose into cells), then a big drop in glucose (hypoglycemia) because all the food has been processed
describe what normally happens vs what happens in dumping syndrome that affects glucose absorption
partly digested food draws excess fluid (ECF) into the SI bc of the excess glucose
why is fluid drawn in in dumping syndrome?
slow propulsion and lots of segmentation (little peristalsis) to allow mixing of enzymes/secretion with food to facilitate digestion; driven by frequency gradient since contractions gradually decrease down the SI to allow slow movement of food through it (from more to less contracting region)
higher at beginning of SI (duodenum) at ab 12 cpm, but lower at end in ileum at about 8cpm
villi allow broken down nutrients to pass through
what type of contraction is prominent in the SI, and what is the pattern of it?
migrating motor complex
about 2 hours after you eat when food is already absorbed, waves of contraction "sweep" along the SI to remove excess debris and move it into the LI; happens in anticipation/need for eating
each wave ends a little more distal and starts a little less proximal
simulated by motilin (hormone secreted by SI during fasting)
inhibited by eating because you don't want sweeping when you have food there to allow for nutrient absorption
what stimulates and inhibits the migration motor complex?
triggered by digested fat (fatty acids) which affects bile release and pancreatic enzyme secretion, but also by AAs and peptides more weakly
inhibited when products of digestion move through the SI into the lower portion because CCK is only secreted in the upper regions of the SI
what stimulates and inhibits CCK release?
triggered by acid mainly, but also by products of protein digestion
inhibited when products of digestion move through the SI into the lower portion because secretin is mainly secreted in the upper regions of the SI
what stimulates and inhibits secretin release?
liver functions
metabolic regulation (responding to changes in glucose/cholesterol and making adjustments, like release/store/make glucose/LDL, etc.), maintains normal blood glucose levels, carb/lipid/AA metabolism
produces bile, plasma protein, clotting factors, and cholesterol
stores iron, glycogen, blood, fat-soluble vitamins
detoxification of alcohol and other drugs
bile
synthesized by hepatocytes and composed of cholesterol based salts, bilirubin, cholesterol (only way to get rid of it when this is excreted, not recycled), and HCO3
stored in the gallbladder
hepatocytes
liver cells; synthesize bile and macronutrients, detoxification
bile duct
where generated bile is released into, which eventually leads to the gallbladder
portal veins
vessels that directly come from GI system and lead to the liver
hepatic artery
vessels that branch from heart and provide O2/nutrients for liver cells or bring nutrients you absorb in GI system to get processed
secretin increases secretion of bicarb by biliary tract (channel for bile to travel in), and can increase secretion of bile as well because it draws in water/fluid
CCK causes contraction of gallbladder and release of stored bile by opening the sphincter of Oddi, and can go to vagus nerve and affect contraction via ACh or increase NO and VIP
how do secretin and CCK work together to affect bile release into the duodenum
in duodenum it acts (does its job)
rescued via enterohepatic circulation; passively absorbed in duodenum into portal veins so it's brought right back to the liver to be reused, actively absorbed in terminal portion of ileum
also can be excreted, which is the only route to dispose cholesterol
describe the path/circulation of bile
pancreas
has exocrine (secretions from cell surface into lumen/"out" of body) and endocrine function (hormones/islets of langerhans) influenced by CCK, secretin, and nervous (vagus/parasympathetic) stimulation
secreted enymes include precursor of proteases, lipase, and amylase
also secretes HCO3
islets of langerhans
release insulin and glucagon (hormones) into blood
acinar portion of pancreas
secretes enzymes, affected by CCK; in high fatty acid CCK is secreted and increases enzyme production
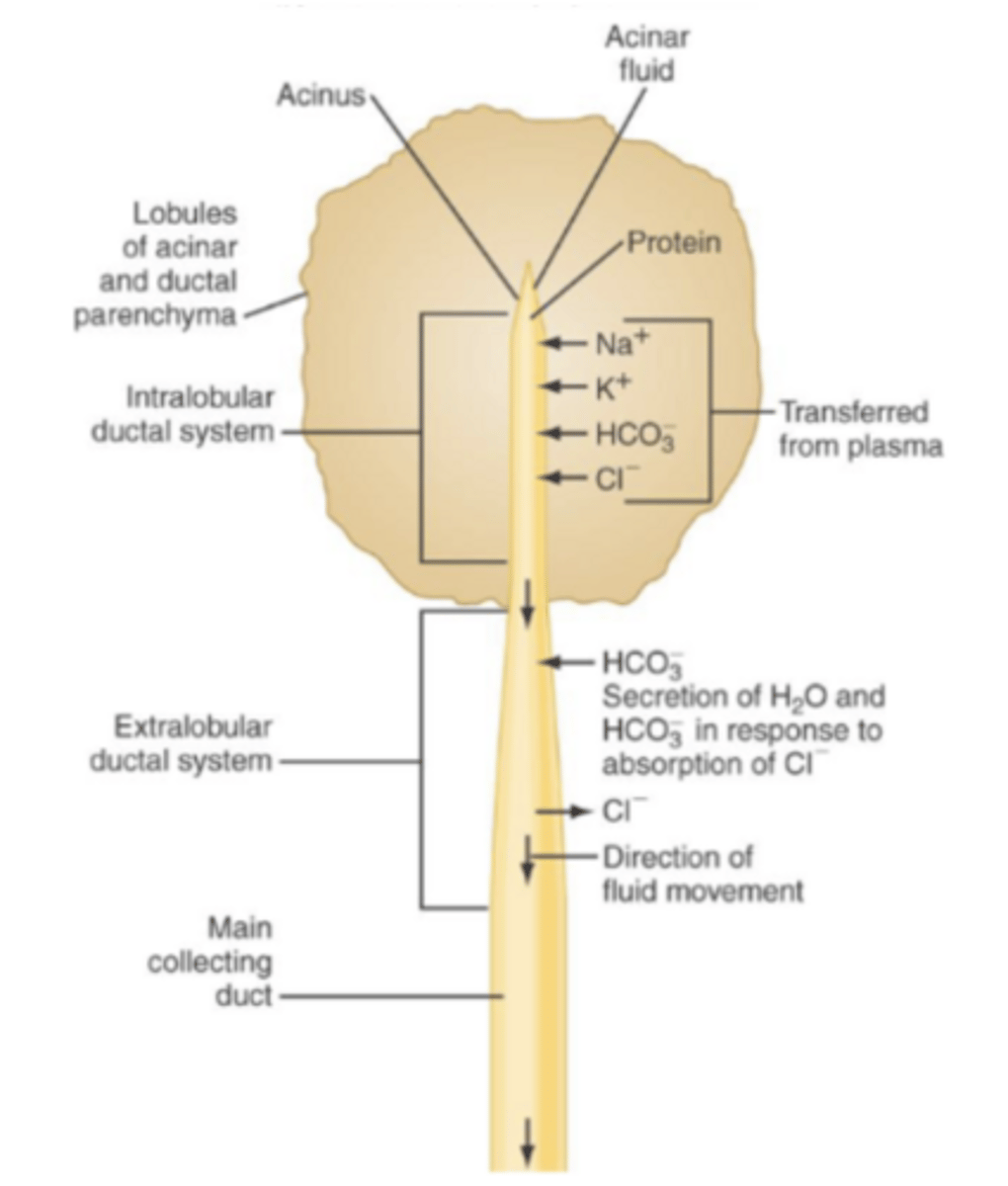
ductal portion of pancreas
affected by secretin; in low pH more secretin is secreted and increases HCO3 concentration in pancreatic secretions
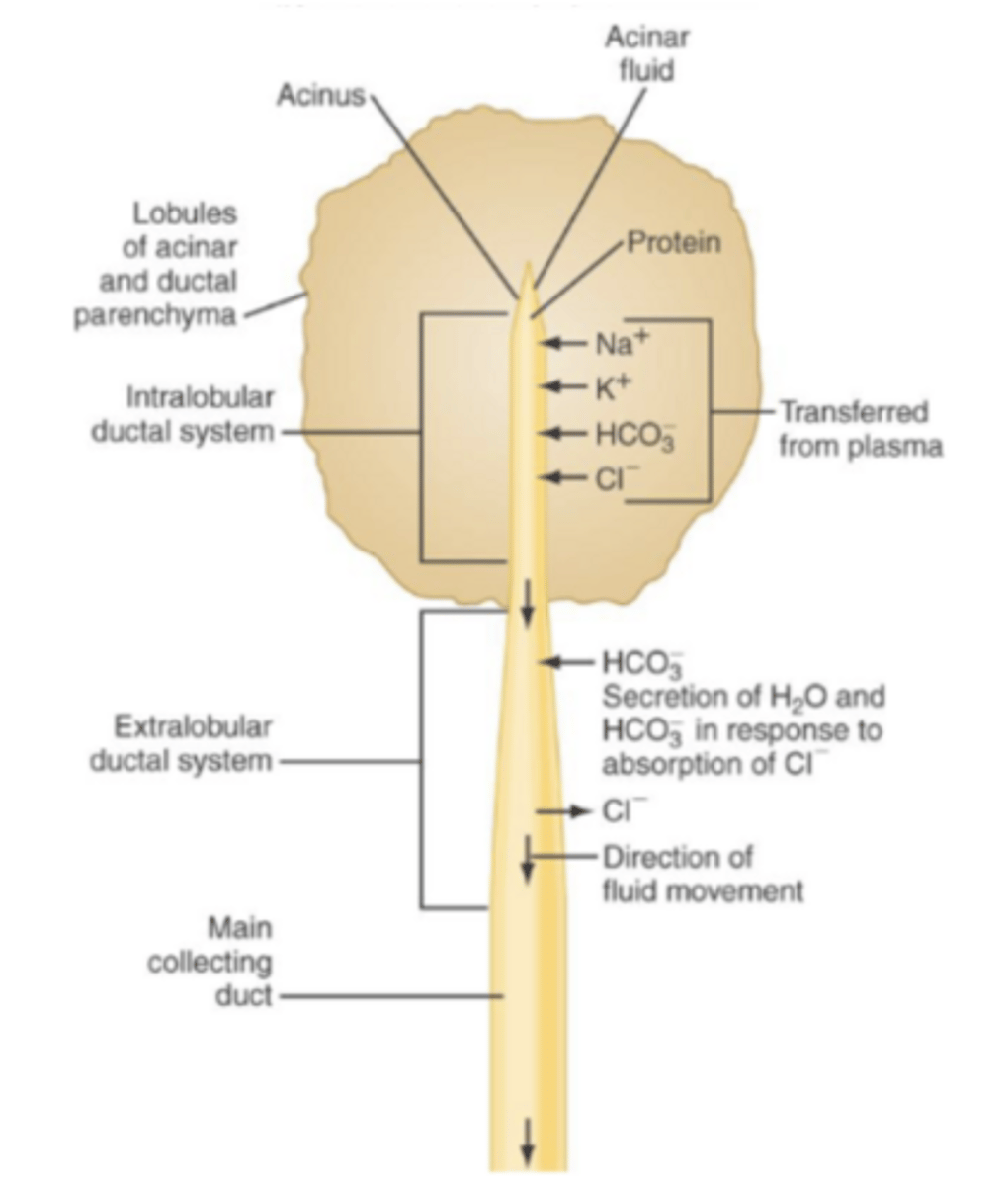
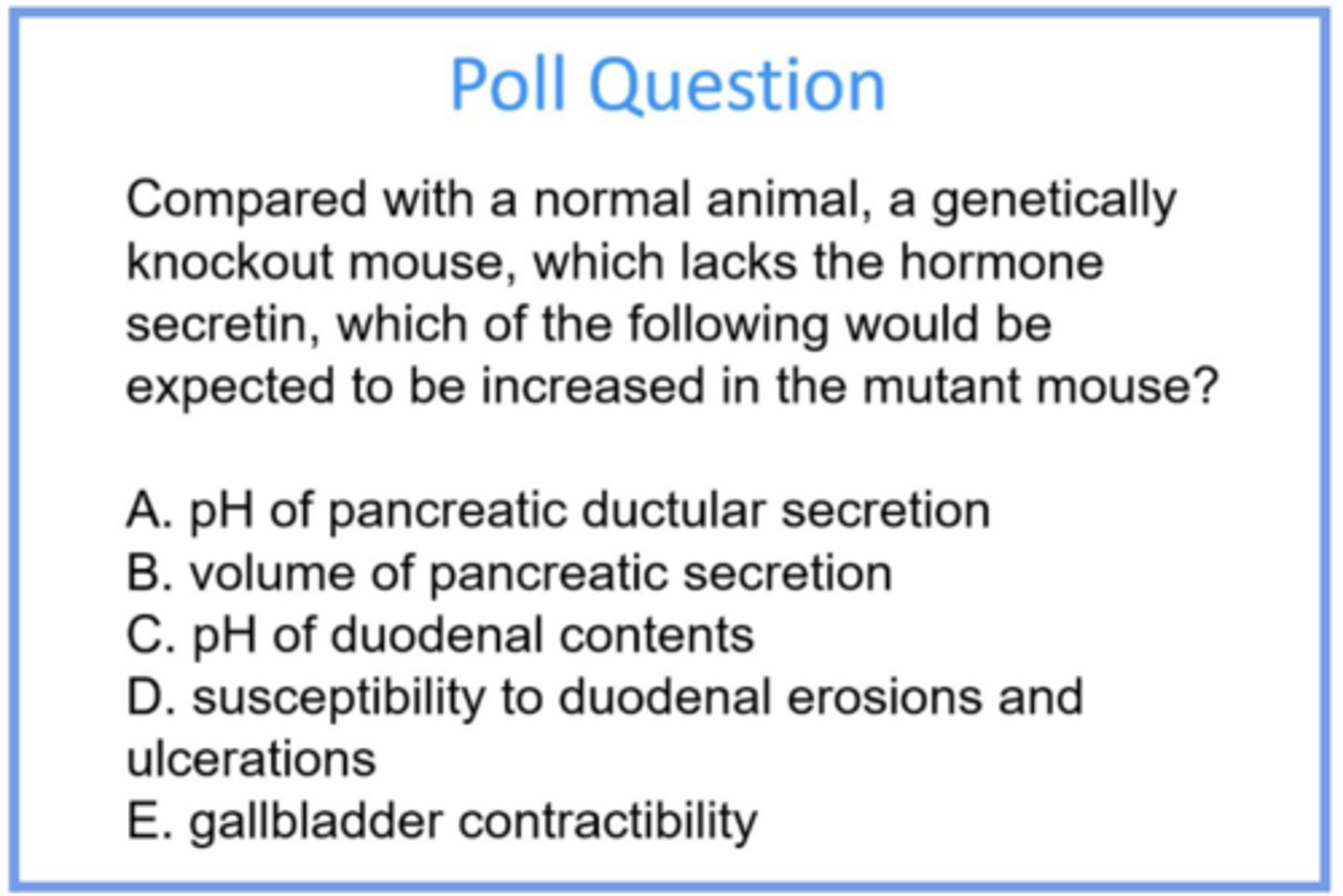
less bicarb (bc less secretin) = less pH buffering = more acidic (lower pH) in duct/ductal secretions and duodenum/duodenal contents
bicarb draws volume in; when you don’t have secretin volume doesn’t increase because bicarb secretion brings fluid (bile secretion can increase bc of biliary secretion of bicarb bc fluid is drawn in)
more acidic environment in SI = more erosions/ulcers
secretin is not involved in gallbladder contractility
answer the question and provide reasoning for all answer choices
in cystic duct, would cause no bile release from the gallbladder BUT there still would be a bile "drip" from the liver
in common bile duct, would cause no bile to be secreted and an enlarged gallbladder (bc its secretions are blocked)
in sphincter of oddi, would cause no bile OR pancreatic secretions into the GIT, which would cause self-digestion bc enzymes would bot back up into organs
what would a gallstone at each of the red circles cause?
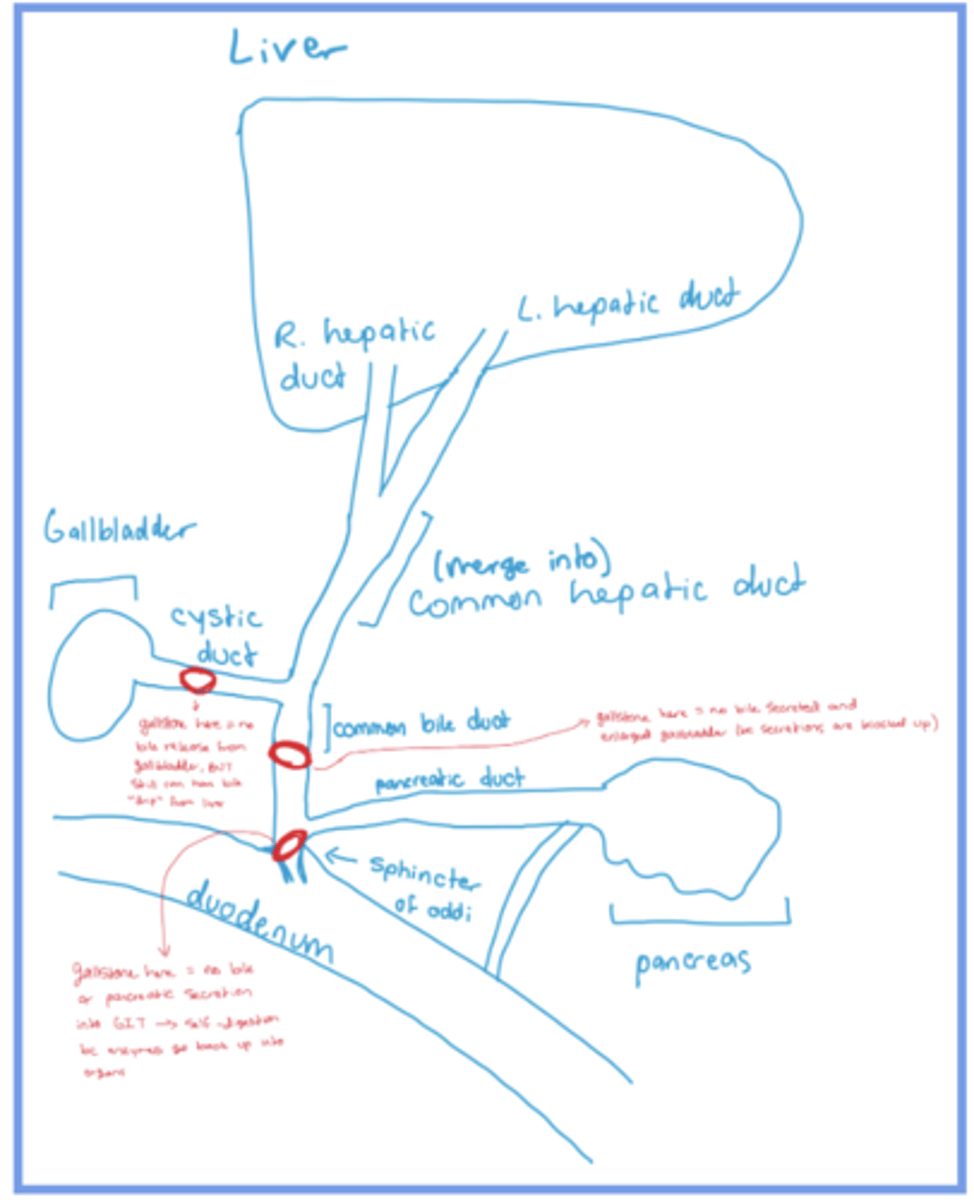
sphincter of oddi
where the secretions from pancreas and gallbladder (bile and pancreatic ducts) pass through to enter the SI