The Cardiac Cycle and Murmurs NEW exam
1/128
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
129 Terms
What is the cardiac cycle?
The cardiac cycle is the sequence of electrical and mechanical events that occur during one heartbeat.
What are the two main phases of the cardiac cycle?
Diastole: Ventricles relax and fill with blood.
Systole: Ventricles contract and pump blood out.
What is the goal of the cardiac cycle?
To move blood efficiently through the heart and into circulation.
What happens in late diastole?
Contraction causes a rise in pressure in both the left atrium (LA) and left ventricle (LV).
What causes the first heart sound (S1)?
After a short delay, LV pressure exceeds LA pressure, causing the mitral valve (MV) to close — producing S1.
What happens when LV pressure rises above aortic pressure?
The aortic valve (AOV) opens — a silent event in a normal heart.
What causes the second heart sound (S2)?
After contraction, the ventricle relaxes; LV pressure falls below aortic pressure, the AOV closes, producing S2.
What does the Wigger’s Diagram show?
It shows the pressure relationship between the left‑sided heart chambers during the cardiac cycle.
What is the cardiac cycle?
It’s the sequence of electrical and mechanical events responsible for atrial and ventricular contraction.
What happens during systole?
Systole is the phase of ventricular contraction.
What happens during diastole?
Diastole is the phase of ventricular relaxation and filling.
What do the atria do during the cardiac cycle?
They accept blood returning to the heart from the systemic and pulmonary veins, which then passes to the ventricles through the open atrioventricular valves (mitral and tricuspid), increasing diastolic pressure.
What occurs in late diastole?
Atrial contraction pushes the last bolus of blood into each ventricle, raising atrial and ventricular pressures and creating the “a” wave.
When does ventricular contraction occur?
At the onset of systole.
What happens when ventricular pressure exceeds atrial pressure?
The atrioventricular valves close, causing the first heart sound (S1).
When do the semilunar valves open?
When ventricular pressure becomes greater than the pressure in the aorta and pulmonary artery, allowing blood to be ejected from the heart.
What happens when the ventricles relax?
Their pressure drops below that of the aorta and pulmonary artery, causing the semilunar valves to close and producing the second heart sound (S2).
What are the components of the second heart sound (S2)?
Aortic component (A2) — usually heard first
Pulmonic component (P2)
What happens when ventricular pressure falls below atrial pressure?
Atrial pressure rises, opening the atrioventricular valves and starting the cardiac cycle again.
What is the “a” wave in the cardiac cycle?
It represents the atrial kick in late diastole — the last push of blood through the valve.
What is the “c” wave in the cardiac cycle?
It occurs as the mitral (MV) and tricuspid (TV) valves close and bulge into their respective atria.
What is the “v” wave in the cardiac cycle?
It results from passive filling of the atria during systole. In the right heart, this is visualized by jugular venous pulsations representing right atrial pressure.
What are the heart sounds?
S1, S2, S3, S4, A2, P2
What is S1?
The first heart sound (“Lud”), Closure of the mitral and tricuspid valves → Start of systole (In early systole.).
Where is S1 loudest?
Near the apex of the heart.
What factors determine the intensity of S1?
The distance separating the valve leaflets at the onset of ventricular contraction.
The mobility of the mitral (MV) and tricuspid (TV) valve leaflets (may be reduced if stenotic).
Why might the mobility of the MV and TV leaflets affect S1 intensity?
If the valve leaflets are stiff or stenotic they close weakly and make S1 softer, but if they are wide apart and mobile they shut forcefully and make S1 louder.
When is S1 accentuated (louder)?
When the PR interval is shorter than normal.
What condition makes S1 louder due to wide‑open valve leaflets?
Mild mitral stenosis (MS), because the leaflets are wide apart and shut forcefully.
In what condition is S1 accentuated (louder)?
High cardiac output states or tachycardia (e.g., exercise) cause an accentuated S1.
What conditions cause a diminished (soft) S1?
Lengthened PR interval (first‑degree AV nodal block)
Mitral regurgitation
Severe mitral stenosis
“Stiff” left ventricle (e.g., left ventricular hypertrophy due to systemic hypertension)
Why does a “stiff” left ventricle make S1 softer?
Because reduced ventricular compliance limits leaflet movement, causing less forceful valve closure and a softer S1.
What is S2?
The second heart sound (“Dub”), Closure of the aortic and pulmonic valves → End of systole (end of ventricular systole.)
How does S2 vary with respiration?
One sound during expiration.
What happens to S2 during inspiration?
It splits into two sounds, called physiologic splitting.
What are the components of S2?
A2 and P2.
What does each S2 component represent?
A2: Closure of the aortic valve
P2: Closure of the pulmonic valve
What happens to A2 and P2 during inspiration?
A2 occurs earlier.
P2 is delayed, causing the split.
What conditions diminish the sound of S2?
Severe aortic stenosis or pulmonic stenosis, where the valve cusps don’t move well, making closure sounds softer.
What happens to S2 during expiration?
A2 and P2 fuse into one sound.
What happens to S2 during inspiration?
A2 and P2 separate, creating physiologic splitting.
What conditions cause widened splitting of S2?
Right bundle branch block (RBBB) and pulmonary stenosis.
Why do RBBB and pulmonary stenosis cause widened S2 splitting?
They delay P2, making the A2–P2 split wider.
What causes widened splitting of S2 in pulmonic valve?
It’s the result of delayed closure of the pulmonic valve.
What is fixed splitting of S2 and what causes it?
Widened but persists unchanged through the respiratory cycle due to unchanged pressures from a left‑to‑right atrial shunt. Condition: Atrial septal defect (ASD).
What is fixed splitting of S2?
Atrial septal defect (ASD).
What is paradoxical splitting of S2?
P2 occurs before A2 (reversed order).
When is paradoxical splitting of S2 heard?
The split is heard in expiration and disappears with inspiration.
What causes paradoxical splitting of S2?
Advanced aortic stenosis or left bundle branch block (LBBB).
What is S3?
Caused by rapid ventricular filling → Early diastole.
What is S4?
Caused by atrial contraction → Late diastole.
What are early extra systolic heart sounds?
Clicks after S1 indicating aortic or pulmonic valve stenosis or dilatation of the pulmonary artery or aorta.
What causes early systolic clicks in aortic or pulmonic stenosis?
The valve reaches its elastic limit and abruptly decelerates, producing the click sound.
How does an aortic ejection click sound?
Heard at the base and apex and does NOT change with respiration.
How does a pulmonic ejection click sound?
Heard at the base and intensity decreases with inspiration.
What are mid or late systolic heart sounds?
Clicks during mid to late systole caused by mitral or tricuspid valve prolapse, often with valvular regurgitation.
What are extra diastolic heart sounds?
Additional sounds heard after S2 during diastole, including opening snap (OS), S3, S4, summation gallop, and pericardial knock.
What is an opening snap (OS)?
A snap heard when the mitral or tricuspid valve opens in stenosis; otherwise diastole is silent.
When does S3 (ventricular gallop) occur?
During rapid ventricular filling.
What causes the S3 sound?
Vibration of ventricular walls as blood rushes in.
In whom is S3 considered normal?
Young adults, athletes, and children.
When is S3 abnormal and what does it indicate?
In adults, it indicates dilated ventricle, heart failure, or increased valvular flow from Mitral regurgitation or Tricuspid regurgitation.
When does S4 (atrial gallop) occur?
During atrial contraction in late diastole.
What causes the S4 sound?
Blood being forced into a stiff or non‑compliant ventricle.
What conditions commonly produce an S4?
Hypertension, ventricular hypertrophy, and ischemic heart disease.
What happens when both S3 and S4 are present?
The patient has S3 and S4 in conjunction with S1 and S2, producing a quadruple beat.
What is a summation gallop?
When a patient with S3 and S4 develops an increased heart rate, the two sounds merge into one, forming a summation gallop.
When does a pericardial knock occur?
In early diastole.
What causes a pericardial knock?
Abrupt cessation of ventricular filling when the ventricle wall meets a rigid pericardium.
What condition is associated with a pericardial knock?
Constrictive pericarditis.
What causes a murmur?
A murmur occurs when blood flow becomes turbulent instead of smooth.
What is one etiology of a murmur involving a narrowed valve?
Flow across a narrowed valve such as aortic stenosis (AS).
What causes murmurs from increased flow through normal structures?
Pregnancy or anemia.
What causes murmurs from ejection into a dilated chamber?
Aortic systolic murmur associated with an aortic aneurysm.
What causes murmurs from regurgitant flow across a leaky valve?
Mitral regurgitation (MR) and tricuspid regurgitation (TR).
What causes murmurs from abnormal shunting of blood between chambers?
Ventricular septal defect (VSD) — blood flows between chambers where it should not.
How are murmurs categorized?
By timing, pitch, intensity, shape, location, radiation, and response to maneuvers.
What does “timing” refer to when categorizing murmurs?
Whether the murmur occurs during systole or diastole.
Continuous murmurs begin in systole and continue through diastole.
What does “pitch” describe in murmurs?
The frequency of the murmur, ranging from high to low.
What causes a high‑frequency murmur?
A large pressure difference between chambers, as in aortic stenosis.
What causes a low‑frequency murmur?
A smaller pressure difference between chambers, as in mitral stenosis.
What does “intensity” describe in murmurs?
The loudness of the murmur, graded separately for systolic and diastolic murmurs.
How are systolic murmurs graded by intensity?
Systolic murmurs are 1-6 (1 is barely audible and 6 is without stethoscope on chest)
How are diastolic murmurs graded by intensity?
Diastolic murmurs are 1-4 (1 is barely audible and 4 is very loud)
What does “shape” describe in murmurs?
How a murmur changes in intensity over time.
What is a crescendo‑decrescendo (diamond‑shaped) murmur?
A murmur that rises and then falls in intensity.
What is a decrescendo murmur?
A murmur that begins at maximum intensity and then becomes softer.
What is a uniform murmur?
A murmur with no change in intensity over time.
Where is the aortic area located for auscultation?
Right upper sternal border.
Where is the pulmonic area located for auscultation?
Left upper sternal border.
Where is the tricuspid area located for auscultation?
Lower sternal border.
Where is the mitral area located for auscultation?
Apex of the heart.
What does “radiate” mean when describing murmurs?
It refers to the direction the sound travels.
What are common bedside maneuvers used to assess murmurs?
Standing, Valsalva, and clenching fists — each affects murmur intensity and helps identify its origin.
Give an example of a detailed murmur report.
Grade III/VI high‑pitched, crescendo‑decrescendo systolic murmur, loudest at the upper right sternal border with radiation toward the neck.
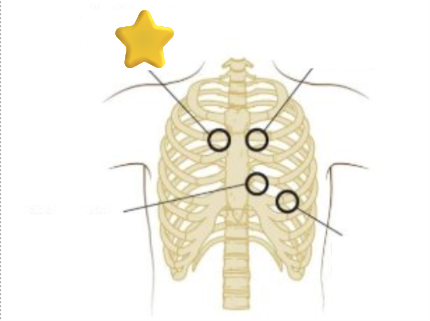
What is this?
Aortic area (2nd-3rd right interspace)
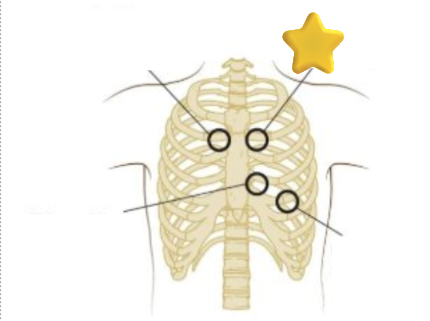
What is this?
Pulmonic area (2nd-3rd left interspace)
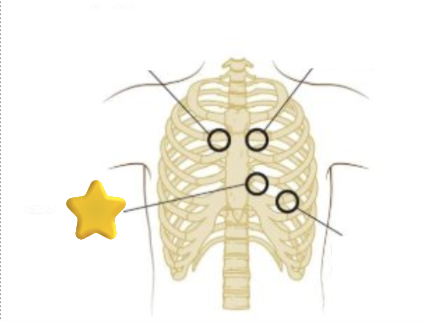
What is this?
Tricuspid area (left lower sternal border)
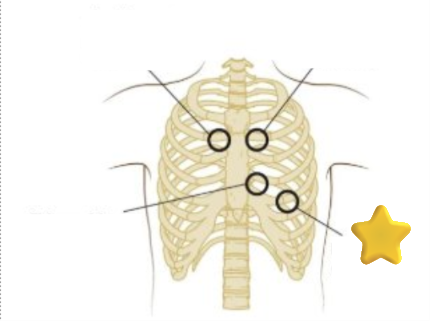
What is this?
Mitral area (apex)
What are the three types of systolic murmurs?
Ejection type, pansystolic (holosystolic), and late systolic.