Neurologic Infections, Autoimmune Disorders, and Neuropathies
1/20
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
21 Terms
Infectious Neurologic Disorders
Meningitis
Brain abscesses
Various types of Encephalitis
Creutzfeldt–Jakob disease (CJD)
Variant Creutzfeldt–Jakob disease (vCJD)
Meningitis (what is it, Manifestations)
Inflammation of the meninges, which cover and protect the brain and spinal cord
Two main types classified as:
Septic caused by bacteria (Streptococcus pneumoniae, Neisseria meningitidis)
N. meningitidis is transmitted by secretions or aerosol contamination, and infection is most likely in dense community groups, such as college campuses and military bases
Aseptic caused by viral infection secondary to cancer or a weak immune system
Pathophysiology: Organism crosses BBB and proliferates in the CSF
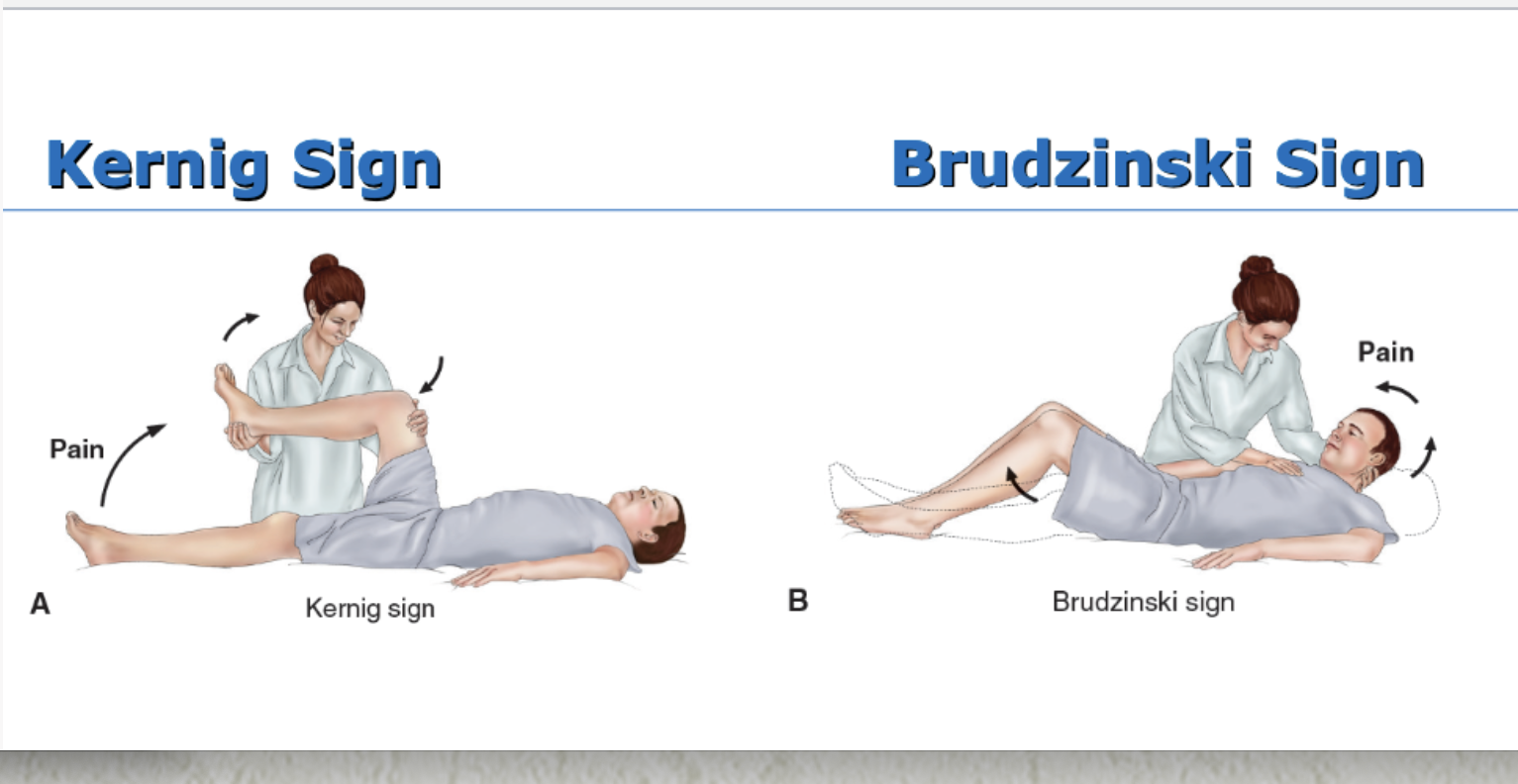
Manifestations of Meningitis: headache, fever, chills, nuchal rigidity (stiff and painful neck), positive Kernig sign, positive Brudzinski sign, and photophobia; rash (skin lesions ranging from petechial rash w purpuric lesions to large ecchymosis); changes in LOC, behavioral changes in older adults; seizures
Medical management of Meningitis
Prevention by meningococcal vaccine
Youth @ 11 to 12 years of age w a booster at 16
Early administration of high doses of appropriate IV antibiotics (Penicillin G w cephalosporins) for bacterial meningitis
If exposed, then treat w antimicrobial chemoprophylaxis (rifampin, ciprofloxacin, or ceftriaxone) within 24 hours after exposure
Dexamethasone (Decadron)
Treatment for dehydration, shock, and seizures
Nursing management of Meningitis
Frequent or continual assessment, including VS and LOC
Pain and fever management
Protect patient from injury related to seizure activity or altered LOC
Hyperthermia: worried about seizures
Monitor daily weight, serum electrolytes, urine volume, specific gravity, and osmolality
Prevent complications associated with immobility
Infection control precautions
Supportive care
Measures to facilitate coping of patient and family
Encephalitis
Acute, inflammatory process of the brain tissue
Causes: viral infections (herpes simplex virus [HSV] is most common in the US), vector-borne viral infections (West Nile, St. Louis), and fungal infections
Manifestations: headache, fever, confusion, hallucinations; vector borne-rash, flaccid paralysis, Parkinson-like movements
Medical management: Acyclovir for HSV infection, amphotericin or other antifungal agents for fungal infection
Nursing management: Frequent and ongoing neuro assessment; supportive care
Diagnostic tests: spinal tap (checking CSF), EEG (also used for seizure)
Multiple Sclerosis (MS)
A progressive immune-related demyelinating disease of the CNS
Destruction of myelin sheath (the fatty and protein material that surrounds certain nerve fibers in the brain and spinal cord)
Clinical manifestations: vary w different patterns
Relapsing and remitting: exacerbations and recurrences of symptoms, including fatigue, weakness, numbness, difficulty in coordination, loss of balance, pain, and visual disturbances
Medical management
Disease-modifying therapies; interferon β- 1a and interferon β-1b, glatiramer acetate, and IV methylprednisolone
targets immune system; flu like symptoms leukakine increased LFTs, h/a, deprssion & skin necrosis
Still need to be on steriod so would switch to PO predison (rather then IV) → tapered started slow → supress immune,, supresses adrenal, mood swings, weight gain, electrolyte imblalence etc.
Symptom management of muscle spasms, fatigue, ataxia, bowel and bladder control
How is patient with Multiple Sclerosis assessed
Neurologic deficits
Secondary complications
Impact of disease on physical, social, and emotional
function and on lifestyle
Patient and family coping
What are the Nursing interventions of patient with Multiple Sclerosis?
Use a collaborative approach
Coordinate and refer as needed to health care services: social services, speech therapy, physical therapy, counseling services, home care services, and so on
Activity and rest
Program of activity and daily exercise
Relaxation, coordination exercises, walking, muscle- stretching exercises
Avoid very strenuous activity and extreme fatigue
Bowel and bladder control
Instruction or administration of prescribed medications
Voiding schedule
Bowel training program
Adequate fluid and fiber to prevent constipation
Reinforce and encourage swallowing instructions
Strategies to reduce risk of aspiration
Memory aides, structured environment, and daily routine to enhance cognitive function
Interventions to minimize stress
Maintenance of temperate environment—air conditioning to avoid excessive heat and avoidance of exposure to extreme cold
Use assistive devices and modifications for home care management and independence in ADLs
Support of coping
Myasthenia Gravis
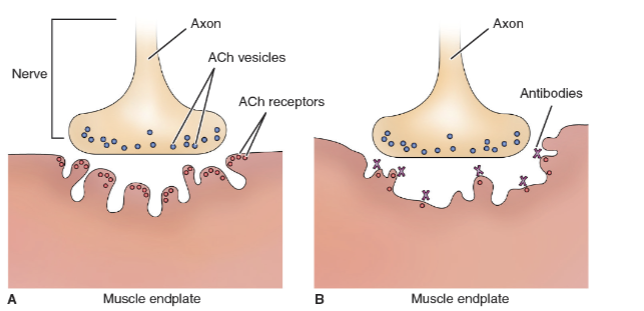
Autoimmune disorder where antibodies directed at acetylcholine receptor sites impair transmission of impulses at the myoneural junction
Characterized by varying degrees of weakness of voluntary muscles (purely motor disorder) → Blocks messaging
Manifestations: variable; ocular (diplopia and ptosis); generalized (weakness of facial muscles, swallowing and voice impairment (dysphonia), generalized weakness)
Medical management of Myasthenia Gravis
Directed at improving function and reducing and removing circulating antibodies
Pharmacologic therapy
Anticholinesterase medications and immunosuppressive therapy
Intravenous immune globulin (IVIG) → S/E; h/a, migraine, & flu like symptoms
Therapeutic plasma exchange - plasmapheresis
Thymectomy (removal of the thymus gland)
No cure for myasthenia gravis
Differenciate between Myasthenic Crisis & Cholinergic Crisis
Get O2 stat, respiratory support → avoid sedatives and tranquilizers to prevent resp. issues
Myasthenic Crisis
Result of disease exacerbation or precipitating event, most commonly a respiratory infection
Severe generalized muscle weakness with respiratory and bulbar weakness
Patient may develop respiratory compromise/failure
Cholinergic Crisis
Caused by overmedication with cholinesterase inhibitors
Severe muscle weakness with respiratory and bulbar weakness
Patient may develop respiratory compromise and failure
Guillain- Barre Syndrome
Autoimmune disorder with acute attack of peripheral nerve myelin
Rapid segmental demyelination of peripheral nerves producing ascending weakness w dyskinesia (inability to execute voluntary movements), hyporeflexia, and paresthesia (pins and needles sensation) → symptoms from feet up
Rapid demyelination may produce respiratory failure and autonomic nervous system dysfunction with CV instability
Most often follows a viral infection
Manifestations: variable; weakness, paralysis, paresthesia, pain, and diminished or absent reflexes,; bulbar weakness; cranial nerve symptoms; tachycardia; bradycardia; hypertension; or hypotension
Medical Management of Guillain- Barre Syndrome
A medical emergency b/c of rapid progression
Requires intensive care management with continuous monitoring and respiratory support
Therapeutic plasma exchange and IVIG are used to reduce circulating antibodies
Recovery rates vary, but most patients recover completely
How is patient with Guillain- Barre Syndrome assessed?
Ongoing assessment with emphasis on early detection of life-threatening complications of respiratory failure, cardiac dysrhythmias, and deep vein thrombosis (DVT)
Monitor for changes in vital capacity and negative inspiratory force
Assess VS frequently or continuously, including continuous monitoring of ECG
Patient and family coping
What are the nursing interventions for patient with Guillain- Barre Syndrome assessed?
Enhancing physical mobility and prevention of DVT
Support limbs in functional position
Passive ROM at least twice daily
Frequent position changes at least every 2 hours
Elastic compression hose or sequential compression boots
Adequate hydration
Administer IV and parenteral nutrition as prescribed
Carefully assess swallowing and gag reflex and take measures to prevent aspiration
Develop a plan for communication individualized to patient needs
Decreasing fear and anxiety
Provide information and support
Referral to support group
Relaxation measures
Maintain positive attitude and atmosphere to promote a sense of well-being
Diversional activities
Cranial nerve disorders (diagram)
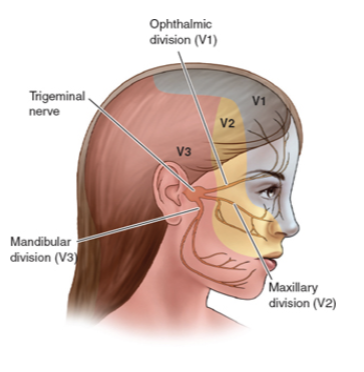
Trigeminal Neuralgia (Tic Douloureux)
Condition of the fifth cranial nerve characterized by paroxysms of pain → extreme
Most commonly occurs in the second and third branches of this nerve
Vascular compression and pressure is the probable cause
Occurs more often in the fifth and sixth decades and in women and persons with MS
Pain can occur with any stimulation such as washing face, brushing teeth, eating, or a draft of air
Patients may avoid eating, neglect hygiene, and even isolate themselves to prevent attacks
Medical management of Trigeminal Neuralgia
Anticonvulsant agents (carbamazepine-tegratol) for pain- (4-12)
Take with food, watch serum levels for toxicity, nausea, dizziness, drowsiness, aplastic anemia
SJS- Steven johnsons syndrome: severe skin and mucous membrane reactions, typically triggered by medications or infections. It begins with flu-like symptoms followed by a painful red/purple rash that blisters and causes the skin to peel, affecting less than 10% of the body surface area. → use suncreen, more used as anticonvulsent rather then mood stabilizer
Hepatotoxic & teratogenic
Check serium sodium, LFT, CBC (serious blood disorders)
What are the nursing considerations: avoid grapefruit juice, affect birth control, report signs of infection (agranulocytosis), use sunscreen
Gabapentin and antispasmodic (baclofen) → good for nerve pain
Phenytoin as adjunctive therapy
Surgical treatment
Microvascular decompression of the trigeminal nerve
Radiofrequency thermal coagulation
Percutaneous balloon microcompression
What are the nursing interventions for Trigeminal Neuralgia?
Patient education related to pain prevention and treatment regimen
Measures to reduce and prevent pain; avoidance of triggers
Care of the patient experiencing chronic pain
Measures to maintain hygiene: washing face, oral care
Strategies to ensure nutrition; soft food, chew on unaffected side, avoid hot and cold food
Recognize and provide interventions to address anxiety, depression, and insomnia
Bell’s Palsy
Facial paralysis caused by unilateral inflammation of the seventh cranial nerve
Manifestations: unilateral facial muscle weakness or paralysis with facial distortion, increased lacrimation, and painful sensations in the face; may have difficulty with speech and eating
Most patients recover completely in 3 to 5 weeks, and the disorder rarely recurs
How is Bell’s Palsy management?
Medical
Corticosteroid therapy may be used to reduce inflammation and edema
Nursing
Provide and reinforce information and reassurance that stroke has not occurred
Protection of the eye from injury; cover eye with shield at night, instruct patient to close eyelid, use of eye ointment and sunglasses
Facial exercises and massage to maintain muscle tone