BIOL 220 Airborne Diseases
1/28
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
29 Terms
What is a positive vs. negative pressure room?
Positive: push air out = very little pathogens to enter when door is open
Negative: suck air in = pathogens enter + do not exit in order to contain pathogens (contagious disease with low LD50)
How can Airborne Diseases spread
Indirect contact/Transmission: Transmission of a pathogen/disease through a contaminated non-living object (Fomite)
Contact transmission: Droplet transmission (airborne particles spread less than 1 meter in distance)
Vehicle Transmission: Airborne transmission (airborne particles greater than 1 meter in distance)
What are common predisposing factor for airborne infections?
Weakened immune system: HIV/AIDS, Cancer and chemotherapy, Autoimmune diseases
Age: Elderly (65+), infants and young children (not well-developed adaptive immunity)
Life style: Smoking/Vaping, Alcohol abuse
Environmental conditions: Crowded conditions, Urban areas with high Air pollution, multigenerational family housing - children
What is the major port of entry for airborne diseases?
Respiratory Tract - Involved in breathing & gas exchange
Upper respiratory tract: Filters air before it enters the lungs
• Nose
• Nasal cavity
• Sinus
• Pharynx (throat)
• Larynx (voice box)
Lower respiratory tract: Facilitates gas exchange between Oxygen intake and carbon dioxide release
• Trachea (windpipe)
• Bronchi
• Bronchioles
• Alveoli
What are the general S/Sx for airborne diseases
• Fever + Chills, Fatigue, Headache and body aches
• Coughs (wet/dry), sneezing, running or stuffy nose, sore throat
• Shortness of breath and difficulty breathing
What are the Host Defenses against Airborne Pathogens
• Normal microbiota (Biological barrier + 1st line defense): found in the upper respiratory tract → competitive
exclusion
• Mucus + Nasal hair : Traps dusts, microbes and other particles → prevents antigens from entering the respiratory tract; has IgA
• Lysozyme: Lytic enzymes secreted by epithelial cells in our airways to break down peptidoglycan
• Ciliary escalator: helps clear mucus, dust, pathogens and other particles up and out of the respiratory tract
• Coughing and Sneezing reflex: Helps expel irritants or pathogens from entering the respiratory tract
What is Streptococcus and its different types? How do we use differential media to differentiate the diffferent types?
Streptococcus (Gram-positive Cocci + arranged in chains)
• Streptococcus pneumoniae vs. Streptococcus pyogenes
Use differential media to help identify Streptococcus bacteria + implement the proper treatment
• RBC’s act as a nutrient source on the agar → Hemolysis occurs (RBCs lysed by hemolysins, type I exotoxin)
• Alpha Hemolysis: Partial lysis/destruction of RBC → Green Zone → S. pneumoniae
• Beta Hemolysis: Complete lysis/destruction of RBC → Clear zone/yellow color → S. pyogenes
Streptococcal Pharyngitis: Alternative Name/Type of Infection, S/Sx, and Causative Agent
Alternative Name: “Strep Throat”
• Upper Respiratory tract infection
S/Sx:
• Inflammation of the throat & tonsils
• Throat feels sore and “scratchy” + white patches or streaks of pus
• Red spots on the roof of the mouth
• Fever
Causative Agent: Streptococcus pyogenes:
• Gram-positive cocci arranged in chains; group A streptococci (GAS)
Streptococcal Pharyngitis: Virulence Factor and Diagnosis
Virulence Factor:
• Beta hemolysin: completely lyses RBC’s (clear zone, yellow color)
• Strepto-kinase: dissolves/prevents blood clot formation
• Hyaluronidase: dissolves substances holding connective tissue cells together
• Capsules + M proteins: allow for adherence and escape of phagocytosis
Diagnosis:
• Serological testing of blood or other body fluids (rapid antigen detection tests) → Beta Hemolysis on blood agar
Streptococcal Pharyngitis: Prevention and Treatment
Prevention:
• Practicing good respiratory hygiene (Ex: cover mouth + nose via masks)
• Avoid sharing cups & utensils
Treatment: with Antibiotics (Penicillin or amoxicillin)
Scarlet Fever: Alternative Name/Type of Infection, S/Sx, and Causative Agent
Alternative Name: Scarlatina
• Upper respiratory tract infection
S/Sx: due to toxemia
• Sore throat & high fever → Type I Exotoxin: SuperAntigen
• Pastia’s Lines: red/purple lines that appear in skin folds → caused by erythrogenic toxins
• Flat red/pink rash that is Sandpaper-like on the chest and throughout the body → caused by the erythrogenic toxin that damages the blood capillaries under the skin
• Strawberry tongue: Red & bumpy tongue covered with a white coating
Causative Agent: Streptococcus pyogenes
Scarlet Fever: Virulence Factor and Diagnosis
Virulence Factor:
• Beta hemolysin, Streptokinase, Hyaluronidase, Capsules + M proteins
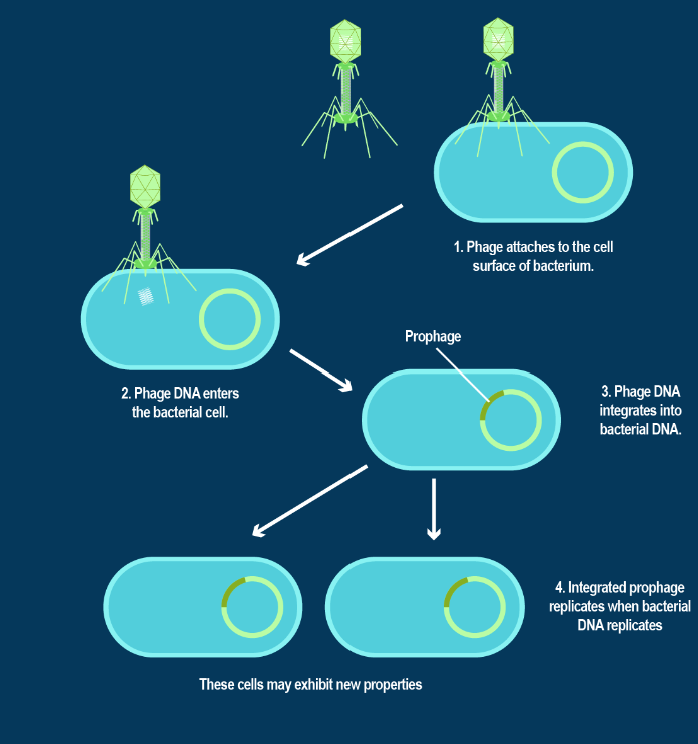
• Erythrogenic toxin (also known as streptococcal pyrogenic exotoxins) made via lysogenic cycle: Toxin producing gene is on a bacteriophage → Viral infection of S. pyogenes leads to a prophage (hybrid genetic material) → S. pyogenes will now produce erythrogenic toxins
Diagnosis:
• Serological tests (Rapid antigen detection tests) + Beta hemolysis on blood agar
Scarlet Fever: Prevention and Treatment? What age group is this disease most common in?
Prevention: Practicing good respiratory hygiene
Treatment: Antibiotics (Penicillin & amoxicillin)
Most common in children (ages 5-15)
• Most common cause of death in children in the 1800
• Rare disease in today’s time
Rheumatic Fever: Alternative Name/Type of Infection and Causative Agent
Alternative Name/Type of Infection:
• Autoimmune Reaction Mechanism: S. pyogenes has M proteins and other antigens that mimic human tissues
in the heart, joints, and brain → immune system makes antibodies to fight the bacteria but the antibodies
mistakenly attack the body’s own tissues → inflammation
• Upper respiratory tract infection, on list of national notifiable diseases
Causative agent: Corynebacterium diphtheriae
• Gram Positive Bacilli
• Pleomorphic: Can exist in a variety of shapes like clubbed shaped
Rheumatic Fever: Virulence Factor and Treatment of Non-toxigenic strain
Non-toxigenic strain
• No exotoxin production
• Less severe S/Sx compared to toxigenic strain
• Mild sore throat, potential ear infection, and skin infections
• Chronic non-healing sores/ulcers on the skin
• Treatment with antibiotics + diphtheria antitoxin (DAT) is not helpful
Rheumatic Fever: Virulence Factor and Treatment of Toxigenic strain
Diphtheria strain: powerful exotoxin, lead to toxemia (produced via lysogeny by a bacteriophage)
• Causes heart and kidney damage → can lead to myocarditis and heart failure
• Nerve damage and partial paralysis
• Psuedomembrane: Thick & gray coating of dead tissue on pallet, nose and throat
• Difficulty breathing and swallowing
• Death (especially when untreated)
• Treatment with antibiotics & diphtheria antitoxin
Rheumatic Fever: Diagnosis and Prevention
Diagnosis:
• throat swab → culture swab
Prevention: Diphtheria vaccine (Based on age group)
1. DtaP (series of 5 shots for young children)
• Diphtheria, Tetanus, acellular Pertussis
2. TDaP (for pre-teens, 11-12 yrs)
• Tetanus, Diphtheria, acellular Pertussis
3. Td (for adults)
• Tetanus & Diphtheria toxoid (bacterial toxin that has been inactivated to trigger an immune response)
Pertussis: Alternative Name/Type of Infection, S/Sx, and Causative Agent
Alterative Name/Type of Infection
• Whooping Cough”
• Highly contagious bacterial infection + targets lower respiratory tract
Causative agent: Bordetella pertussis
• Gram-negative aerobic coccobacillus
S/Sx:
• 5–10 day incubation period; no symptoms
• Initially mild S/Sx: Cold like symptoms- Runny nose, mild cough, Fever, and sneezing = infectious without • showing severe coughing
• Progress to more severe S/Sx: Uncontrollable violet coughing; can last for weeks-months (also called
the 100-day cough)
Pertussis: Virulence Factor and Diagnosis
Virulence factors:
• Capsule production for the attachment to ciliated cells in the trachea
• Tracheal cytotoxin: damages ciliated cells and shuts down the ciliary escalator
Diagnosis: Culturing of throat mucus sample
Pertussis: Prevention and Treatment? How is it dangerous to babies?
Prevention: Pertussis Vaccine
1. DTaP (Diphtheria, Tetanus, acellular Pertussis)
2. TDaP (Tetanus, Diphtheria, acellular Pertussis)
Treatment: Antibiotics (Penicillin or Amoxicillin) + Supportive care (Rest + Fluids)
Dangerous in babies because of their tiny airways → respiratory complications, may get clogged by inflammation
Pneumonias: Alternative Name/Type of Infection and the two types of Pneumonias
Alternative Name/Type of Infection:
• Lower respiratory infection → inflammation + fluid build up in one or both lungs
2 Types of Pneumonias:
1. Typical: Caused by Bacteria (S. pneumoniae)
2. Atypical: Caused by other microorganisms that are Viral or Fungal
Typical Pneumonia: Alternative Name/Type of Infection, S/Sx, and Causative Agent
Alternative Name/Type of Infection:
• Pneumococcal Pneumonia
• Lower respiratory tract infection
Causative Agent: Streptococcus pneumoniae
• Gram-positive bacterium, Encapsulated diplococci + Very large capsules
• ~ 90 different serovars/strains
S/Sx:
• Acute
• Chest Pain, Fever, Chills, fatigue
• Fluid accumulation in the lungs (specifically at the alveoli level) → interfere with gas exchange
• RED FLAGS: Labored/rapid breathing + bluish lips, face or fingers + coughing up blood/mucus
Typical Pneumonia: Virulence Factor and Diagnosis
Virulence Factors:
• Production of Large capsules
• Alpha hemolysin – partially lyses Red Blood Cells (green zone)
Diagnosis:
• Blood tests, Alpha hemolysis on blood agar, presence of capsular antigen in patient’s urine
Typical Pneumonia: Prevention and Treatment
Prevention:
• pneumococcal conjugate vaccine PCV13/Prevnar 13
• Protects against 13 serovars/strains based on capsule structure
• Age is a predisposing factor
Treatment: Antibiotics (Penicillin/Amoxicillin)
Atypical Pneumonia: Causative Agents
Caused by non-bacterial Microbes/Biological Agents:
1. Influenza virus & Sar-CoV-2 → Viral Pneumonia
2. Pneumocystis jirovecii → Fungal Pneumonia (Typically seen in immunocompromised Hosts like HIV/AIDs patients)
Tuberculosis: Alternative Name/Type of Infection, S/Sx, and Causative Agent
Alternative Name/Type of Infection:
• Lower respiratory tract infection
• Leading cause of death from infectious diseases worldwide
• 1/3 of the world’s population has latent TB (Infected but inactive) = No symptoms, not contagious
Caused by Mycobacterium tuberculosis
• Acid-fast bacterium, bacilli, obligate aerobe
• High lipid content in cell walls; resists traditional staining methods
• Fungus-like growth
S/Sx/Chronic Symptoms from a ruptured tubercle:
• Persistent low grade fever, night sweats, weight loss, weakness
• Bloody cough – means alveolar damage
• In Miliary Tuberculosis: Bacterial spread from the primary infection site (alveolar of the lungs) to other areas of the lungs, liver, nervous system and even bone
• Tuberculosis encephalitis
• Tuberculous hepatitis
Tuberculosis: Virulence Factor and Diagnosis
Virulence Factor:
• Mycolic Acid (waxy lipid) in the cell wall
• Allows bacteria to escape phagocytosis and multiply in macrophages
• Resists lysosomal enzymes + drying out
Diagnosis:
(Step 1)
• Mantoux Test (Tuberculin skin tests)
• Subdermal injection of Tuberculin proteins → check for induration (raised bump or hardness) 48-72 hours later (Delayed immune reaction)
• T cells react to Tuberculin protein
• Positive reaction indicates current or previous infection
(Step 2)
• Patient X-ray/CT Scan → Look for calcified tubercule (white spots indicate tubercle formation)
• Positive chest x-ray means a current or previous infection
(Step 3)
• Acid fast Stain: Collect sputum (fluid at lung base) from the patient → Culture and isolate bacterial colonies → Run an acid-fast staining technique (Mycobacterium stains pink vs. Non-Mycobacterium stains blue)
Tuberculosis: Treatment
• Minimum of 6 months of multi drug therapy due to slow growth + dormancy
• Initial treatment: Multiple drug cocktail
• First-line drugs: most effective and least toxic treatments
• Second-line drugs: used when first line drug treatments are not effective
• Multi-drug-resistant (MDR) strains: resistant to first-line drugs
• Extensively drug-resistant (XDR) strains: resistant to second-line drugs
What is the Pathogenesis of Tuberculosis
1. Inhaled bacteria is phagocytized by alveolar macrophages → Mycolic Acid allows the bacteria to survive and multiply inside the macrophages = causes an inflammatory response
2. More macrophages are recruited → surround and isolate the bacterial infection inside a tubercle/granuloma (aggregation of activated macrophages trapping the bacteria inside)
2 possibilities after tubercle formation = Latent TB vs Miliary TB
Latent TB
• Bacteria stop growing in the tubercle lesion and the disease process stops for now → Causes the bacterial infection to remain dormant
• Tubercule heals and calcifies (Ranke complexes) → Can get reactivated if patient has a weakened immune system
Miliary TB
• Bacteria grow/multiply outside of macrophages
• Tubercle gets broken down → releasing the bacteria into the lungs and cardiovascular system → Leads to a systemic infection