A.P in the Heart
1/22
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
23 Terms
Conducting cells (especially those at the sinoatrial node) = set the heart rate. They are the Effector cells for modulating heart rate
depolarize rhythmically on their own
electrical signal spreads quickly from conducing cell to contracting cell
How does the action potential spread from cell to cell?
If the heart is removed from the body…
it will continue to self-depolarize and contract (as long as it receives the necessary resources for making ATP)
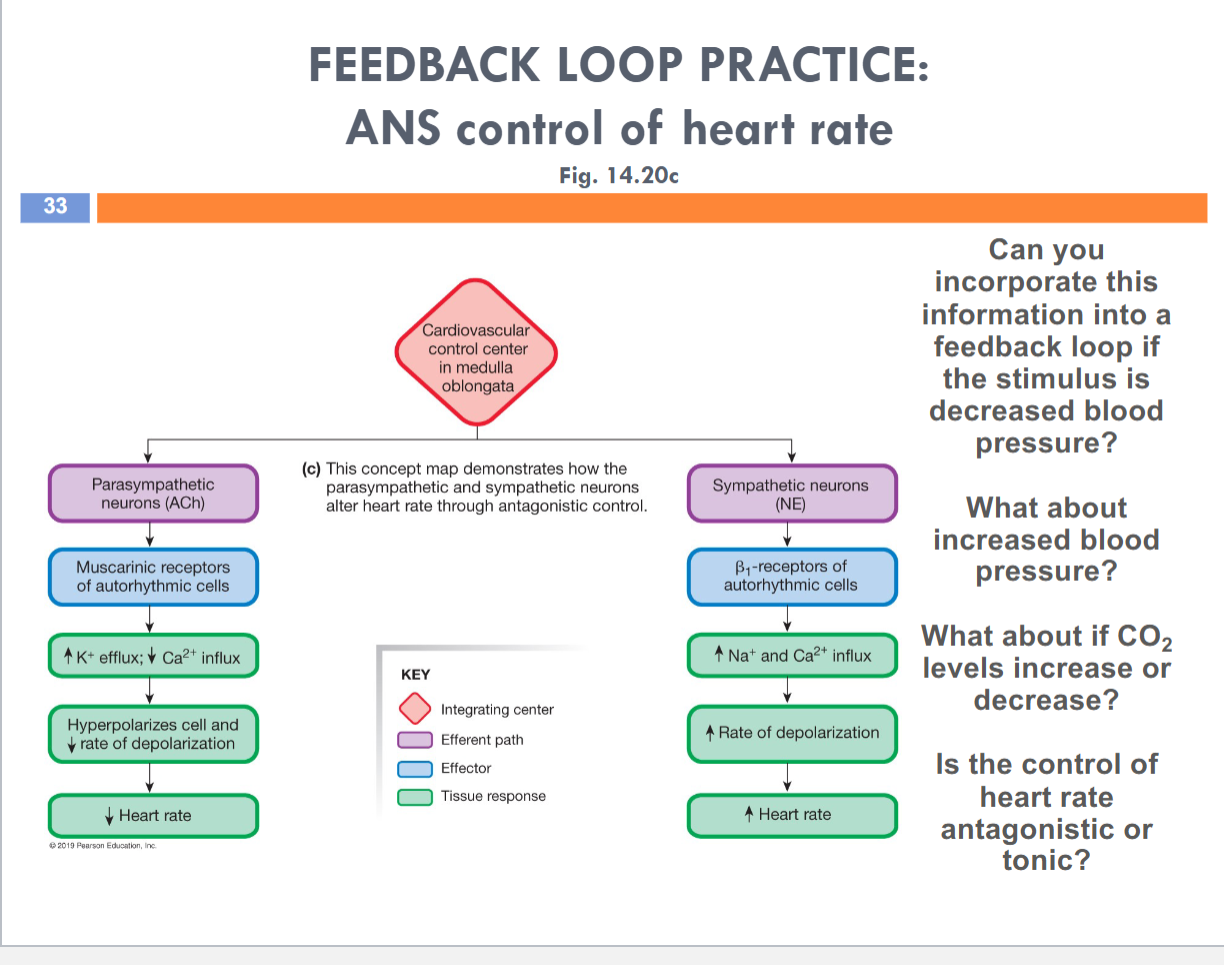
What if heart rate needs to increase or decrease?
The autonomic nerv sys will change the function of SA node conducting cells
Sympathetic neurotransmitter + receptor: Norepinephrine onto B1 receptor
Parasympatheric neurotransmitter + receptor: Acetylcholine onto Muscarinic receptors (GPCR)
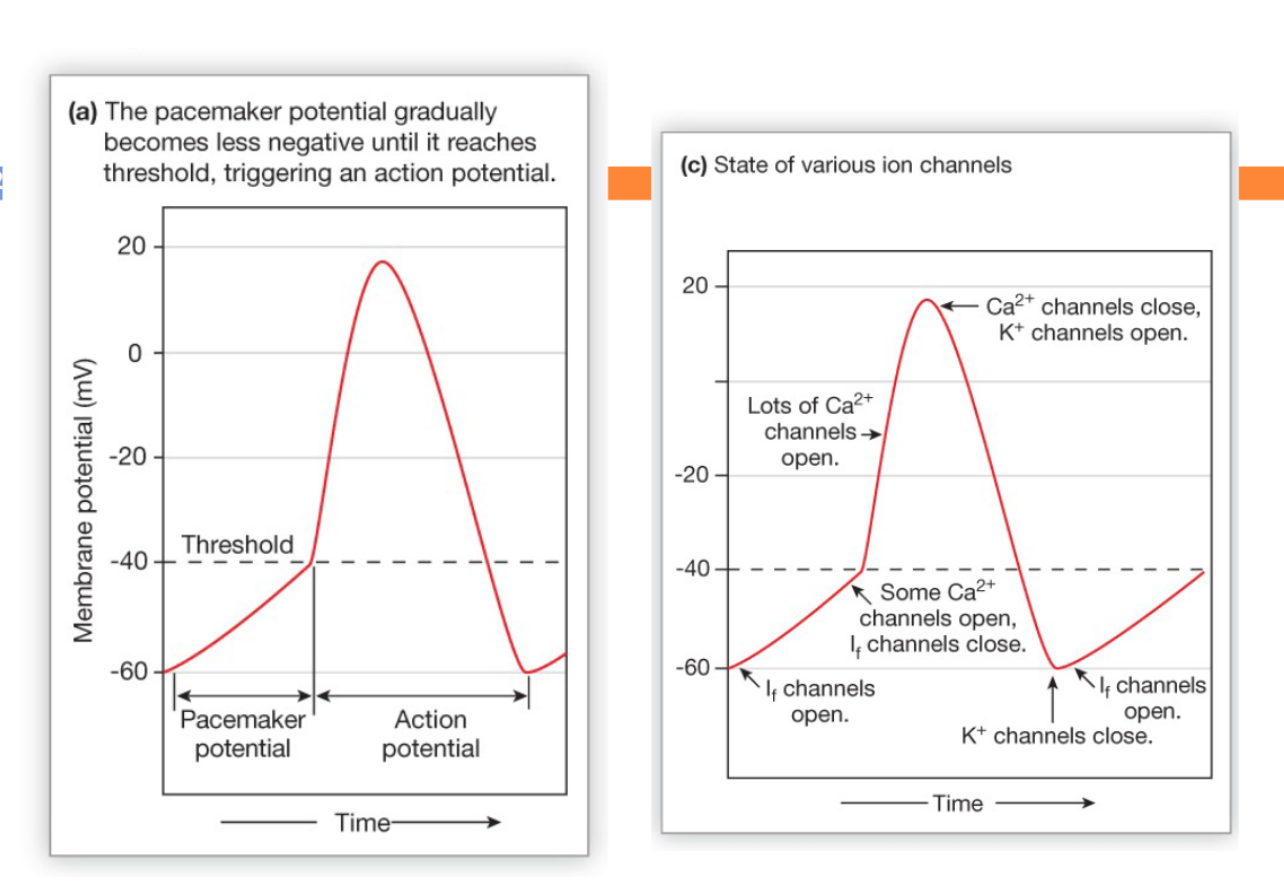
Steps of an autorhythmic cell action potential
The pacemaker potential makes these cells “autorhythmic” or “self-depolarizing”
→ it beings with If (“funny” current) channels opening at resting membrane potential (-60mV), allowing more Na+ influx and less K+ efflux (If channels are monovalent cation channels)
Just before the threshold (-40mV), the If channels close and a “1st set” of Ca++ open
→ speeds membrane potential towards threshold
→ these Ca++ channels close at threshold
At threshold, a “2nd set” of Ca++ channels open, depolarize the cell to its peak then close
K+ channels also start to open at threshold, but are slower, so they only contribute to the repolarization phase
→ these channels close when the cell returns to its resting membrane potential (-60mV)
The sinoatrial (SA) node
is a cluster of conducting cells that determines heart rate
it is the Effector for modulating heart rate
Sympathetic stimulation of the SA node conducting cells…
Norepinephrine released onto B1 receptors → leads to an increase in heart rate
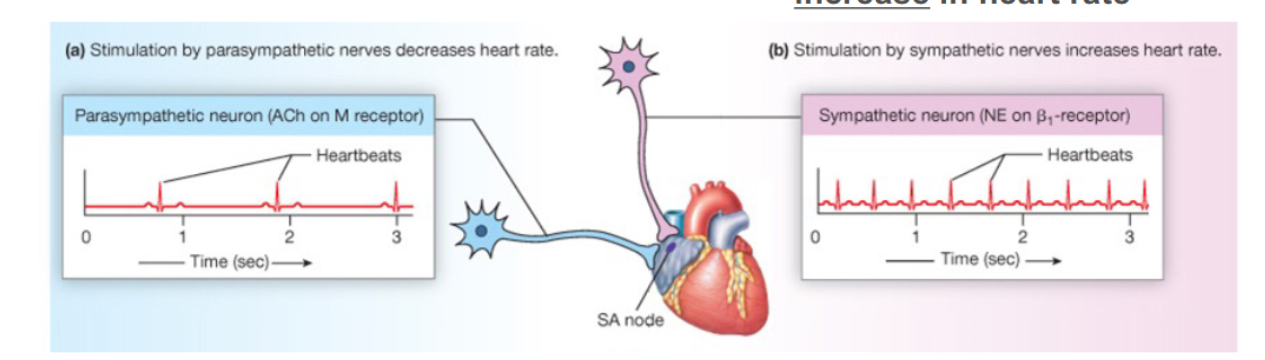
Parasympathetic stimulation of the SA node conducting cells…
Acetylcholine released onto muscarinic receptors → leads to a decrease in heart rate
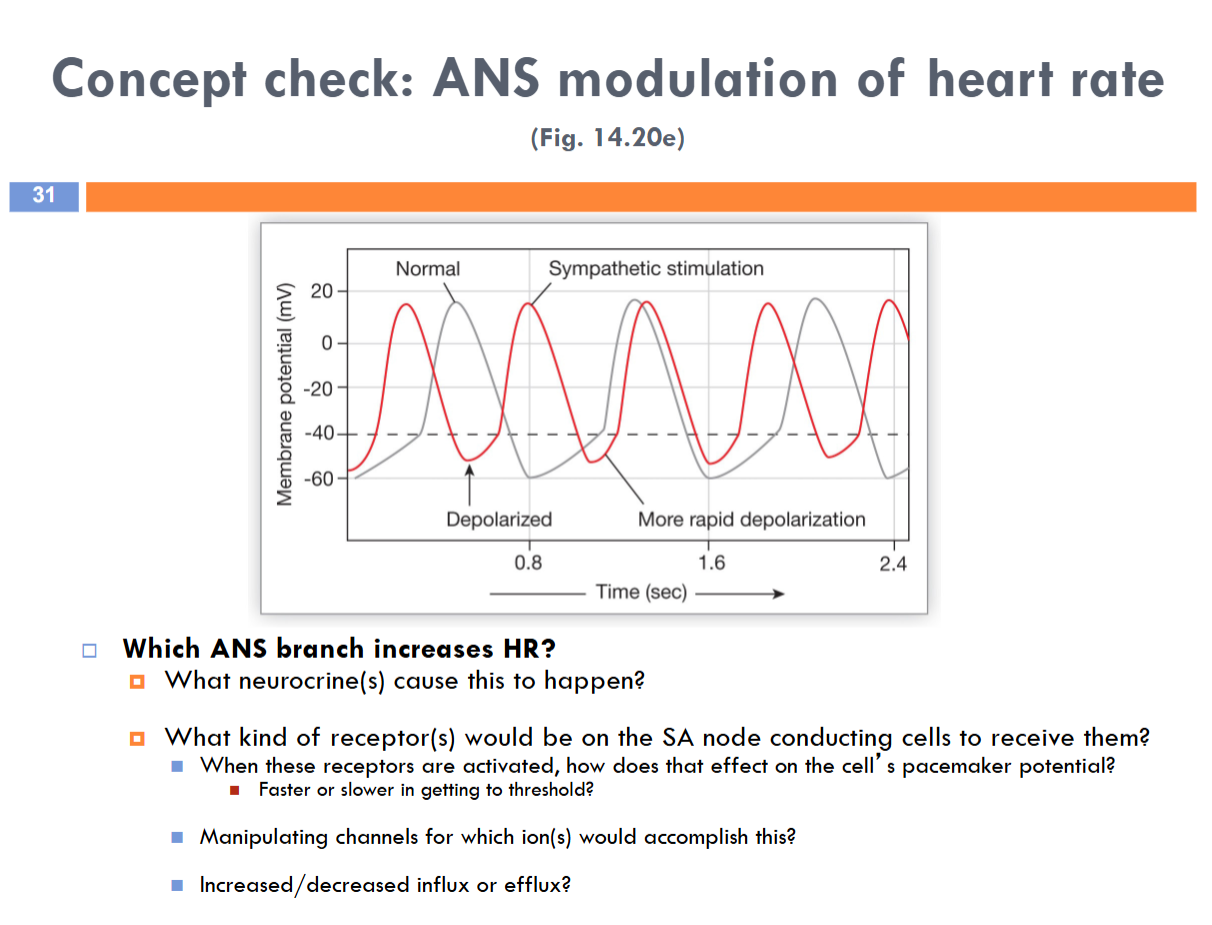
Sympathetic branch of ANS increases HR
Norepinephrine
B1 receptors — faster in getting to threshold
Manipulating channels for If and first set of Ca++ channels
Increase influx
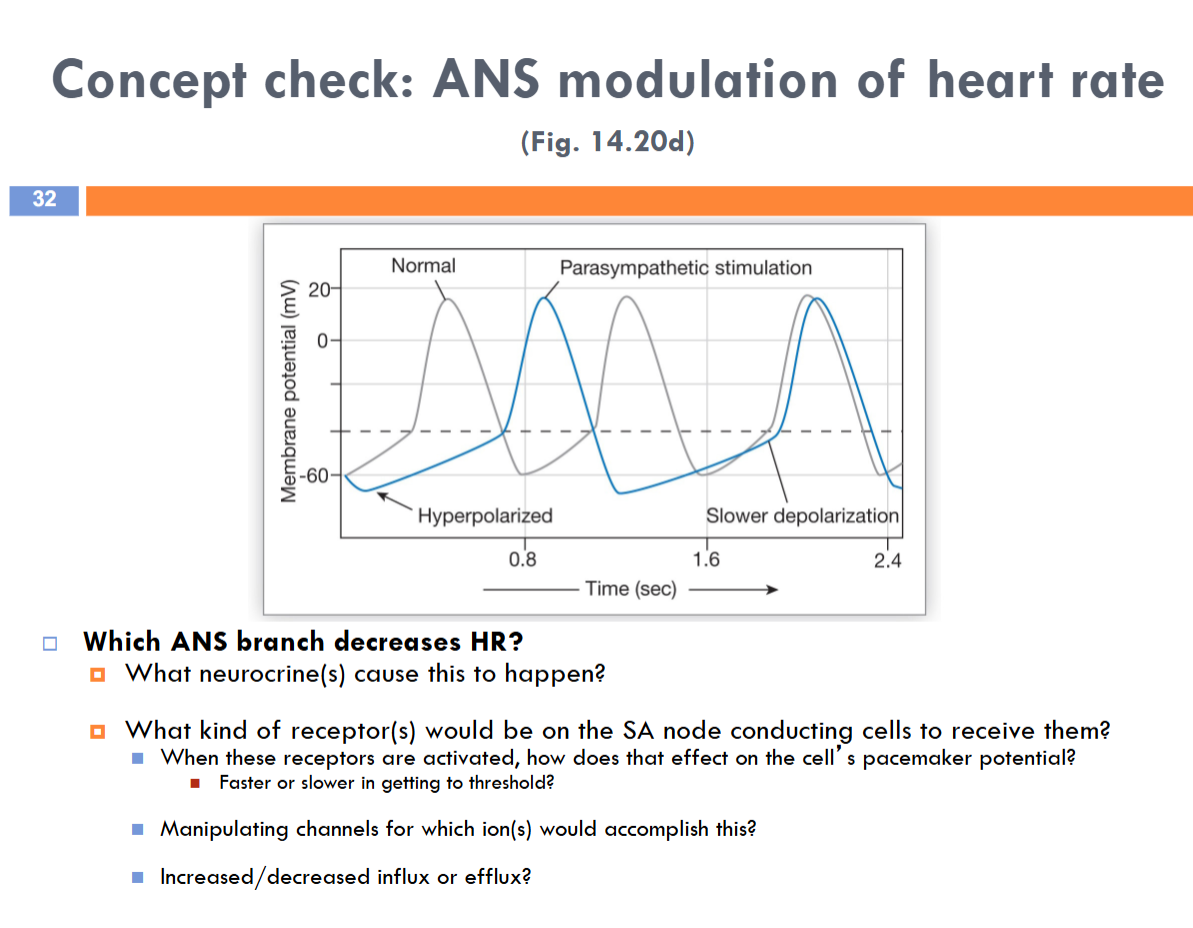
The parasympathetic branch of ANS decreases HR
Acetylcholine
Muscarinic receptors — slower in getting to threshold
Manipulating first set of Ca++ channels and If channels would accomplish this
Decrease Efflux
look at ur notebook!
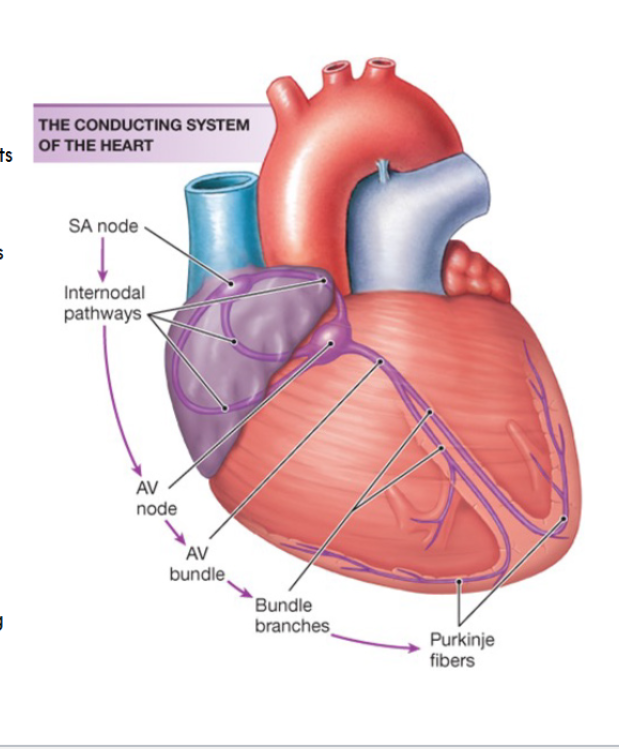
Electrical Conduction Pathway
Begins at the sinoatrial node
→ which is the lead pacemaker, whose function is regulated by the sympathetic and parasympathetic efferent pathways
→ its rate of depolarization determines how fast the action potentials zip through the remaining components of this circuit
Intra-atrial and internodal pathways
→ spreads action potentials to all atrial contracting cells through gap junctions
Atrioventricular (AV) node
→ when the action potential reaches this point, it slows down momentarily and the atria contract
Bundle of His (or AV bundle)
→ spreads action potentials into the ventricles
Right and left bundle branches
→ spreads action potentials down either side of the ventricular septum
Purkinje fibers
→ spreads action potentials to all ventricular contracting cells through gap junction, causing the ventricles to contract from the bottom up
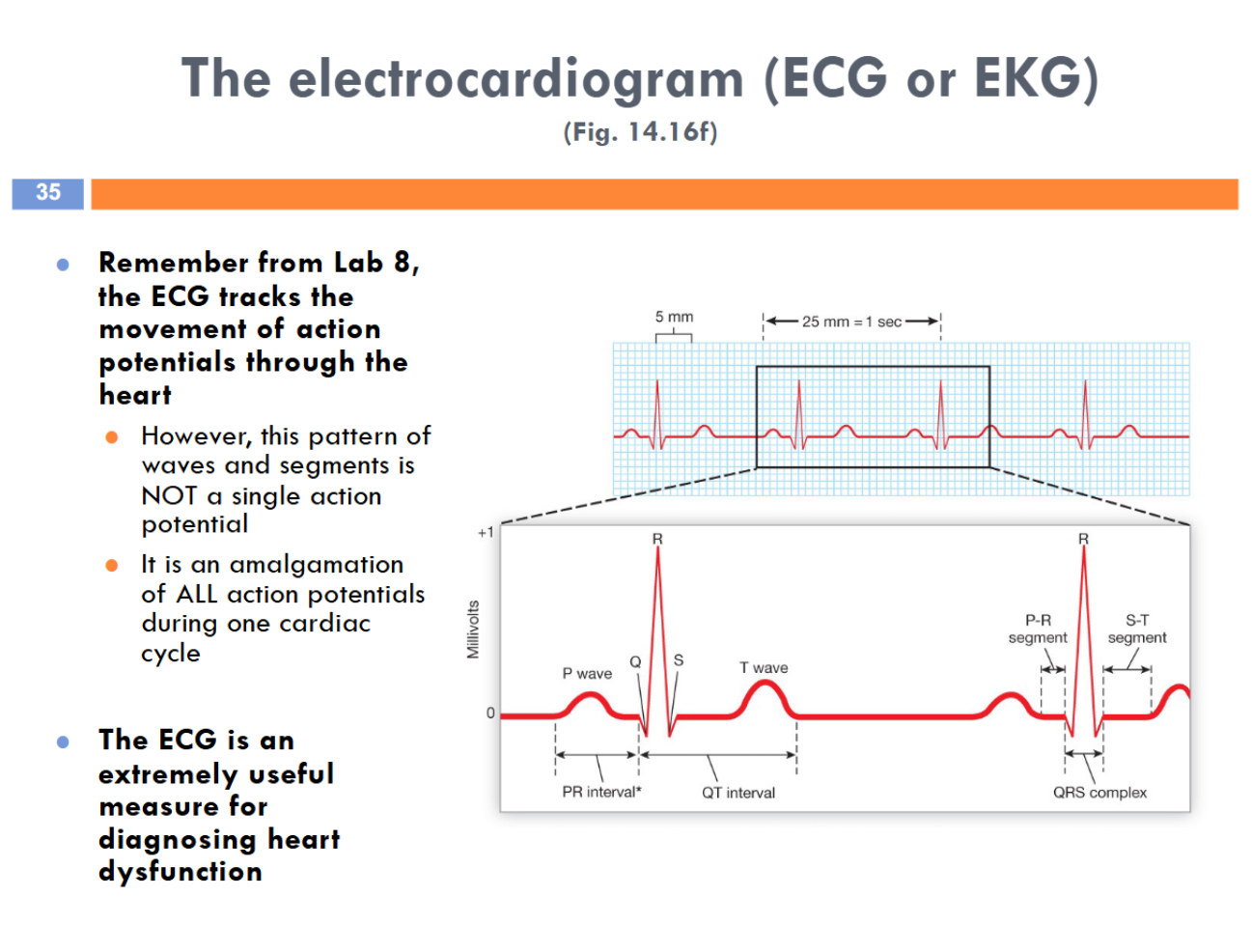
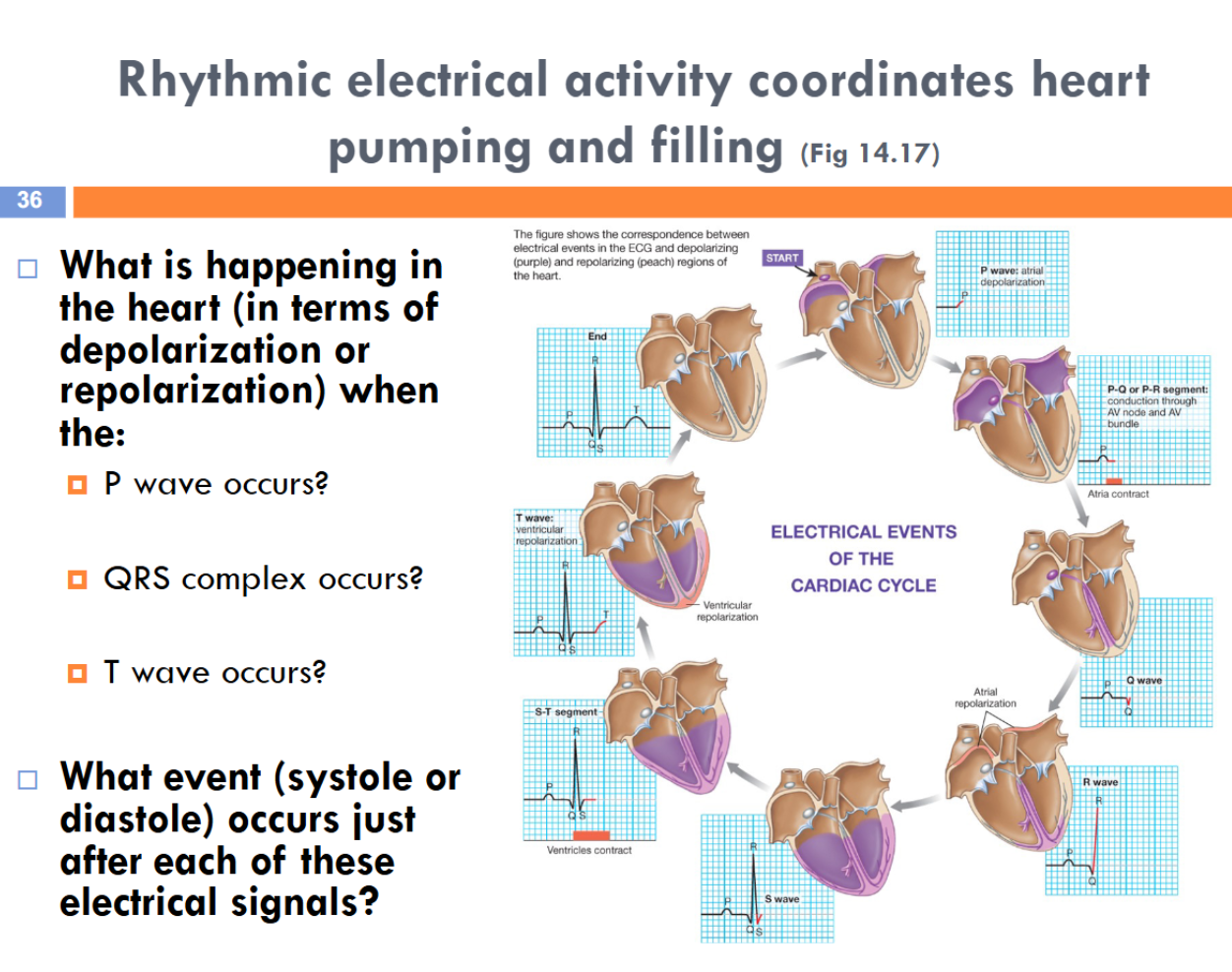
Electrocardiogram
Contractile cells, especially those of the left ventricle, are the Effector for modulating…
Stroke volume!
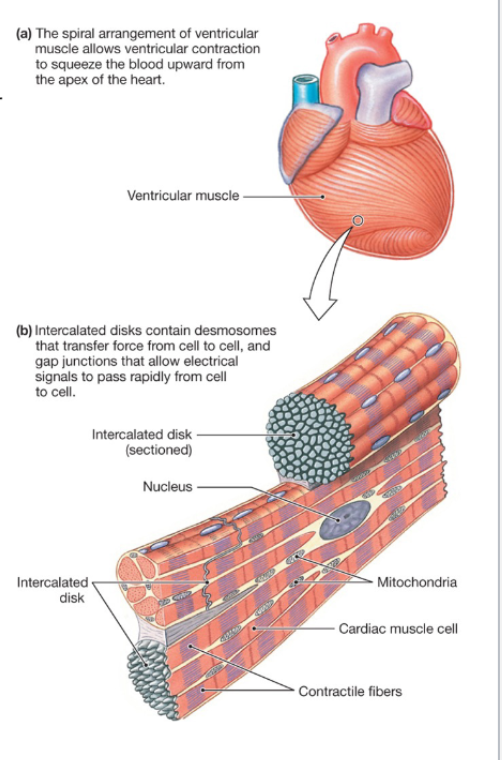
Compared to skeletal muscle, myocardial contractile cells are…
smaller and have a single nucleus
connected by intercalated disks that contain…
→ Desmosomes: provide strength and transfer force between cells
→ Gap junctions: allow transfer of action potentials between cells
Sarcoplasmic reticulum is smaller
→ Ca++ also enters cell from interstitial fluid
Lots of mitochondria
→ occupy 1/3 of cell volume to synthesize ATP
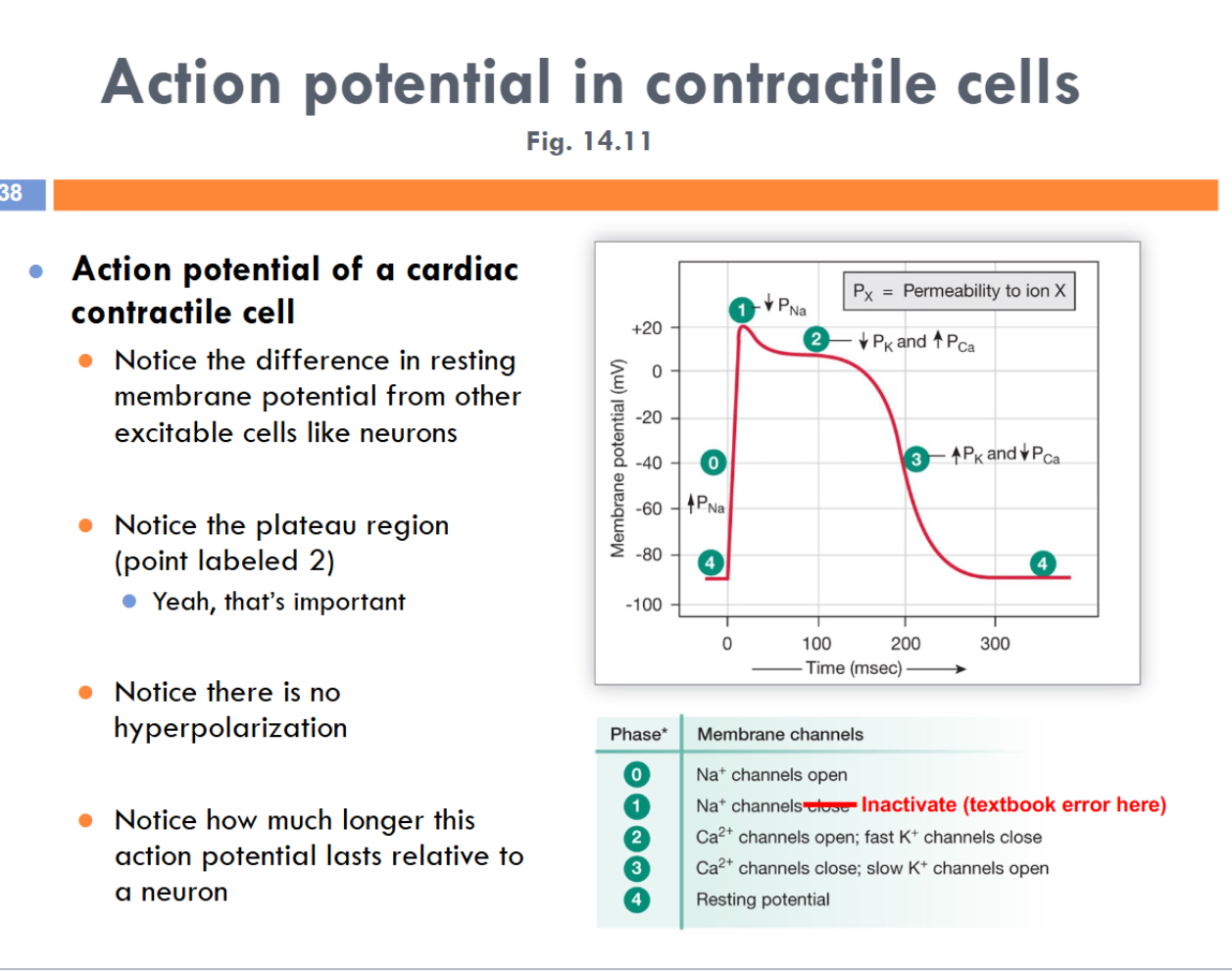
resting membrane potential: -90mV
long duration of an action potential
plateau region (like a constant region) helps extend the action potential
No threshold
2 sets of K+ channels
L-type Ca++ channels: open at depolarization, not fully open until there’s a brief K+ efflux
At the Plateau region, Ca++ influx and K+ efflux is the same
K+ channels dont FULLY open until after the plateau region
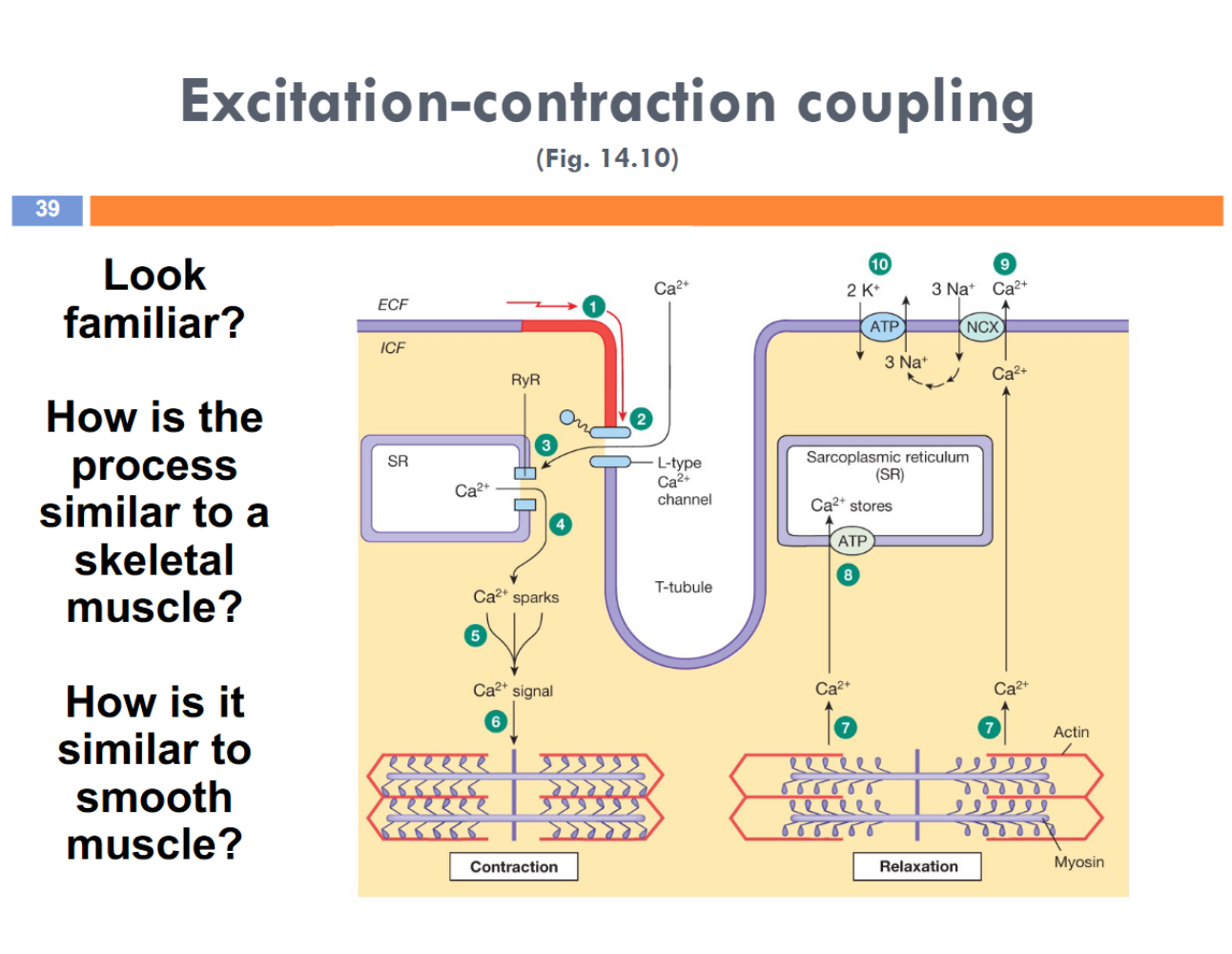
A.P goes down T-tubules and Ca++ binds with L-type Ca++ channels which open, and stimulates Ca++ efflux from the sarcoplasmic reticulum (ryanodine channels)
Calcium induced-calcium release —> amplification
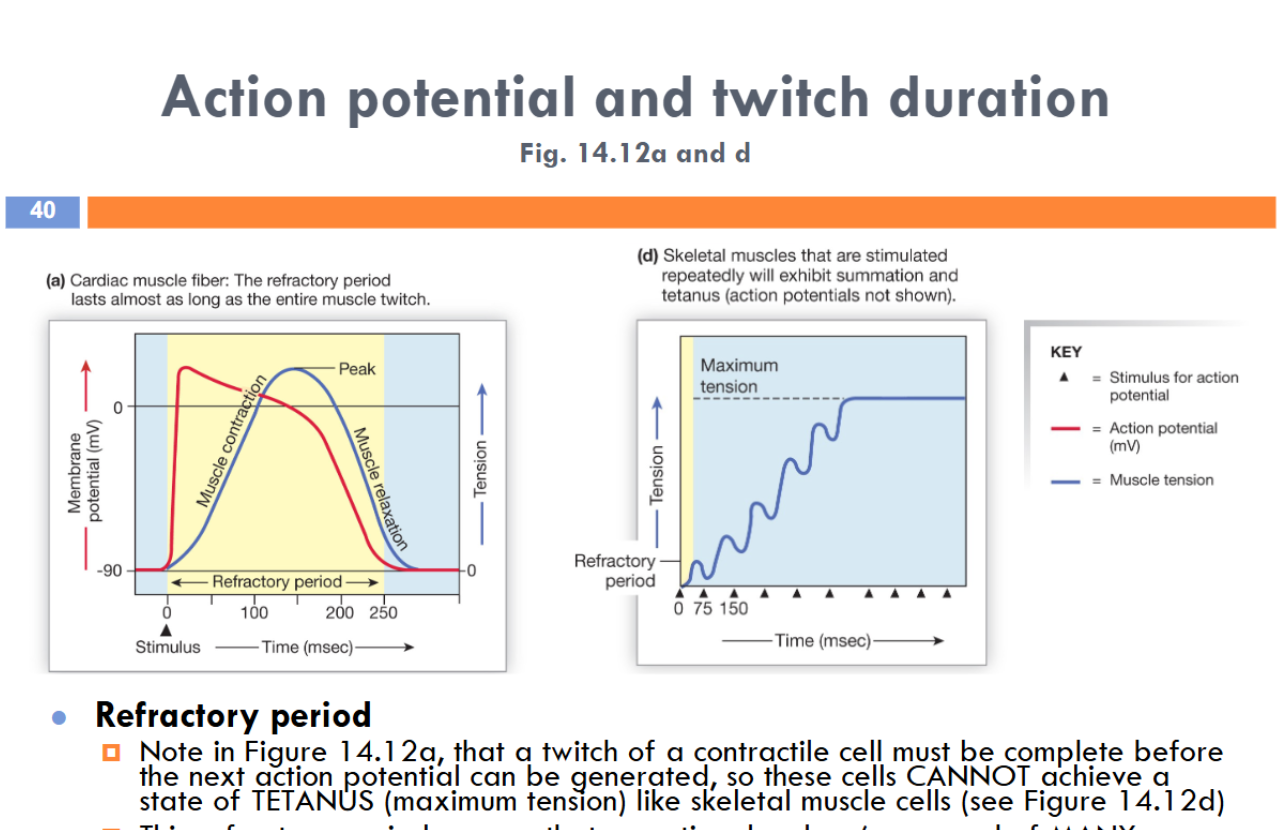
The refractory period ensures that an entire chamber (composed of MANY interconnected contractile cells) will relax fully before being cued to contract again. That ensures an efficient pumping action of the heart, despite how vigorously it is being stimulated!
Force can be graded similar to smooth muscle, but unlike the “all or none” contraction of a skeletal muscle
How can the contraction force vary?: depends on how much Ca++ enters a contractile cell from the interstitial fluid
→ what might affect Ca++ levels outside the cell?: how much Ca++ u might have..
—> what might limit entry into the cell?: fewer L-type Ca++ channels opening, less Ca++ influx, less contraction
Sarcomere length (overlap of thick and thin filaments) ALSO affects force of contraction
similar to the length-tension relationship
According to the Frank Starling Law, the heart must pump all the blood that returns to it AND its force of contraction is partially determined by how much blood is arriving to it (and it is stretched by venous return) at any given moment
→ more venous return leads to increased stretch of the heart chambers, which causes better alignment of thick and thin filaments and increased force of contraction
→ less venous return leads to the opposite conditions and effect on contractile force
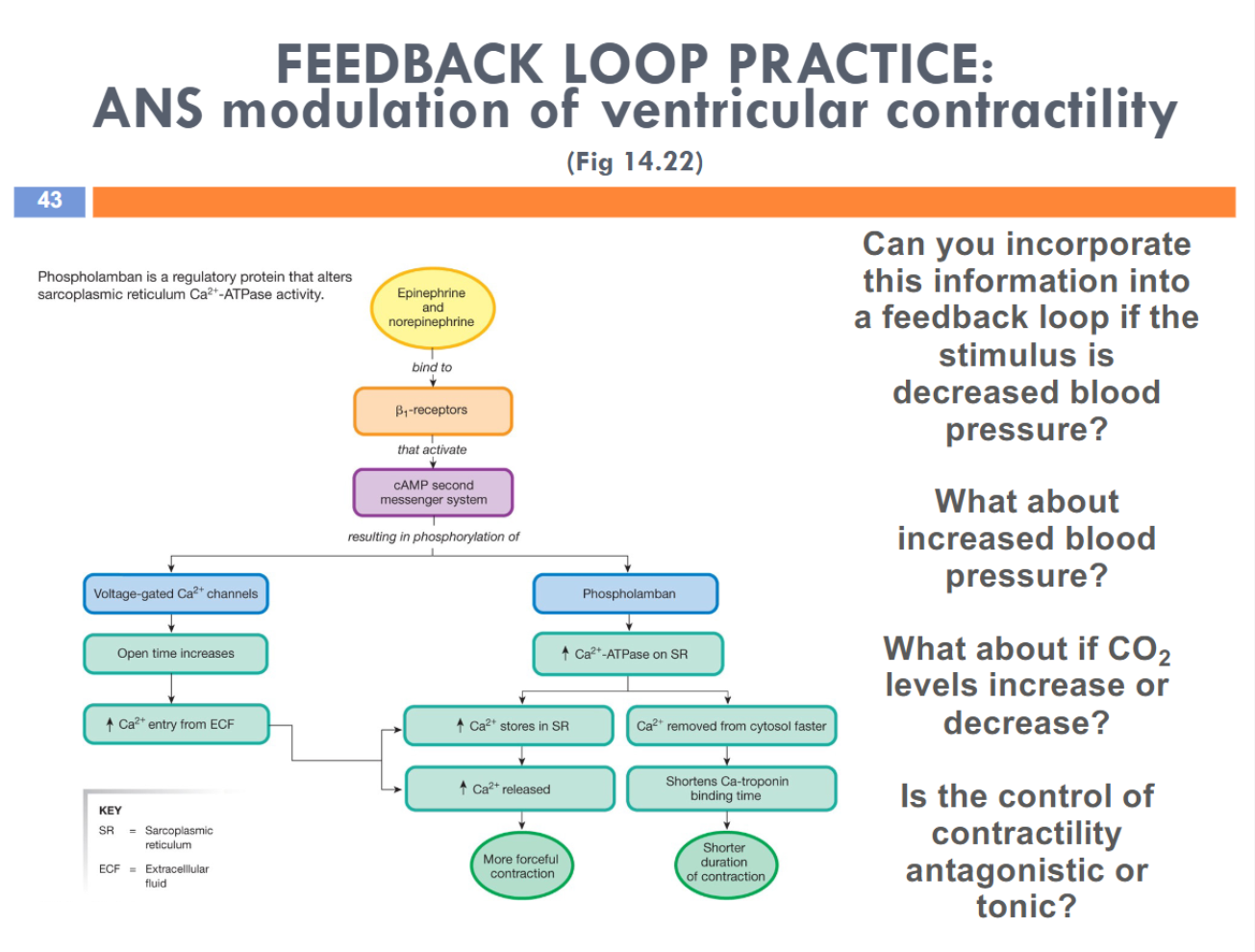
control of contractility is tonically controlled
