Gastric Tubes and Enteral Nutrition
1/28
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
29 Terms
Nutritional Support
-There are 2 routes for the delivery of nutritional support in pts:
-Enteral Nutrition: includes PO ingestion of foods and the delivery of nutrients through a GI tube, Generally easier, safer and more cost effective
-Parenteral Nutrition (PN): IV nutritional therapy, custom solution pt-specific
Nutritional Assessment
-Dietician and Physician: need to get them before giving a tube feed
-GI function? not eating enough?
-How long will this be needed? Trauma? Surgery?
-Is the pt at risk for complications…such as aspiration
Enteral Feeding Routes
-Nasogastric (NG): inserted through the nose and into the stomach
-Nasointestinal (NI): is passed through the nose and into the upper portion of the small intestine (nasoduodenal and nasojejunal)
-Nasogastric decompression tube (salem sump)
-Gastrostomy tube: goes straight to the stomach
-Percutaneous Endoscopic gastrostomy (PEG) tube
-Low-profile gastrostomy device (LPGD): tube end is flat against the surface of the skin
Indications for Tube Use
-Decompression (upper GI)
-Gastric lavage (toxins)
-Diagnostics for motility disorders
-Administration of meds and feedings
-Management of obstruction
-Severe constipation
-Aspiration of gastric contents
-Bowel rest
Nasogastric (NG) and Nasointestinal (NI) tubes
-Short-term use, generally <4 weeks
-Acidic pH secretions protect against infection
-Some tubes may be more rigid than others: Levin tube, Dobhoff tube
-NI tubes used for aspiration risks or delayed motility
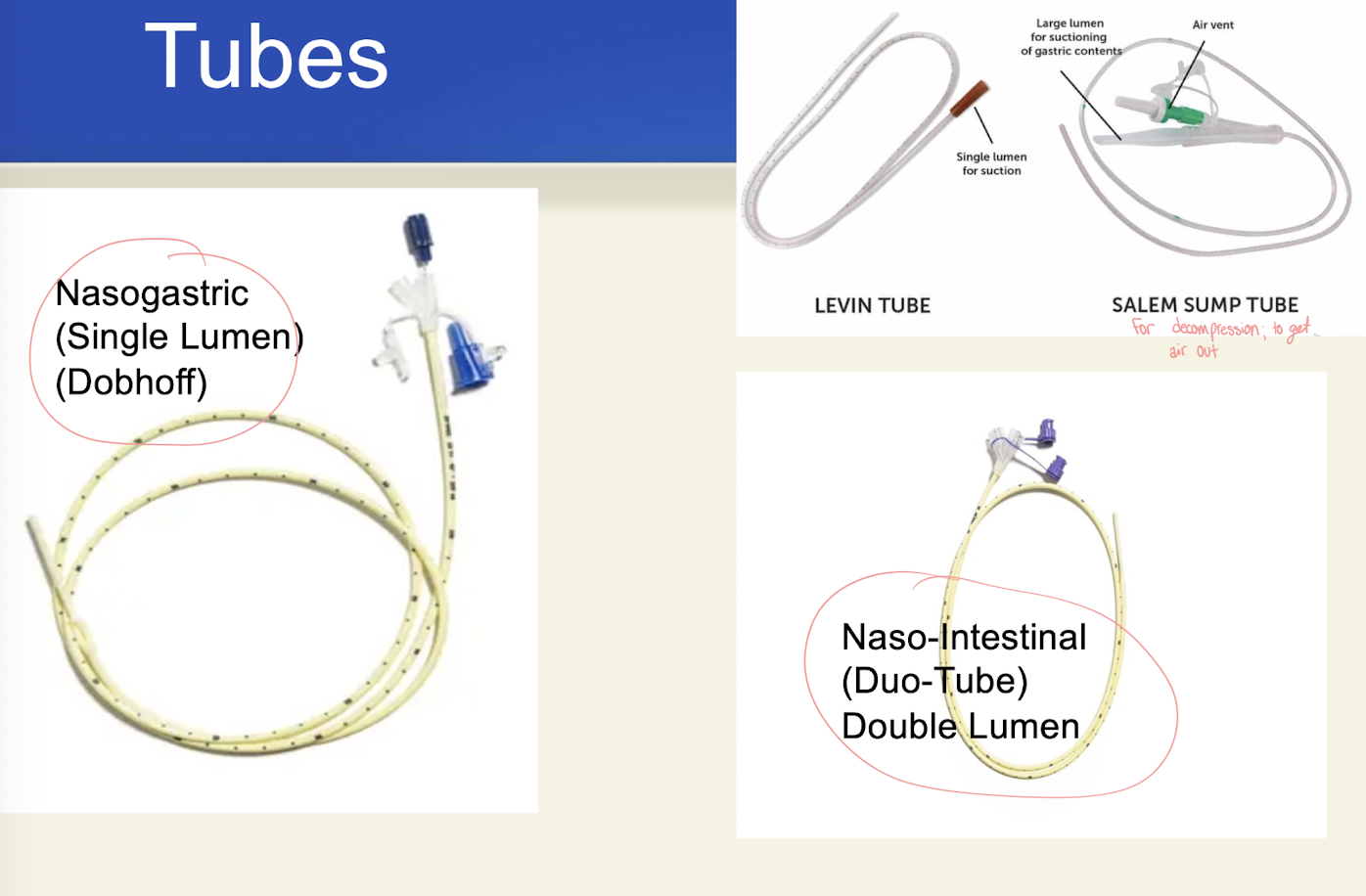
Salem Sump
-Used to decompress upper GI tract
-2 lumens: one is a blue air vent→ prevents adherence to stomach lining
-To prevent reflux, always keep above pt’s waist
GJ tube
-Gastric port for meds
-J port for feedings
-Gastric port may be attached to no intermittent suction or gravity drainage

Procedure for insertion
-RNs may place NGs (no guidewire)
-MDs or CRNPs; weighted tubes (wired)
-Measure tip of nose to earlobe, then earlobe to xyphoid process (mark with tape)
-Pt in High fowler’s (cover chest)
-Lubricate tube and wear gloves
-Inspect nostrils for patency, healed and/or acute trauma
Insertion Procedure
-Insert tube into nare ~30 degrees
-At nasopharnyx, lower head slightly
-Easier if pt can safely sip water through straw as tube advanced
-Check in mouth to be sure not coiled
-Tape securely in place
Nursing Responsibities
-Two or more of these techniques in conjunction with each other increases the likelihood of correct tube placement
-Radiographic examination (always and required)
-Measurement of aspirate pH (only on insertion)
-Monitoring of carbon dioxide
pH
-Stomach: Suggested limits for a safe range are from <4.0, <5.0, and <5.5
-<5.5 means you are in the stomach
-Intestines: pH 7.0 or higher
-Respiratory tract: >=6.0
-This method will not effectively differentiate between intestinal fluid and pleural fluid
Daily care
-Once confirmed by x-ray, the number you see on the tube, closest to the nostril is your safe measurement; always check measurement and document first number under the nose
-Mouth care at least every two hours- skin care prn (clean nostril with moistened cotton tipped swabs, change tape q2-3 days)
-Lozenges, ice chips, hard candy (responsibly)
-Careful record of intake and output→ mainly whats coming out if on decompression
-Weight at least twice a week
-May also ingest PO food with enteral feedings
Ongoing evaluation
-Monitor lab work:
-Electrolytes
-BUN, creatinine
-Glucose
-Protein and albumin levels
-H&H
Nursing Responsibilities of Feedings
-Standard formulas contain intact molecules of protein, carbs, and fats, requiring the patient to have normal digestion and absorption
-Hydrolyzed formulas contain proteins and other nutrients in simple forms that require little or no digestion
-These formulas are used with pts with impaired digestion or absorption
Types of feedings
-Bolus formula (no feeding pump): 200 to 400ml volume, 15-60min- syringe
-Intermittent: set volume at regular intervals
-Continuous: set volume: 12, 18, or 24 hours
Flushing Tube
-As ordered by physician
-Before and after feedings or meds
-When feeding is interrupted/restarted
-Following aspiration of stomach contents
-Pump can be set flush
Check for Residual
-Attach syringe and pull to collect aspirate
-No aspirate is the ideal finding
-Verify facility policy on residual amounts
-Once complete, push contents back in
-Do not aspirate tubes in the small bowel
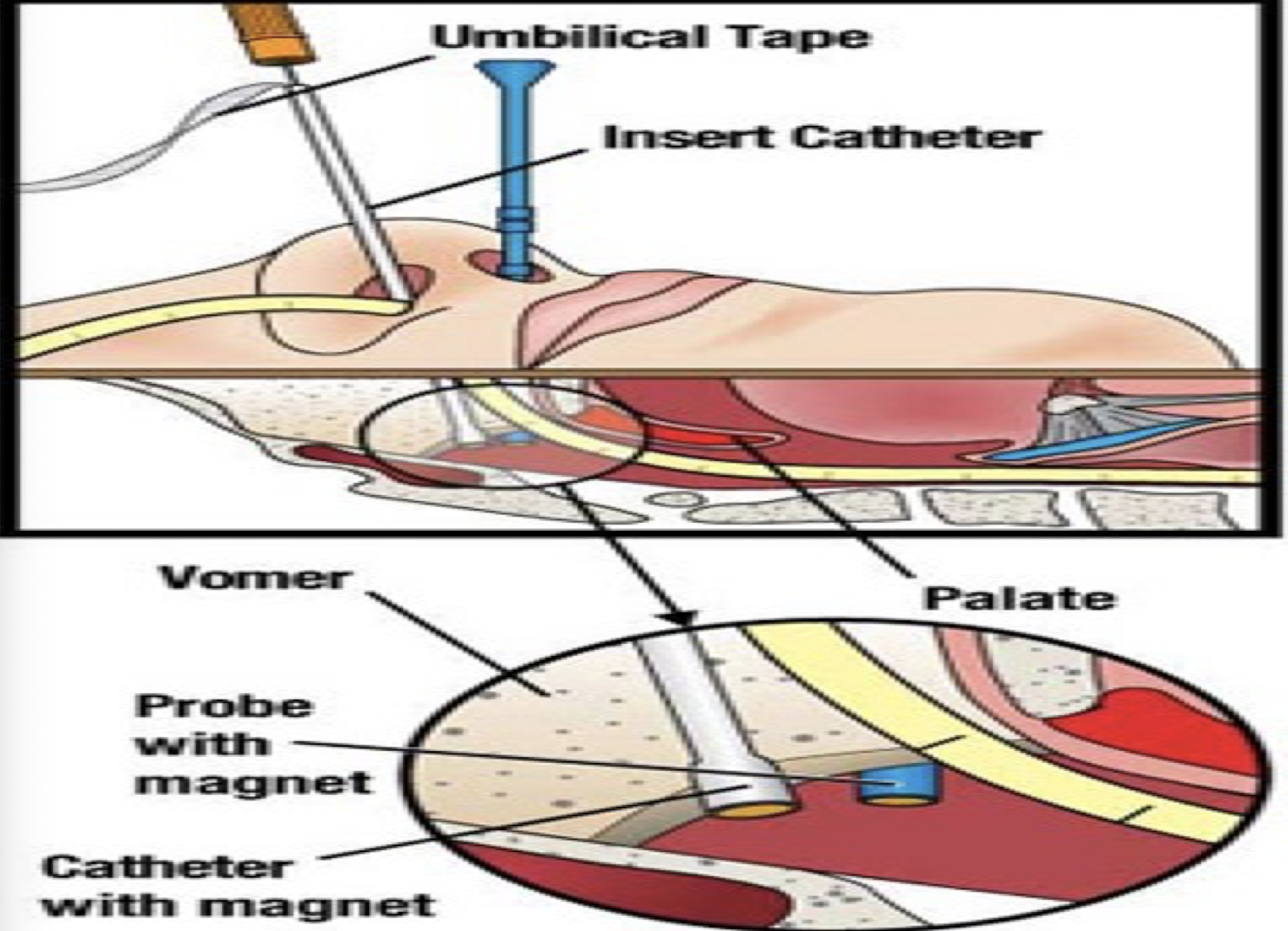
Bridling (Magnetic Anchoring)
-Prevents dislodgment
-Patient supine, tube inserted into nare
-Probe inserted into other nostril (cloth tape attached)
-In nostril with tube, bridle catheter inserted→ the catheter and probe each have a magnet, will hear them click together
-Withdraw probes- just cloth left→ clip two pieces of cloth together on tube and cut off extra
Tube Feeding Complications: Diarrhea (side effect) or constipation, N&V
-Reassess formula rate and composition
-Consider contamination: equipment should be changed daily, more frequently PRN
-Explore alternative causes
-Ensure formula is at room temeprature
Tube Feeding Complications: Fluid and electrolyte imbalance
-Dehydration, fluid overload
-Strict I&O monitoring
-Clinician may order individual water flush protocol
-Ongoing pulmonary assessment
Tube Feeding Complications: Aspiration
-Keep head elevated 30-45 degrees during and for 2 hours after feeding
-HOB up at all times during continuous feeds
-Check placement before each feeding by checking position on nose
-Establish and maintain suction set up at bedside
Tube Feeding Complications: Tube displacement
-Routinely verify tape/bridle is secure
-If removed completely, replace and confirm placement with x-ray before initiating use
-Explain the importance of the tube to the patient’s well-being to discourage self-removal of the tube
<30 days of use
-Nasogastric tube feeding
-Nasojejunal tube feeding
-Salem sump: suction or decompression
> 30 days of use
-PEG tube
-PEJ tube
Placement- is my tube in the correct place to safety administer feeding or medication
-When the tube is inserted, there will be a number in centimeters that is marked and visible
-You should always check that number to make sure it is in the same place
-Tubes do migrate. This can be dangerous
-You need to verify every time you use the tube that the number is the same
-Verify with your facility their correct procedure
Residual- What is my gastric residual volume
This is the amount of contents that remain in the stomach before feeding. There are specific volume amounts disclosed in physician orders with instructions
Patency- Is my tube flowing freely without resistance?
Flushing is required for all tube use. Flush with 30cc tap water before and after use. If giving medications, each med should be crushed in a separate container and diluted with 5-10cc. After med pass complete, finish with 30cc to clear the tube
Additional notes for tube feeding
-No blue food coloring to check for aspiration: may cause organ damage/failure and death (toxic to mitochondria)
-Prefilled bottles can hang for 48 hours
-UPMC recommends tubing changed each time new feeding container hung. Can use same tubing for a second bottle if feeding infuses in <24hrs
Discontinuing an NG tube
-Physician does it most often
-First, assess the abdomen
-Usually removed when bowel sounds are present and flatus
-MD will trial off suction and check contents
-Turn off suction, check tube placement and flush
-Have patient breathe deeply and slowly exhale as tube is quickly removed
-Ongoing oral and nasal hygiene and care
-Measure and record drainage
-Dispose of equipment in biohazard bag