Oropharyngeal and Nasopharyngeal Cancers
1/66
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
67 Terms
oropharyngeal cancers are fast increasing due to rise of _____________
HPV
Most HPV+ occur where in oropharyngeal cancers?
BOT/tonsillar (likes to hide in reticulations)
oropharyngeal cancers are 85-95% ________
squamous cell carcinoma
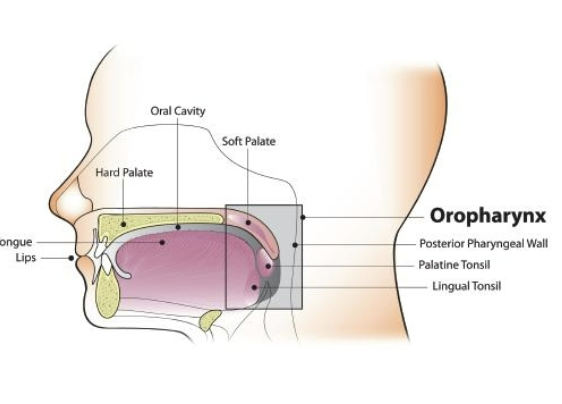
Oropharyngeal cancer sites:
Soft palate
Lateral and posterior pharyngeal walls
Tonsils (lingual/palatine)
Posterior 1/3 of tongue (BOT)
how many levels of of lymph nodes are there?
5 levels
Oropharynx cancer nodal spread
Subdigastric Level 2a
Neck Involvement
lateral lesions
midline lesions
lateral lesions= unilateral
midline lesions= bilateral
Single predictive factor for metastatic spread is what?
neck node involvement
Distant metastases of oropharyngeal cancers are associated with:
Bilateral neck nodes
Nodes in lower neck
Large neck nodes
Extranodal spread
3 most common sites of metastases for oropharyngeal AND nasopharyngeal cancers
Lungs
Liver
Bones
Diagnosis/Staging of Oropharyngeal AND Nasopharyngeal Cancer
Clinical exam by ENT
Histological evaluation of biopsy
TNM stage after physical exam, MRI, CT, and pathology
Neck staging
where is biopsy typically performed for oropharyngeal cancer and with what? how is this different that nasopharyngeal cancer?
Typically performed in clinic with local anesthetic due to easy access to oral cavity
nasopharyngeal is not easy access so no local anesthesia, but still done in clinic
TNM stage after what? what are the 2 types?
for both oropharyngeal and nasopharyngeal
physical exam, MRI, CT, and pathology
cTNM = clinical stage
pTNM = pathologic stage
Neck staging for oropharyngeal cancer
Palpation of the neck combined with CT or MRI
Ultrasound and FNA (clinical standard)
What is the most common type of oropharyngeal cancer?
squamous cell carncinoma
Midline lesions are more likely to result in which type of nodal spread?
bilateral
Signs Specific to Oropharynx Cancer
Sore throat that does not go away
Trouble swallowing
Trismus
Reduced lingual ROM
Unexplained weight loss
Ear pain
lump in the throat (globus sensation)
White patching (leukoplakia)
Coughing up blood
Oropharyngeal AND nasopharyngeal cancer Staging
Tumor size: T0-T4 greater size/depth of invasion
Node involvement; N0-N3 ipsilateral/bilateral and size of node
Metastasis: M0/M1 present or absent
Curative Treatment for Oropharyngeal Cancer
easily accessed/small= eligible for surgery or RT
larger the tumor the larger the surgery for resection + CRT
Oropharyngeal RT Side Effects include what 2 types of effects?
acute toxicities
late toxicities
Acute toxicities of RT effects for the oropharynx
Mucositis
Necrosis
Xerostomia
late toxicities of RT effects of the oropharynx
Xerostomia
Dental decay
Osteoradionecrosis (necrosis of the bone)
Most common approach in oropharyngeal cancers
CRT
radiosensitizer: chemo makes tumor more sensitive to RT
gold standard chemo treatments in oropharyngeal cancer
platinum-based chemo (cisplatinum & carboplatinum)
CRT for Oropharyngeal Cancer per previously discussed protocols (fractionations)
Chemo: 3 infusions every 3 weeks
RT: 7 weeks of 5 days per week RT x 35 fractions
CRT for Oropharyngeal Cancer may be recommended after surgery if:
+ Surgical margins
+ Multiple lymph nodes
Extranodal spread (through LN and into adjacent tissue)
Neck Dissection is the removal of what?
diseased lymph nodes and those assumed to have disease or in disease area
classification of neck dissection
radical, modified radical, and selective
clearance of all neck levels, SCM, and/or IJV and/or nIX spared
modified radical
clearance of all neck levels, SCM, IJV, and nIX all spared
selective
clearance of all neck levels, SCM, IJV, and nIX sacrificed
radical
What are 2 symptoms of oropharyngeal cancer?
trismus, ear pain
Name 1 surgical treatment option for oropharyngeal cancer.
composite resection- mandible split open, invasive
What is the most common approach to treating oropharyngeal cancers?
CRT
SLP Role in Oropharyngeal Cancer
Early evaluation, education, counseling
Swallow intervention pre-HNC tx if baseline dysphagia
Swallow intervention post-op or during C/RT
Post-tx swallow therapy
swallow intervention deals more with what swallow components in oropharyngeal cancer?
pharyngeal clearance & reduced efficiency
can still affect oral prep/transit
Post-tx swallow therapy in Oropharyngeal Cancer
Exercise based therapy
Manual therapy
Diet advancement
Manual therapy in Oropharyngeal Cancer
Scar management
Manual manipulation and lymphatic drainage
Myofascial release of neck/jaw/face
oropharyngeal etiology
HPV, Alcohol and tobacco
oropharyngeal AND nasophayrngeal lymph nodes
Level 2A
oropharyngeal AND nasophayrngeal risk of metastasis (node involvement)
Bilateral neck nodes, Nodes in lower neck, Large neck nodes, Extranodal spread
oropharyngeal AND nasophayrngeal metastasis areas
Lungs, liver, bone
oropharyngeal AND nasopharyngeal evaluation
Exam by ENT, biopsy, MRI/CT, PET-CT
oropharyngeal treatment
CRT
Small (<2cm) easily accessible tumors may be removed surgically (less common)
Neck dissection
Large surgeries require reconstruction with flap from where?
from arm or leg
FLAPS DON’T FUNCTION
oropharyngeal additional rehab
May need dentures post-CRT if many extractions
NPC often associated (75%) with _________
Epstein-Barr virus (mono)
Types of NPC
Keratinizing ScCa
Nonkeratinizing ScCa (EBV related)
Undifferentiated nonkeratinizing ScCa (EBV related)
NPC population tends to be:
younger; higher likelihood in men
NPC has a higher incidence where?
China, Indonesia
Incidence = 5-6 per 100,000 people
what type of incidence of NPS in US?
Sporadic cases in the US
Incidence = .5 per 100,00 people (lower)
Signs Specific to Nasopharyngeal Cancer
Neck swelling
Neck mass (75% @ dx)
Nasal blockage in advanced cases
Bleeding from nose or throat
Eustachian tube dysfunction causing aural symptoms
Headache
Cranial nerve palsy
What is the most common virus associated with nasopharyngeal carcinoma?
Epstein-Barr virus
Who is at higher risk for NPC?
males and younger people
What are two signs/symptoms specific to pts with NPC?
headaches, hearing loss
sites of nasopharyngeal cancers
Fossa of Rosenmuller
Lateral/Posterior pharyngeal walls
NPC may extend to what structures?
Skull base
Parapharyngeal space
is lymph node involvement common in nasopharyrngeal cancer?
yes, very common
Bulky, bilateral nodal involvement
biopsy of Nasopharyngeal Cancer is typically performed where?
in clinic
neck staging of nasopharyngeal cancer
Palpation of the neck combined with CT or MRI
Ultrasound and FNA (clinical standard)
60-70% present at stage 3 or 4
PET to evaluate for distant spread
Treatment for Nasopharyngeal Cancer
C/RT is primary modality
Surgery in selected cases
OMFS collaboration often necessary for functionality given limitations of surgical reconstruction
what is the field of C/RT like for nasopharyngeal cancer?
Radiation field very large; primary site + bilateral neck
What percentage of NPC pts present at stage 3 or 4?
60-70%
What is the primary treatment modality for NPC?
C/RT
nasopharyngeal structures
Mucosa of roof of nasopharynx, Fossa of Rosenmuller, Skill base, Parapharyngeal space
nasopharyngeal etiology
EBV, Alcohol and tobacco
nasopharyngeal additional rehab
Work with OMFS for creation of obturators, dentures, lifts, etc.