CM II Week 8 (Orthopedic Back Pain)
1/90
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
91 Terms
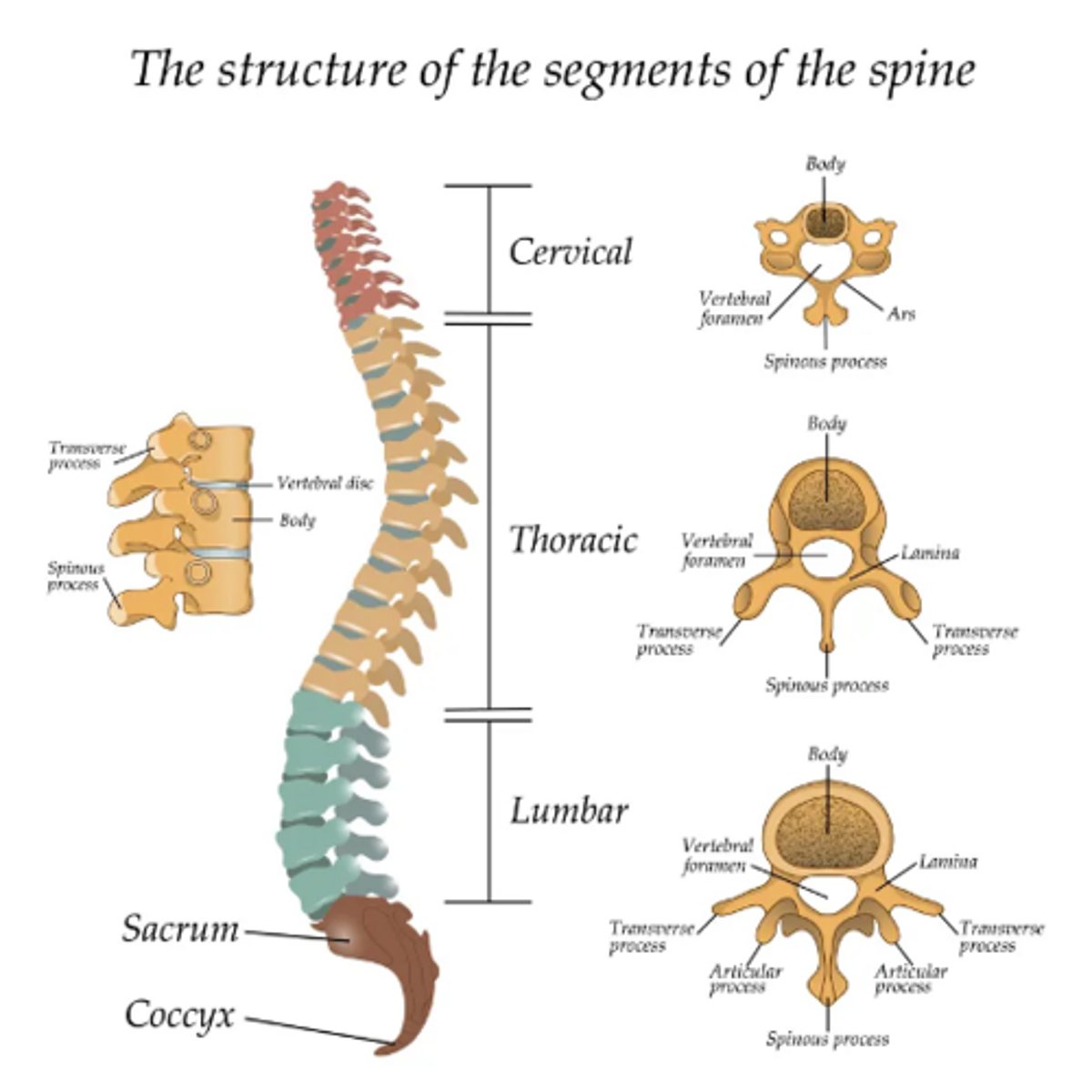
spine anatomy review
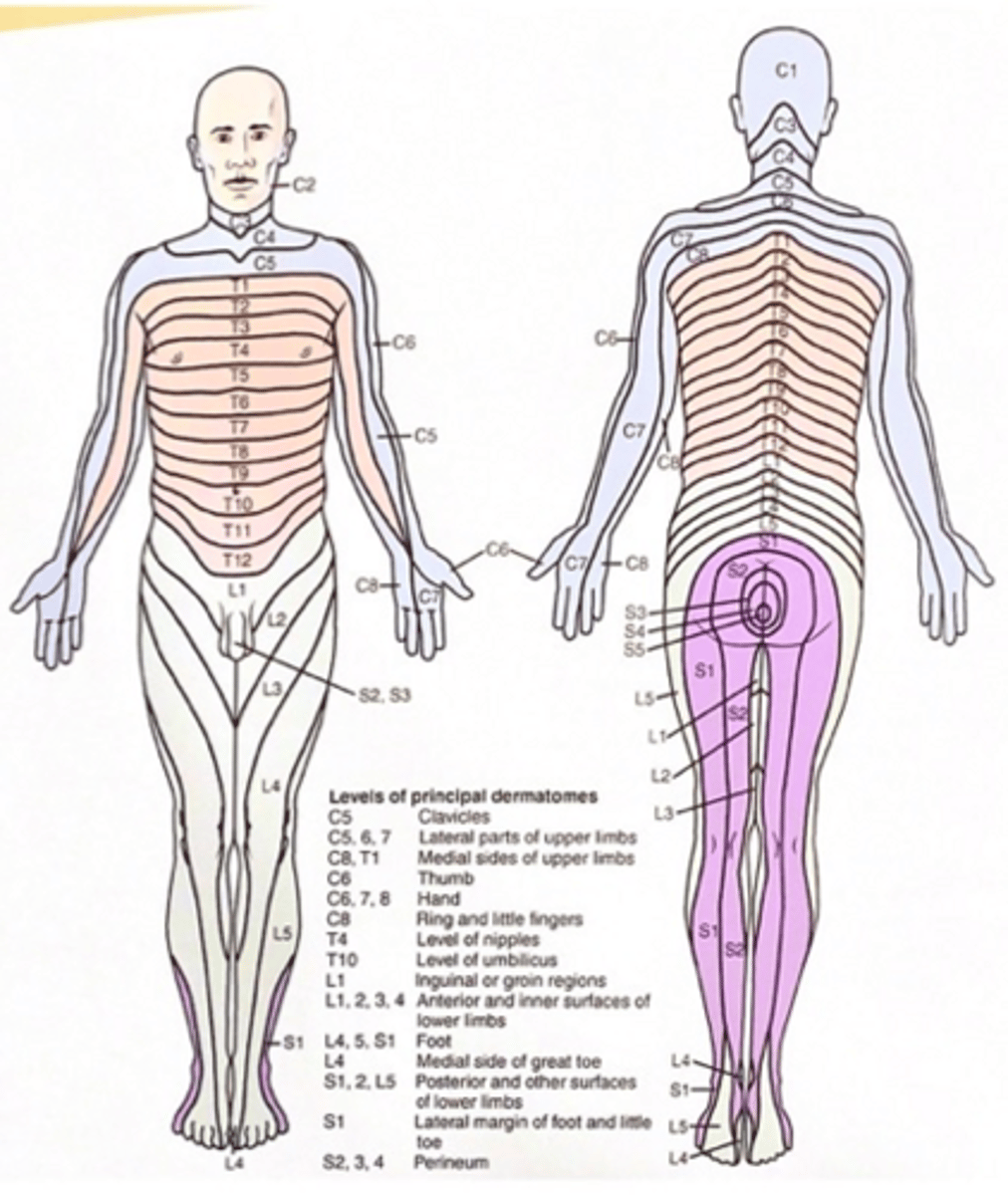
dermatome picture
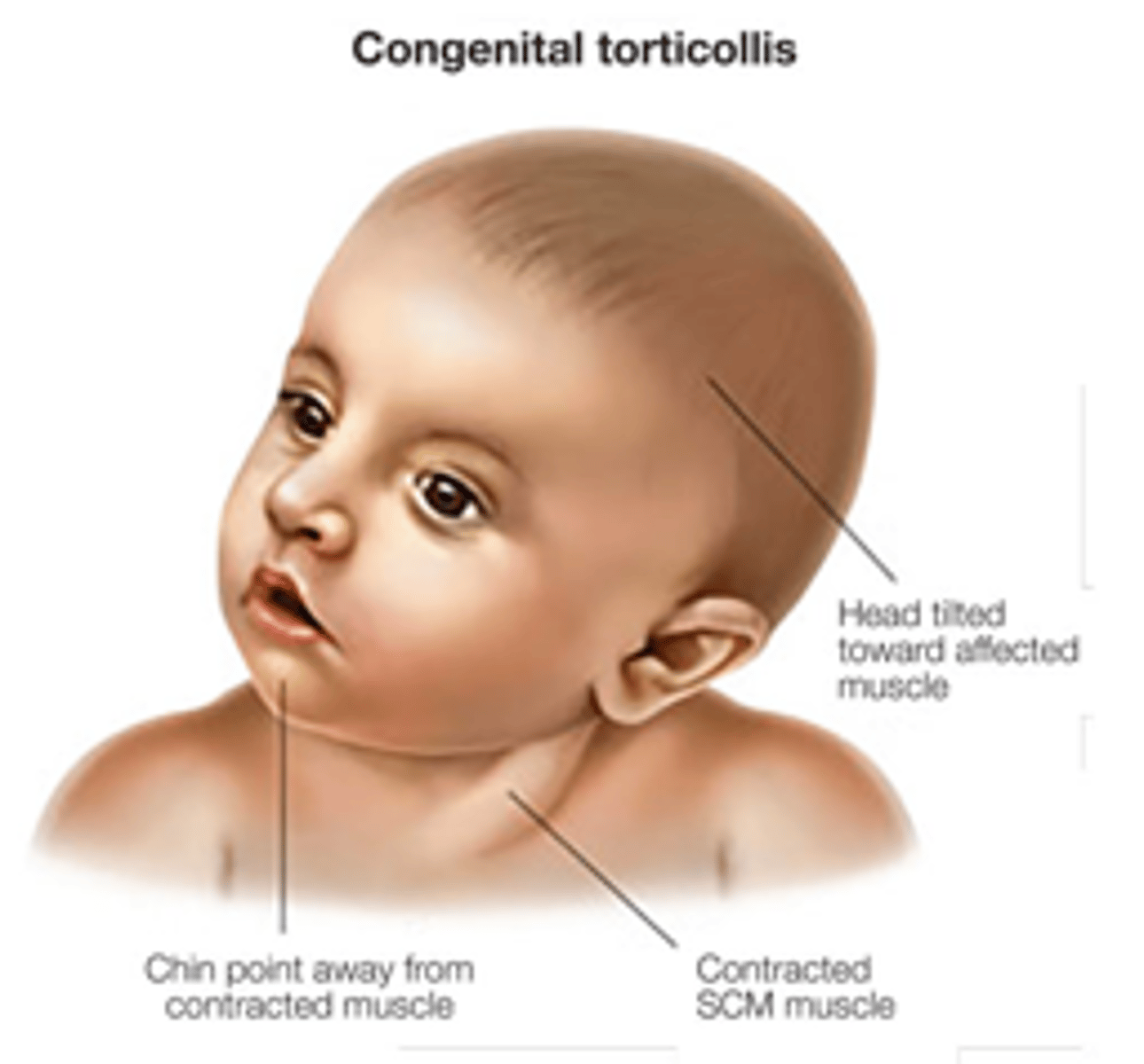
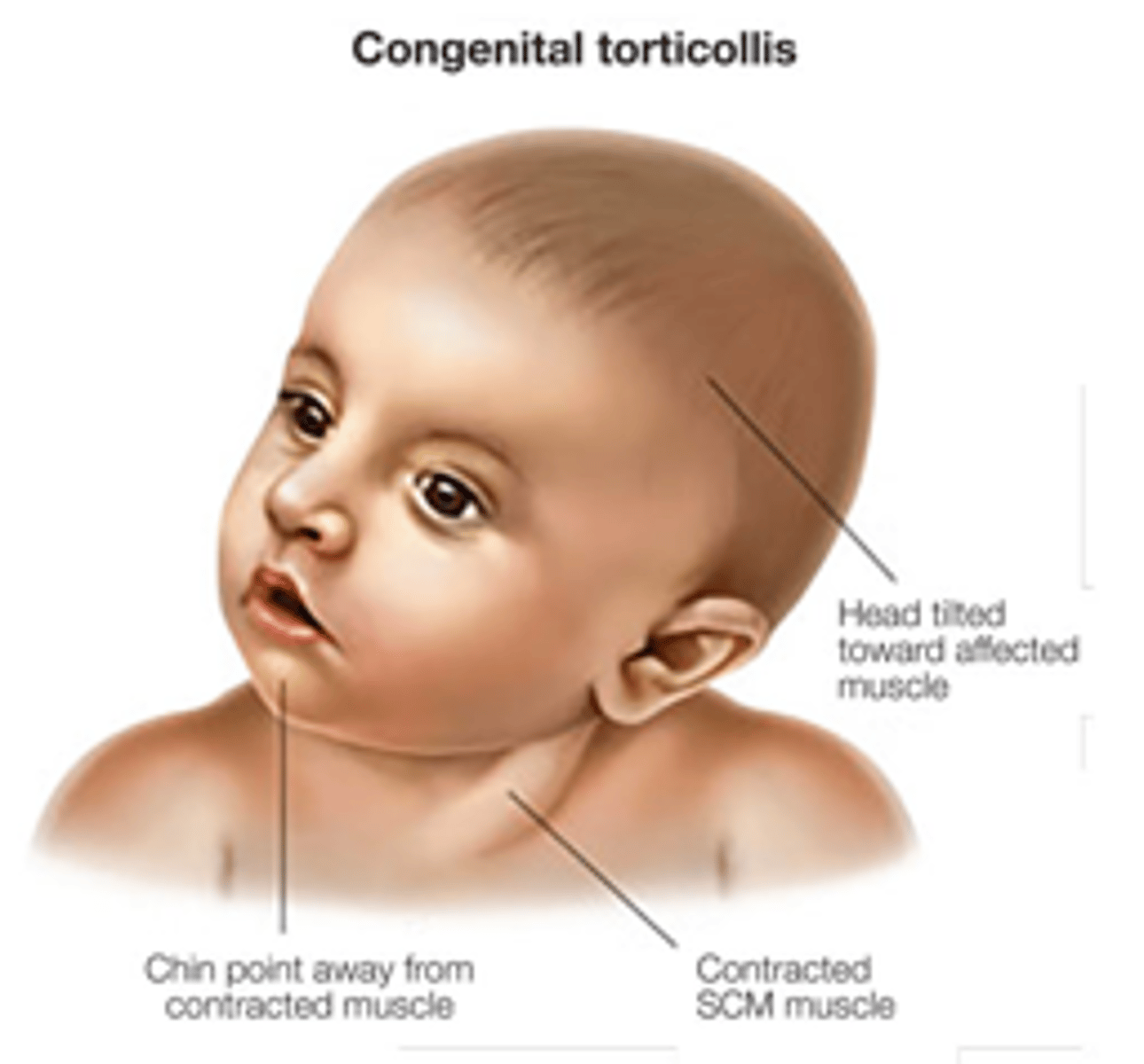
Torticollis is caused by
abnormal contraction of SCM (head tilted to side of involvement)
Torticollis epi/RF
•More common in Males 3:2
•Common in infants and children
•Risk Factors: oligohydramnios, first pregnancy, traumatic delivery, breech delivery
Torticollis History
•Parents stating child only looking towards one side
•Difficulty turning head when cued
•Upset with tummy time
Torticollis PE
•Inspection: visible contraction of the SCM muscle, neck tilt toward effect side and chin rotated away from effected side
•Palpable neck mass along SCM
•Older children will have a tight band at the SCM resulting in rotation and lateral bending restriction
Imaging for torticollis
•X-ray: cervical spine films. Rule out bony pathology.
•CT: Rule out atlantoaxial (C1-C2) instability
•Ultrasound: Helpful to differentiate congenital muscular torticollis vs. neurologic abnormalities
Conservative tx for torticollis
Passive stretching within the first year of sx
when to initiate surgical tx for torticollis? what is surgery?
•Failed conservative management with at least 1 year of stretching
•Release of SCM or Z-lengthening
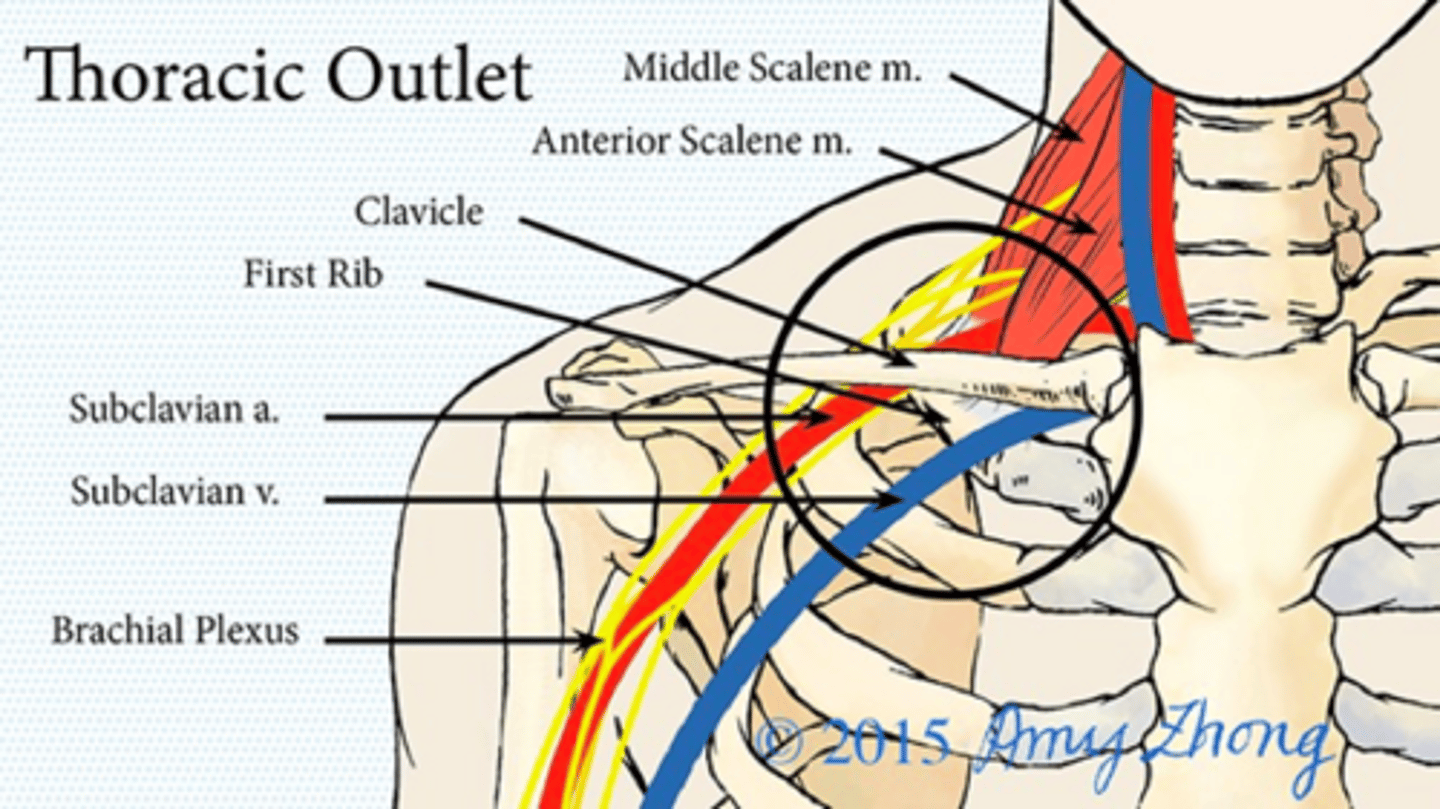
Thoracic Outlet Syndrome
•Compression of the neurovascular structures of the brachial plexus and/or subclavian vessels between the neck and axilla
•Neurogenic is most common (95%)
Thoracic Outlet Syndrome epi
•More common in females 3:1
•Thin, long neck, and drooping shoulders
Thoracic Outlet Syndrome hx
•Pain, weakness, numbness and paresthesias over the trapezius, neck, chest, shoulder and/or arm
•Intermittent discoloration and swelling of the upper limb (venous involvement)
•Raynaud-type symptoms: coolness, pallor, erythema, symptoms associated with temperature change (arterial involvement)
Thoracic Outlet Syndrome PE
• sposture that may increase load on brachial plexus
• skin, hair and nail changes.
• muscle atrophy
• pain or palpable mass over the supraclavicular region
*special tests have high false positive rates*
Imaging needed for Thoracic Outlet Syndrome
X-ray
CT
MRI - soft tissue
EMG
Doppler US
what are you looking for on X-ray in thoracic outlet syndrome
chest/cervical spine films
prominent C7 transverse process or low hanging shoulder girdle
what are you looking for on CT in thoracic outlet syndrome
space occupying lesion
malunion of clavicle/rib fracture
What test can be used in thoracic outlet syndrome to detect neurogenic compromise?
EMG
What is used in thoracic outlet syndrome to detect obstruction such as emboli & thrombus?
Doppler US
Evaluate obstruction, embolic and thrombosis of venous or arterial structures
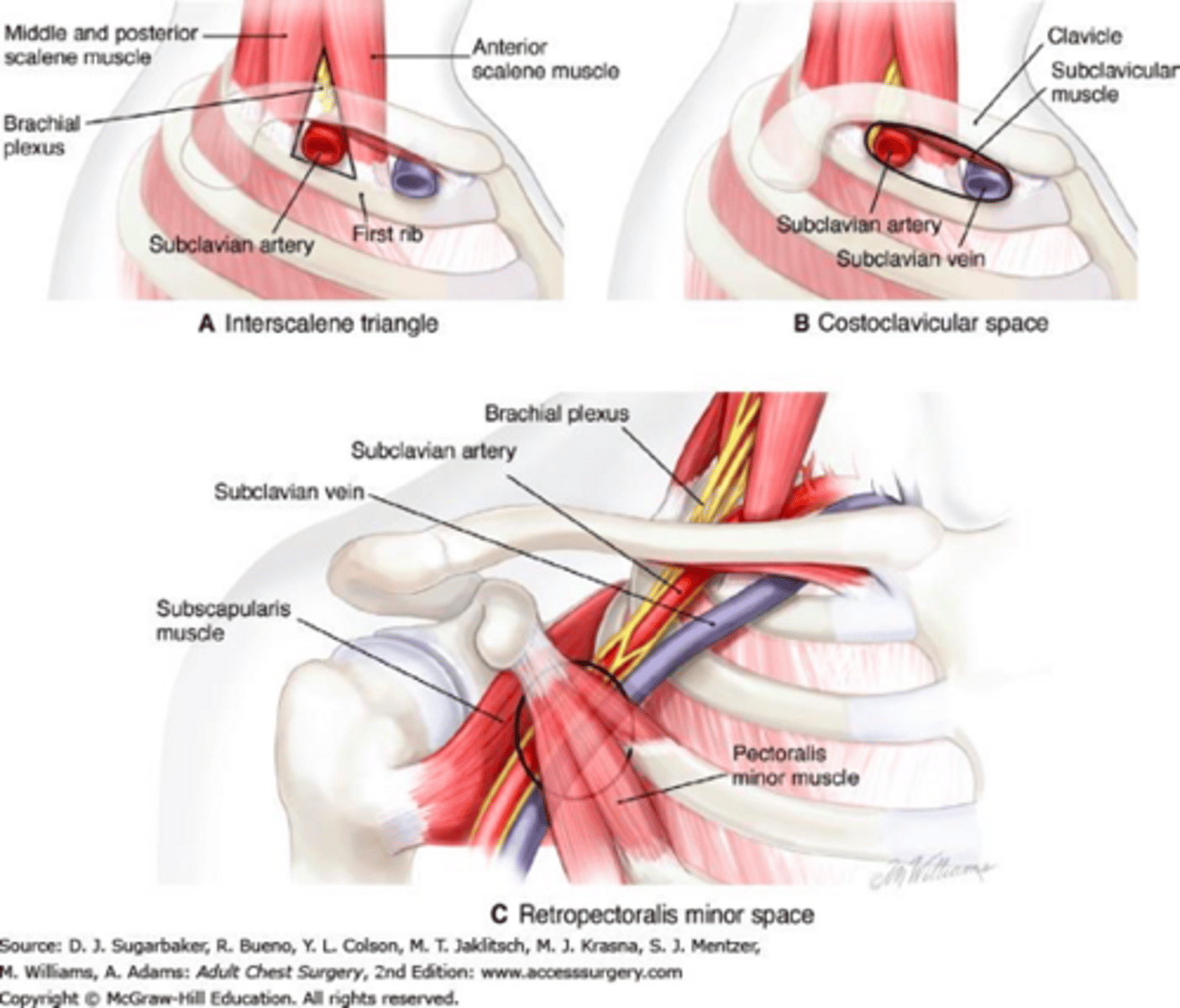
Thoracic Outlet Syndrome: Special Test
Supraclavicular pressure test: Compression at the interscalene triangle
https://youtu.be/ZRKPVtlN59k
Adson test: Compression at the interscalene triangle
https://youtu.be/BnwwvuSagIU
Costoclavicular maneuver: Compression at the costoclavicular space
https://youtu.be/XEWO_cFy5YI
Wright test: Compression at the retropectoralis minor space
https://youtu.be/e-6AiDPyd2Q
Roos test: Evaluates the entire thoracic outlet
https://youtu.be/0oGGdcQsBKY
Cyriax release test: evaluates the result of unloading the brachial plexus
https://youtu.be/kX1mUhyjZwk
NOTE: Special test have a high rate of false positives!
Conservative Treatment for Thoracic Outlet
NSAIDs, muscle relaxers, limiting over head ROM
PT: back, shoulder girdle and core strengthening
Anterior scalene blocks: US-guided lidocaine or Botox injections
Surgical management of thoracic outlet
Thoracic outlet decompression if conservative treatment failed for 6 months
Treat any vascular event appropriately (stenosis, aneurysm, thrombosis/ischemia, embolism)
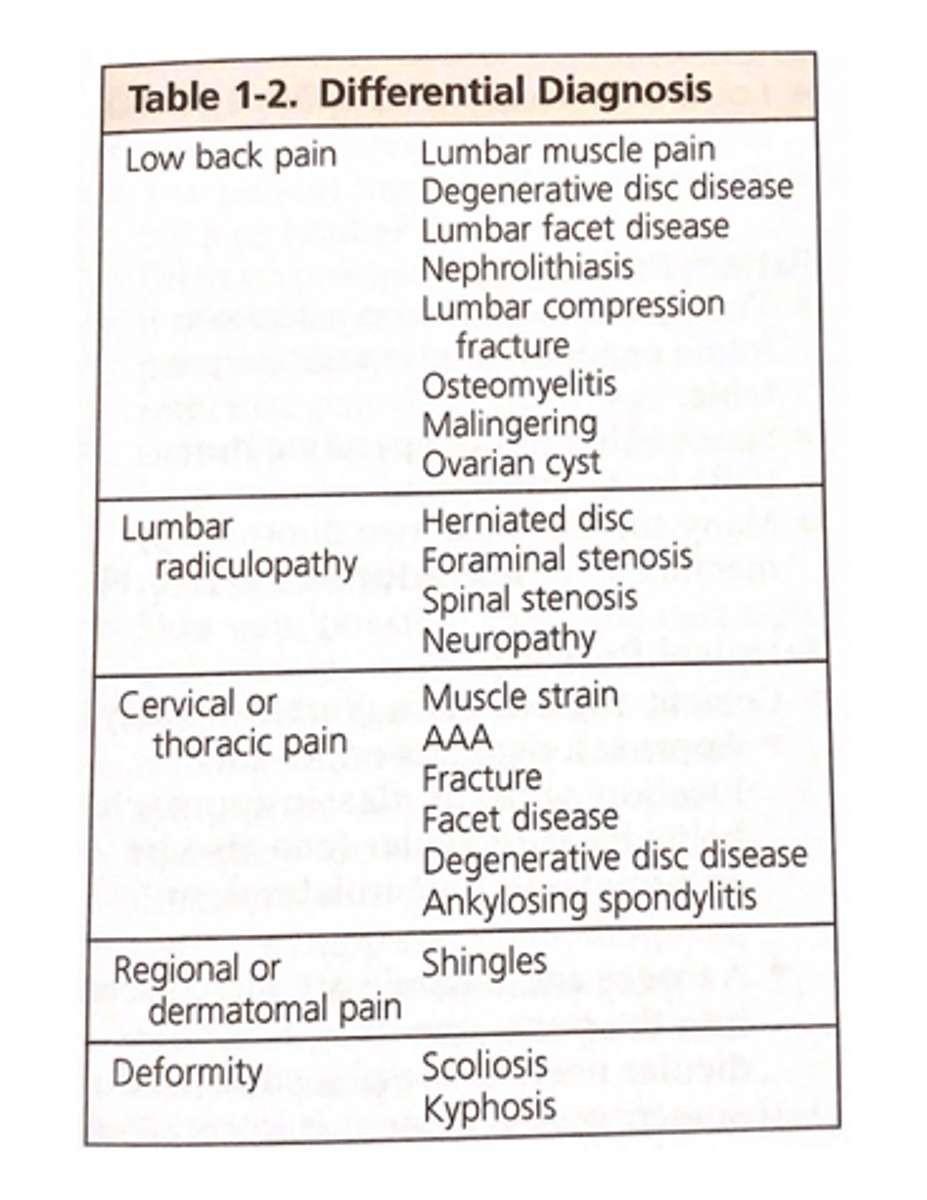
Most common cause of lower back pain? RF?
Muscle strain
•Risk factors: obesity, smoking, gender, heavy lifting, vibration, prolonged sitting, poor posture
•90% of low back pain resolves w/in one year
low back pain hx considerations
•Mechanism of injury
•Location and description of pain
•Radiating pain
•Severity and duration of pain
•Time of day
•Neurological symptoms
•Aggregating and relieving factors
•PMH: Cancer, herniated disc, OA, RA, trauma
•Social history: Stress, IVDA, work, domestic issues
low back pain PE
•General: weight, temperature, posture
•Inspect: muscle spasm, lumbar lordosis or kyphosis
•Gait: normal, limp, walking on heels or toes
•Palpate: paraspinal/paravertebral muscles, local tenderness, trigger points, spinous process/step offs, sacroiliac joints
•ROM: forward flexion, extension, lateral bending, rotation
•Neurological: nerve root compression tests, reflexes, sensory, muscle strength
•Consider rectal, pelvic, abdominal or breast with suspicious history
imaging for lower back pain
x-ray
mri
low back pain red flags (summary)
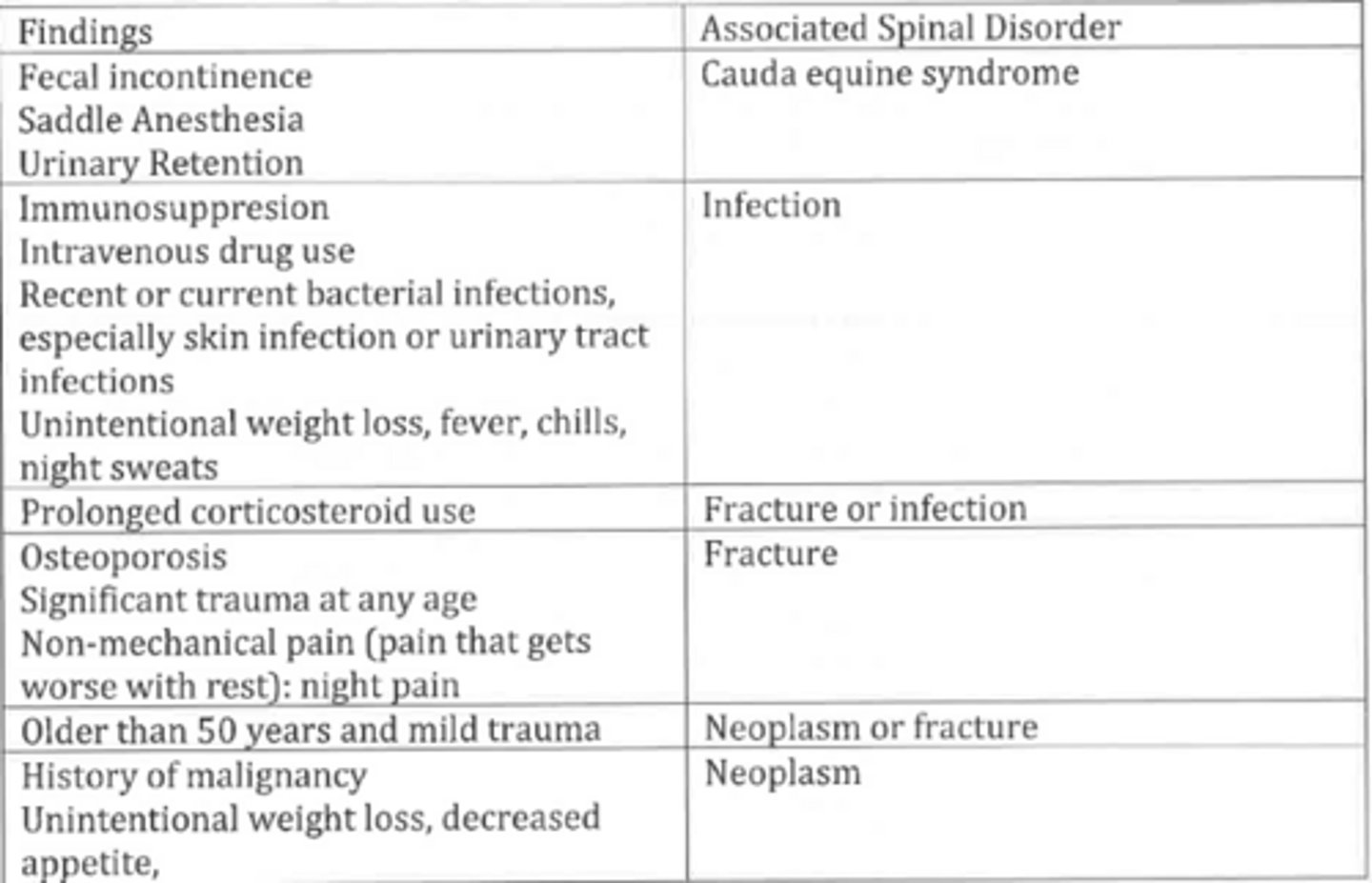
Pt presents with:
- fecal incontinence
- loss of sensation in "saddle" area
- urinary retention
What are you concerned about?
Cauda equina syndrome
Cauda Equina Syndrome
•Lumbar compression of the nerve root in the thecal sac
•Commonly caused by an acute lumbar disc herniation
Cauda Equina Syndrome epi/location
•More common in males
•Commonly occurs at L4-L5
Cauda Equina Syndrome Hx
•Back pain with heavy lifting with lumbar spine flexed
•Unilateral/bilateral leg pain
•Saddle anesthesia
•Bladder/bowel dysfunction
PE of cauda equina syndrome
•Unilateral/bilateral lower extremity weakness
•Decreased rectal tone on voluntary contraction
•Decreased/no sensation to sharp touch in the perianal region (S2-S4 dermatomes)
•Decreased/absent lower extremity reflexes
Gold standard imaging of cauda equina?
other?
Urgent MRI: Gold Standard. Central disc herniation with complete spinal canal compromise
You suspect cauda equina syndrome, but pt has cardiac pacemaker (CI for MRI). What imaging can you perform?
CT myelography
Treatment of cauda equina
surgical decompression within 24 hours!
No later than 48 hours... an emergency, delays in dx and tx lead to permanent impairment!
Define lumbosacral sprain
•Acute or chronic muscle tendon or ligamentous strain
•Most common cause of lower back pain
PE of lumbosacral sprain
•Slow/antalgic gait
•Tenderness to palpation over muscular structures
•Pain with lumbar ROM: flexion, extension, ipsilateral bend or rotation
•Normal neurologic exam
back pain that worsens with bending, twisting, and lifting, coughing or sneezing is indicative of
lumbosacral strain
hx may include +/- pain radiating down legs but does not pass the knees
Lumbosacral Strain Imaging
Xray: rule out degenerative cause of lower back pain.
Normal if lumbosacral strain is the primary cause
treatment of lumbosacral strain
•1-2 days of bed rest for severe pain
•NSAIDs/Acetaminophen
•+/- Muscle relaxers
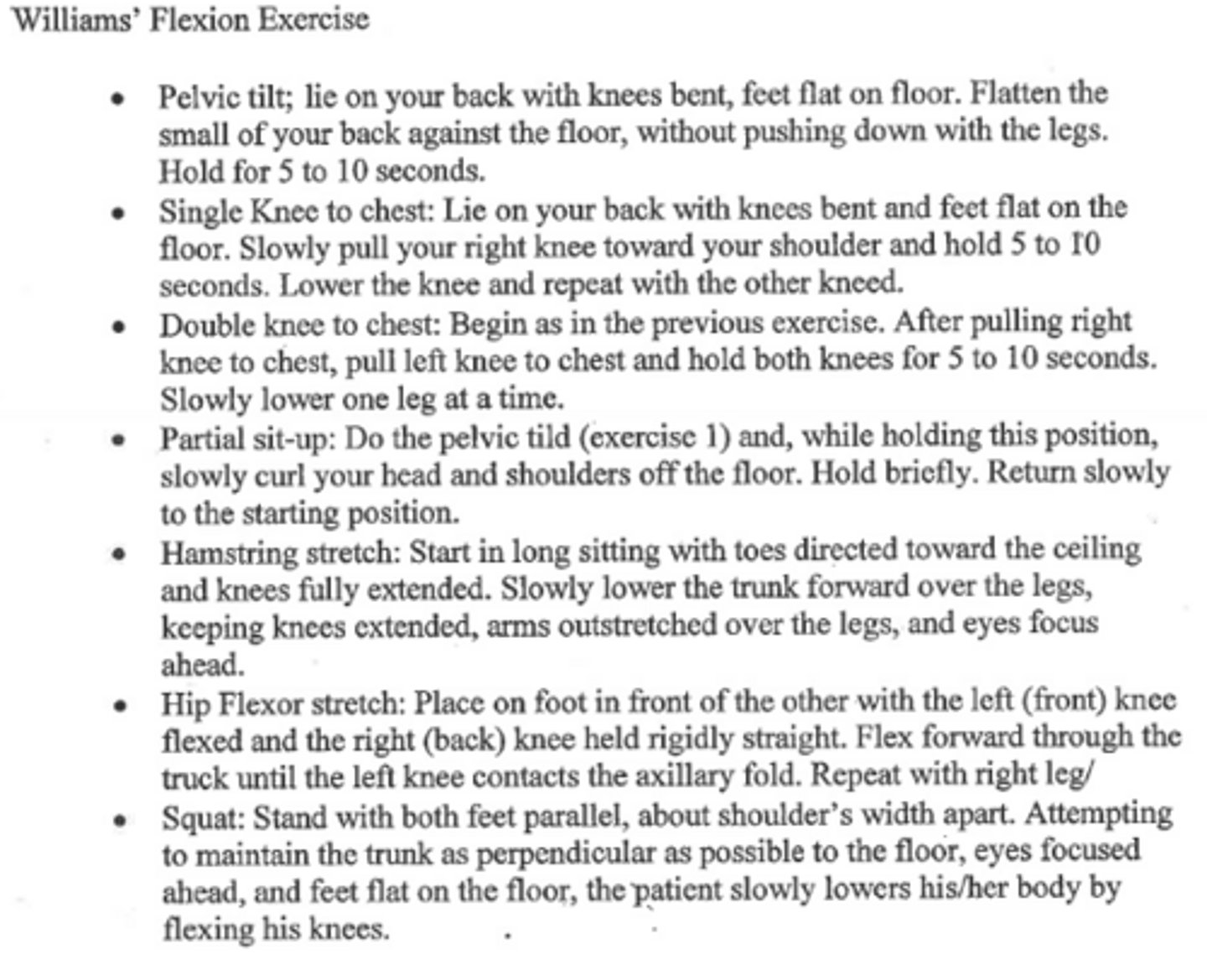
•Physical therapy (Williams Flexion Exercise)
NO Narcotics!
Willams Flexion Exercise
Set of physical exercises that help to improve:
1. Lumbar flexion
2. Avoid lumbar extension
3. Strengthen abdominal and gluteal muscles
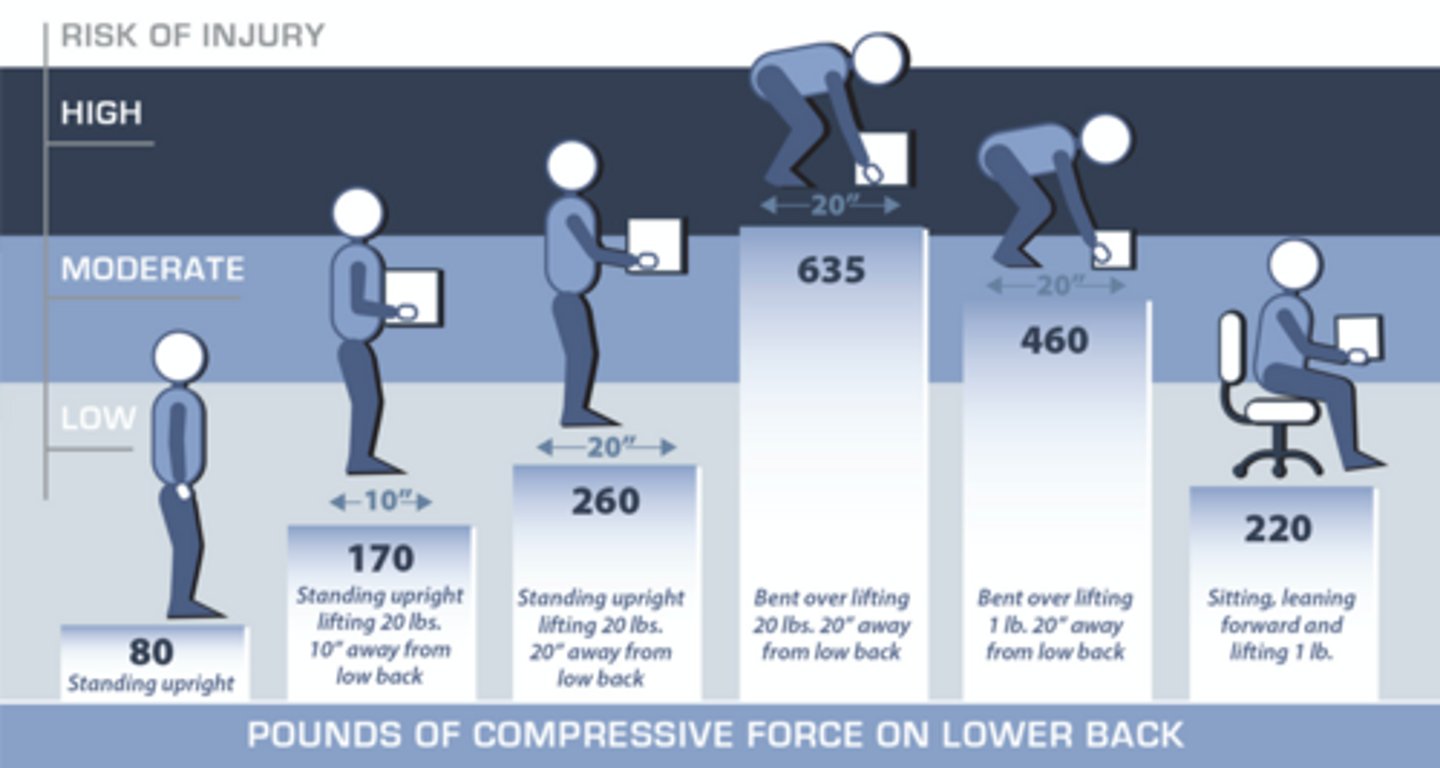
lifting techniques...
lift with your legs not your back
Positive Waddell Signs may indicate...
psychological cause of back pain (possible malingering)
these are test to assess for nonorganic lower back pain
What are the Waddell Signs
1. Tenderness that is not anatomic (superficial/diffuse)
2. Axial loading (should not cause low back pain)
3. Distraction on straight leg raise while in seated position
4. Nonanatomic or breakaway weakness that do not follow neuroanatomy
5. Overreaction (most important Waddell sign)
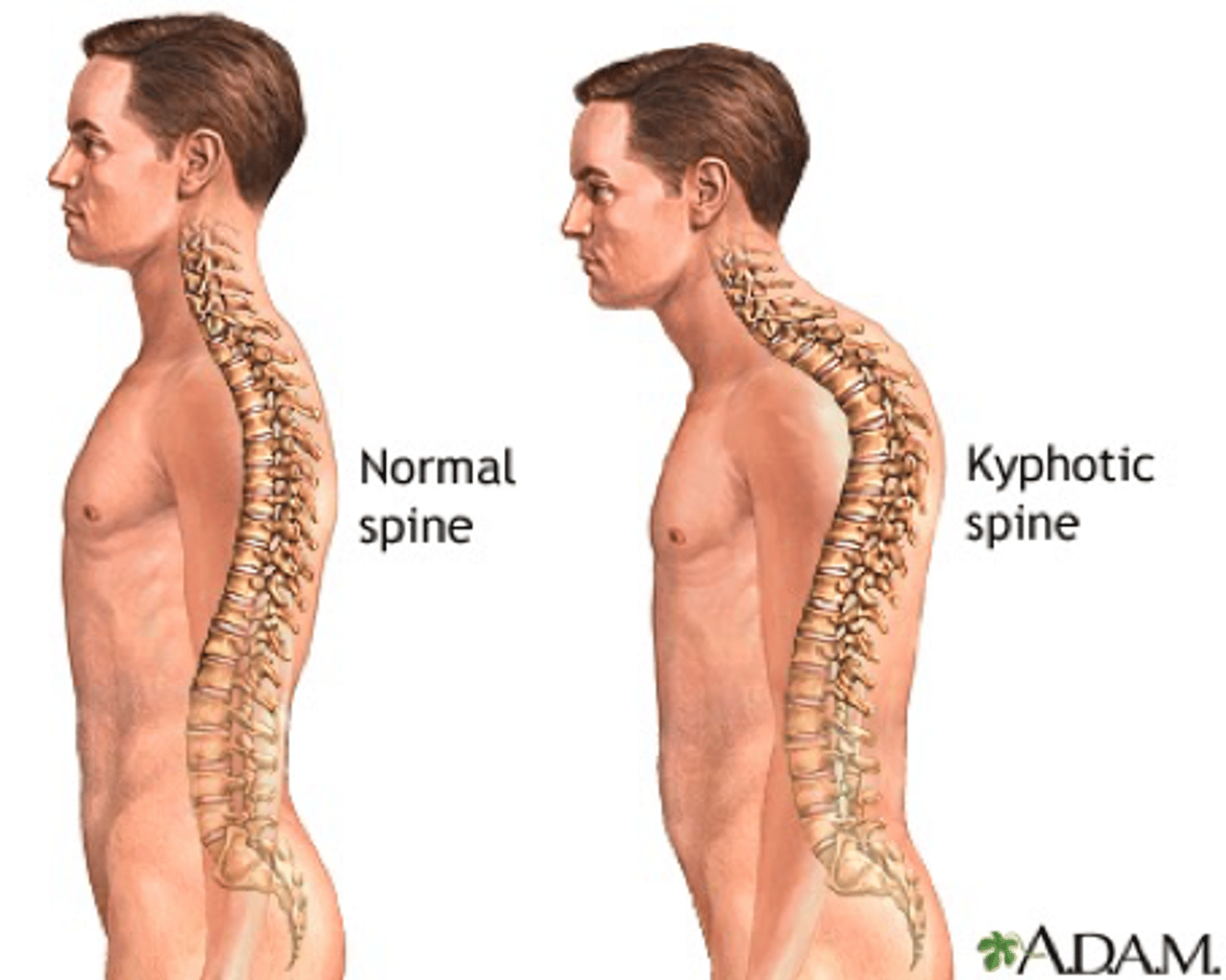
Kyphosis "Hunch Back"
•Anterior wedging of >5 degrees in at least 3 vertebrae
•Thoracic spine commonly effected
epi kyphosis
•10-12 y/o common age of onset
•More common in males
hx kyphosis
•Thoracic or lumbar pain
•Cosmetic complaints
PE kyphosis
•Visible deformity which is worsened with leaning forward
•Normal kyphosis between 20-45 degrees
•Tight hamstrings, iliopsoas, and anterior shoulder
•+/- hyperlordosis of the cervical and/or lumbar spine
Imaging necessary for kyphosis & findings
Xray w/ AP & Lateral view
Anterior wedging & disc narrowing
Conservative tx of kyphosis
Kyphosis <60 degrees and mild symptoms
PT: postural improvement exercises and back extensor strengthening
Bracing: kyphosis between 60-80 degrees.. usually does not lead to correction but can stop progression
when is surgical intervention indicated in kyphosis?
kyphosis >75 degrees
neurologic deficit
spinal cord compression
severe pain in adults
Surgical tx of kyphosis
Posterior spinal fusion +/- osteotomy +/- anterior releass
Scoliosis involves what plane
Coronal plane spinal deformity
What portion of the spine is affected by scoliosis (common)
Thoracic spine commonly effected
epi of scoliosis
•More common in females
•More common in adolescent 10-18 y/o
•Right sided thoracic curve most common
•Four common types of scoliosis: congenital (malformation), neuromuscular (cerebral palsy, polio, neurofibromatosis), degenerative and idiopathic
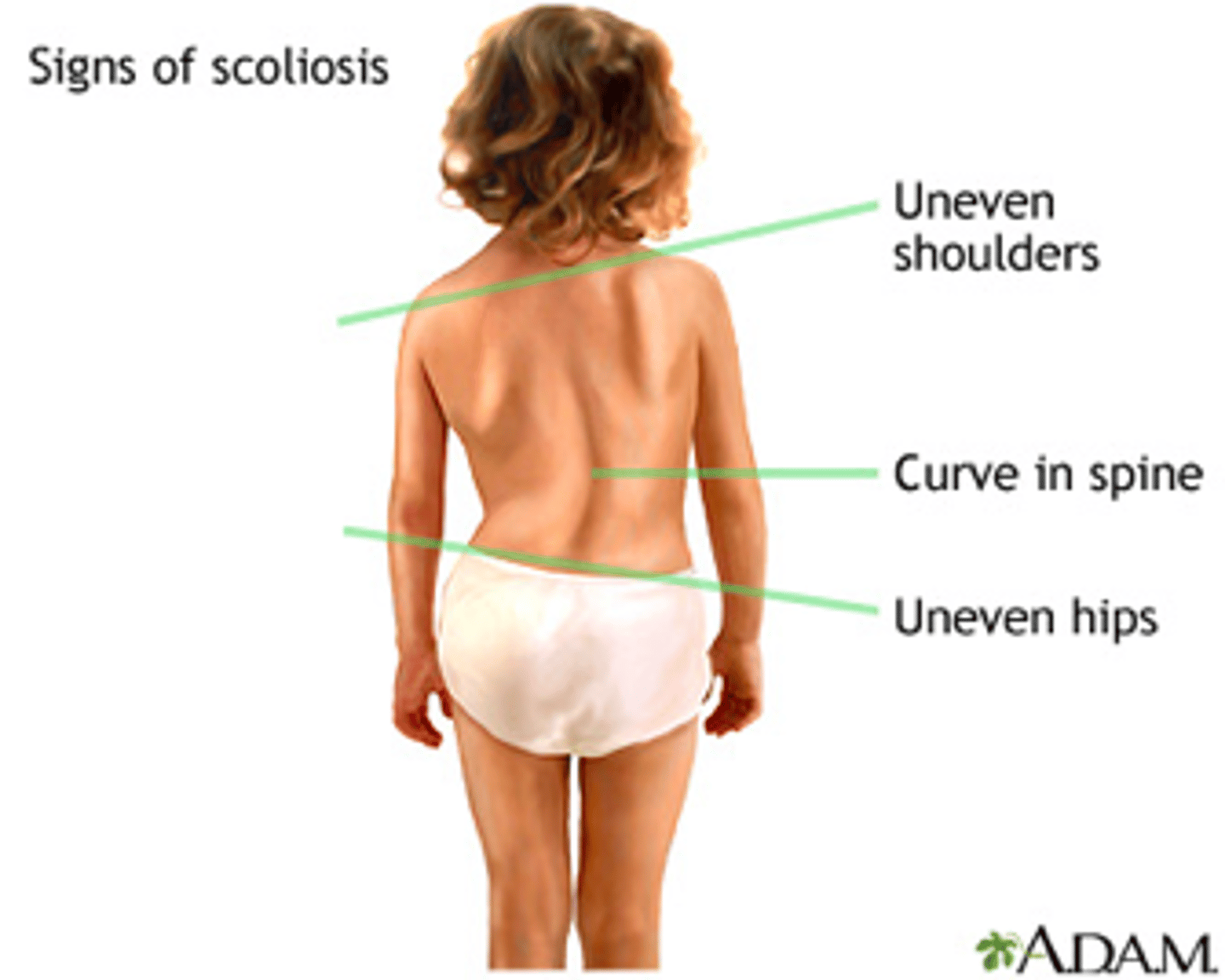
hx scoliosis
•Dorsalgia or lumbar pain
•Uneven shoulders
•Radiating pain down legs (impingement)
•Fatigue
PE of kyphosis
•Visible deformity of spine with +/- uneven shoulder and/or pelvic height
•Often picked up during school screening. Adams forward bending test >7 degrees on scoliometer
•Hairy patches on back or cafe-au-lait spots (neurofibromatosis)
•Respiratory restriction in severe cases (PFT)
Gold standard imaging for scoliosis
X-ray: standing AP & lateral view
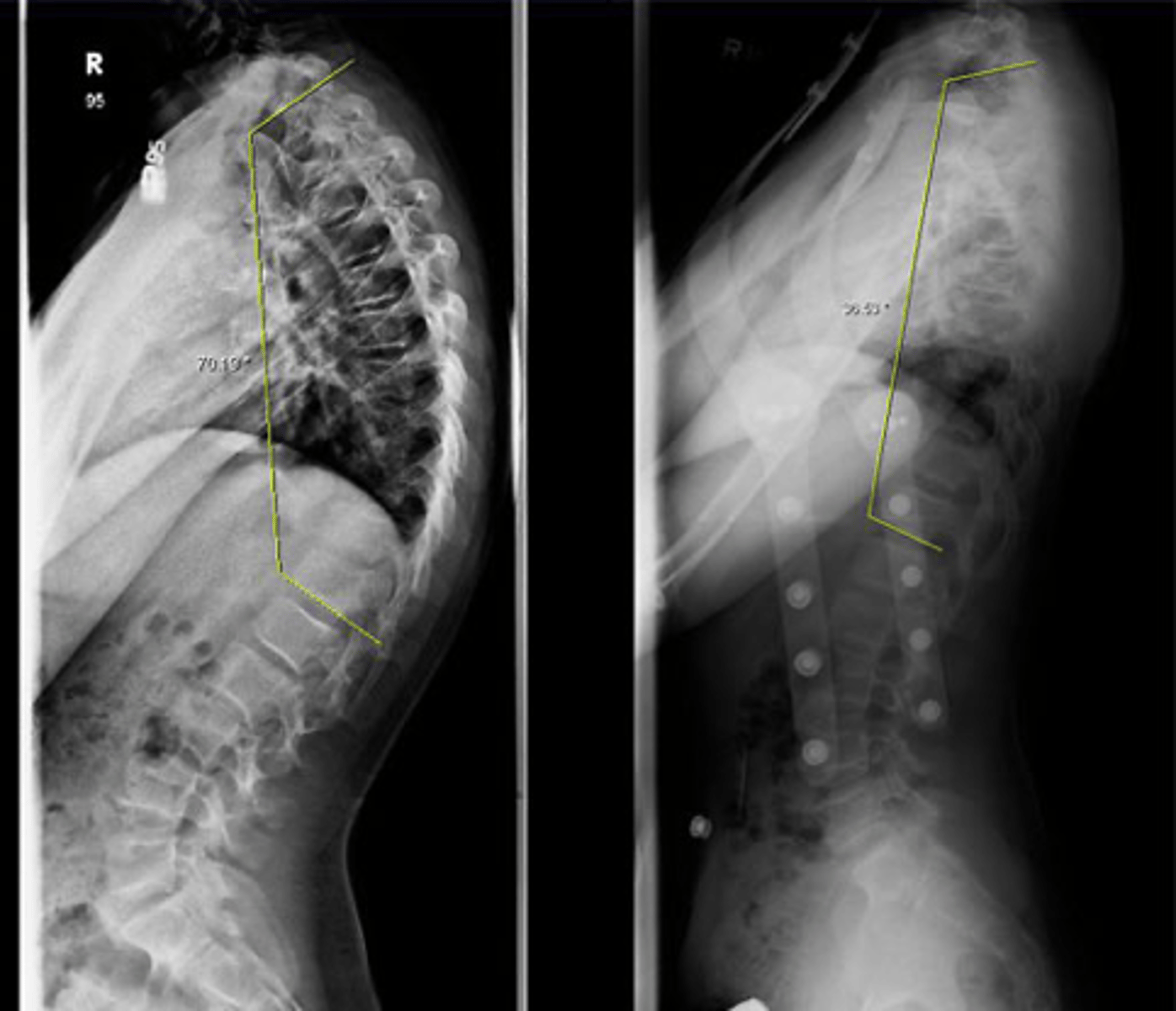
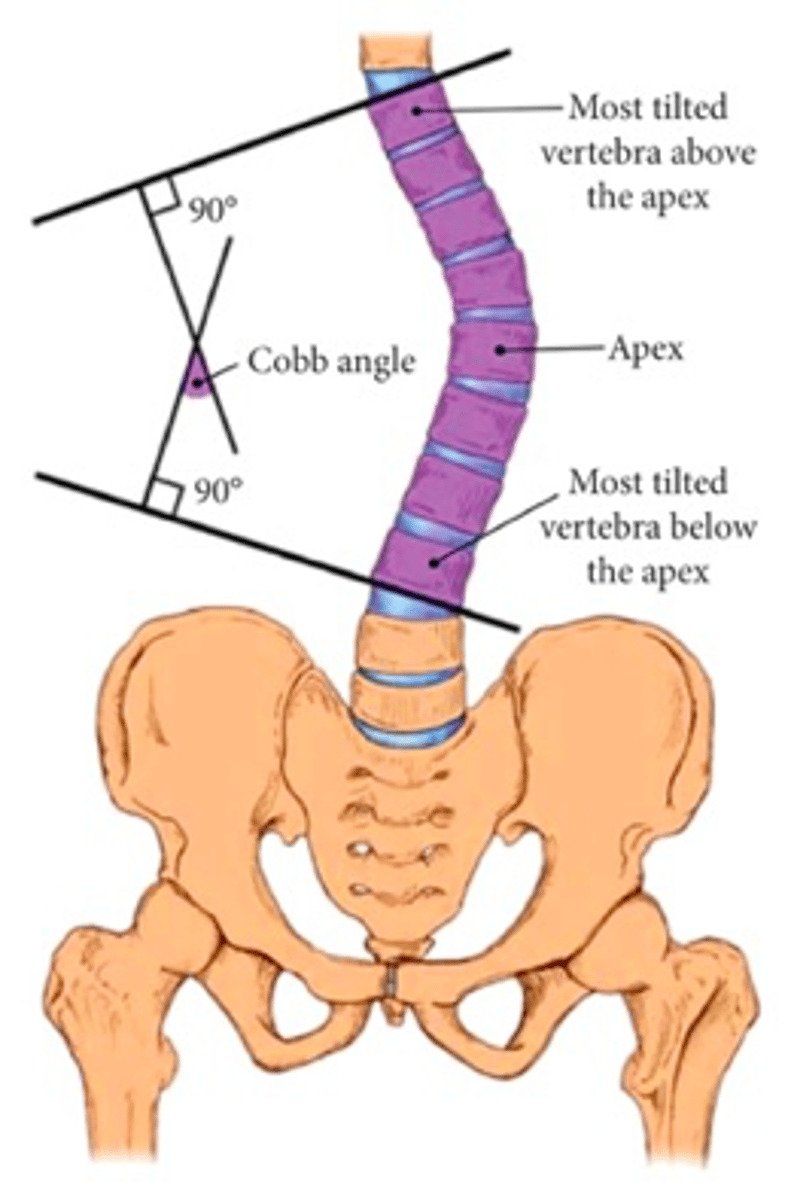
What measurement tool is used to determine the severity of scolosis curvature & determine tx plan?
Cobb angle
angle between 2 lines perpendicular to the upper and lower most involved endplate vertebrae. Helps determine severity of curvature and facilitate tx plan
Conservative tx of scoliosis
Observation (mild, <25 degrees of curvature) with serial xrays
Bracing & PT (Moderate, 25-45 degrees of curvature). Bracing won’t fix deformity but will help stop progression.
Posterior spinal fusion is indicated in what degree of scoliosis
Scoliosis cobb angle >45 degrees
Spinal stabilization of the curve > correction.
Degenerative disorder of the spine
Osteoarthritic changes of the spine over time that can affect surrounding structures and lead to chronic neurological symptoms
degenerative disorders of the spine
insidious onset of neck or lumbar pain
radiating pain that follows a dermatome (impingement)
no associated injury w/ onset of symptoms
degenerative disorders of the spine - PE
Slow/wide gait
"Step off" second to spondylolisthesis
ROM: Pain with flexion, extension, and radicular pain
Neurological: Weakness, sensory changes and decrease strength with resisted strength testing. Diminish/hyper reflexes
Differentiate PE findings between degenerative disorder & lumbosacral pain
In degenerative you WILL see NEURO changes and RADICULAR pain (none in lumbosacral pain)
Gold standard testing for Degenerative Disorders of the Spine?
MRI
MRI + contrast to evaluate infection or tumor
other imaging for Degenerative Disorders of the Spine
•Xray: Decreased disc space, instability (anterolisthesis), obvious deformity
•CT Myelogram: If MRI is contraindicated (pacemaker, metallic implants)

Treatment of degenerative disorder
•Oral steroid taper (Medrol Dose pack)
•NSAIDs
•Activity modification
•Physical therapy
•Often effective in the first 6 weeks of sx onset
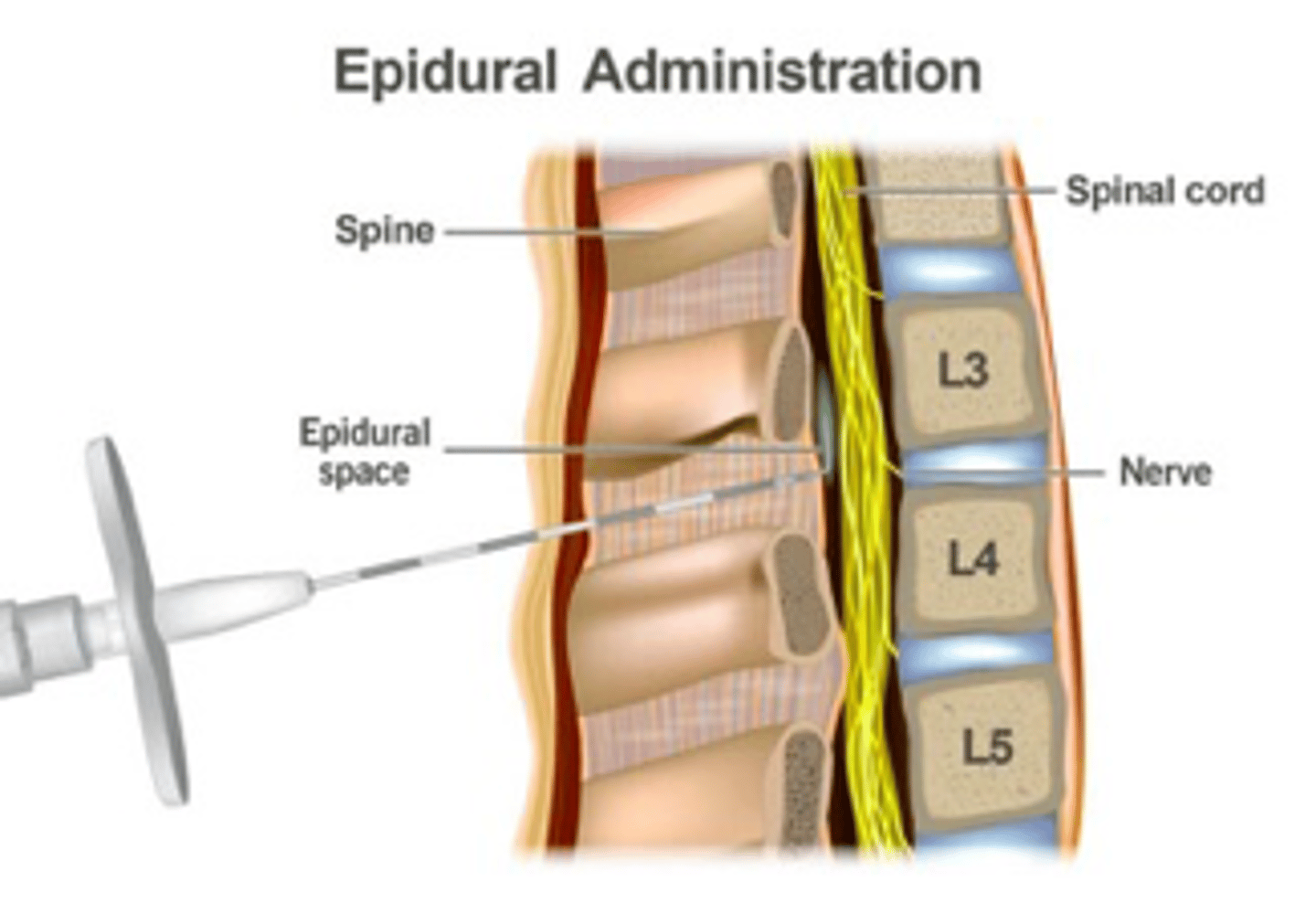
•Epidural steroid spine injections
Surgery --> Refer to ortho for definitive tx
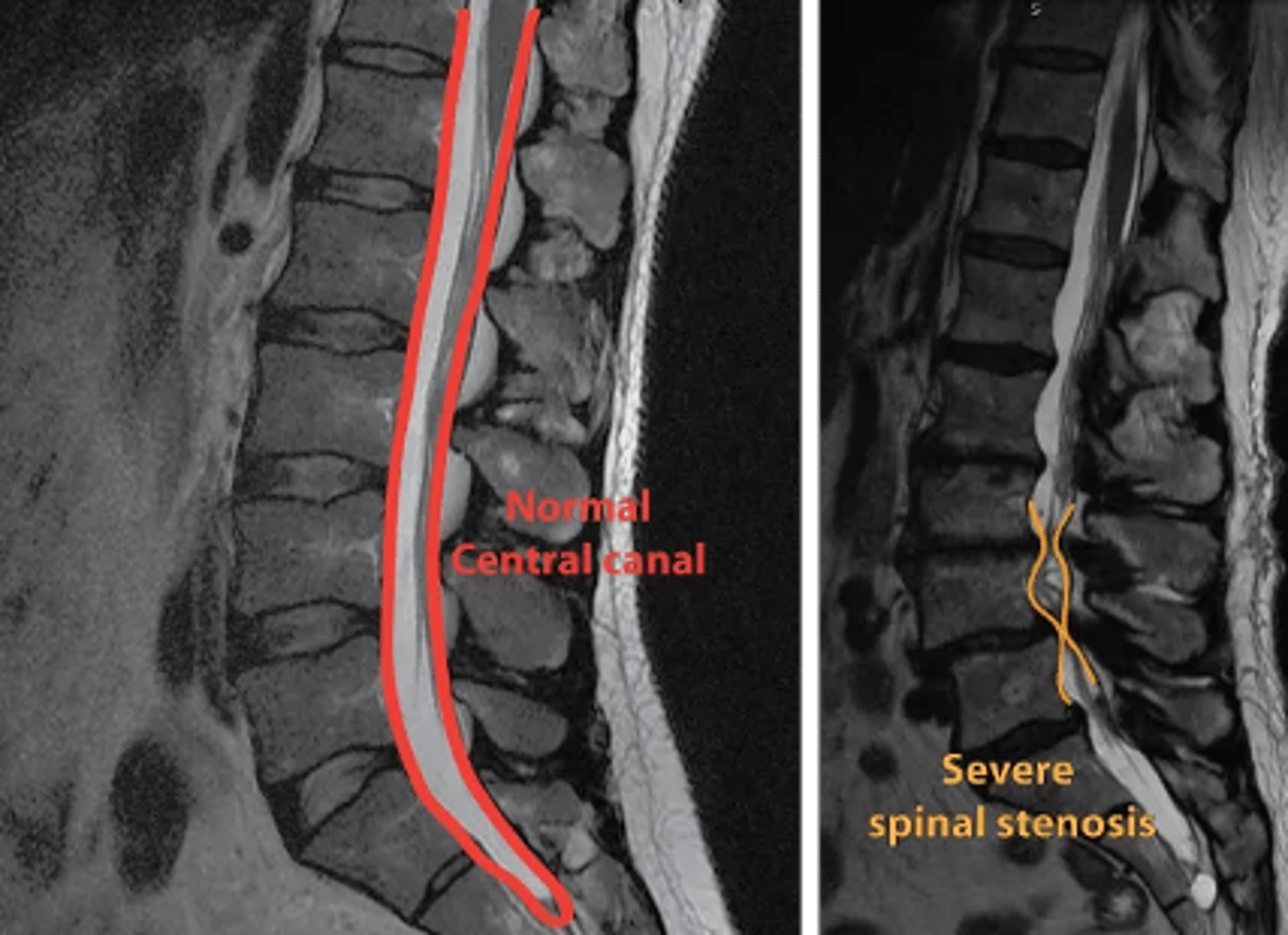
What is spinal stenosis?
degenerative spinal condition characterized by the narrowing of the central spinal canal, lateral recess or neural foramen
What structures may cause spinal stenosis?
Facet Osteophytes
Spondylithesis
Herniated Disc
Ligamentum flavum hypertrophty
spinal stenosis epi/RF
•Most common reason for lumbar spine surgery in patients > 65 years old
•Most commonly occurs at L4-5 (91%)
•Risk factors: Caucasian, increased BMI, congenital spine anomalies (20%)
spinal stenosis hx
•Back pain (referred pain to gluteal region)
•Unilateral leg pain
•Pain worse with extension (walking, standing upright)
•Pain relieved with flexion (sitting, leaning over shopping cart, sleeping in fetal position)
•Weakness
PE spinal stenosis
•Limited physical findings
•Kemp sign = Positive
•Straight leg raise = Negative
•Valsalva test = Negative (+ in herniated disc!)
Kemp sign
Unilateral radicular pain from foraminal stenosis made worse by extension of the back
+ IN SPINAL STENOSIS
Valsalva test is negative in ____ and postive in ______
spinal stenosis; herniated disc
Gold standard imaging for spinal stenosis
MRI
MRI findings in spinal stenosis
•Central stenosis with a thecal sac
•Obliteration of perineural fat and compression of lateral recess or foramen
•Facet and ligamentum hypertrophy
other imaging for spinal stenosis
Xray
•Nonspecific arthritic changes (disk space narrowing, osteophyte formation)
•Degenerative scoliosis
•Degenerative spondylolisthesis hypertrophy
CT Myelogram
•If MRI is contraindicated (pacemaker, metallic implants)
Conservative management of spinal stenosis
•NSAIDs
•Physical therapy
•Weight loss
•Bracing
•Steroid injections (epidural and transforaminal)
spinal stenosis - surgery
refer to orthopedics if failed conservative management or severe leg symptoms interfere with activities of daily living
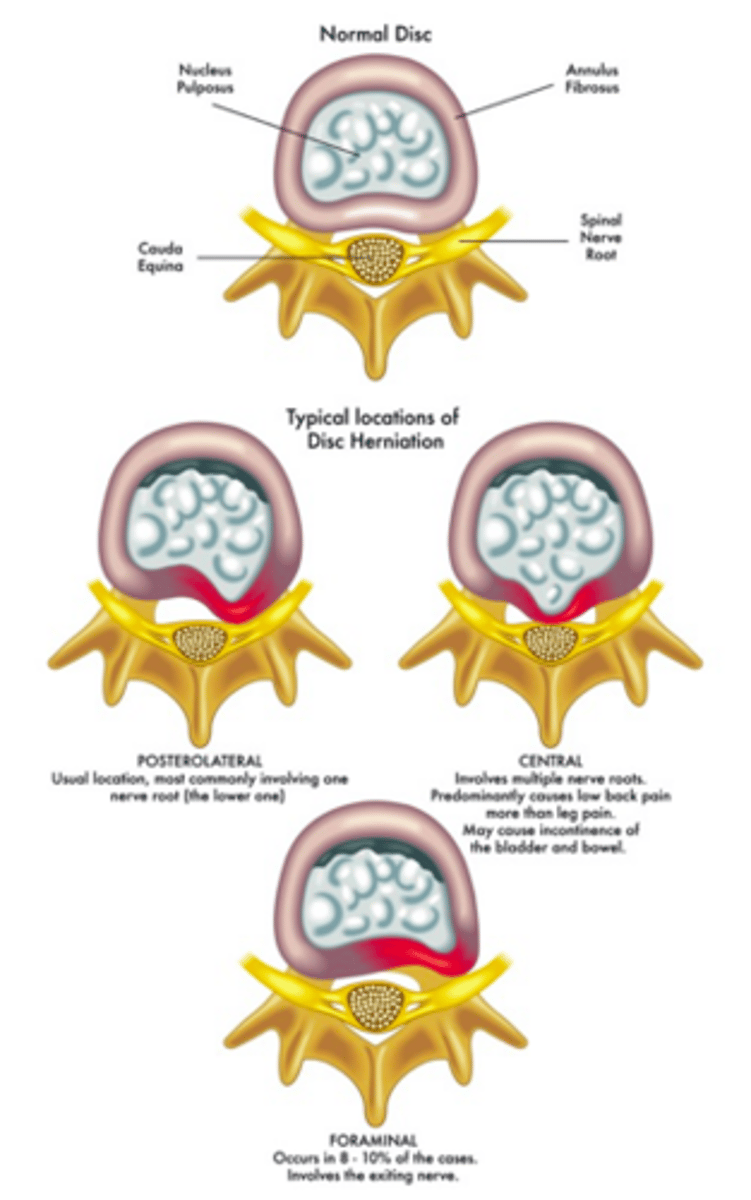
define disc herniation
part or all of the soft, gelatinous central portion of an intervertebral disk is forced through a weakened part of the disk
epi of disc herniation
•Peak incidence in 40s and 50s
•More common is males 3:1 ratio
etiology disc herniation
•Recurrent torsional strain leads to tears of the outer annulus resulting in herniation of nucleus pulposis
•L4-L5 or L5-S1 are the most common levels affected 95%
disc herniation history
•Lower back pain
•Radicular pain. Worse with sitting, coughing or sneezing and improved with standing.
•Pay attention to possible cauda equina symptoms (Bilateral leg pain, LE weakness, saddle anesthesia or bowel/bladder incontinence)
Special Tests for Disc Herniation
•Straight leg raise (SLR)
•Cross straight leg raise (CSLR)
•Sitting root test (SRT)
•Kernig test - Rule out meningitis
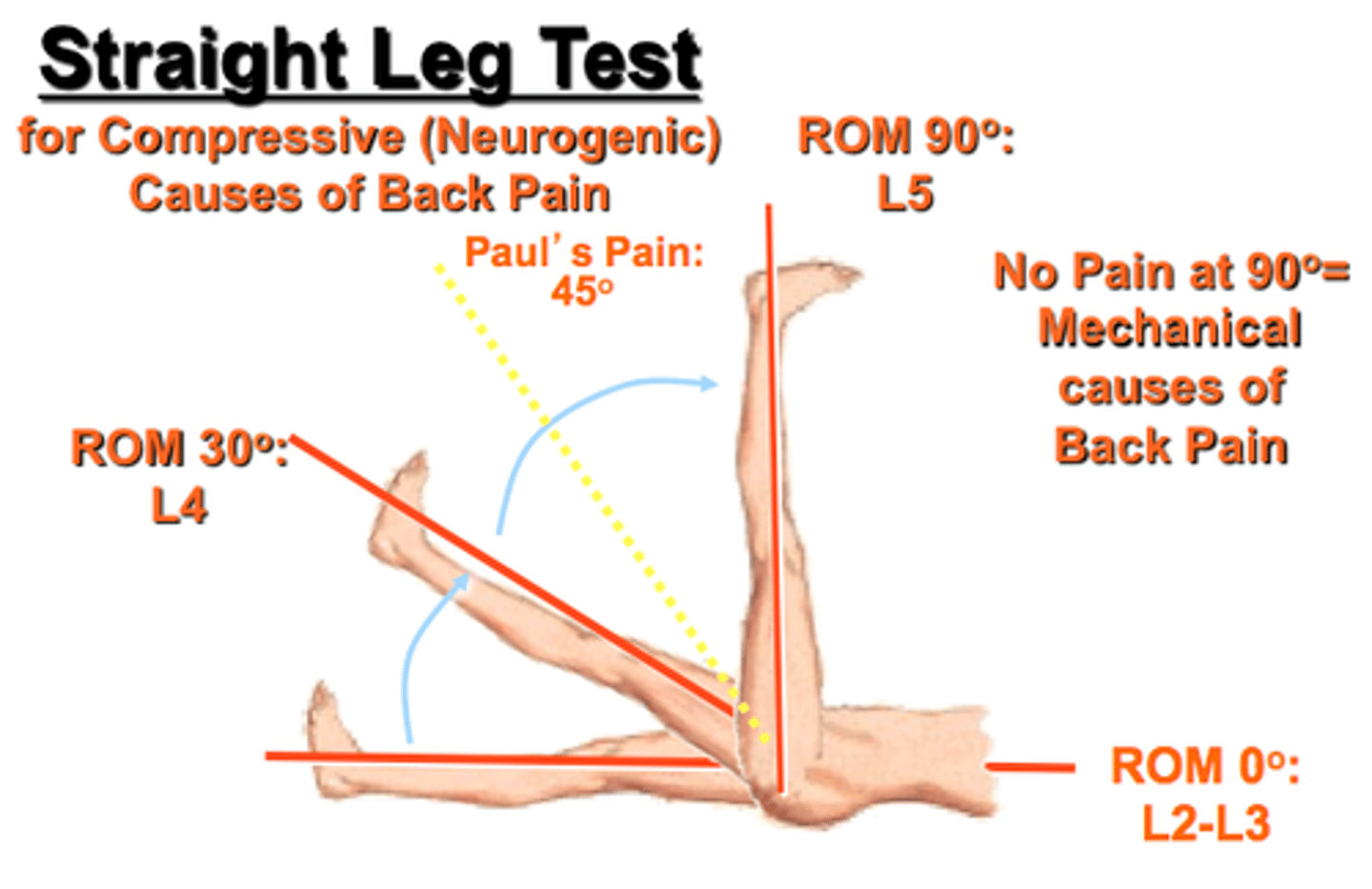
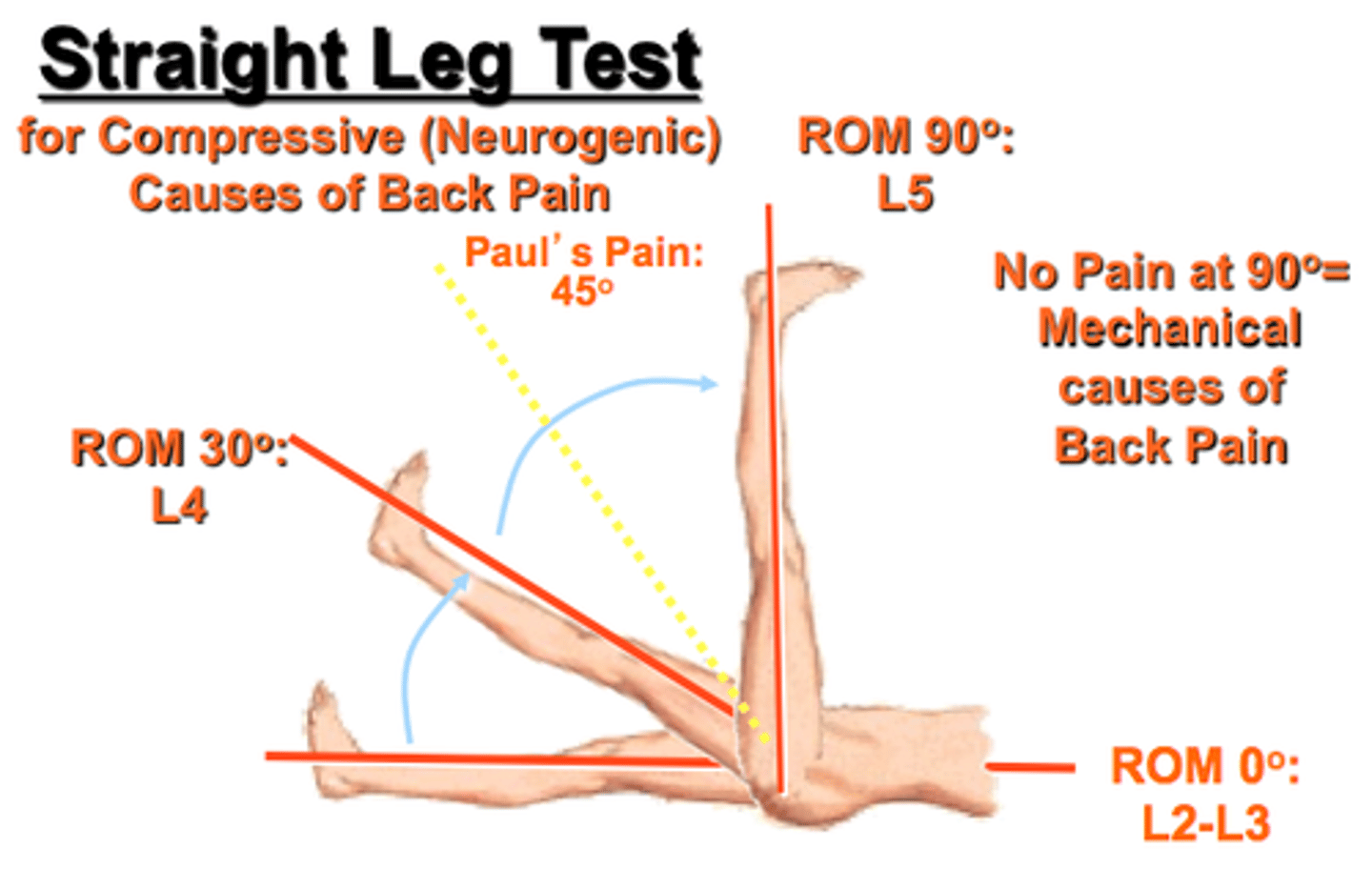
Straight leg test
•Puts tension on L5 or S1 nerve root
•May be done sitting or supine
•Positive with pain and paresthesia down the leg at 30-70 degrees hip flexion
•Most important test for identifying who is a good candidate for surgery
Identify the type of prolapse:
•Back pain only
•Can associate with cauda equina syndrome
Central prolapse (disc herniation)
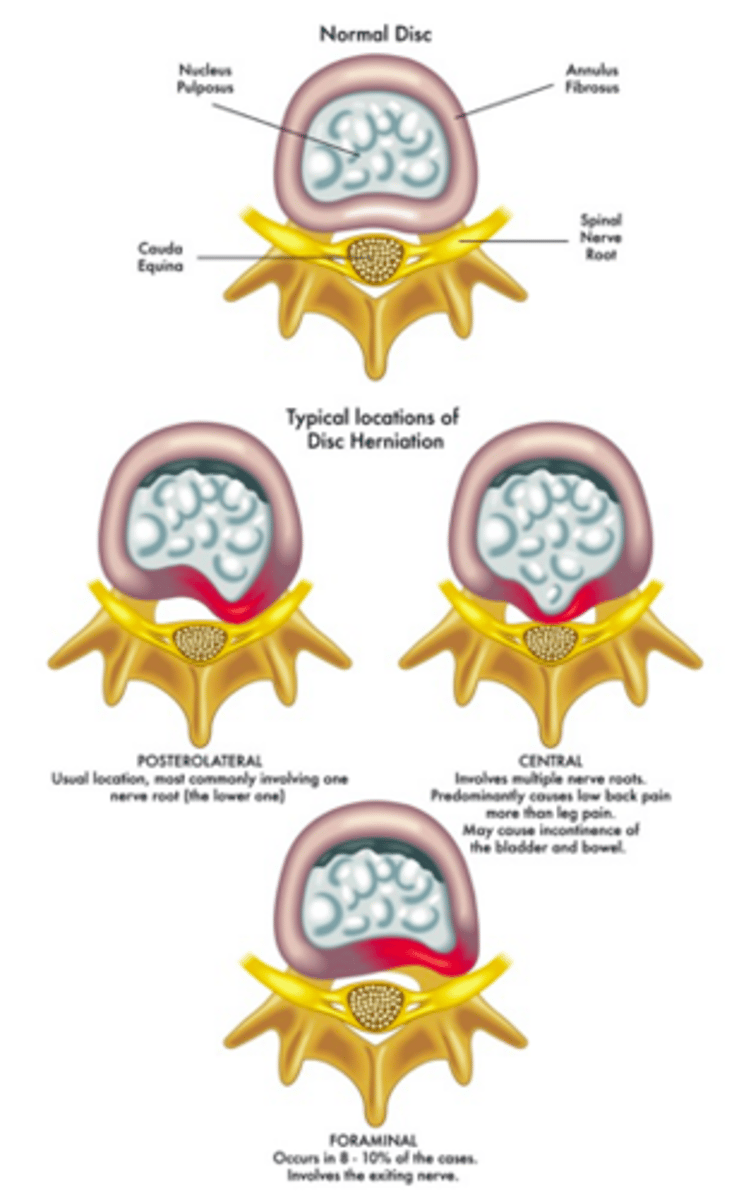
Identify the type of prolapse:
•Most common (90-95%)
•Weak posterior longitudinal ligament (PLL)
•Affects the descending/lower nerve root
•at L4-L5 affects L5 nerve root
Posterolateral prolapse (disc herniation)
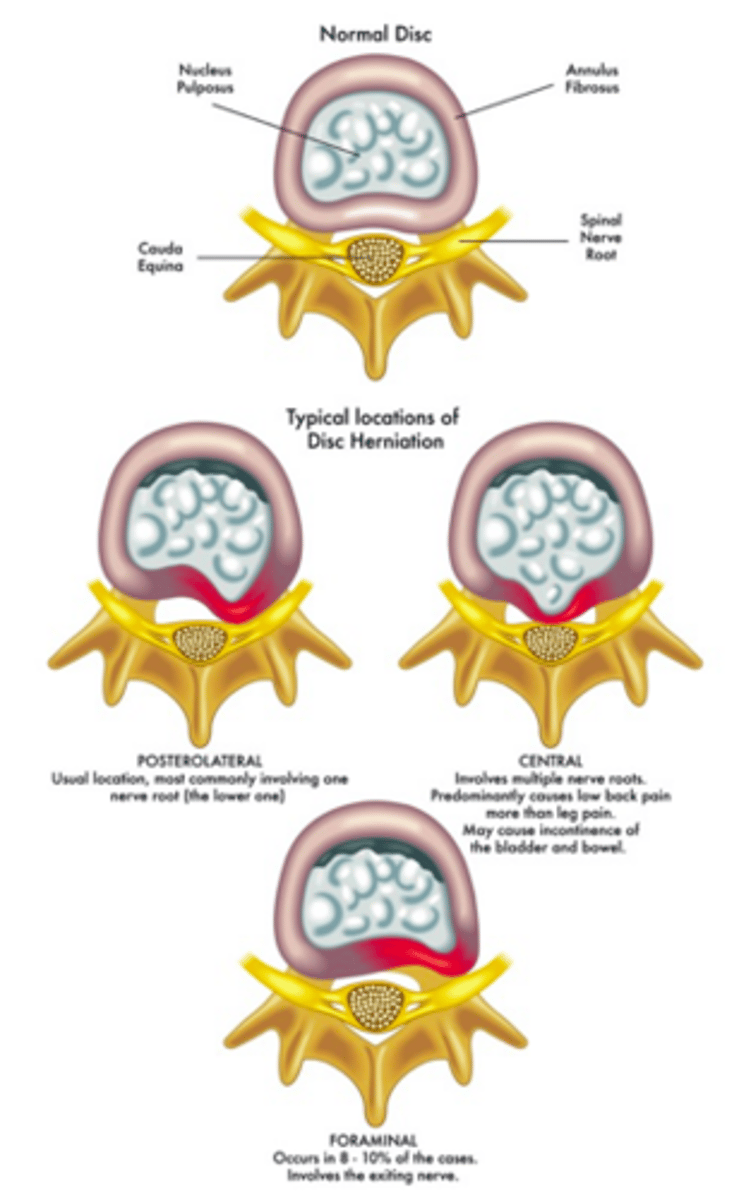
Identify the type of prolapse:
•Affects exiting/upper nerve root
•at L4-L5 affects L4 nerve root
Foraminal prolapse (disc herniation)
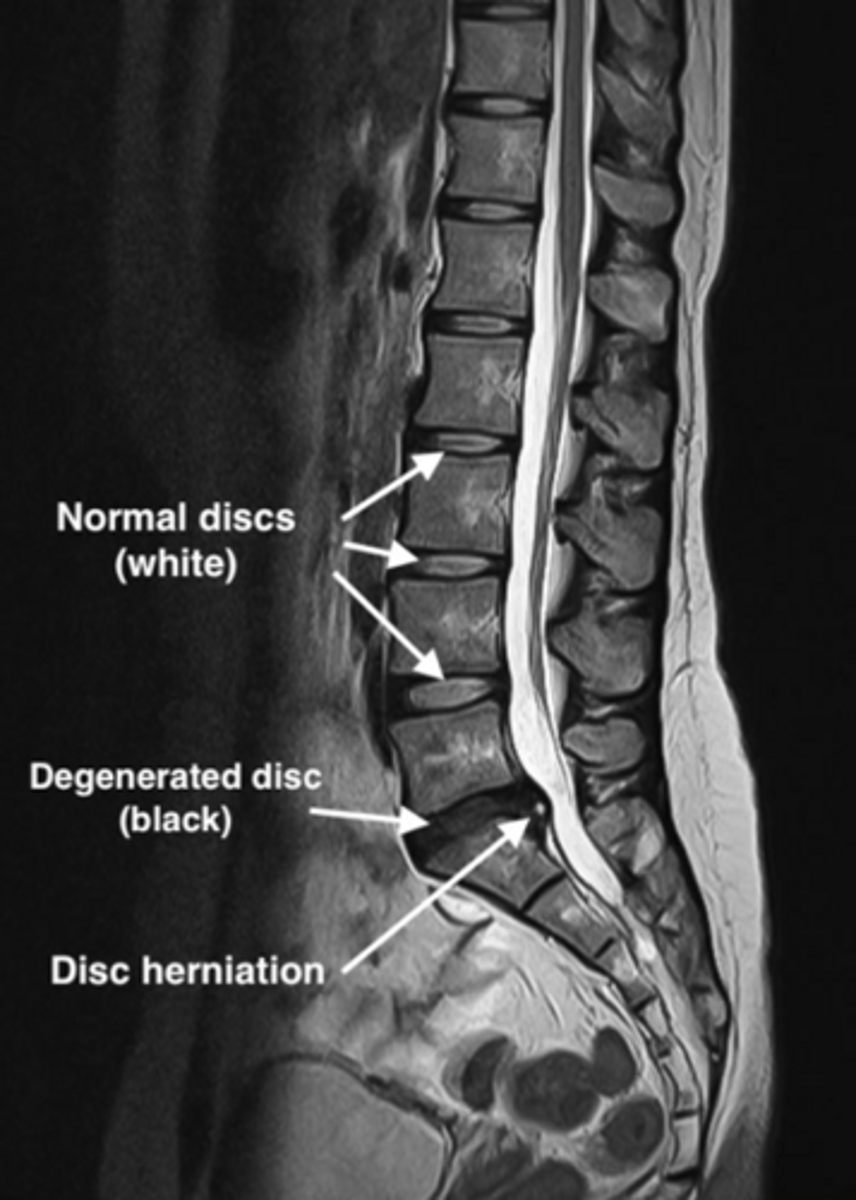
Gold standard for disc herniation
MRI
•Highly sensitive and specific
•Red Flags = MRI ASAP!
treatment of disc herniation (conservative)
•Couple days of bedrest followed by activity as tolerated
•Medications: NSAIDs, Muscle relaxers/Gabapentin, Oral steroid taper (Medrol Dose pack)
•PT: Focus on extension exercises
•Corticosteroid injection: epidural injections and nerve blocks
treatment of disc herniation (surgical)
•Failed conservative management or red flags are present
•Refer to orthopedics (laminotomy and discectomy)