A & P 3: Exam 2
1/110
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
111 Terms
Adult Body water
45-60% water
Content varies between tissues
Bone: Low = 22%
Fat: Low = 10 %
other Typical Tissues 70-80%
Obesity: low water content
S#x: females have higher content
Age: The older the dryer
Infant: High percentage 75%
Water compartmentalization % of Total Water
Intracellular Fluid: 65%
Extracellular fluid: 35%
Interstitial Fluid: 25%
Plasma & Lymph = 8%
Others (CSF, Synovial joint, Eye circulation) = 2%
Osmolarity
Total Solute Concentration = 300 mM
Chug water: osmalarity goes down
Salty food: Osmolarity goes up
ICF = ECF
Plasma Osmolarity > Interstitial fluid Osmolarity
Solute composition in ECF & ICF
ECF:
Sodium (Na) = 145 mM
Chloride = 103 mM
Potassium (k) = 4mM
ICF:
Sodium (Na) = lower
Chloride = lower
Potassium (k) = higher
Osmosis
Special case of simple diffusion
Includes:
Isotonic = 300 mM (regular body) (no net exchange)
Hypotonic < 300 mM (chugging watter)
Hypertonic > 300 mM (salty food)
Water goes from high to low water
350 goes into 300
Water Budget in Body Inputs
Typical Daily Turnover ~ 2500 mL/day
Inputs:
Drinking & Eating = 2300 mL/day (8 glasses og H2O per day = preformed water) can change ex: eating watermelon ↑
Metabolic Water Production
200 mL/day
Equation of life: O2 + Fuel → CO2 + ATP + Heat + H2O
Another form of water production per day made by body
can make more by eating & drinking (needed)
Water Budget in Body Output
Sensible (sweating) Perspiration ~ 100mL/day
sweating via sudoriferous glands
eliminates heat by evaporation
controlled by Thermoregulatory center (in hypothalamus)
Variable:
increases with heat and activity
blood is now diluted
Insensible Perspiration
Sweat from the lungs (Respiratory water loss) or skin (Transcutaneous water loss)
700 mLDay
RWL is high in cold and dry activity
when when breath cold air we need to warm it up with water
Skin is gonna be highest when its hot and dry
dryness evaporates water off from skin
Air is Desicatting (more dry than you)
Saltwater = lose water (dehydrated swimming in ocean)
Freshwater = gain water
Fecal water lost
Fecal matter is ~ 70% watr
lose abt 200 ml/day (inevitable)
KIdney
lose about ~1500 mL/day
decreases w/ dehydration (vice versa)
possible to overhydrate (can lose goodies)
cannot make water but can preserve/conserve it to minimize lost of water
Fluid imbalances: Dehydrated
input of water < output of water
leads to hypovolemia → hypotension (low pressure)
pressure always follows volume
loser more water than salt
Can lead to hypetonic plasma &
Cardiovascular system increases Arterial Pressure (Acute/Short term)
Kidney (long term): takes longer to filter
Ultimately requires: behaviour (hormones change, makes us thirsty abd seek out water)
Hypertonic plasma
Happens when the body sweats so we lose more water than solutes
(drink water w/ a little salt) to balance
Fluid imbalances: Overhydration
Input > Output
Leads to:
Hypervolemia -» Hypotension
dilutes the plasma (hypotonic plasma < 300 mM) & blood (swells up the cells) CAN DIE FROM THIS
Input isn’t regulated by the body: have to pee it away
overworks kidneys
Drinking 1L of water: gut absorbs all of it
Compensation:
Acute: Cardiovascular can minimize pressure increases
Chronic: Kidney rapidly eliminate excess water
Renal System
Balances water: Renal Regulates & Balances Blood Volume & Pressure
Balances Individual Ion Concentrations & Total Osmolarity (sodium, chloride, calcium, potassium, magnesium, hydrogen, bicorbonate)
Eliminate Wastes from Blood
Directly Regulates Plasma
Indirectly Affects All ECF Composition and Volume
Produces hormones:
EPO (Erythropoietin)
activates Calcitriol (Vitamin-D Pathway & Calcium Homeostasis) ON EXAM
Structure of the kidney
Very small up to 1% of Body Mass
blood flow is exceptionally high here (16-20% of Cardiac Output)
high mass metabolic rate (not propotionate)
one of the most active organs per gram
doesnt use as much oxygen as brain
Inputs & Outputs:
Renal Artery (Major input)/ Vein (output)
Ureter→ drain vein to bladder
Efferent/Motor Nerves:
Lymphatic Drainage: fluid out
Adipose Padding: Mechanical Protection
Nephron
The functional unit of the kidney & reabsrobs ~ 99%
includes: corpuscle + tubule
Associated Vasculature: (in it’s order of flow)
- Afferent Arterioles
- Glomerular Capillaries
- Efferent Arterioles
- Peritubular Capillaries (surrounds tubule, has net reabsroption)
- Renal Venules
Kidneys general abt 100 mL per min and reabsorbs
includes Portal System: 2 capillary beds in series (#2 OF 3)
Corpuscle Function: Nephron
a capsule that has the glomerulus (a modified capillary) that produces filtrate
goes down the tubule for processing
Two ways:
1) Reabsoption: reabsorb fluid from tubule then reabsorb in pertubular capillary & secretes some of it into interstitium into the tubular filtrate
what isn’t reabsorb will go into the urine
2)
Reabsorption: Tubule Filtrate à Interstitium
à Peritubular Capillaries
- Secretion: Peritubular Capillaries à Interstitium
à Tubule Filtrate
- Excretion: Final Product = Urine
Filtration by Glomerulus equation
The plasma is filtered to the capsular space across the filtration membrane
the rate filtration that is formed by both kidneys abt 100 ml/min
Rate of Filtation = Glomerular Filtration Rate
GFR (mL/min) Proportional to: Kf Net Filtration Pressure (NFP) * Renal Plasma Flow (RPF)
GFR (mL/min) Proportional to: Kf * [(Pglomerulus – Pcapsule) – (πGLOMERULUS – πCAPSULE)] * Renal Plasma Flow (RPF)
Kf = Glomerular Filtration Coefficient = HIGH = (High Surface Area & High Hydraulic Conductivity) very leaky due to gaps
Net Filtration Pressure (NFP) = Outward Hydrostatic > Inward Osmotic Pressures
fluid from filtration is > than fluid from reabsorption
typical capillary = 0.1% (60 mmHg)
renal plasma flow @ rest = 20% (High Filtration Fraction = Kf * NFP)
high glomerular pressure in comparison to typical capillaries
High osmotic reaborption due to reduced Filtration of moderately sized proteins
These forces offset each other: Typical Glomerular NFP = 10 mmHg
Result: High Filtration Fraction
Result: GFR is High (110 mL/min)
GFR = Filtration Fraction = Renal plasma Flow
Measures of Renal Filtration at rest ON EXAM very important
Cardiac Output
5 L/min
Renal Blood Flow (RBF)
20% of cardiac output A rest = 1L/min
Renal Plasma Flow (RPF)
55% of RBF
RBF = 0.55 L/min = 550 mL/min
Glomerular Flitration Rate GFR
total filtrate formation in both kidneys
110 mL/min (lots of fluid)
Total Plasma Volume filtered every 25 mins
Filtration Fraction
GFR/RPF = 20% typical
GFR = RPF x FF = RPF x (NFP x Kf)
GFR = RPF x (Pglomerulus)
Rate of Filtration by Glomerulus
filtratiom membrane includes the capillaries
the basement membrane includes the visceral capsule which have podocytes on them which allows selective filtering
plasma comes out of blood but NOT plasma proteins
Selective filtration of the glomerulus
Selectively limits what is filtered and restricts movement accross filtration membrane so that we don’t have to reabsorb it!
formeed elements: Medium/Large Plasma Proteins: (Albumin, Glbulins, Fibrinogen)
Complement & Antibodies
Medium/Large Anions
Size and negative charge/Hydrophobic solutes bound to plasma protein (thyroid hormones)
clotting factors stay in the blood
Non-selective filtration by glomerulus
Things that get filtered
Small things (positive & negative) always get filtered into the filtrate
ex: glucose, free amino acids, ions (Na, K, Cl, Ca, H+, HCO3-, Phosphates, Sulfates)
only POSITIVE medium cations things are filtered
Toxins, waste products (urea, urobilinogen, etc)
free hormones like (ADH, oxy, ALD)
Large things NEVER filtered
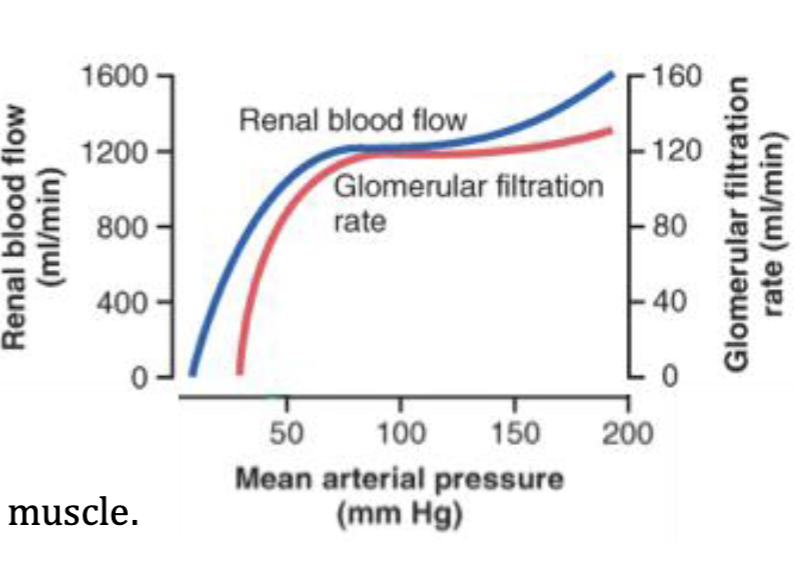
Changes in Glomerulus Filtration Rate
1) Arterial Pressure
“autoregulation” minimizes changes in renal blood flow and glomerular pressure despite changes in arterial pressure
showcases that → Glomerular pressure is CONSTANT! despite arterial pressure unless it is going down
Autoregulation of GFR
Has two ways
1) Myogenic mechanism = intrinsic property of smooth muscle
resists large sudden changes in blood flow
ex: walking with your hands → blood rushes to brain w/vasodilation = alkalosis (trys to maintain pressure however)
2) Turbuloflomerular Feedback from Juxtagolumerular Appartatus
Adjusts GFR to medoerate and constant level under normal conditions
Exception: Arterial Hypotension
GRF decreases dramatically
reflects decrease in golmerular pressure causing dramatic decrease in urine production
urine is proportional to arterial pressure
Severe hypertension?: no increase of GFR
urine can still increase
can lose viable solutes
Sympathetic stimulation of Renal Activity
Stimulation inhbits renal activity
ex: exercise causes alpha-1 vasoconstriction of Afferent arterioles (decreases capillary pressure + NFP + filtration fraction) which is below 20% at resting
decreases renal blood flow/renal plasma flow
maintains arterial blood pressure to supply active heart and skeletal muscle
decrease Pglomerulus → decreases GFR
Sympathetic stimulation w/ a Hemmorrhange
Maintains sufficient blood pressure to perfuse other organs
depends on how hydrated you are
lower GFR
due to Alpha-1 vasoconstriction of afferent arteriole
efferent arteriole dilation is due to lack of SNS not activation PSNS
osmolarity changes a little, decrease in volume
Processing of flitrate in the tubules
The filtrate is a combination of Good and bad things,
Keeps good solutes (reabsorb) and gets ride of bad solutes (not reabsorb)
both will enter the urine
Primary Tubule Segments
Divided into 5 segments
Proximal Tubule
Loop of Henle which includes (thin Descending loop and thick Ascending loop)
Distale Tubule
Collecting duct (tubule): does process
Papillary duct: No processing occurs here
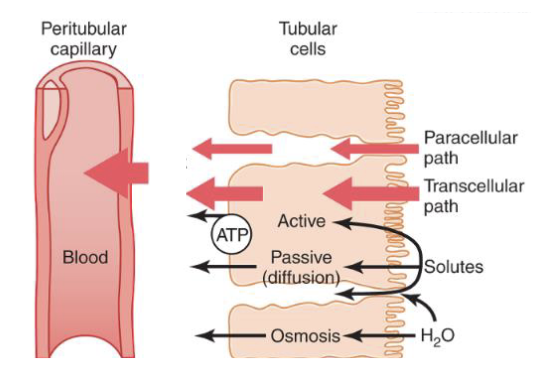
Reabsorption of
Most filtered solutes are reabsorbed (99%)
Goes from the filtrate in the tubule, reabasorbed in thto the peritubular capillaries → across the tubular epithelium, to the interstium (intersgtital fluid)
this process requires a Transport Across Tubule Epithelium (2 types)
1) Transcellular
2) Paracellular
Transcellular reabsorption Transport
Crosses both luminal (apical) and Basolateral (basal) membrane causing reabsorption
does this with carrier proteins and channels which is driven by sodium/potassium ATPase (on basal membrane
drives sodium transport on apical membrane
soidum potassium ATPase is found on the basal membrane and we co-trans with this a lot
an example of transcytosis
Transcytosis
Slow and metabolically expensive
are subject to saturation
Paracellular
sneaking between epithelial cells
has loose jundctions of some tubules allows this type of passive diffusion
often driven by gradients created by transcellular mechanisms
Good solutes
the solutes that are filtered from the blood and returned/filtered to the blood
most are good, if not filtered no problem, stays in the blood
- ex: formed elements + Plasma proteins (albumins)
If it is freely filtered it must be reabsorbed
low amt of solutes are good
Typical Hydration: 99% Reabsorption
Bad solutes
wastes, toxins and excesses are NOT reabsrobed = remains in tubular fluid (capillaries) and excreted into the urine
excess solutes are bad
Dehydrated
water is reabsorbed more completely: Increases to 99.9% Reabsorption
- Urine Flow Rate Decreases = 0.01 ml/min
- Results in Concentrated Urine Solutes (lots od wastes) = Increased Specific Gravity
- Maximum [Urine] = 1200 mOsm
increases in osmolarity
more water is lost than solutes
decrease in volume
Overhydrated
Water is now bad means decrease in reabsorption
- Ex. 90% Reabsorption
- UFR = GFR x 10% = up to 10 mL/min
- Diuresis:
decrease in osmolarity, increase in volume
Normonatremia
where 99% Filtered Sodium is reabsorbed
1% lost of avg
normal volume and osmolarity
Hypernatremia
is an excess Sodium Consumption causing Sodium to be “Bad”
Decrease % Reabsorbed to = 98% Reabsorbed (usually 99% so this # is stil high)
usually we pee it away and dont retain it
results in Natriuresis: increases sodium excretion causing a secondary diuresis (bc water follows salt)
increase in volume, increase in osmolarity in blood
Hyponatremia
When sodium levels are low
majority of sodium is now vastly reabasrobed → increases back to 99.9% reabsorption
Free water soluble Hormones
also eliminated by the kidney on the regular
Are freely filtered (has a short half life b/c not reasborbed)
Larger Protein Hormones Filtered at Lower Rates = Moderate half Life.
why? we dont want the hormonal effect forever
if we need more hormones we can make it
small hormones are filtered easier
hydrophilic (water loving) = secreted easier
Hydrophobic Hormones Bound to Plasma Proteins
Only free Fraction can be Filtered and Excreted.
Lost in Urine at Relatively Lower Rate = Longest ½ Life.
ex: thyroid hormone
bigger/hydrophobic hormones are harder to secrete
Osmosis
The reabsorption of most water
across tubular epithelium into → interstitium → across peritubular capillaries
water follows reabsorbed solutes (follows salts/solutes) = lower to higher osmolarity
tubular fluid equilibrates with interstitium
some tubule segments ar enot water permeable and this wont take place there
Secretion
frome the peritubular capillaries pumped into the filtrate
how we get rid of stuff, putting it into the filtrate and out into the urine
peritubular capilaries → interstium → across epithelium → filtrate
via carrier mediated transport (very specific stuff only)
can include “bad stuff”: wastes, toxins, & excesses/too much acid (we dont want things to accumulate)
must be secreted if not filtered by glomerulus
or secreted in addition to being filtered = filtered + secreted
Excretion of urine
what is lost in the urine
filtered - reabsorbed + secreted
always includes some water (we cant pee chunks)
Urine Flow Rate (UFR)
UFR = GFR x 0.01 (1%) what is peed away
ex: UFR = 110mL/min (0.11L/min) x 0.01 = 1.1 mL/min (remember units b/c TESTED)
higher GFR → generally higher UFR
% of reabsoprtion varies depending on hydration
Solute excretion
Leads to inevivatble water extcretion
called secondary diuresis
ex: natriuresis → diuresis
water follows solutes
Peritubular Capillaries
Reabsorbs solutes and water from interstitum
all good stuff from tubules
lots of solutes and water
everytime solutes are being reabsorb, water follows via osmosis
Mechanism for Peritubular Capillaries
Blood within efferent arteriole goes in
drops in peritubular pressure (low) and increases osmotic gradient (high
Normal blood = 20% filtrate
High plasma proteins
low pressure
net filtration pressure (NFP) = negative
oxygen levels: high, due to passive filtration
Why are fluid balance challenges “complex”?
becauase the body must regulate both osmolarity (solute concentration) and volume/pressure at the same time, using different systems
body uses seperate receptors for volume and osmolarity b/c they measure diff problems and allow body to respond more precisely to each
when receptor detect a change it sends signals that trigger appropriate physiological responses depending on situation
complex bc it involved 4 diff hormones and different mechanism in different kidney tubule segments
each hormone acts on diff parts of the nephron to adjust fluid and electrolyte balances
Baroreceptors
Helps detect changes in volume and pressure in the kidneys, arteries and the heart
What detects osmolarity
Osmoreceptors in the hypothalamus
regulating volume and osmolarity is not enough, addition regulation is required
ions like Na⁺, K⁺, Cl⁻, Ca²⁺ and pH (acid-base balances)
ions affect nerve function, muscle contract and fluid balance
The renin Angiotensin system (RAAS)
System is triggered by low blood pressure in renal arterioles
juxtaglomerular cells in kidneys release renun
renin converts angiotensiongen (from liver) to Angiotensin I
Angiotensin 1 converts into Angiotensin II
Angiotensin II effects
causes vasoconstriction leading to highblood pressure
stimulates aldosterone increase sodium (Na+) + water absorption
stimulates ADH increasing water reabsorption
stimulates thirst
results: high blood volume AND high blood pressure
Angiotensin II target and role
Role: Active hormone that responds to low blood pressure and a primary stimulus for thirst (dehydration)
Targets:
systemic arterioles
systemic veins
kidney (afferent & efferent arterioles, proximal tubule)
Hypothalamus: Stimulates thirst and provokes behavioral acquisition of water and drinking
Adrenal cortex: Stimulates Aldosterone Secretion (RAAS)
Overall effect:
Increase in blood pressure + maintain kidney filtration
Angiostensin II and systemic blood vessels
causes vasoconstriction of arterioles which increase systemic resistance which causes an increase in blood pressure
venoconstriction equals to increase venous returns and increase blood pressure
Ang II squeezes BOTH pipes, but squeezes the OUT pipe (efferent) to SAVE filtration
Angiotensin II constricting afferent arteriole
Causes decrease in renal plasma flow, glomerular pressure, and GFR
only affected by the SNS
Angiotensin II constricting efferent arteriole
causes a bigger decrease in renal plasma flow, BUT
maintains glomerular pressure prevents GFR from dropping to zero
SUPER IMPORTANT
this helps counteract afferent constriction helping…
maintain glomerular pressure maintain GFR despite low blood floor
without it → GFR could go to zero
Angiotensin II affect on Proximal Tubule
Direct effect: Increases the solute reabsorption esp sodium and other salts
indirect effect: Increase in water reabsorption
Net effect: Rentention of both causing reabsroption of plasma from the filtrate back into the body where its supposed to be (b/c we are already low on volume)
Aldosterone (ALD)
It is a hydrophobic Mineralocorticoid produced in Adrenal Cortex that is stimulated from Angiotensin 2 and high potassium levels (hyperkalemia) BC od dehydration
hypokalemia: not a stimulus for aldosterone
Target: Principal Cells of Distal Tubule
Effects:
- Increase Sodium (Na+) Reabsortion
- Increase Potassium (K+) Secretion (peed away by hyperkalemia)
- Net Solute Reabsorption: Sodium Reabsorption > Potassium Secretion (3 to 2 ratio) 3 sodium out 2 potassium in
also increase absorption in water
Indirect Effect?: water reabsorption
Anti-Diuretic hormone (ADH)
Origin:
Posterior pituitary (extension of hypothalamus)
Stimulus (PRIMARY):
high Plasma osmolarity (detected by hypothalamic osmoreceptors) - Example: Dehydration
→ High osmolarity → ↑ ADH release
Targets: Kidney causing increase in water reabsorption (anti-diuretic hormone) low urine output and no direct solute reabsroption
Results: in low plasma osmolarity and high blood volume
this hormone increases in response to Dehydration
Atrial Natriuretic Peptide/Hormone (ANH)
this hormone is stimulated by too much volume (Hypervolemia) causes body to pee away the sodium causing diuresis (peeing away fluid)
comes from the atria of the heart
chemical structure: peptide
Targets: Kidney and Juxtaglomerular apparatus inhibiting renin secretion (suppresses angiosin 2)
inhibits net solute; inhibiting solute reabsorption (so we dont absorb more volume;water)
indirect affect: diuresis
Atrial Natriuretic Peptide/Hormone (ANH) and blood vessels
causes systemic arterials to vasodilate and if pressure is too high it will decrease arterial pressure increasing capillary pressure
this increases filtration making fluid move out of plasma into the interstitium
Affects the kidneys causing
afferent arteriole vasodilation
increases glomerular pressure, GFR, and filtration fraction ultimately increasing urine formation
ultimately, ↑ urine output
↓ plasma volume
↓ blood pressure
Brain Natriuretic Peptide works similarly (released from ventricles)
During hypervolemia (high ANP), what happens to ADH, Ang II, and Aldosterone?
Atrial Natriuretic Peptide: ↓
Angiotensin II: ↓
Aldosterone: ↓
👉 Because the body is trying to lose fluid, not retain it
Normovolemia (baseline)
Atrial Natriuretic Peptide ADH: normal (baseline)
Angiotesin II: low baseline
Aldosterone: low baseline
Proximal tubule
a very active tubule (due to mass reabsroption of glucose, Na+, Water, nany solutes) and is one of the longest segments that emerges from the glomerulus also reabsrops peptides
secretes plasma - plasma protein
this tube reabsorbs 65% of solutes
pumps sodium outwards by using ATP
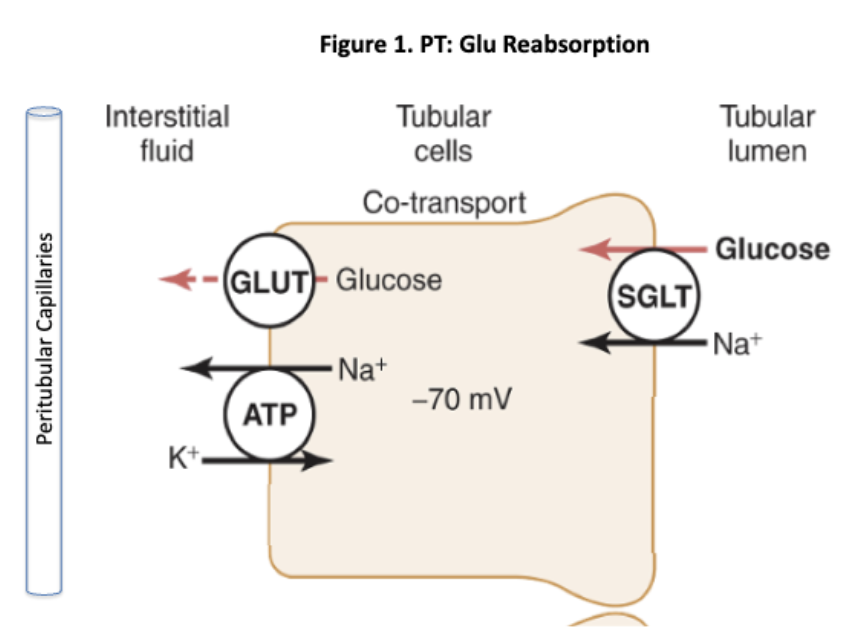
plays in Glucose Reabsorption
1. Basolateral (blood side):
Sodium-Potassium ATPase pumps Na⁺ out
👉 Creates low Na⁺ inside cell
2. Apical (tubule side):
Na⁺ + Glucose symporter (SGLT)
👉 Glucose enters cell using Na⁺ gradient (secondary active transport)
3. Basolateral exit:
GLUT transporter
👉 Glucose leaves cell → blood (facilitated diffusion)
Driven by the Na⁺ gradient created by the Na⁺/K⁺ ATPase
transport maximum (Tm) of glucose
The maximum rate at which glucose transporters can reabsorb glucose
Normally:
Plasma glucose ≈ 90 mg/dL
Glucose is freely filtered
100% reabsorbed in proximal tubule
👉 No glucose in urine
Glycosuria
When plasma glucose exceeds the transport maximum and it cant leep up
the excess glucose stays in filtrate causing diuresis (exretion)
How is glucose reabsorbed
Apical: Na⁺-glucose symport (secondary active transport)
Basolateral: GLUT (facilitated diffusion)
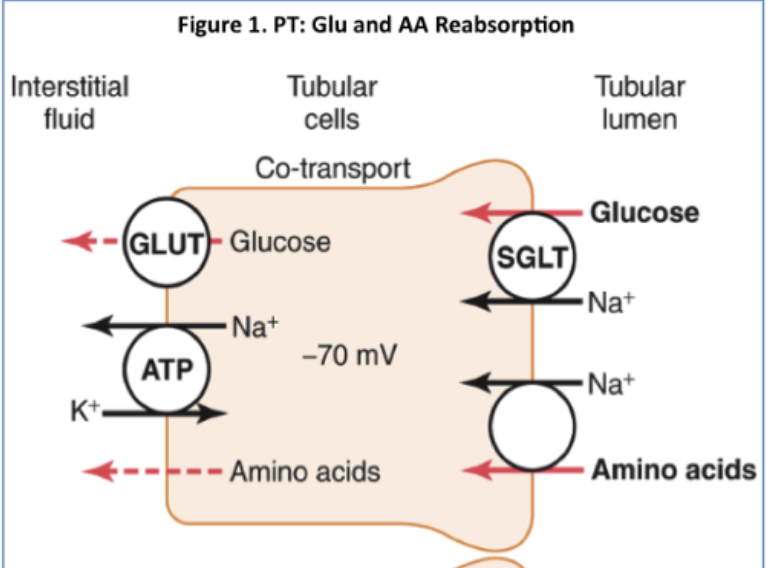
Amino acid reabsorptiomn in proximal tubule
Freely filtered from blood
Apical membrane: Na⁺ + amino acid symport
Basolateral membrane: Facilitated diffusion into blood
Occurs in proximal tubule
Saturatable (has a Tm)
Similar to glucose reabsorption
Protein Reabsorption in the Proximal tubule
1. Apical surface:
Peptidases break peptides → amino acids
2. Small peptides:
Reabsorbed via transcytosis (endocytosis → exocytosis)
Slow and easily saturated
Normally minimal protein in filtrate
Easily saturated because transcytosis is…
slow, energy expensive, not designed for large protein loads
Proteinuria
Due to kidney damage (ex: inflammation) causing increase in protein filtration
reabsroption mechanism becomes overwhelmed/saturated
protein “spills” into urine
Water Reabsorption in the proximal tubule
Promixmal tubule is highly water permeable has aquaforins
moved by osmosis
water follows solutes (esp Na+)
Osmolarity remains at 300 m0sm, so it stays the same solutes are reabsorbed, water follows proportionally
Angiotensin II effects on the Proximal tubule
stimulates and increases Sodium (Na+)/Potassium (K+) ATPase
due to a low volume content, more water will follow by osmosis when Angiotensin is high
increases solutes reabsroption from 99% to 99.9%
Goal: maintain plasma volume = maintain arterial blood pressure minimizing loss of water
majority if waste/toxin secretions occur here + hormones/vitamins and drugs
Many not filtered easily so cannot be excreted by filtration alone
Hypovolemia
Leads to hypertension increasing angiotension II formation
stimulates Na/K ATPase
Increases % sodium reabsorption → more water follows osmotically
Maintains plasma volume = blood pressure
Afferent and efferent arteriolar vasoconstriction
Decreases renal plasma flow and decreased GFR
Hypervolemia
Causes hypertension, drinking too much water can lead to decreased renin secretion compared to regular tonic levels
decreases angiotensin II
Which decreases Na+/water reabsorption: only 98%
Which doubles natriuresis and diuresis
Chronic Hypertension and hypervolemia
Theres a pathology so we treat it with ACE blockers which inhibits ACE enzymes
decreases angiotensin II formation
Increases natriuresis and diuresis
Decrease in plasma volume
Loop of Henle
Thin loop that descends into medulla
composed of descending (thin) and ascending (thick) loop
Concentration gradient increases within deeper medullary interstitium: primarily NaCl and Urea
Up to 1200 m0sm
Descending loop
A thin loop from the loop of henle that is made of simple squamous epithelium
no active transport here
Has a very high water permeability (water is reabsorbed here) but little solute permeability
Surrounding osmolarity increases from 300 to 1200 m0ms/L
Osmosis: filtrate equilibrates with medulla
Bottom of juxtamedullarly loop → filtrate =
Thick Ascending loop
It is not permeable to water (does not have aquaforins)
does not exchange its water with the interstitium
has a double (not single) membrane
Has a lot of solute reabsorption taking place
It is hypertonic: abt 150 m0ms
An active segment
Has a specific transporter:
reabsorbs Na+ out of lumen/for every 2 Cl- (becomes positive luminal charge)
Calcium (Ca+), magnesium (Mg+), Potassium (K+) are reabsorbed too (ON TEST)
This is called Paracellular reabsorption
Effect?
causes further dilution and solute reabsorption only
Decreases osmolarity to 150 mOms
Concentration of filtrate goes down at top of the loop
Causes hypotonic filtrate
Juxtamedullary loop
Maintains medullary gradient
primarily concentrations of urea and Na+/Cl-
are collecting ducts that transit the medulla allowing for potential reabsorption here
Cortical loops
Shallow loops
are collecting ducts that transit the medulla allowing for potential reabsorption here
Early distal tubule
This is the early portion of the Distal tubule
less activity and metabolism compared to the proximal tubule
A unique NaCl transporter for reabsorption
Uses sodium potassium ATPase to drive out sodium
Sodium is accompanied by chloride ion to go in?
1 to 1 ratio of Na and Cl does not create a luminal charge
Target of common diuretic that blocks NaCl ???
Water impereable so abt 100 m0ms
later Distal Tubule
Contains important cells: Principle cells
potassium here is not able to love across membrane making it increase in concetration of the cell
Sodium still moves out and is reabsorbed using ENaC (an apical epithelial sodium channel)
driven by by Basal Na/K ATPase
Ratio of 3 Na/2K+
Net solute reabsorption or secretion????
Further dikutes to 50 mOms bc its water impereable
High aldosterone levels?
Due to increase in angiotensin II and hyperkalenia which decreases in volume pressure and increase in potassium (Na/K ATPase activity) and ENac expression
effect increase Na+ reabsorption and K+ secretion
Effect: we reabsorb more water but still water impermeable
causes hypervolemia
Side effect questions on test
Hyperaldosternoism
Causes edma/swell causing hypoalkemia (due to excess potassium)
increases hypertension due to reabsorpption of too much net solutes
Aldosterone blocker medication helps with hypotentions or hypertension
Side effect is hyperkalenia
Aldosterone effects on Principal cells of distal tubules
blocks the ENaC (channel on apical membrane) which prevents sodium (Na+) from moving in which prevents potassium from being secreted out into the filtrate
effects: prevents net solute reabsroption and water reabsroption
the water and solutes go into the urine
Collecting duct and ADH (testable)
this duct decides how much water you keep based on Aldosterone
it is the final site where water reabsorption is regulated
filtrate passes through the medulla (high osmotic gradient) and has the potential to reabsrob water depending on permeability
permeability depends on aquaporins controlled by high ADH (vasopressin) on the apical membrane
when ADH targets aquaporins it shifts to the apical/luminal membrane (now water can move thru)
What happens if collecting duct is permeable to water
The water moves out of the filtrate into the hyperosmotic medulla (down gradient)
increase of water reabsorption, decrease in urine volume
High ADH effects on collecting duct
increase in aquaporins which increase water reabsorption
leads to a concentrated urine and causes dehydration/high osmolarity
increases solute reabsorption in AL/DT
increase diltute filtrate (50 m0ms/L)
low ADH effects on collecting duct
decrease in aquaporins, decreasing water permeability
water is less reabsorped and so the urine is diluted (overhydration/low osmolarity)
less solute reabsorption in AL/DT
resulting in less dilute filtrate (ex: 150 m0sm/L)
Angiotensin II and Aldosterone effects on Collecting duct
it increases Na+ (solute) reabsorption upstream making medulla more concentrated
this enhances water reabsorption potential in collecting duct
Hypotonic Plasma? (low osmolarity)
Less ADH is releases, meaning less aquporins in collecting duuct
collecting duct is now impermeable to water
causes less water reabsorption
FIltrate is dilute which increase urine output (diuresis)
This is bc….
No ADH = no water reabsorption
👉 Water stays in filtrate → excreted as urine
Aldosterone during normal hydration
the baseline is tonic for ADH secretion
moderate water reabsorption
normal values of ADH = 1-5 pg/mL
urine concentration: ~ 300-900 mOsm
How does alcohol affect ADH
It inhibits ADH from the brain by
decreasing water reabsorption which increases urine output
this is why u wake up with a headache
Turbulogolmerular feedback
feedback starts in the macula dense cells (distal tubule) and communicates with the afferent arteriole
too diluted = bad (not enough Na+ delivered downstream)
later nephrone segments need Na+ to function properly
Too much salt → constrict (slow down)
Too little salt → dilate (speed up)
Works with myogenic mechanism
High NaCl in distal tubule?
Means the filtrate is moving too fast (high GFR)
afferent arteriole constricts, which decreases glomerular pressure and decreases GFR
Low NaCl in Distal Tubule?
means the filtrate is moving too slow (LOW GFR)
Response:
afferent arteriole dilates, increase glomerular pressure and increase in GFR
Main components of acid-base balance
Bicarbonate (HCO₃⁻) = “good” (buffer)
Hydrogen ions (H⁺) = “acid” (bad)
→ Goal: keep H⁺ low and controlled
CO2+H2O↔H2CO3↔H++HCO3−
→ This system allows the body to:
Convert CO₂ into acid (H⁺)
Or buffer acid using bicarbonate
Importance of acid regulation
The body produces more acid than base daily
So it must:
Buffer it (bicarbonate)
Blow it off (lungs)
Excrete it (kidneys)
→ “Breathe CO₂, Pee H⁺, Keep HCO₃⁻”
Lungs → remove CO₂
Kidneys → remove H⁺
Bicarbonate → buffers everything