kale nutrition support & infants
1/88
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
89 Terms
male IBW
50kg + 2.3 (inches- 60)
female IBW
45.5kg + 2.3 (inches - 60)
daily water requirement (DWR)
35ml/kg
daily caloric requirement
30kcal/kg/day
daily protein requirement
1.5g/kg/day
1g protein= _______ cals
1g carbs= ________ cals
1 g fat= _______ cals
1g protein= 4 cals
1g carbs= 3.4 cals
1g fat= 9 cals
what does a % solution mean
g/ 100ml
fat yields ____cals/gram
10% lipids= _______ cal/ml
20% lipids= _______ cal/ml
30% lipids= ________ cal/ml
fat yields 9 cals/gram
10% lipids= ___1.1__ cal/ml
20% lipids= __2__ cal/ml
30% lipids= __3___ cal/ml
propofol yields _____cal/ml
1.1
adjusted body weight formula
ABW = IBW + 0.4(actual weight - IBW)
-> to be used if pt weights more than 1.3(IBW)
Males: IBW = 50 kg + 2.3 kg (inches- 60)
Females: IBW = 45.5 kg + 2.3 kg (inches -60)
when is pt actual weight used? IBW? ABW?
actual weight: if less than IBW
IBW: weights btwn IBW and 1.3(IBW)
ABW: if greater than 1.3(IBW)
t/f: a good nutritional assessment would have a positive nitrogen balance
true. more nitrogens in proteins in body than the amount we are losing in urine
which of the following would be the best monitoring parameter to ensure protein repletion (is pt receiving enough)?
a. albumin
b. transferrin
c. prealbumin
d. retinol binding protein
c. prealbumin. at baseline then q week
has short half life= 2days. albumin half life is 18 days- not good immediate indicator.
-transferrin is 8 days, also influenced by iron.
-retinol binding protein has rlly good half life (12hrs) but its more representative of vitA and kidney fxn, not protein
would the following lead to an increase or decrease in water requirement
a. renal impairment
b. cardiac impairment
c. fever
d. GI loss (ex: vomiting)
renal impairment= decrease
cardiac impairment= decrease
fever= increase
GI loss= increase
monitoring parameters for water requirement
- in and out amounts
- mucus membranes
- skin turgor
- weight
monitoring parameters for proper carb nutrition
- glucose
- LFTs to detect fatty infiltration (too many carbs-> converted and stored)
monitoring parameters for proper protein nutrition
- prealbumin: short half life
- BUN
- nitrogen balance
electrolyte requirements:
sum of CALCIUM and PHOSPHATE cannot exceed __________
45meq/L
might cause precipitation
(remember 1mM PO4= 2mEq PO4)
in a 1-liter TPN solution you add 12 mEq of calcium and 15 mmol of phosphate. is this appropriate and why
calcium and phosphate cannot exceed 45meq bc of precipitation
15mmol of phosphate= 30mEq (remember 1mmol PO4= 2meq bc of +2 charge)
12 + 30= 42 so yes thats ok
what can increase the chances of calcium and phosphate precipitating in an electrolyte solution
- increasing the concentrations of either
- increase temp or pH
- using CaCl2 salt form (rather than carbonate)
- mixing Ca before PO4
- decreased amino acids
t/f: mixing phosphate before calcium can increase the chances of precipitation
false. you should always add phosphate first and calcium last when compounding TPN
"phosphate first"
in which pts is folic acid and thiamine TPN supplementation necessary
folic acid= deficiency or pregnancy
thiamine= prevent alcohol induced wernickes encephalopathy (vitamin B1 deficiency)
t/f: basal insulin should be given once a day to maintain a constant amount, and rapid acting insulin should be given in bolus doses 1/2/3x a day along with meals prn
true. mimics body's natural insulin pattern: a constant baseline (basal) + spikes at mealtimes (bolus)
aspart, lispro, glusine:
regular:
NPH:
glargine, detemir
rapid-acting insulins (Aspart, Lispro, Glulisine): Fast onset, short duration; used for meals
regular insulin: Slower onset, moderate duration; used for meals or emergency
NPH: Intermediate duration; used for basal coverage, typically twice daily
long-acting insulins (Glargine, Detemir): Slow onset, no peak; used for basal coverage, typically once daily
what kind of insulin is used in TPNs?
regular insulin used in IV for TPN. this is administered continuously so theres no need to give a long acting insulin
(even if pt usually takes long acting insulin at home, give regular insulin IV in a 1:1 ratio. d/c the subq)
pt AB requires TPN. they usually inject insulin glargine 21 units QHS. how do you adjust this for the TPN
give 21 units of regular insulin IV. d/c subq one while he is receiving this one
sliding scale insulin
-adjusted doses dependent upon individual blood glucose
- pts on TPN are started on SSI and insulin amount is adjusted
what are acceptable blood sugar levels while on TPN? how is insulin adjusted if its above?
<150mg/dL
if above: 2/3 of total SSI needed in 24hrs is added to TPN in the form of REGULAR insulin
(ex: if 9 SSI units were given to combat blood sugar, then 2/3(9)= 6. so you would add 6 units of insulin to the baseline)
pt AB has been started on 10 units regular insulin IV for his TPN. he has had a blood sugar of 132, 164, and 172. the nurse gave 6 units sliding scale. was this appropriate? how should his TPN be adjusted?
yes appropriate. we want blood sugar to be below 150.
we want to add 2/3 of the ssi to his baseline. so 6(2/3)= 4.
we add 4 to the 10 baseline. pt should be on 14 units REGULAR insulin
what is propofol used for
-induction and maintenance of general anesthesia
- sedation in critically ill
how much fat is in propofol and how many calories does it provide
100mg fat per mL
provides 1.1cal/ml
what should be monitored with the use of propofol
- blood pressure (may cause bp drop)
- triglycerides
indications for parenteral nutrition (avoiding gut)
1. cant absorb nutrients via GI
2. severe diarrhea/vomiting, cant eat 7-14days
3. bowel obstruction
4. cancer (malnourishment)
5. severe pancreatitis (>5-7days)
6. unable/cant ingest
7. critical care, burns, organ failure
what are the 2 forms of parenteral nutrition administration
1. peripheral (PPN)= short term, less concentrated, lower infection risk
-> use peripheral vein (arm)
2. total (TPN)= long term, complete nutritional support, higher infection risk
-> central (subclavian vein)
-> peripherally inserted central catheter (PICC)
-> cycle= increases mobility and freedom from pump
PPN indications and CIs
indication:
1. short term: less than 5-7 days
2. pt tolerates large volume of fluids
3. osmolarity of solution <900 mOsm (10%)
CIs:
1. long term (> 7 days)
2. pt is fluid restricted
3. very catabolic, needs high energy
if a severe burn victim requires nutrition for 2 weeks, what would be the best method of implementation
TPN. over 7 days and has high energy requirement
probs has GI dysfunction so EN isnt good option. PPN would have to be <7 days and lower energy requirements
PPN pros and cons
pros:
- less invasive/ easy vein access through standard vein
- lower risk of infection/complications
cons:
- risk of phlebitis
- hard to infuse a lot (<900 msom)
central TPN pros and cons
pros:
- easier to maintain access
- can sustain large nutrient requirements (>900 mosml)
cons:
- expensive, highly trained personnel
- complications, pneumothorax
t/f: a PICC line is an example of a PPN
false. TPN
what metabolic monitoring is necessary with PPN and TPN
- blood sugar q6hrs till stable then qd
- BUN and electrolytes daily
- LFTs at baseline then q2-3 days
- fluid balances every shift
- weight daily
- prealbumin baseline then q week
refeeding syndrome
what is it?
what can happen?
starvation causes loss of PO4 from cells. when you refeed, theres a shift from fat to carbs [within 4 days of refeeding)
cells begin to take in PO4, K+, Mg2+
= hypophosphatemia, hypokalemia, hypomagnesaemia
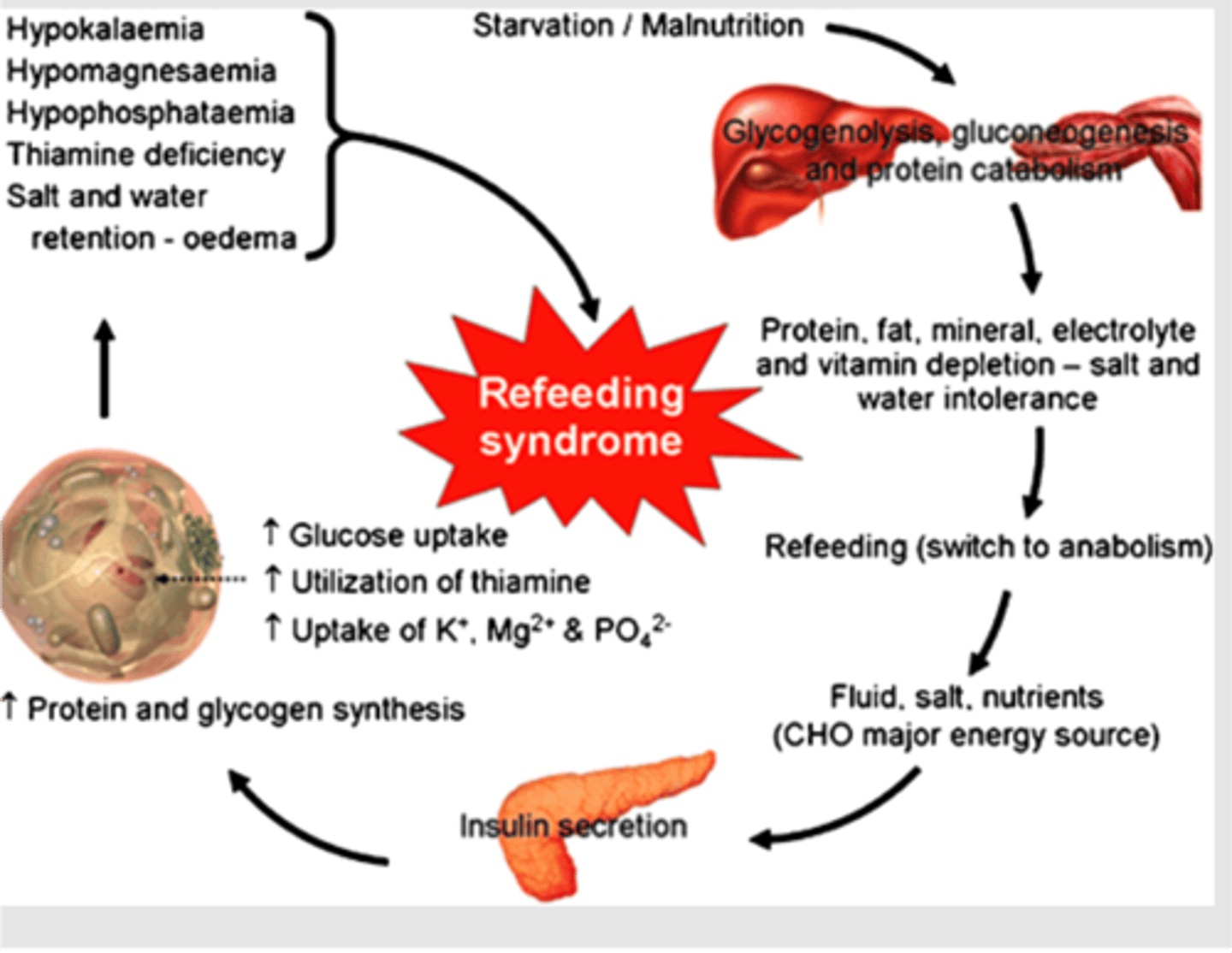
t/f: refeeding syndrome results in hyperphosphatemia and hypermagnesiumia
false. hypophosphatemia, hypokalemia, hypomagnesaemia
indications of enteral nutrition
-GI tract is functional
-inability to consume adequate nutrition orally
ex: anorexia, neck surgery, burns, trauma, IBD, demyelinating diseases
contraindications to enteral nutrition
- intractable vomiting
- intestinal obstruction
- adynamic ileus
- upper GI bleed
- enteric fistula
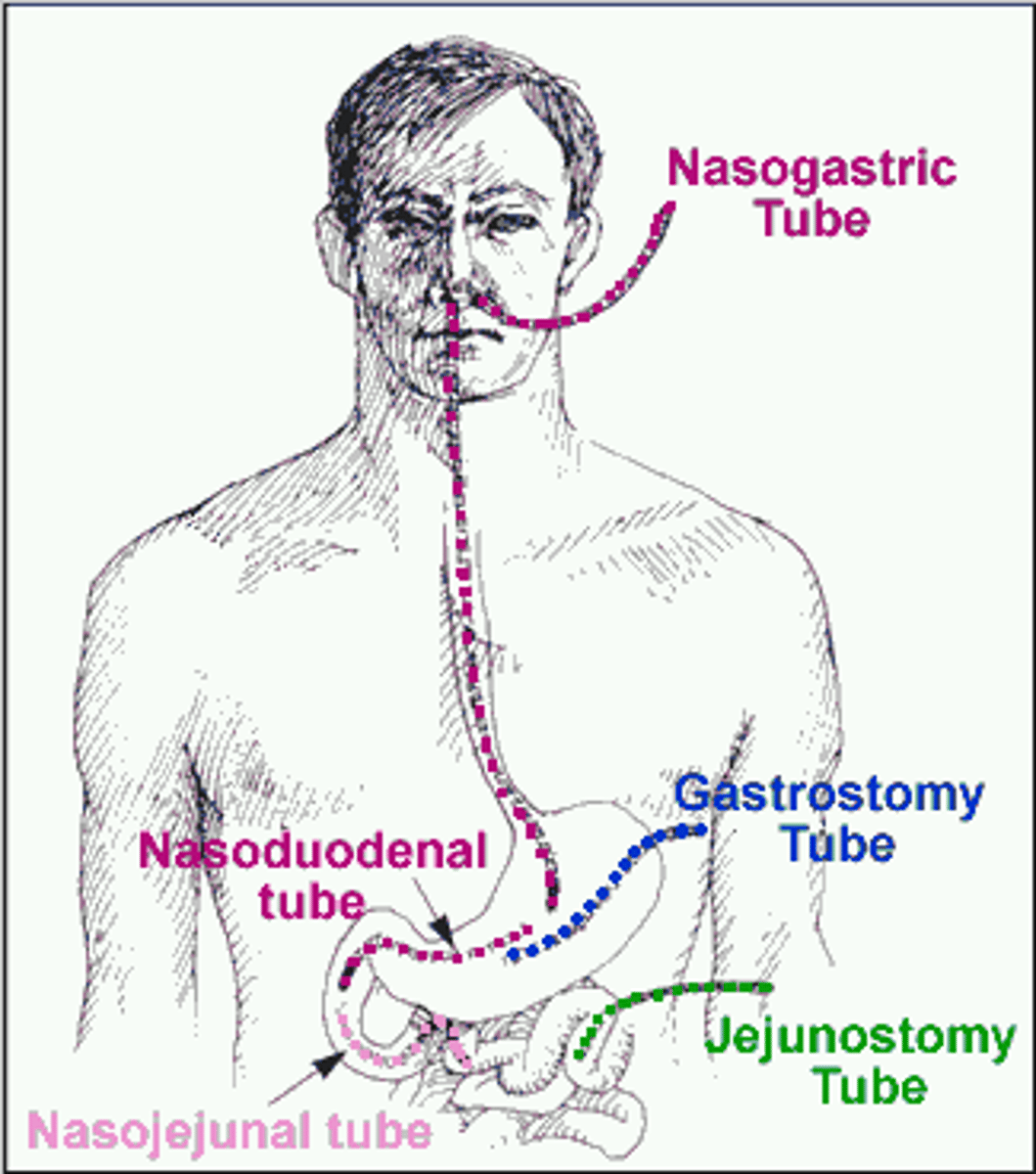
which form of EN nutrition has biggest risk of aspiration
nasogastric
for EN route choice, when is stomach preferred? small intestine? how do you choose?
stomach: well tolerated and can accept high osmotic load! buffers and dilutes it
- BUT: risk of reflux and aspiration (especially nasogastric!)
intestines: preferred in pts with gastroparesis or high aspiration risk
- BUT: tolerates small volumes, and low osmotic load (dumping syndrome!), cramping/distention. harder to place tube
when should you use polymeric carbs/fats/proteins in EN? elemental?
if pt cant digest (ex: pancreatic insufficiency) then give elemental. if they can digest, give polymeric
indications for:
- low osmolality (1cal)
- high density (2cal)
- chemically defined/ elemental (1cal)
- low osmolality: all purpose
- high density: fluids or electrolytes restricted (renal, cardiac)
- chemically defined/ elemental: GI cant absorb or digest
of the following which is NOT nutritionally complete
- low osmolality (1cal)
- high density (2cal)
- chemically defined/ elemental (1cal)
chemically defined- elemental
t/f: EN supplements are usually nutritionally complete and palatable, with a high osmolality
true (ex: ensure)
dumping syndrome
Rapid emptying of gastric contents into small intestines. pt experience ab pain, nausea, vomiting, explosive diarrhea, weakness, dizziness, palpitations & tachycardia.
tube lumen obstruction management
tap water, cranberry juice, coke syrup, adolph's meat tenderizer
what should be done if pt aspirates food during EN feeding
-discontinue feedings
- suction pt
- restart feeding past pylorus
what are the issues with the following meds and EN/TPN
phenytoin(DPH):
warfarin:
fluoroquinolones & tetracycline:
1. phenytoin(DPH): binds to tube. stop feed 1-2hrs pre and post OR give it IV
2. warfarin: know how much VitK in feed and adjust
3. fluoroquinolones (oxacin) and tetracycline: stop feed 1hr before and after
what are the issues with the following meds and EN/TPN
omeprazole/lansoprazole:
antacids:
SR and EC products:
omeprazole/lansoprazole: oral suspension over granules preferred
antacids: those w aluminum pay precipitate protein. give after feeding and flush w water
SR and EC products: DO NOT CRUSH. switch to immediate release
which of the following would be CORRECT monitoring parameters for TPN therapy
a. once daily glucose
b. daily prealbumin
c. weekly fluid balance
d. once daily weight
d. once daily weight= correct
a. once daily glucose= too infrequent
b. daily prealbumin= too frequent. should be once at baseline then every week (half life= 2 days)
c. weekly fluid balance= too infrequent. need to check way more often like q12hrs
d. once daily weight= good
match the following:
child, adolescent, neonate, infant
birth-1 month:
1-12 months:
1-12yrs:
12-18yrs:
birth-1 month: neonate
1-12 months: infant
1-12yrs: child
12-18yrs: adolescent
t/f: neonates and children have higher caloric and water requirements per kg than adults
true
for pediatric nutrition:
for carbs, you initially start with ___% dextrose and increase by ___% as tolerated
10%, 5%
what is the fat initiation for neonates and infants/children?
neonates: 0.5g/kg/day (must not exceed 60% of total cals)
infants/children: 0.5-1g/kg/day (must not exceed 30%)
children <____ should receive pediatric formulation of multivitamin products
11
what can a thiamine (B1) deficiency in children result in
1. wet beriberi: affects cardiovasc system (increases HR, SOB, leg swelling)
2. dry beriberi: affects CNS (numb hands and feet, confusion, lactic acidosis)
what can a B6 (pyridoxine) deficiency result in
seizures
pellagra
the niacin-deficiency disease, characterized by diarrhea, dermatitis, dementia, and eventually death
what is the difference between vitd3 and d2?
function of vitD?
deficiency leads to?
d3= cholecalciferol; synthesized from UV light
d2= ergocalciferol; yeast and plant sterols
fxn= calcium homeostasis, bone mineralization
deficiency=
rickets in children
osteomalacia in adults
zinc fxn=
deficiency=
protein, lipid, carb, bone metabolism
deficiency= skin lesions, alopecia, delayed wound healing, immunosuppression
copper fxn=
deficiency=
fxn= hemopoiesis, bone metabolism, CT metabolism
deficiency= anemia unresponsive to iron, neutropenia, bone changes
chromium fxn=
deficiency=
carb, cholesterol, protein metabolism
deficiency= abnormal glucose tolerance, weight loss, increased serum free fatty acids
manganese fxn=
deficiency=
fxn= amino acid metabolism
deficiency= growth retardation, wound healing
selenium fxn=
deficiency=
antioxidant activation, cardiac fxn, T4->T3 conversion
deficiency= cardiomyopathy, hair and nail loss
iodine fxn
deficiency=
thyroid fxn
deficiency= goiter, weight loss, tachycardia, feeling warm
what is Iron Dextran used for
parenteral formulation for iron deficiency or pts with end stage renal disease on erythropoietin
CI for enteral nutrition in children
1. non function gut/ disruption/ ischemia
2. severe peritonitis
3. shock= systolic <90
monitoring parameters for children
-weight, height, diet
-head circumference (pts <3yo)
-developmental assessment
- psych function
-clinical exam
what does AAP recommend regarding breastfeeding length
- breastfeed exclusively for first 6 months
-12 months or longer encouraged
- especially for premies
advantages of breastfeeding
- probiotic bacteria enhances infant immunity
- reduced diseases seen in infant (asthma, RSV, obesity, etc)
-reduced risk of diabetes, leukemia, SIDS
- promotes neuro development
- has hormones, IGs, enzymes
20cal/30ml avg
what are the 3 infant formula categories
1. Term infant
- standard cow milk
- lactose free
-partially hydrolyzed whey
- follow up
2. Preterm Infant
- human milk fortifiers
- standardized in hospital preterm
- post discharge
3. Specialty formula
- soy
-hydrolyzed
-high MCT
which Term formula is preferred for all infants
preferred= breast milk
appropriate= Cow's milk
what is the difference between cows milk and partially hydrolyzed whey? when is the latter recommended?
cows milk has whole casein and whey, while the partially hydrolyzed formula is more easier to digest. its an alternate for infants that are intolerant to cows milk but will NOT help in cow milk allergy
- may also increase weight gain and reduce atopic conditions
predominant whey protein in cows milk vs human milk
cow= beta lactoglobulin
human= alpha lactalbumin
when is a follow-up formula used
9-24 months
- has higher iron, calcium, and phosphate
t/f: partially hydrolyzed whey formula may be used for infants with a cow milk allergy
false. can be used for intolerance but not allergy
how many calories are in normal human breast milk
20cal/30ml
what are the 3 types of Pre-term formulas available (other than breast milk)
1. Human milk Fortifiers
- add this to human milk to increase calories, protein, calcium, and phosphorus
- expensive
2. In hospital
- high cal, protein, 40-50% MCT
- fortified with vit d, calcium, iron, phosphorus
3. Post discharge
- cheaper than human milk fortifiers
- 22cal/30ml
- 20-25% MCT
- fortified with vit d, calcium, iron, phosphorus
what are the specialty formulas available for infants
1. Soy
- for lactose intolerant infants, vegans
- 30-50% cross sensitivity with CMA!!
2. Hydrolyzed protein/ free AA
- lactose free
-MCT ranges 0-55%
- INDICATED FOR SEVERE CMA
3. high MCT
-80-87%
-INDICATED FOR PANCREATIC, BILIARY, OR SHORT BOWEL SYNDROME
what is MCT and when would a high % be preferred for infants
medium chain triglycerides. they are absorbed directly into portal circulation and dont require pancreatic enzymes.
good for babies with pancreatic, biliary, or short bowel syndrome
which formula would you give the following infant
healthy infant:
infant with CMA:
infant with lactose intolerance:
pre-term baby:
pancreatic/biliary/short bowel syndrome:
healthy infant: breast milk preferred. cows milk appropriate
infant with CMA: hydrolyzed protein/ free amino acid (NOT soy. still cross sensitivity)
infant with lactose intolerance: lactose free, partially hydrolyzed, or soy
pre-term baby: human milk fortifier, in hospital, or post discharge formula with higher cals, protein, MCT
pancreatic/biliary/short bowel syndrome: high MCT
when is vitamin D supplementation indicated for babies getting human milk
if baby is getting <1L per day
when is iron supplementation indicated for baby? not?
indicated= if shows sign of deficiency at a dose of 2mg/kg/day
not=
1. infant is <4-6 months of age
2. infant is eating iron fortified cereal