FINAL CHRONIC
1/67
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
68 Terms
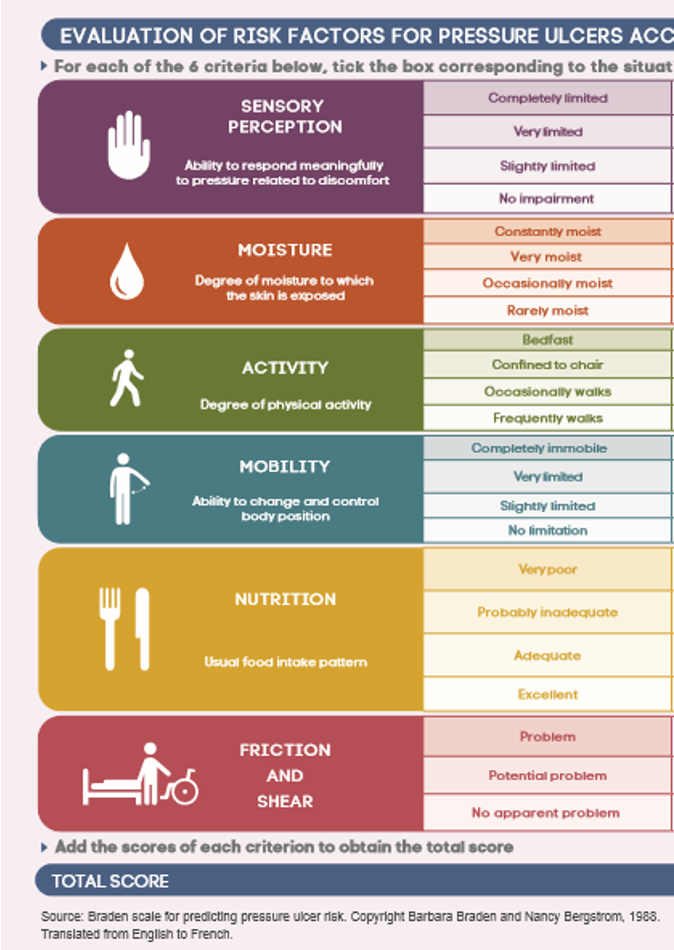
Braden scale
Assess risk for pressure injury:
sensory perception
moisture (ex. due to incontinence)
activity/mobility
nutrition
friction/shear
Score: 6-23
<18 → at risk MUST implement preventative measures
Psoriasis
Immune disorder causing chronic inflamm of skin
skin cell produc. > shedding → epidermal thickness
Signs: occur anywhere → elbows, knees, palms, soles, scalp
thick, raised red patches w/ silvery flaking scales
painful & itchy
Lab: based on signs
elevated CRP & ESR (serum inflamm markers)
Tx: no cure
topicals/ointments (corticosteroid, retinoids), uv light therapy (kills cells), methotrexate
Care:
pt are better in warmer climate → uv kills cells

Skin cancer
Cause: uv radiation
Types:
(#1) basal cell carcinoma → usually tx b/c localized
melanoma → harder to tx
Labs: changes in skin (size, color, sensation)
Tx: chemo, radiation
Care:
limit sun exposure (spf 30, hats/long sleeve)
monthly self exams
Burn injuries types
1) Superficial (sunburn)
affect only epidermal
signs: mild erythema/hypersensitivity
tx: resolves in 24-72 hrs (no meds necess.)
2) superficial partial thickness
affect epidermis & superficial
signs: very painful b/c exposed nerve endings, wet weeping pink blisters, cap refill normal
tx: heals in 1-2 wks
3) deep partial thickness
affect epidermis & extend into deeper portions
signs: appear waxy (no weepy blister), pink/cherry red, vary pain, NO cap refill
4) full thickness
affect epidermis, dermis, subcut tissue, maybe muscle/bone
destroy hair follicles, sweat gland, nerve ending → poor temp control & no pain
tx: skin graft
Burn injuries
Risk: pt age & medical hx
Effects: burn shock & fluid/electrolyte imbalance secondary to massive fluid shifts
fluids/electro leak out of intravascular space into interstitial b/c increased cap perm.
initial: hyerK
late: hypoK & hypoN
Burn injury stages
1) emergent
goal: resolve immediate life threat → baseline eval, airway, fluids, prevent hypothermia, initiate wound care
care: 100% humidified o2, place large bore iv cath (fluid resus), warming measures (ex. blanket)
2) immediate (after resus & stabilize 48-72hr later)
goal: wound healing & closure, optimal nut., prevent infection & pain
care: assess labs (protein, wbc, albumin), wound care, nut. (maybe feeding tube)
3) rehab (may last for years)
goal: rehab & pyschological support
care: community resources, teach pt how to apply pressure garment (prevents hypertrophic scarring)
pt w/ burn may lack sweat gland & skin graft is sensitive to light
increased metabolic rate & caloric need post burn
HIV
Virus that attacks body’s immune system
targets CD4+ lymphocytes → integrate rna into host cell dna through reverse transcriptase
Cause: STI (#1), blood, breast milk
fluid MUST come in contact w/ mucous membrane/injected into bloodstream
Lab: annual screening
viral load & cd4 count to establish baseline
Tx: no cure → proper managment
antiretroviral therapy (ART)
w/o proper tx → AIDS develops
Care:
avoid food that irritate bowel (raw fruit/veg, carbonated)
may need enteral/parenteral nut.
avoid high risk (use condom, reduce partners, no share needles)
hygiene → hand wash, avoid crowds
Stages of HIV
Stage 1: acute
develop 2-4 post exposure → very contagious
hiv rapidly spread → increase viral load → body can still control the virus → CD4 return to normal levels (500 cells/mm3)
signs: temporary flu like symp (fever, chills)
Stage 2: chronic
prolonged → last several decades w/ tx or a decade w/o
low CD4 → 200-499
sign: asymp but STILL contagious
nonspecific sign → resp. tract infection, enlarged lymph
Stage 3: aids
CD4: <200 = aids
HIV tx
Antiretroviral therapy (ART)
interfere w/ ability of hiv to reproduc. & suppress virus
use: confirmed case, pre/post exposure prophylaxis
uses multiple agents & adherence is required
atleast 95% adherence for tx to be effective
eval renal & hepatic
Pneumonia
Inflamm of lung parenchyma from infection
Signs: pleuritic chest pain, cough, fever
Lab: chest x-ray
elevated wbc, crp, positive sputum
starts as resp. alka → later: resp. acid
Tx:
bronchodilator: albuterol or combivent → open airway
antibiotic → broad then specific
Care:
SaO2 >92%
position: good lung down, hob 30
TB
Resp. infection caused by mycobacterium tuberculosis
spread via aerosolized droplet (NOT direct contact) → airborne precaut.
Types:
latent → asymp. & NOT contagious
active → abnormal chest x-ray/sputum
Signs: hemoptysis (coughing blood), weight loss, night sweat
Lab: tuberculin skin test (mantoux test) → assess induration (size/firm)
Tx: 3-9 months
2 phases: intensive → continuation
Asthma
Intermittent, reversible airway obstruction from inflamm → increase mucus, bronchospasm
Signs: wheezing, dyspnea, coughing, increased sputum/RR, tachy
Lab: spirometry, chest x-ray, abg
Tx: anti-inflamm (inhaled corticosteroid), bronchodilator
Care:
maintain o2 >90%
teach action plan, pursed lip, peak flow meter
Laryngeal cancer
Originate from squamous cells that line larynx/hypopharynx/ esophagus entry → slow develop
Risk: (#1) tabacco & alcohol
Signs: change in voice (lower, raspy, >2 wks), persistent sore throat, ear pain
Lab: laryngoscopy, barium swallow
Tx: radiation, chemo, surgery
Care: post op
trach care/suction, pulmonary hygiene (deep breath), nut., emergency equip at bedside
Hypertension
BP that is above normal “silent killer”
Types:
primary (#1) → multifactorial, chronic
secondary → caused by underlying, acute
Signs: increase bp
late → headache, chest pain, sob, vision change
Lab: >2 bp reading at SEPARATE times
Tx: slowly & cautious
start w/ 1-2 med (LOW doses) → diuretic, beta block, ½ dose for older
HTN complications
Hypertensive crisis
hypertensive urgency → bp very high but no sign of organ damage
hypertensive emergency → bp >180/120 + possible damage
Coronary artery disease (CAD)
Obstruct/dysfunc of blood vessels that deliver o2 rich blood to heart muscles → ↓ perfusion of myocardial tissue
Cause: atherosclerosis (harden/narrow of arteries b/c plaque)
Risk: elevated serum lipids
cholesterol >200, trig. >150
Sign: asymp until 40% block → angina
Lab: lipid profile
Tx: surgery (ex. stent)
aspirin (stop aggregate)
nitroglyercin (relief) → every 5 min x3
Care: bleeding precaut.
diet: decrease saturated fat (meat, whole milk), increase complex carb (whole grain)
Peripheral artery disease (PAD)
Narrow/block of vessels that carry blood from heart to upper/lower extremities → deprive o2 → ischemia, necrosis
Cause: atherosclerosis
Signs: intermittent claudication (#1) → muscle pain b/c lactic acid buildup, foot pain worse w/ elevation, coolness, thin shiny skin
Lab: vascular assessment (palp, auscul, inspect), ABI
Tx: meds, angioplasty
Complications: nonhealing ulcers + gangrene → may need amputation
Venous thrombus
Blood clot in vein → potential to break off (thromboembolism)
Signs: Virchow’s triad
stasis, endothelial injury, hyercoag.
Sign: swell, tender, redness, warmth
Lab: duplex ultrasound (confirm), D-dimer (+ test)
Tx: heparin or enoxa. (for active clot only) → transition to long term oral anticoag (warfarin (INR 2-3))
Care: watch out for bleed (bruise, petechiae, hematuria)
Venous insufficiency
Occurs when leg veins do not allow blood flow back to heart → blood flow backward & pools in leg
Sign: “heavy pain”, skin change (brown), varicose vein, venous stasis ulcer (ankles/calves)
twisted, enlarged vein
Tx: surgery
sclerotherapy, vein ligation & stripping
HF
Progressive disease characterized by myocardial cell dyfunc. & muscle weakening
Sign: fatigue, weight gain, tachy
left side: sob, crackles, fatigue, cool/weak
right: JVD, hepatomegaly, ascites, edema
Types:
HFrEF → inability to pump forward “weak pump”
EF <45%
HFpEF → unable to relax & fill “stiff, improper fill”
EF >45% but low CO
Lab: ecg
troponin, BNP/NT-proBNP (released in response to high bp/fluid)
Tx: diuretic, ACE inhibitor (#1), beta block
Cancer
Uncontrolled growth of malignant cells that compromise normal cells
Risk: exposure to carcinogen → cellular mutation
Types:
solid tumor → arise from specific organ (ex. lung)
hematological → from cells (ex. leukemia)
Staging: TNM (tumor size, spread to lymph, metastasis)
Sign: CAUTION
Lab: biopsy
Tx: radiation, chemo, bone marrow transplant
End of life
Pt goals guide treatment
Signs: dyspnea, anorexia, delirium, depression
late → gurgling, terminal bubbling
Care:
suctioning, position (lateral w/ elevated head), antimuscinaric/anticholinergic to dry up secretions
Anemia
Reduction in o2 carrying capacity b/c less rbc or reduction in hemoglobin
Causes: blood loss, inadequate rbc produc, increased rbc destruct., deficiency
Types:
iron defic. (#1) → insuff. hemoglobin to carry o2
sign: hypoxia, pallor, fatigue
lab: low serum ferritin, low H&H
tx: red meat, dark leafy, dried beans, fortified cereal/bread (take w/ vit C)
vit b12 → need for func. of CNS, formation of rbc, dna reg.
sign: cns changes → spinal cord degen, altered mental
lab: b12 assay
tx: animal protein → meat, seafood, egg, dairy
folic acid → need for formation of heme for rbc mature
sign: pallor, tachy, dizzy
lab: cbc
tx: fortification of cereal/grains → supplements for preg.
sickle cell → cause hemoglobin to be sticky → block blood flow → hypoxic
sign: vassooclusion → pain swell
tx: o2 therapy, avoid cold
Polycythemia vera
Disorder of bone marrow → makes blood more viscous (thick) → slow circulation & o2 exchange
increase in volume of rbc BUT still hypoxic
Cause: JAK2 gene
Sign: takes years for symp → sob, headache, risk for clot
Lab: routine blood test
Tx: therapeutic phlebotomy (remove blood)
Care:
hydration (3L/day), elevate legs
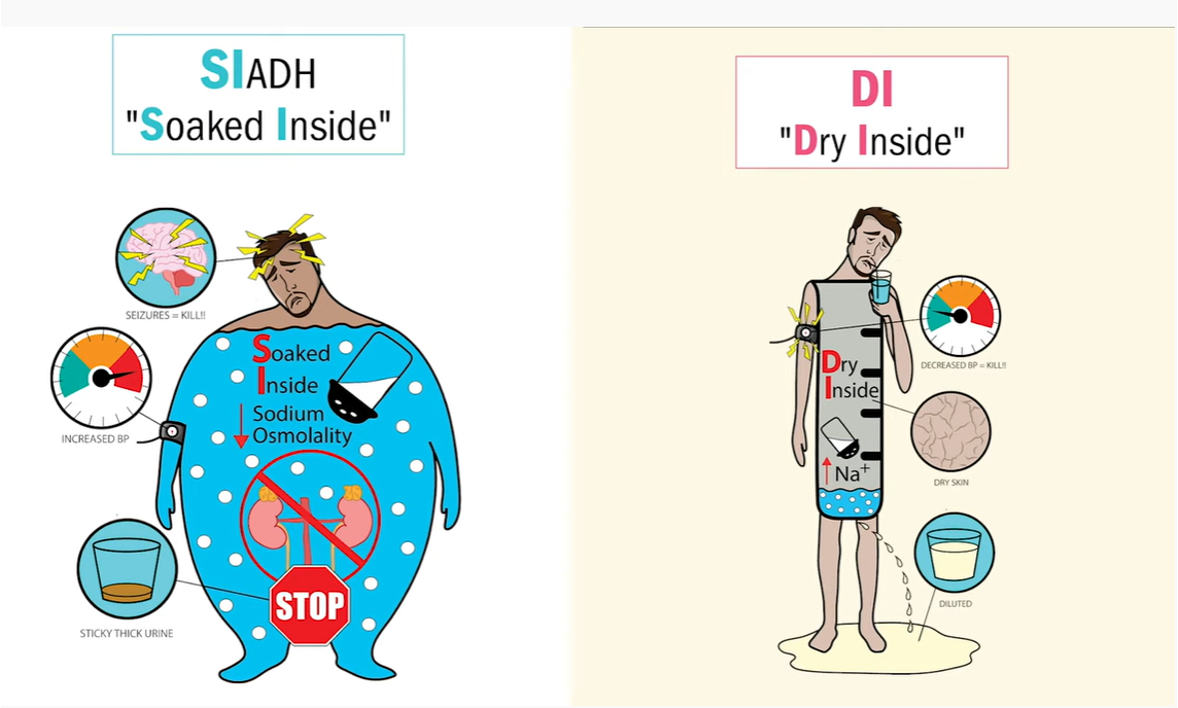
Diabetes Insipidus (DI)
Deficiency of ADH (helps regulate h2o)
reduce ability of kidney to collect/concentrate urine → excessive dilute urine → “DRY INSIDE”
Signs:
polyuria, polydipsia, hemoconcentration (elevated serum sodium & hematocrit), skin tenting, dry mucous mem., weak pulse
Med:
desmopressin or vassopressin
cause water reabsorption in kidneys
DI Management
Diagnostic:
low →urine electrolytes, urine osmo. (<200), USG (<1.005)
high → serum
when serum osmo increases but no increase in urine osmo
Care:
maintain adequate fluid status PO or IV
at risk for circulatory collapse
mouth care → for dry mucous membranes
watch for dehydration, hypovolemia, hypernatremia
SIADH
Excessive release of ADH
renal reabsorption of water → water intoxic. → cellular edema → dilutional hyponatremia “SOAKED INSIDE”
Signs: volume overload + hyponatremia
weight gain, tachy, crackles, distended neck vein, headache, personality change, hostility
SIADH Management + Tx
Diagnostic:
low → serum
high → urine electro., urine osmo, USG
Care:
PO fluid restriction & increased salt intake
comfort measure for thirst → ice chips
Tx:
diuretics, hypertonic sodium chloride IV
SLOW correction of hyponatremia (risk brain damage)
SIADH vs DI
Hypothyroidism
↓ function of thyroid → ↓ metabolism
associated w/ iodine deficiency (needed for thyroid synth.)
Signs:
↓ energy, fatigue, increased sleep, weight gain, susceptible to cold temp, dry skin, thin hair, ↓CO
Diagnostic: Low T3 & T4, high TSH
Tx: levothyroxine
taken FIRST thing in morning (1hr b/f meal or 3 hr after)
start at low dose and increase gradual → lifelong
side effects: weight loss, nervous, tremor, insomnia
Myxedema coma (hypothyroidsm complication)
Emergency → hypoxia and co2 retention, fluid/electro. imbalance, hypothermia
Signs:
increased sensitivity to sedatives, analgesics, anesthetic
↓ CO → bradycardia, hypotension
Tx:
IV thyroid hormone
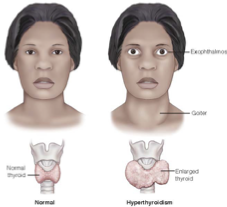
Hyperthyroidism
Accelerated metabolism and overstim. of SNS
usually caused by Grave’s
Signs: everything is increased
elevated HR, heat intolerance, gastric activity (BM/D), increased app, weight loss, exophthalmos & goiter
Diagnostic: high T3 & T4, low TSH
Hyperthyroidism Tx
Meds:
long term → antithyroid
short term → iodine prep. (decrease blood flow through thyroid)
beta block (slow HR, decrease palpitations)
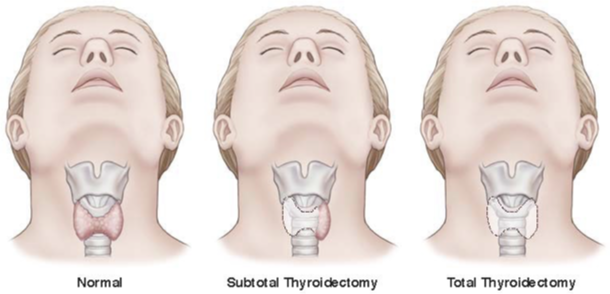
Surgery: thyroidectomy
for pt w/ hypersecreting tumor or tracheal compress. unresponsive to med
establish “normal” thyroid function before surgery
complications:
removal of all parathyroid tissue → hypoparathyroidism
laryngeal nerve damage → affect swallow/voice
Thyroid storm/thyrotoxicosis (hyperthyroidism complication)
Signs:
tachycardia, fever, systolic hypertension, abd pain, tremors, change in LOC
Care:
Airway + fluid resuscitation
cooling blankets
meds: glucocorticoids
↓ conversion of T4 to more active T3
↓ release of TSH
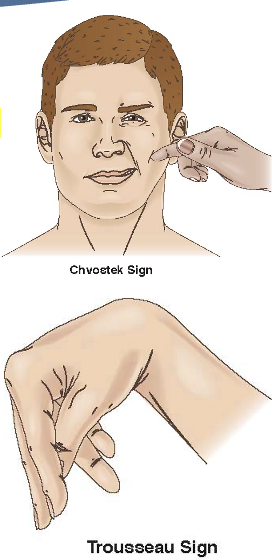
Hypoparathyroidism
Lack of parathyroid hormone → calcium not mobilized from bones/conserved in kidney/absorb in small intest. → hypocalcemia
Cause: (#1) removal of parathyroid
Signs: ↓ Ca (Ca plays major role in membrane potential, neuronal excit., muscle contract.)
numbness/tingling around mouth/hand/ft, tetany (severe muscle spasm → can cause laryngospasm & airway compromise), skeletal deformity, positive Chvostek sign & Trosseau
Diagnostic:
low serum calcium, serum PTH
high serum phosphate
Hypoparathyroidism Management + Tx
Meds: focus on raising serum calcium
Acute: IV calcium → followed w/ oral calcium + vit D (enhance absorp.)
Chronic: oral calcium + vit D
Care:
adhere to med → lifelong Ca supplementation
eat foods high in calcium BUT low in phosphorus (can bind to Ca → ↓ lvls more)
eat: dairy, milk, cheese, OJ, yogurt
avoid: beans, lentils, nuts
Hyperparathyroidism
Hypersecretion of parathyroid hormone → hypercalcemia → leads to bone breakdown & increased renal/bowel reabsorp of Ca
Signs:
kidney stones, polyuria, abd pain, muscle weakness
cardiac change → prolonged PR, short QT, vent. dsyrhythmis
Diagnostic:
↑ serum/ionized Ca, serum PTH
↓ serum phosphorus
Tx:
furosemide → increase renal excretion of Ca
avoid thiazide diuretic (increase reabsorp)
Care:
prevent bone injury (use lift sheets)
if unresponsive to med → subtotal parathyroidectomy
increase fluid to minimize renal injury
decrease consump. of calcium containign antacid + vit D
Addison’s disease
Destruction of adrenal glands → low hormones (cortisol + aldosterone)
mostly females
Signs: asymp until 90% of adrenal cortex destroyed
hypoglycemia, weight loss, depression, darken bronze hyperpigment., hyponatremia (salt craving), water loss, hyerK,
Diagnostic: test hypothalamic pituitary axis & adrenal cortex, serum electro
Care:
replacement of cortisol, fix electrolyte imbalance, maintain fluids
take hormone replace daily
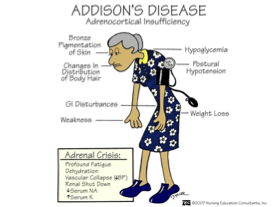
Adrenal crisis (addison’s comp.)
Severe hypovolemia & hypotension
Cause: pt who have underlying adrenal hypofunction who undergo stressful event
Na & fluid loss, hyperK, hypogycemia
Cushing’s disease
Excessive circulating glucocorticoid (cortisol) or ACTH → excess hormones
Signs:
hyperglycemia, thin/friable skin, moon face, male sexual characteristic develop in female (breast atrophy, voice deepen)
Diagnostic: assess cortisol, suppression test, serum electrolytes
Care:
prevent fluid overload
turn pt frequently/protect skin
Tx: meds that interfere w/ ACTH & glucocorticoid produc.
monitor adrenal supress → hypoglycemia & hypona
Diabetes Mellitus
Group of disorders characterized by ↑ blood glucose lvls
Cause: insulin deficiency, resistance, both
glucose cannot cross cell membrane to enter cell so it remains in bloodstream - insulin is the “key”
T1DM
Insulin producing beta cells of pancreas are destroyed → NO insulin
Signs: polyuria, polydipsia (increased thirst), polyphagia (increased app)
primary cause of diabetes in children
Tx: insulin
subcutaneously
T2DM
Defect in cell membrane → even though insulin is present, the cell “resists” it
leads to ↑ insulin demand & beta cell failure
Signs: polyuria, polydipsia, polyphagia, poor wound heal, visual disturbance
more common in adult
Tx: oral meds
sulfonylureas → stim pancreas to produce insulin
biguanides → decrease hepatic glucose output
alpha glucosidase inhibitor → delay intestional absorp of glucose
Diagnosis for DM
Hemoglobin: 6.5% or higher
measures amount of glucose that binds to rbc
Fasting blood glucose: >126 mg/dL
no caloric intake for at least 8 hrs
Two-hour postprandial test: >200 mg/dL
blood sample taken prior to consump then after at 1 hr & 2hr post
DKA (DM comp.)
Inadequate insulin for cells to obtain adequate glucose for normal metabolism
rapid breakdown of fat stores → release fatty acids → converts to ketone → lead to metabolic acid.
increased release of hormones (glucagon & cortisol) → severe hypergylcemia
Diagnostic:
blood glucose >250
blood pH <7.3
serum bicarb <16
Signs: polyuria, kussmual, fruity acetone breath
Tx:
administer o2
correct electrolyte PRIOR to insulin (will make hypoK worse)
priority: fluid → potassium → insulin
Hyperosmolar hyperglycemic syndrome (HHS)(DM comp.)
Occurs when there is enough insulin to prevent rapid fat/ketones but NOT enough to prevent hyerglycemia (>600)
leads to osmotic diuresis → electro imbalance, neurological defect
EXTREME dehydration
Tx: IV insulin, NaCl infusion
Seizures
Sudden burst of uncontrolled electrical activity in brain → temp disrup of normal func.
Causes: trauma, surgery, tumors, strokes, electrol.
Chronic = epilepsy
Diagnosis: 2 unprovoked seizures that occur at least 24 hrs apart
Signs: *document when seizure starts, presentation, how long it last
4 phases
prodromal → precedes seizure (confusion, anxiety mood, anger)
aural → sensory warning leading up to seizure (flashing light, visual disturbance, smells, voices)
ictal → seizure itself
postictal → rest & recovery (5-30min until baseline)
Other: episodes of daydreaming, unilateral muscle move., repetitive unconscious moves (lip smack, chew, swallow)
Diagnostic: CT/MRI, ECG (may need to repeat)
Tonic clonic (seizures)
Formerly “grand mal” → (#1) generalized seizure
involves both hemispheres
2 phases
Tonic → body stiffens, last for 10-20 sec
Clonic → jerking of extremities, last 30-40 sec
cyanosis, excess saliva, tongue/cheek biting
postictal: soreness & fatigue → pt may sleep for hours & not feel normal for hrs-days
Status epilepticus (seizure comp.)
Seizure activity lasting >5 min OR >2 seizures w/o full recovery of conciousness
Cause: head trauma, hydrocephalus, drug/alc withdrawal (anticonvulsive)
>30 min can cause resp failure, brain damage, death
Seizure management + tx
Med:
antiepileptic/anticonvulsants → ex. gabapentin, levetiracetam, lamotrigine, topiramate
do not stop abruptly → can precipate seizure
side effects: diplopia (blur vision), ataxia, drowsiness
Care:
bed in lowest position, suction at bedside, do not force object in mouth, turn pt to side to prevent aspiration, do NOT restrain
driving restrictions
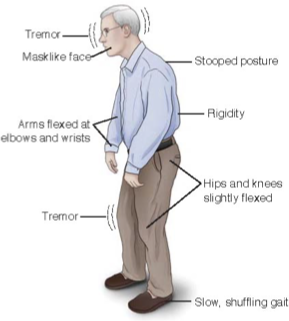
Parkinson’s
Progressive neurological disorder affecting movement, balance, coordination → loss of dopamine producing brain cells
Signs:
resting tremor, muscle rigidity, slow/loss move (bradykinesia/akinesia), postural instability (falls), shuffle & wide gait
Diagnostic: ≥2 cardinal symptoms are observed
Tx: focus on controlling symp
(#1) dopamine receptor agonist → mimic dopamine
side effect: disorder of impulse control (gambling), LE edema, urinary freq
anticholinergics → reduce tremor/drool (not used in older due to side effect)
dopamine pre-cursor (cardidopa-levodioa) → for advanced stage
Care:
fall risk (short, deliberate steps), psychosocial (depression)
Multiple Sclerosis
Chronic progressive neurological disorder → nerves of CNS degenerate → demyelination of nerve fiber + buildup of scar tissue/plaque
Signs: slow nerve conduction → impaired sensation, move, think
numbness in limb, unsteady, muscle spasm, memory, vision, bladder dysfunc, speech impair
Diagnostic: no specific → ruling out other conditions (takes month-yrs)
Tx: no cure
beta interferon, immunosuppressive → slow progession
corticosteroid - tx attacks, inflamm
Care: collab with pt to improve ROM, increase venous return/prevent stiff
rest period to prevent fatigue/overheat
bowel/bladder control → self cath may be needed, increase fluid/fiber
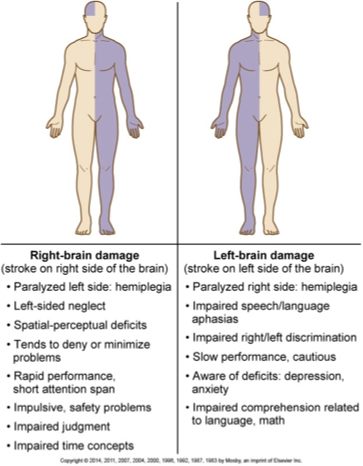
Stroke
Occurs when there is an interruption of blood supply to the brain from ischemia or hemorrhage
also known as “brain attack” or “cva”
Risk factors: htn, smoking, hypocholesterolemia
Signs:
left sided strokes lead to right side deficit (& vice versa)
swallowing, speech, receptive aphasia (loss of comprehension), excessive aphasia (loss of produc of language), global aphasia (no communication)
Diagnostic: CT/MRI
STAT head CT → initial - looks for bleed and determine tx
Care: understand pt baseline, supportive, preventative
monitor serum electrolytes (esp. Na)
bedside swallow screen (NPO until cleared), tuck chin when swallow, thicken liquids, oral care, elevate paralyzed/weak limbs to prevent edema
Transient ischemic attack (TIA)
Temp episode of neurologic dysfunc caused by brief interruption of blood supply to brain
“mini stroke”
no cell death or perm damage, symp resolve in 24 hrs, typically not detected in brain scans
Tx:
meds: antiplatelet & statin
surgery: carotid endarterectomy, stent
Ischemic stroke
Inadequate blood flow to the brain from partial or complete occlusion of an artery
(#1) stroke
Tx: TPA - reestablish blood flow through blocked artery to prevent cell death
pt must be appropriate “candidate” and screened carefully
must be administered within 3.4.5 hrs of symp onset
no recent gi bleed, stroke, head trauma, no major surgery within 14 days
Hemorrhagic stroke
Bleeding within the brain caused by rupture of vessel
Cause: htn
Comp: aneurysm rebleeding, cerebral vasospasm
Tx: control bp, aneurysm clipping or coiling
poor prognosis
Cataracts
Alteration in lens protein/chemical change → gradual clouding of lens
Risk: exposure to UV
Signs: worse w/ progression
vision → clouded, blurred, dim, halo around light source, double vision in single eye
Diagnostic: visual acuity test & direct ophthalmoscope exam (checks opaqueness)
Tx: (#1) surgical removal of lens (replace w/ artificial)
Care:
administer mydriatic (dilating) & cycloplegic (paralyzing) eye drops pre-op, drainage & prevent increase in IOP post-op (fluids, fiber, hob)
maintain eye patch
Glaucoma
Characterized by increased 1) increased IOP, 2) optic nerve atrophy & damage, 3) peripheral vision loss
Normal IOP = 11-21
Types:
primary open angle (gradual): asymp → gradual loss of peripheral vision (both eyes) and tunnel vision (advanced)
IOP 22-32
angle closure (acute): medical emerg → IOP rises very quick & signs include severe eye pain, visual disturbance, reddening
IOP >50
Tx: eye drops (decrease aqueous humor, drain fluids → ↓ IOP)
surgery:
laser trabeculoplasty → open clogged drainage canals
filtering surgery → meshwork to allow aqueous humor to exit
drainage implants
Macular degeneration
Responsible for sharp, central vision → driving, reading, recog. faces
Types:
Dry (#1)(can progress to wet): presence of drusen bodies (yellow deposits under retina)
Wet: when abnormal blood vessels grow under macula → fragile & leak blood & fluid → macula raises from usual position
Signs: distorted central vision → straight lines appear disorted/wavy, difficulty recognizing faces
Diagnostic: Amsler grid, fluorescein angiogram
Tx: no cure
supplements (vit C, E, leutin, zeaxanthin), laser surgery

Meniere’s disease
Disorder of inner ear → leads to vertigo, tinnitus, hearing loss
Cause: unknown → infection, high stress, trauma, excess endolymphatic fluid
mainly affect females 40-60
Signs: varies → n/v/d, abd pain, uncontrollable eye move
Diagnostic: based on presentation/ruling out
Tx: no cure → goal is decrease body fluid & CNS stim.
meds (diuretics, antiemetics, antivertigos)
surgery for severe: vestibular nerve transection, labrynthectomy (removal) → result in total hearing loss
Care:
avoid sudden move, bright lights, caffeine/alcohol, at least 8hr sleep, acupuncture
Osteoporosis
Chronic condition results in deterioration of bone tissue & density → risk for fracture
#1 bone disease
rate of bone resorption (osteoclast) > bone rebuilding (osteoblast)
Risk: aging, ↓ calcitonin, estrogen, ↑ parathyroid hormone
Diagnostic: “silent disease” not diagnosed until fracture/fall/strain
Signs: kyphosis of dorsal spine, loss of height, back pain
Tx + care: prevention & early screening are KEY → prevent/slow progression
↑ calcium & vit D (help w/ collagen synth & bone form.)
calcium: 1200 mg/day
vit D: 15 min/day or 800-1000 units
meds: bisphosphonates - inhibit osteoclast, calcitonin, estrogen
Osteomyelitis
Infection of bone from direct bone contamination (open frac, trauma), extension of soft tissue infection, bloodborne spread
Signs: pain not relieved by rest, swelling/warmth/tender on site
Diagnostic: bone biopsy (#1)
Tx: antibiotic therapy (IV x4-6 weeks → then transition to PO (long term))
surgery/debridement of infected tissue/bone, amputation for severe
Care:
↑ protein, vit for wound heal
thermal therapy (hot + cold)
Fractures
Disruption or break in continuity of a bone (emergency)
usually occur in young/old (b/c bones are porous/weak)
Diagnostic: radiography or CT
Care:
assess neurovascular, immbolize w/ splinting, cover open frac w/ sterile dressing (do NOT attempt to reduce)
diet: ↑ protein, calcium, vit
pulmonary hygiene: deep breath/cough
Tx:
nonsurgical: closed reduction (fractures are manually manipulated & realigned)
surgical: open reduction w/ internal or external fixation (hardware)
Fracture tx
Casts: very rigid → made from fiberglass → may take 24-72 hrs to dry (handle with palms of hands)
assess “CMS” → circulation, movement, sensation
5 Ps → pain, pallor, pulselessness, paresthesia, paralysis
notify provider if noticed
External fixation device: manage open fractures w/ soft tissue damage OR support for complicated/comminuted (crush, splintered)
discomfort minimal → early ambulation, elevate limb, pin care
Traction: short term → pulling force to injury
must be continuous → weights NEVER removed unless order
ropes must be unobstructed & weight hanging freely
Amputation: removal of part of body
DO NOT put pillow under → flat or prone instead
wrap limb to prevent edema + better fit for prosthetic
phantom pain common
Fracture complications
Neurovascular compromise:
any source of ↓ blood flow and o2 to tissues
Compartment syndrome:
↑ pressure in compartment causing compression of nerves/blood vessels
Venous thromboembolism/fat embolism:
clots can hinder circulation and travel to lungs
Traumatic rhabdomyolysis:
damaged muscle tissue releases proteins and electrolytes into blood → damage heart & kidneys
Hemorrhage, hypovolemia:
severe loss of blood
Malunion and nonunion:
fractures fail to heal in correct alignment
Disuse syndrome:
muscle atrophy with loss of strength
Osteoarthritis
Slow progressive disorder involving breakdown of cartilage within joint & underlying bone change “wear and tear”
usually involve weight bearing joints → knees, hips, feet, lumbar spine
Risk: older, female (↓ estrogen)
regular moderate exercise shown to ↓ likelihood/progress.
Signs: joints impacted ASYMMETRICALLY
pain worse w/ activity → relieved by rest, crepitus
Diagnostic: based on signs, x-ray (may only show in advanced)
Tx: no cure
meds: acetaminophen (not exceed 4 g daily)
nsaids: risk of bleed
joint replacement: for severe
assess for orthostatic hypotension & dizziness
hip precautions (for 6-12 wks) → no flex >90 degrees, raised toilet, no crossing leg
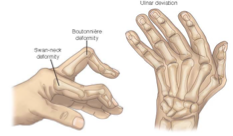
RA
Chronic, systemic, autoimmune inflammatory disease characterized by inflamm that affect daithrodial (freely moving) joints
commonly affect hands, wrist, knees symmetrically
Signs: SYMMETRICAL joint pain, morning stiffness >30 min
Diagnostic: combination (labs (ESR, CRP), radiograph/ultrasound, signs)
Tx:
initial: analgesic (acetam., narcotic), nsaid, glucocorticoids
if ineffective → methotrexate
surgery
Care:
keep up w/ vax (NO live vaccines)
Gout
Accumulation of uric acid crystals in joints → body attempt to get rid of them resulting in inflamm
Risk: red meat/seafood/alcohol, use of thiazide diuretic
Sign: starts w/ inflamm of great toe
Diagnostic: observing crystal in synovial fluid
Tx: avoid high purine foods
meds:
acute: pain relief & inflamm (nsaid)
chronic: allopurinol (lower uric acid)