NCLEX need to know topics - OB
1/71
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
72 Terms
Presumptive and probably signs of pregnancy:
Presumptive signs of pregnancy: missed period, n/v, breast tenderness, & quickening (first fetal movements felt between 16-20 weeks).
A positive pregnancy test is a probable sign of pregnancy, along with Chadwick's sign (a bluish-violet or purplish discoloration of the cervix, vagina, and vulva that starts/shows up as early as 4 weeks), Goodell sign (good and soft cervix), and Hegar sign (uterine softening)
Timing of Prenatal Visits:
One a month until 28w
Every other week between 28w and 36w
Once a week after 36w (at 42w, delivery should be induced or by c-section)
Station
relation b/w fetal presenting part and the mother’s ischial spines. Once the baby hits 0, they are engaged.
PCOS: causes? tx?
Causes ovarian cysts, irregular menstrual cycles, weight gain, insulin resistance, and infertility.
Clomiphene citrate treats infertility.
The client should receive a transvaginal ultrasound and monitoring for ovulation and hyperglycemia.
PCOS increases the risk for type 2 diabetes mellitus and cardiovascular disease.
1st Stage of Labor key fx
Dilation & Effacement
Latent: 0-5 cm, mild contractions
Active: 6-8 cm, moderate contractions Q2-3min
Transition: Rapid progression to 10cm, intense contractions Q1.5-2min
Interventions: rest, ambulation, pain mgmt, emotional support, breathing techniques
2nd & 3rd Stage of Labor key fx
Delivery of the baby - Encourage pushing, monitor fetal descent, and assist with the delivery
Delivery of the placenta - Ensure fundus is firm & monitor for hemorrhage
4th stage of labor key fx
Recovery & Stabilization
1-4 hours postpartum
Assess these 4 things Q15m: fundus, lochia (roll PT to see underneath her too), & VS
Encourage skin-to-skin and breastfeeding
The height of the fundus after delivery should be at what? descent?
umbilicus (or naval)
It involutes about 2cm every day PP
Risk factors for cervical cancer include:
Multiple sexual partners, Multiple pregnancies
History of HPV and/or STIs (chlamydia) & Insufficient HPV vaccination
Long-term oral contraceptive use
Cervical Cancer tx options and key fx of each
A hysterectomy is recommended when the client does not desire pregnancy. This removes cancerous cells and prevents spread.
Internal radiation causes vaginal fibrosis, dryness, and scarring. Vaginal lubricants are recommended to decrease vaginal pain during intercourse after internal radiation.
Cryosurgery involves freezing abnormal cervical cells and can cause heavy, watery-brown vaginal discharge that can last several weeks. This is a normal part of healing
A LEEP involves removal of abnormal cervical cells using a heated wire loop. Cramping and mild bleeding are common side effects
Conization can lead to preterm delivery but does not cause infertility. Procedures that remove cervical tissue (e.g., conization, LEEP) weaken the cervix, potentially causing cervical incompetence which can affect the client’s ability to carry a pregnancy to term. However, pregnancy can still occur.
gonorrhea key fx
an STI that is often asymptomatic and can lead to PID
PID s/s? education?
a bacterial infection causing lower abdominal pain, dysmenorrhea, scarring of the fallopian tubes, and infertility.
Getting rest
Completing antibiotics
Avoiding intercourse until infection has resolved
Obtaining endocervical cultures post-treatment
chlamydia increases the risk for what during pregnancy? tx/priority?
chorioamnionitis - requires prompt antibiotic treatment.
The known infection should be treated to prevent chorioamnionitis before addressing augmentation or pain.
This would still be priority over a FHR strip with minimal variability, as this can be benign, like from the baby sleeping (as long as there’s no other symptoms/decels).
Tx for this (administering abx) would also be priority over starting an oxytocin infusion, even if FHR is showing early decelerations
Ectopic pregnancy teaching includes:
The client is at risk for rupture and life-threatening hemorrhage. Rupture causes bleeding in the peritoneum, resulting in sudden, sharp abdominal pain; referred shoulder pain; and Cullen sign.
Avoid analgesics stronger than acetaminophen to avoid masking symptoms of tubal rupture.
Ectopic pregnancies are non-viable.
Pregnancy is possible with one fallopian tube, but should be avoided for ≥3 cycles.
Rh-negative clients receive Rh immune globulin to prevent isoimmunization.
Chlamydia, gonorrhea, and previous ectopic pregnancies increase risk.
Teach clients that frequent β-hCG monitoring is needed to confirm pregnancy termination.
Avoid sexual intercourse until β-hCG is undetectable
Prolapsed cord
risk factors? s/s? interventions?
There is an increased risk for a prolapsed umbilical cord if the fetus is in a malpresentation (ex: breech), not engaged/negative station, or if there is polyhydramnios.
It is characterized by fetal heart rate (FHR) decelerations, fetal bradycardia w/ minimal variations, most frequently following membrane rupture (e.g., amniotomy).
If prolapse occurs, position knees-to-chest or in Trendelenburg and lift the presenting part with a sterile gloved hand to relieve cord compression. Do not push the cord back in.
Increase IV fluids and prepare for a fetal scalp electrode placement.
amniotomy: ensure what beforehand?
confirm the fetal head is engaged (0 or positive station)
“LION” interventions for tetany, maternal HTN, vena cava syndrome, toxemia, uterine rupture, low fetal HR, low baseline variability, late decelerations, etc:
Left Side, IV, Oxygen, and Notify HCP. Stop Pitocin if it is running - the first thing to do! If stopping oxytocin isn’t an option, the first thing you do is turn the PT on their left side.
Variable decelerations interventions
The nurse should assess for umbilical cord prolapse and initiate intrauterine resuscitation. It is treated with discontinuing oxytocin, repositioning, and amnioinfusion.
Early decelerations interventions
They can be documented as normal. The nurse can assess cervical dilation and prepare for delivery as needed.
Fetal tachycardia is commonly caused by what?
maternal fever and should prompt the nurse to assess maternal temperature
In clients with PPH caused by uterine atony, administering what is the priority?
uterine stimulants (e.g., methylergonovine)
even over giving RBCs
Oxytocin & Preeclampsia Priorities to Monitor:
Oxytocin has antidiuretic effects.
Prolonged oxytocin use increases water intoxication risk due to water retention.
Preeclampsia causes decreased renal perfusion and can lead to magnesium toxicity.
Monitoring urinary output is the priority.
headaches after what week gestation indicate a pregnancy complicaton
persistent headaches after 26 weeks gestation accompanied by hypertension could indicate a pregnancy complication such as gestational hypertension or preeclampsia
Symptoms of preterm labor & PT teaching/interventions:
Manifestations of preterm labor include constant, mild lower abdominal cramps; cervical changes (“bright pink vaginal spotting” from effacement/thinning); diarrhea; rupture of membranes (“PT states episode of urinary incontinence”); and pelvic pressure.
Teach clients with contractions or backache occurring <37 completed weeks to stop activity immediately, lie down on their side, hydrate, and notify HCP after 1 hour if there is no improvement in PTL symptoms.
When pre-term labor is suspected, what interventions does the nurse perform?
Assessment of uterine contractions, cervical changes, and fFN (fetal fibronectin) test should be performed. As well, rest and limited physical activity are often recommended
Administering betamethasone is administered IM to clients <34 weeks gestation at risk for preterm delivery within 1 week or in labor. It is a steroid, so it can increase glucose.
For active PTL, administer tocolytics (terbutaline, magnesium sulfate, nifedipine, indomethacin) to slow or stop uterine contractions. Give Magnesium sulfate for neuroprotection.
Sympathomimetic drugs (e.g., cocaine) increase what?
uterine contractility and precipitous labor risk.
Prolonged contractions? cause what?
Prolonged contractions cause fetal hypoxemia and increase the risk of placental abruption and uterine rupture. Therefore, if a PT has them, it is a priority.
Uterine contractions should be no longer than 90 seconds and no closer than 2 minutes
They prevent uterine rest and placental reperfusion.
Precipitous labor increases the risk for:
Perineal tears
Uterine atony
Postpartum hemorrhage
Retained placenta
With precipitous labor, the nurse should:
Prepare the delivery table
Attach a tocodynamometer
Obtain an order for methylergonovine to prevent PPH
Obtain a type and screen for potential blood replacement
Nursing interventions for painful back labor caused by an Occiput Posterior (OP) fetal position:
Position (Knee-Chest): Have the mother get on her hands and knees in a "knee-chest" position to use gravity to rotate the baby and relieve pressure off the sacrum.
Push (Sacral Counterpressure): Take the heel of your hand or your fist and push firmly directly into her sacral area to provide counterpressure and alleviate the intense back pain.
should the mother push during contractions with shoulder dystocia?
NO
How to prevent newborn respiratory depression r/t opioid and epidurals
avoid administering opioids if delivery is expected within 4 hours
before epidural placement, preload with 500- 1,000 mL IV fluids to prevent hypotension.
If a mom who recently got an epidural calls out with nausea and lightheadedness, these are signs of what? action?
epidural-induced hypotension, and the priority action would be to increase the IV fluids.
PPH risk factors include:
Precipitous (fast; <3 hours) labor
High parity (# of pregnancies; 5 or >)
Macrosomia
Bladder distension
Perineal trauma (episiotomies and lacerations)
History of uterine atony
Chorioamnionitis manifestations include? tx?
Uterine tenderness, Fever, maternal and fetal tachycardia, & Strong-smelling discharge
The nurse should: Administer ampicillin (broad-spectrum IV abx), Obtain a WBC, and Monitor maternal temperature and FHR.
what are the conditions in “Other” in the TORCH infection acronym? key fx of each r/t interventions/treatment/screening/risks?
(e.g., HIV, Hepatitis B, Group B Streptococcus [GBS])
HIV: If viral load is high, mother must deliver by cesarean. Breastfeeding is contraindicated. Bathe the newborn immediately after delivery, if stable. Administer ART to newborns within 12 hr of birth and teach the importance of follow-up testing.
Hep B: Administer hepatitis B immune globulin (HBIG) and hepatitis B vaccine to newborns of affected mothers within 12 hr of birth.
GBS: Screen clients at 35-37 weeks with vaginal-rectal swab. If mother is GBS-positive or unknown, administer IV antibiotics during labor. Newborn risks: Sepsis, pneumonia, meningitis, death.
how is cytomegalovirus spread? key teaching? s/s?
CMV is spread by saliva and urine. Emphasize hand hygiene during pregnancy, especially when handling diapers or saliva from young children.
CMV can be asymptomatic but is the most common non-genetic cause of sensorineural hearing loss. Newborns exposed to CMV will require hearing screenings to monitor for hearing impairment. CMV complications can also include microcephaly, hepatosplenomegaly, purpuric rash, epilepsy, and cognitive impairments.
key fx of herpes simplex virus in pregnancy & birth
For clients with a history of HSV, administer suppressive therapy (acyclovir) during the last
trimester to prevent an outbreak. Treat infected newborns with IV acyclovir.
If vaginal lesions are present, mother must deliver by cesarean. Avoid breastfeeding if there are active breast lesions.
uterine rupture s/s? risk factors for it? interventions?
Characterized by abdominal pain, abnormal FHR, uterine tachysystole, prolonged decelerations, weakening/cessation of maternal contractions, and vaginal bleeding. If a mom states she has new abdominal pain, her stomach is soft, and there is loss of fetal station → emergency b/c its signs of uterine rupture.
The #1 risk factor for uterine rupture is laboring after a previous cesarean delivery or other uterine surgery.
Clients attempting vaginal birth after cesarean section (VBAC) have an increased risk for uterine rupture
Emergent cesarean section is required to safely deliver the fetus as the uterus cannot effectively contract.
placenta previa s/s? interventions?
PAINLESS bright red vaginal bleeding. If d/c home, the PT should be taught to notify the provider if they even have a small amount of painless bleeding and to limit activity/strain on the body.
Clients with placenta previa require pelvic rest, which includes no intercourse, no vaginal exams, and no labor. Administer steroids in anticipation of premature delivery if <34 weeks gestation.
placental abruption s/s? risk factors? tx?
abnormal FHR, abdominal pain, firm abdomen, and dark vaginal bleeding.
Increasing fundal height indicates concealed bleeding from placental abruption and requires emergent delivery.
Hypertension can lead to placental abruption
A postpartum client with continued excess uterine bleeding related to DIC should be prepared for what intervention? nursing actions?
a hysterectomy.
The nurse should notify anesthesia and administer blood products, an IV fluid bolus, and oxygen.
what is a classical uterine incision? key fx?
up and down
cannot have a vaginal delivery after one
Incompetent Cervix tx
Prepare client for a cervical cerclage if <23 weeks gestation to keep the cervix closed. Removed at 36 weeks gestation or when labor begins.
When fetal bradycardia is a concern, the nurse should:
Verify maternal pulse, Obtain blood glucose, & Assess for recent viral infections.
what are Epstein pearls
Palatal cysts of the newborn, which are small white or yellow cystic vesicles. This is normal.
what is erythema toxicum neoratorum
Pink rash with firm yellow-white papules or pustules on the face, chest, abdomen, back, and buttocks. Usually appear 24-48 hours after birth and disappear in a few days.
what is Gastroschisis? complications? priority? tx?
A congenital defect where an infant is born with abdominal organs outside the body.
Gastroschisis complications include hypothermia, infection, and dehydration.
A priority assessment to monitor for would be sunken fontanelles
Bowel decompression is implemented with an NGT & suction
Abdominal contents should be loosely covered in moist gauze or plastic.
To prevent kernicterus (permanent brain damage), immediately notify the HCP of any jaundice occurring when? s/s? Interventions?
within 24 hours of birth
infant will present with opisthotonos position (hyperextended posture → emergency). If the newborn is in this position, put them on their side.
encourage feeding ≥8 times/24 hours to ensure hydration and help reduce bilirubin levels through excretion in stool and urine
when do you adiminister rhogam
to all Rh-negative mothers at 28 weeks and again within 72 hours of birth or any sensitizing event
Placing newborns <__ weeks in a polyethylene bag prevents heat loss by evaporation and is the BEST option to support thermoregulation
29
When caring for premature infants:
Use skin protection barriers between the tubing and the skin. Secure NG tubing to the cheek by padding the skin with a hydrocolloid dressing or wafer underneath the tube.
Ensure visualization of IV sites - Leaving the arm with the VAD unswaddled allows visualization of the VAD site to monitor for complications.
Use pressure reduction devices - A small gel pillow underneath the infant’s head relieves pressure at the occiput, which is more prominent in infants and young children. Pressure reduction devices (e.g., pillows) at bony prominences prevent pressure injuries in infants with decreased mobility.
Use water and gauze to remove adhesives - Alcohol dries and irritates a premature infant’s skin.
Postpartum and post-hysterectomy education:
Routine pap smears are no longer required
Prophylactic enoxaparin is continued for 6 weeks postpartum due to the history of pulmonary embolism
Hormone replacement is unnecessary since the ovaries remain intact
PP baby blue symptoms persisting >10 days indicate possible postpartum depression and require follow-up
Notifying the provider about bowel and mood changes >2 weeks
Avoid driving for 2 weeks post-surgery to allow incisional healing.
Avoid lifting anything heavier than your baby for 6 weeks
Menstruation cessation & need for protein increase in diet
A client with mastitis is at the highest risk for developing what?
an abscess
Manifestations of worsening Neonatal Abstinence Syndrome include:
Poor sleep (ex: only 1.5 hours of sleep between feeds)
Excessive suck (ex: drinking 60mL in 7 minutes)
High pitched cry, Loose stool, Tight tone (ex: no head lag), & Skin excoriations (ex: chin redness)
Newborns with fetal alcohol syndrome (FAS) intervention
they are easily overwhelmed by sensory input. Eye contact can be overstimulating and cause the newborn to struggle with feedings. Therefore, caregivers should provide a calm environment and avoid eye contact during feedings
Assessment data indicative of hip dysplasia includes the following:
tx?
extra or asymmetrical thigh/buttock folds; hip instability, clicks, or pops (i.e., positive Barlow or Ortolani tests); decreased hip abduction movement (noticed when changing diaper); pain/discomfort; and lordosis/swayback posture
the goal of medical management for this condition is to ensure the ball of the hip remains in the socket to facilitate normal growth of the joint and often includes the use of bracing, a closed reduction and casting, or an open reduction and casting.
DDH: Pavlik harness use involves keeping the client’s legs flexed and thighs abducted. Caregivers should avoid applying lotions and powders under the straps and dress the infant in clothing (T-shirt, onesie) and a single diaper to prevent skin irritation.
molar pregnancies s/s? interventions?
Molar pregnancies present with dark brown vaginal bleeding with grape-like clusters that fill and enlarge the uterus and can present on the perineal pad, causing it to resemble a more advanced pregnancy (fundal height being higher than expected & uterus larger than expected).
Serum beta-human chorionic gonadotropin (β-hCG) levels rise dramatically, resulting in hyperemesis gravidarum
After removal of molar pregnancy (which should be asap), monitor β-hCG levels for up to 1 year to assess for malignancy. Teach client to avoid pregnancy until malignancy is ruled out and to not use an intrauterine device (IUD) for contraception.
Care for pregnant clients with HIV includes:
Delivery of choice, depending on viral load
IV antiretrovirals (even if laboring)
Avoidance of breastfeeding
Immediate newborn bathing and antiretroviral administration
newborns delivered by cesarean are at risk for what
transient tachypnea of the newborn
key fx of interventions after forcep/vacuum use
Suspected broken clavicles require x-ray confirmation.
Facial asymmetry results from intrauterine pressure, requiring no intervention.
A cephalohematoma requires bilirubin monitoring. It occurs within 24-48 hours after birth.
Scleral and retinal hemorrhages resolve within 10 days without intervention.
This client has absent fetal heart tones (FHT) on transvaginal ultrasound, a closed cervix, and no vaginal bleeding, which means no fetal tissue has passed, indicating what? Interventions?
missed miscarriage
The nurse should educate the client about misoprostol, a tablet inserted intravaginally that promotes cervical dilation and uterine contractions to aid in expelling fetal tissue. In addition, surgical removal by dilation and curettage can also be done.
For a successful vaginal delivery, the fetus should be in ___ position (i.e., parallel with maternal spine), ____ (i.e., chin to chest), and ______ (i.e., head down) presentation.
vertex, flexed, cephalic
facial presentation key fx
occurs when the fetal head is fully extended, requiring immediate intervention (e.g., emergent cesarean section)
delivering vaginally can cause trauma, spinal cord injuries, fetal distress, and demise.
what is uterine dysfunction? actions?
Uncoordinated contractions occur in the middle of the uterus and fail to cause cervical change prolonging labor and causing exhaustion (ex: PT is 3 cm dilated after 7 hours of labor but has strong contractions occurring every 1.5 minutes)
Actions: Facilitating rest encourages the coordination of contractions and transition to active labor. Nurses promote rest with hydrotherapy (e.g., showering), analgesics (e.g., morphine), or zolpidem (Ambien). The risk for hypertonic uterine dysfunction increases in primipara clients (i.e., first pregnancy) and those experiencing anxiety, as relaxation is difficult.
After passing the initial meconium, newborns should have ≥___ stools daily
3-6
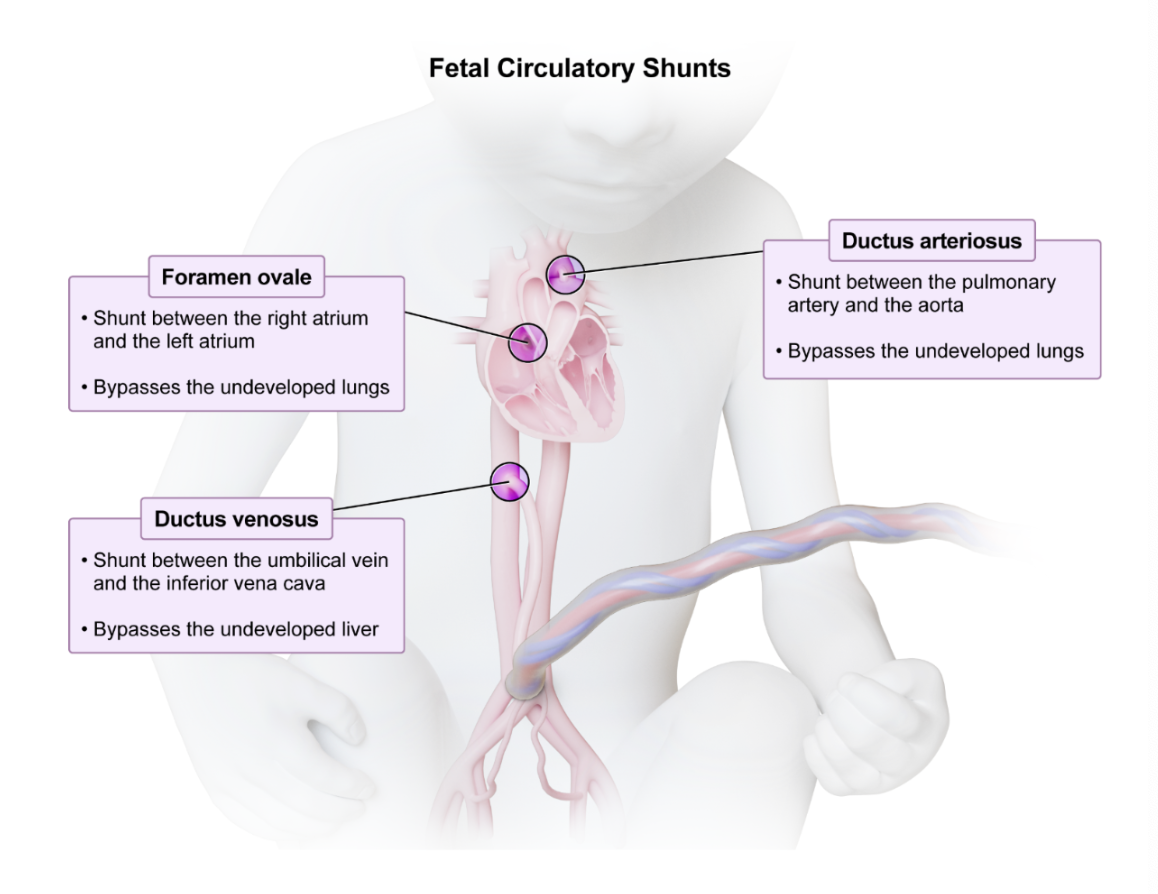
fetal circulatory shunts key fx
Breast care when breastfeeding
Wear a supportive, wireless bra to prevent clogged ducts and mastitis.
Use analgesics and ice to manage breast discomfort.
Place cabbage leaves on breasts to relieve engorgement - Limit use to 15-20 min for breastfeeding
mothers to avoid decreasing milk supply.
Eat an additional 450-500 calories while breastfeeding
For exclusively formula-feeding clients, suppress milk production by:
avoiding breast stimulation:
No pumping or massaging breasts; instead, hand express small amounts of milk for pain relief.
No warm water on the breasts
Rapidly increasing head circumference, persistent downward gaze (“sun-setting” sign), and high-pitched cry are signs of ______ in infants.
hydrocephalus
Any postmenopausal vaginal bleeding should be evaluated for..?
endometrial cancer
endometritis s/s? interventions?
Causes fever, foul-smelling lochia, and inflamed tissue, resulting in uterine pain and tenderness upon palpation
Interventions for endometritis include:
Administering IV antibiotics, antipyretics, analgesia
Positioning in Fowler’s position, Providing cold compresses, & Assessing vital signs