SOCPSY 3A03 Test 2
1/76
Earn XP
Description and Tags
Weeks 4-6
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
77 Terms
Social Identity Theory
Social identification → in-group bias
In-group favouritism: like people more who are in-group members than out-group
Fundamental need for belonging
The Social Cure
Multiple social groups → protects against poorer health
All eggs in one basket vs many baskets
Social Identity and Life Transitions
Students → university → lower well-being
More group memberships → less depression
New social identity → better well-being
Belonging to more groups → lower depression
Stronger university social identity → higher well-being and motivation
Social Cure for Loneliness
Social Cure for Loneliness
Loneliness: “ psychological experience of unwanted social isolation”
Social Prescribing
Social Prescribing
Used by healthcare professionals to increase social integration
Help people buffer against social identity loss by encouraging to join new group that promotes social identity
Benefits of Group Type Diversity
Reduce loneliness, increase well-being
The Social Cure Across Cultures
High Relational Mobility: freely enter/leave groups (western, independent)
Low Relational Mobility: group memberships less permeable (non-western, collectivistic)
What Happens When We Belong to Social Groups that are Unsuccessful?
Membership in low esteem group → decreases well-being
High Strength and Centrality of Social Identity
Success → Bask in Reflected Glory (BIRGing)
Loss → less likely to Cut Off Reflected Failure (CORFing), re-affirm in-group commitment
Low Strength and Centrality of Social Identity
Less BIRGing, more CORFing
Social Identification and Discrimination
Black Americans facing discrimination → lower well-being, but stronger social identification
But should hold social structures responsible rather than individual to empower themself
BBC Prison Study
BBC Prison Study
Better version of Stanford Prison Experiment
Prisoners: strong social identity
Guards: social identity did not develop
Reading: Social Group Memberships Protect Against Depression - Cruwys et al
Belonging to more social groups → lower future depression
Positive effects especially strong for depressed individuals
More group memberships linked to lower relapse risk
Building social group connections useful for public health interventions
Reading: Tackling Loneliness Together - Haslam et al
Social prescribing reduces loneliness and improves mental health when it successfully connects people to groups
Group membership and social identification key
Benefits greater when individuals feel they belong to and identify with groups they join
Social identity-based approaches improve outcomes across different SP levels (community, group, and individual interventions)
Social Ties and Mental Health
Tie Strength
Vitamin S and Well-Being
Tie Strength
Weak Ties: low time spent together and emotional intensity, intimacy, and reciprocity
Weak ties → well-being and mental health
Small talk with stranger → well-being
Strong Ties: high time spent together and emotional intensity, intimacy, and reciprocity
Relationship problems → people seek counselling
Social isolation → mortality
Poor-quality strong-tie relationships → depression
Strength of Weak Ties
Diffusion of information through social network
More likely to be exposed to more information
Vitamin S and Well-Being
Vitamin S: Vitamin Social contact
Most interactions with strangers benign
Strangers benign
Interactions with strangers can fulfil need for social contact
How do Social Ties Enhance Mental Health?
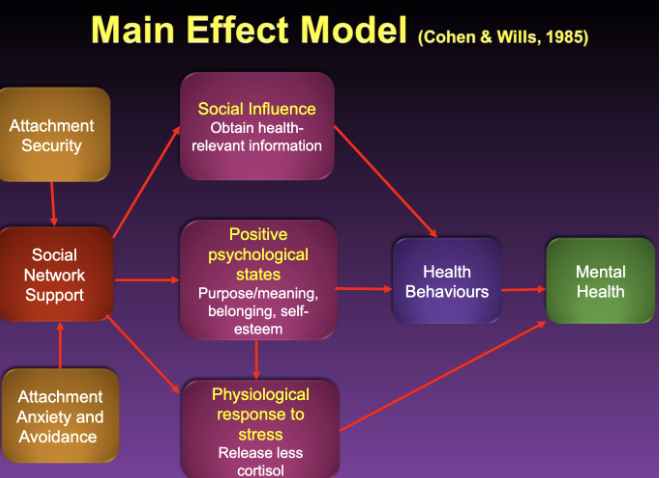
Main Model Effect
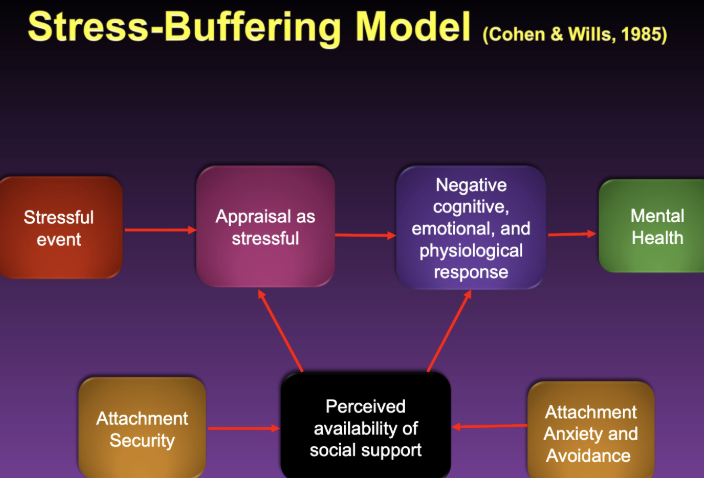
Stress-Buffering Model
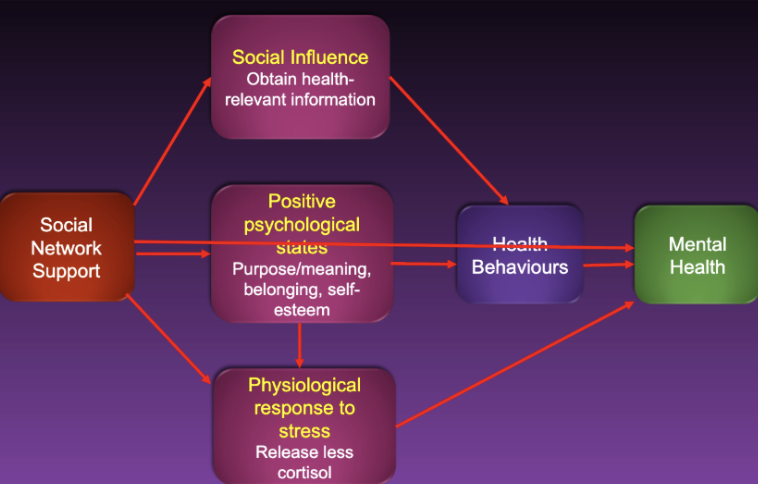
Main Effect Model
Social relationships improve mental health for everyone regardless of person’s stress levels
Social network support: people more likely to seek help if social network suggests it first → social influence → positive health behaviours → improved mental health
Social contact itself → positive psychological states → positive health behaviours → improved mental health
Positive psychological states → decrease psychological response to stress → improved mental health
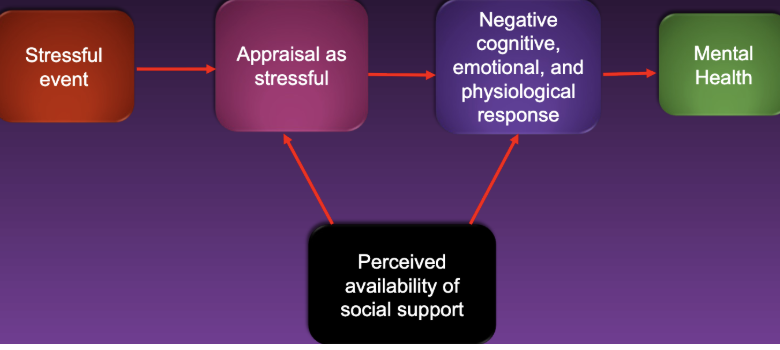
Stress-Buffering Model
Social relationships improve mental health mainly for people who experience high stress
Perceived availability of social support → decrease appraisal as stressful → lowers negative stress response → improved mental health
Perceived availability of social support → lowers negative stress response → improved mental health
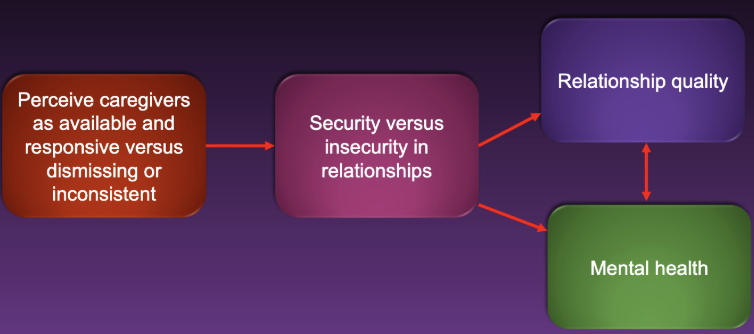
Attachment Theory
How early childhood relationships influence perceptions of social support availability as adults
Infant’s history of interactions with primary caregiver → willingness to trust and depend on close others
Attachment Anxiety
Attachment Avoidance
Attachment Security
Attachment Anxiety
Caregiver inconsistently responsive
Negative model of self
Worry about caregiver’s availability, fear abandonment
Threats → hyperactivating strategies
Seek closeness, feel angry, distressed, possessive
Attachment Avoidance
Caregiver neither sensitive nor responsive
Negative model of others
Mistrustful and self-reliant
Avoid closeness
Threat → deactivating strategies
Deny attachment needs
Attachment Security
Low in anxiety and avoidance
Caregiver sensitive and responsive
Positive model of self and others
Self is worthy of love
Comfortable with closeness
Attachment and Mental Health
Insecurity (anxiety/avoidance) → risk of depression, anxiety, PTSD, eating disorders, personality disorders
Attachment-Mental Health Link: Mechanisms
Low self-worth
Emotional dysregulation
Relationship problems
Attachment insecurity ↔ genetic predispositions to mental health disorders and stressful life events
Main Effect Model: high attachment security more likely to seek social network support in healthier ways
Stress-Buffering Model: secure individuals more likely to perceive social support as available, less likely to appraise event as stressful
Attachment-Mental Health Link: Main Effect Model
Attachment-Mental Health Link: Stress-Buffering Model
Committed Relationships Can Protect Mental Health
Marriage → better physical and mental health
Committed Relationships Linked to Better Health
Premarital Relationships and Health
Why are Committed Relationships Linked with Better Health?
Selection Hypothesis: people with better mental health more likely to get married
Social Support Hypothesis: ties in with Main Effect and Stress-Buffering models
Behavioural Regulation Hypothesis: spouses encourage healthier behaviour
Premarital Relationships and Health
Premarital relationships similar to marital relationships
Risky behaviour in university students
Students in committed relationships (vs single students) → less risky behaviour → better mental health (but not physical health)
Happy Singles
Single people who avoid conflict as high in life satisfaction as people involved in relationship
Free of relationship anxiety
More single people than ever before
Relationship Maintenance and Mental Health
Staying in committed, low-quality relationship bad for mental health
Predictors of greater relationship quality:
Few negative communication behaviours
More interactional synchrony
More positive support behaviours
Self-Expanding Relationships Decrease Depression
Sexual Satisfaction as Relationship Maintenance
Self-Expanding Relationships Can Decrease Depression
Self-Expansion: augmenting or re-organizing self-concept to include new content or skills
Incorporate partner’s identity, engage in activities that are novel and arousing
Self-expanding relationship → decrease depression
Sexual Satisfaction as Relationship Maintenance
Sexual satisfaction → relationship quality
Sexual frequency → relationship satisfaction well-being
Make-up sex after a fight → maintains relationship quality
Breakups and Mental Health
Related to onset of:
Negative emotions and intrusive thoughts
Major depression
Physiological disruption
Breakup Narratives
Attachment Anxiety
Ghosting and Breadcrumbing
Divorce and Depression
Breakup Narratives Reveal Clues about Mental Health
Study conducted over 6 months of breakup description:
Time 1: detailed explanation of breakup reasoning
Time 2: simplified version as they went through search for meaning and have greater sense of closure
Language
Language and breakup Narratives
Writing about breakup featured higher frequency of:
Negative emotion words
Causal words
Sensory words
Present-tense words
First-person pronouns
Can detect future breakup
Increase in I-words (preoccupied with internal turmoil), we-words (collective focus and difficulty dissociating from relationship), and cognitive processing words (meaning making)
Low analytic thinking words
Attachment Anxiety and Reactions to Breakups
Anxious have more negative reactions
Distress, drug/alcohol abuse, preoccupation with ex-partners
Social media surveillance of ex
Harder time letting go, rebounding helps
Breaking up by Ghosting or Breadcrumbling
Ghosting: ending a relationship by disappearing
Drop in relational value
Breadcrumbing: stringing partners along with intermittent attention/flirtation
Breadcrumbing associated with poorer psychological well-being
Divorce and Depression
Poor marital quality ↔ depression
Less evidence that depression generates stressful marital interactions
Breakups can Relieve Depression
Divorce experienced as loss, humiliation, shock → onset of depression
Ending bad marriage → recovery from depression
Divorce as escape from chronic stress of bad marriage
Reading: Romantic Relationships and Mental Health - McIntyre et al
Higher self-expansion in romantic relationships → lower depression symptoms
Daily level: higher self-expansion = lower same-day depression (no reliable next-day or partner effects)
Longitudinally: increases in self-expansion over time → decreases in depression and better mental health
Overall pattern: more relationship self-expansion linked to better mental health outcomes
Reading: Psychological Correlates of Ghosting and Breadcrumbing - Navarro et al
Breadcrumbing: lower life satisfaction, higher loneliness, higher helplessness
Ghosting: no significant relationship with any psychological outcomes
Combined victims: worst well-being outcomes overall
Regression results: breadcrumbing predicts lower life satisfaction and higher loneliness (weak effect for helplessness)
Overall: breadcrumbing shows negative psychological impact, ghosting does not in this study
Reading: Social Media Language Effect on Romantic Breakups - Seraj et al
Language changes appear ~3 months before breakup, peak at breakup, normalize by ~6 months after
More I/we words and cognitive processing, less analytic thinking
Effects show up across all online activity, not just relationship posts
Longer posting about breakup → worse long-term adjustment
Screen Time and Adolescent Mental Health
Depression and suicide deaths increased
Correlated with electronic device use
Linear dose-response
Social Media Use and Adolescents’ Depression
Gender difference: girls’ internet use predicts later depression
Contributes to teenage depression
Contributes to social comparison
Why Might Social Media Use Contribute to Teenagers’ Depression?
Social media use at night → poorer sleep quality
Cyberbullying
Edited images make people have negative self-image
Social Comparison Theory
Find out where you stand
Downward Comparison
Someone is worse off → relief, schadenfreude
Feel superior to others
Upward Comparison
Someone is better off
Feel inferior to others
Negative emotions
Envy lowers well-being
Evidence that Social Media Use Increases Envy
Social Presentation
Dramatic performances
Goffman’s theory
Seeing Attractive/Successful People
High envy
Upward Conditions
Make people feel negative, emphathetic towards others’ failures
Mechanisms Linking Adolescent Social Media Use to Mental Health Problems
Behavioural Mechanism: risky behaviour → high publicness and permanence
Cognitive Mechanism: social comparison → high quantifiability
Neurobiological Mechanism: increasing stress → low synchronicity
Do Adolescents with Diagnosed Mental Disorders Use Social Media Differently?
Unhealthy use of social media ↔ mental health disorder
Internalizing disorder
Correlation of Digital Technology Use with Teenagers’ Well-Being
Digital technology use contributes to poorer well-being, small effects
Null Effects of Social Technology
Active social media use increases social capital
Prosocial use of social media increases well-being
Canadians > Thais: knowledge-sharing → greater life satisfaction
Canadians = Thais: emotionally-supportive prosocial behaviour → greater well-being
Null Effects of Social Technology Use on Mental Health
No evidence that social technology contributes to suicide
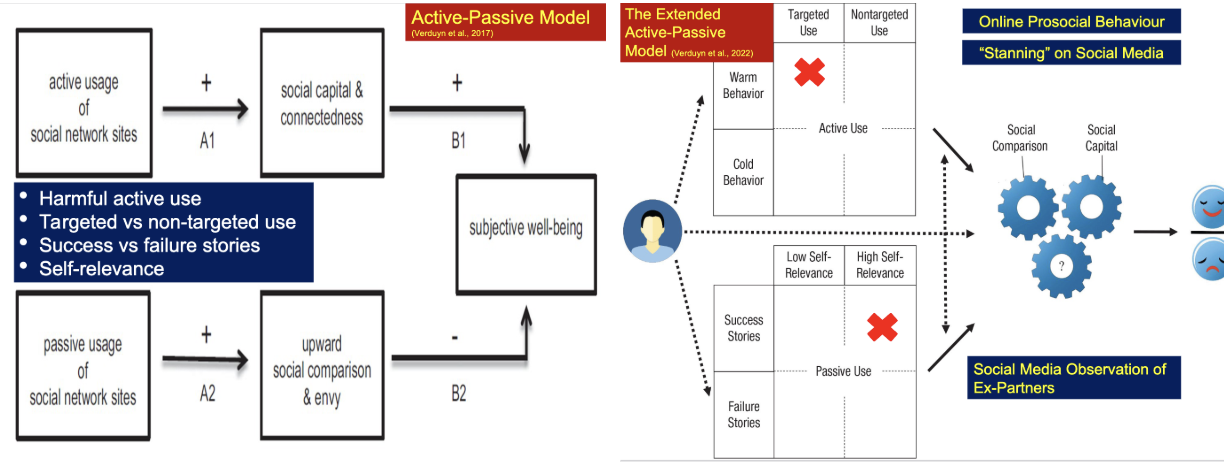
Active-Passive Model
Active-Passive Model
Distinguishes between active and passive use of social media
Active: direct interaction with users
Passive: social media use that does not directly interact with other users
Reading: Social Media and Well-Being: Pitfalls, Progress, and Next Steps - Kross et al
Social media has small negative effect on well-being
Results mixed when looking only at time spent online
Main conclusion: how people use social media matters more than how much they use it
Reading: Increase in negative Well-Being Due to Social Media Use - Twenge et al
Depression and suicide rates increased among adolescents after 2010, especially in girls
More in-person activities and exercise → better mental health
Screen use increased while nonscreen activities decreased over same period
Main conclusion: rising social media and phone use may have contributed to worsening adolescent mental health
Stigma
Goffman: prejudice and discrimination directed at people with “devalued” attributes
Mental Health Stigma
Cues, stereotypes, prejudice, and discrimination
Mental Health Stigma: Cues
Psychiatric symptoms
Deficits in social skills
Physical appearance
Labels
Mental Health Stigma: Sterotypes
Beliefs about a stigmatized group
Inaccurate and can lead to stigma
Mental Health Stigma: Prejudice
Believe stereotypes + negative emotional reactions
Mental Health Stigma: Discrimination
Acting on one’s prejudice
Outgroup hostility, ingroup favouritism
Avoidance
Public Stigma
Negative reactions from members of public
Ex. employers, landlords, police officers, medical professionals
Mental health more stigmatized than physical health, psychotic > anxiety, depressive disorders
Self-Stigma
Negative reactions towards oneself
Underutilization of Mental Health Services
Stigma → may not seek treatment at all
Stigma → underutilize services, low adherence
Stigma → end treatment early
How Does Stigma Lead to More Negative Attitudes Toward Help-Seeking?
Mental health stigma → greater anxiety → lower self-efficacy → more negative attitudes toward seeking professional help
Reducing Stigma
Protest
Education
Contact
Empowerment
Reading: How Stigma Interferes With Mental Health Care - Corrigan
Mental health stigma is major barrier to seeking and continuing treatment
People avoid care to escape label of mental illness and associated discrimination
Mental Health Literacy
“Knowledge and beliefs about mental disorders which aid their recognition, management or prevention”
Mental Health Literacy: Recognition of When a Disorder is Developing
Delay help-seeking after onset
Need to get rid of ethnocentrism
Recognition of depression
Canada, Australia > Japan, Sweden
Depression > schizophrenia, anxiety disorders
Low recognition → less help-seeking
Delayed recognition in youth
Recognition → help-seeking, but risk of stigma and labelling
Mental Health Literacy: Knowledge and Beliefs About Help-Seeking and Treatment
Knowledge of sources available and belief sources effective
Informal Help: friends, family, spouses
Professional Help: doctor, clinical psychologist, psychotherapist, counsellor
Informal > professional
Less helpful for severe problems
Non-Western > Western
Public: negative attitudes towards medication, positive attitudes towards psychological interventions
Positive beliefs → more likely to seek
Mental Health Literacy: Knowledge of Self-Help Options for Milder Mental Health Problems
Public has positive attitudes towards self-help
Effective to try different self-help techniques in waves
Self-help for mild/moderate distress
More severe → professional help
Mental Health Literacy: Mental Health First Aid Skills
Family/friends can recognize person’s disorder and provide social support
Mental Health Literacy: Knowledge of Mental Illness Prevention
Societal Level
Reduce likelihood of trauma and structural inequality
Individual Level
Public and therapists agree on everyday prevention
Disagree about stress: public avoid stress, professionals → face stress head-on
What Role do Influencers Play in Mental Health Literacy?
Young people more vulnerable to mental health problems, few pursue professional help-seeking
Mental health influencers on TikTok and Instagram
23% TikTok and 7% posts reflected component of recognition
<10% promoted knowledge of professional help-seeking
Majority of Instagram accounts promoted crisis support
Reading: Empowering the Community to Take Action - Jorm
Mental health literacy generally low in public
Many struggle to recognize mental disorders and know how to get help
Educational interventions consistently improve mental health literacy
Better mental health literacy → improved help-seeking and support
Increasing mental health literacy should be public health priority