phys 4
1/59
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
60 Terms
endothelial layer
all vessels have endothelium (1 cell layer thick)
innermost
elastin layer
allows more constriction or dilation
on vein and arteries
smooth mm layer
contracts to shunt blood to correct location under medium pressure
highest in artery, then a little less in arterioles and veins for shunting a ton of blood
fibrous layer
reinforces wall w/ high pressure (artery)
highest in veins and arteries, a little in venules
outermost layer
blood flow
parallel (brain, heart, liver, …)
recondition to keep contents the same in blood
reconditioning organ receive more blood than needed for metab
kidneys, liver, heart
organs vary is tolerability of lowered blood flow (brain has almost no tolerabililty
flow rate
F = Delta P / R
delta P = pressure gradient from heart
pressure diff between beginning and end of vessel
decreases when resistance R increases
R = resistance from friction
blood viscosity
vessel length (longer = more res, does not change)
vessel radius (smaller = more res, changes often dila or constri)
R
radius is biggest determinant of flow rate
increases by factor of 4 each time radius is increased by 1
R = 1/ r^4
r + 1 = F x4
poiseuiles law
F = (3.14 x delta P x r^4) / (8 x n x l)
n = viscosity (# of RBCs)
l = length
Surface area
vessel length and radius
RBCs bumping against the cell wall
extrinsic factors = symp release nor on a1 = constriction
intrinsic = signals from tissue
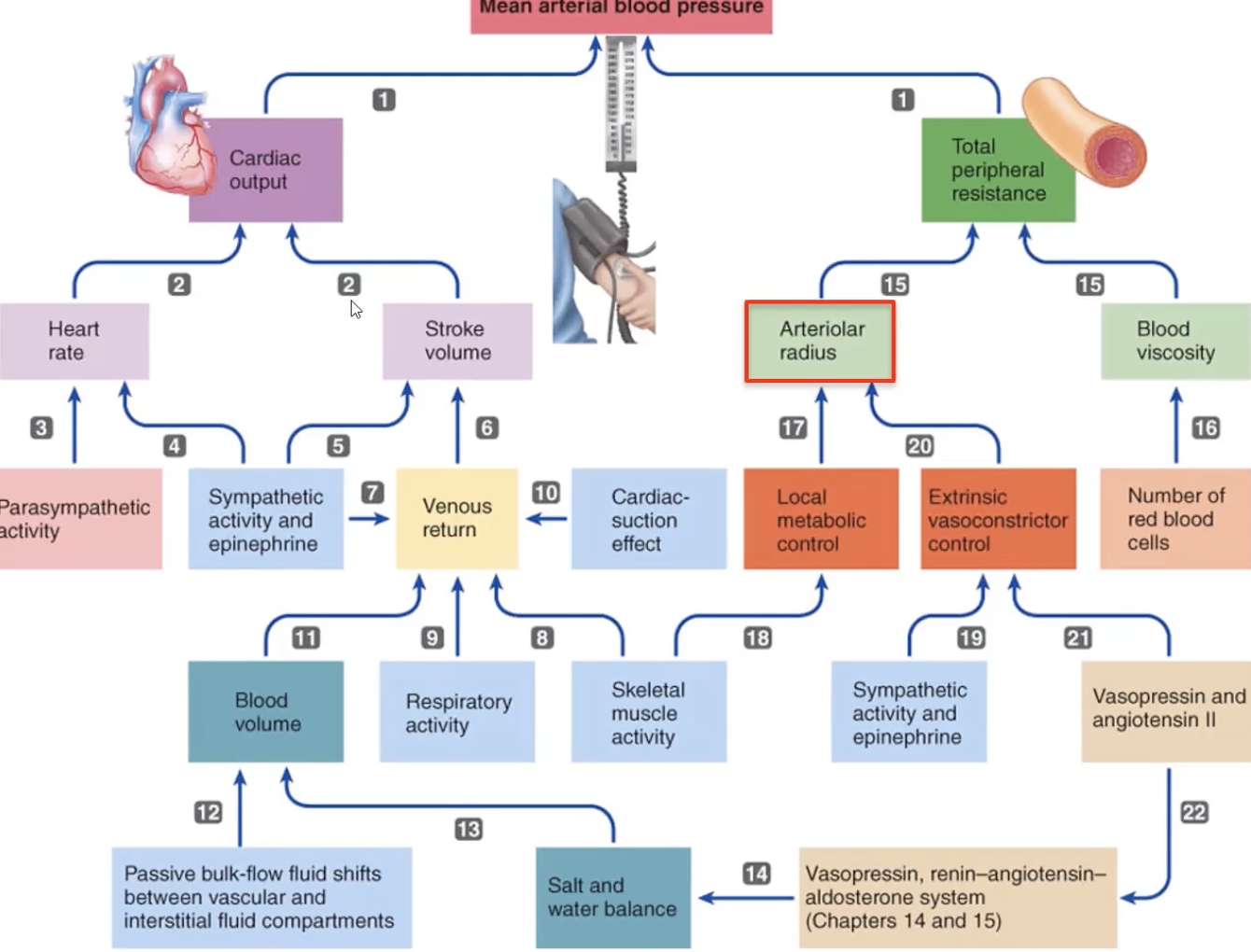
MAP
avg arterial pressure driving blood forward
diastolic + 1/3 pulse pressure
determined by
CO
TPR
volume
formula
CO x TPR (total peripheral resistance)
TPR increases → MAP increases → increased blood flow to specific organ
closer to diastolic pressure
mean systemic pressure
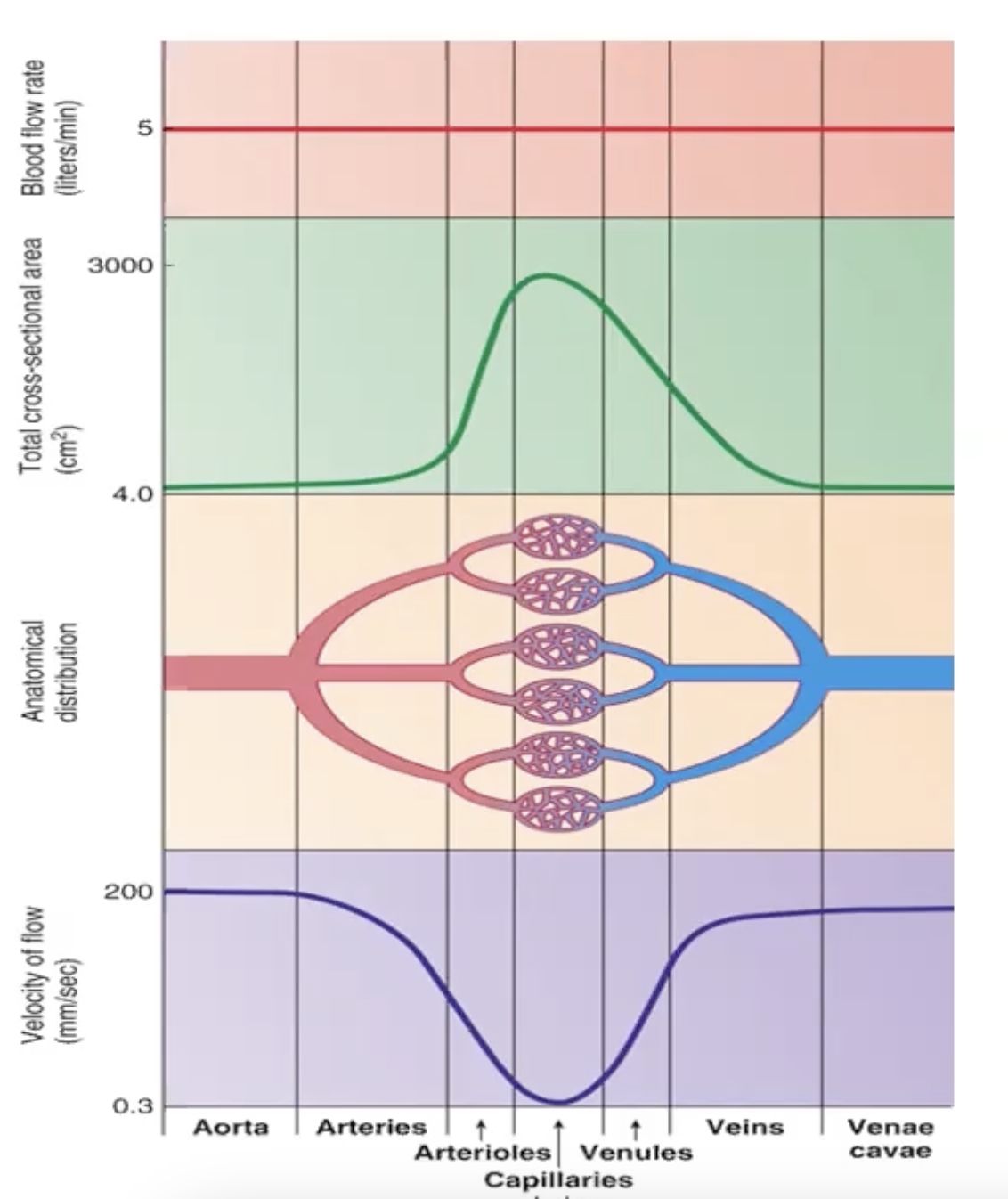
slowly decreases from 95 in aorta to almost 0 in vena cava
pressure on arteriolar side (high)
determined by
CO
SV
total peripheral res / systemic vascular res
less venous compliance = less venous return
central venous pressure
low pressure
systole
peak pressure against walls
1/3 of blood from artery enters arterioles
diastole
minimum pressure on walls
blood draining down vessels (not arteries)
elastic recoil and pressure pushes blood into arterioles
smooth mm
receptor a1
neurotran = epi = speeds up reaching threshold
gap jxns
more actin, no troponin, less SR
actin/myosin arranged in diagonal bundles
unstable resting mem potential → threshold = multiple AP
arteries
large r = little res
aorta has highest pulsing pressure and slowly decreases as it flows outward
elastic recoil sends blood further
pressure reservoir b/c when heart is relaxed and no blood is pumped, blood still flows from driving force from elastin
MAP is 93
arterioles
MAP is 40, largest drop in pressure
converts the pulsing pressure into stable pressure in capillaries
dictates blood flow w/ cons or dil or smooth mm
inn by symp postganglions → inc blood pressure
controlled by
local factors
hormones (nitric oxide = dilation)
mechanical stretch (intrinsic)
vascular tone
constant partial contraction = baseline res
increase/dec pressure as needed
determined by
Ca channels
continuous release of Nor from sym
adrenoreceptors
a1: vasocon
a2: inhibition of nor/Ach in CNS
B1: tachycardia
B2: vasodilation
a1 receptor
increased peripherial res, increased BP
on all tissue except the brain
vasoconstriction
B2 receptor
vasodilation, decreased peripheral res, bronchodilation
activated by epi
mostly in arteriolar smooth mm in coronary arteries, lungs, smooth skeletal mm
vasoconstriction
increased myogenic activity/tonic for ongoing contraction
increased O2
decreased CO2, metabolites
increased endothelin
increased symp vasopressin/angiotensin II
vaso dilation
decreased myogenic activity/tonic for ongoing contraction
decreased O2
increased CO2, metabolites
increased nitric oxide
decreased symp histamine/ heat
capillaries
single layer of endothelial
sphincter = stopcock, since no smooth mm
contraction = reduced flow to organ
relax = increased flow
2 types of passive exchange
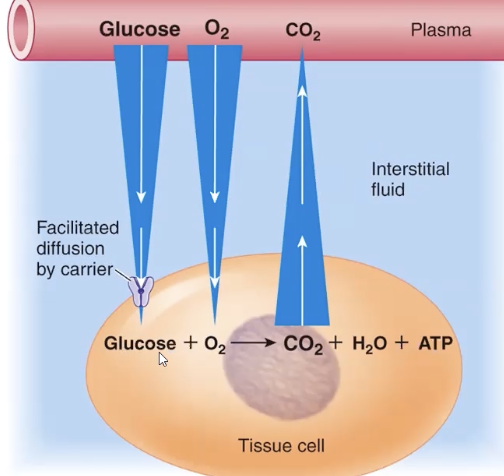
diffusion: CO2 and O2
bulk flow: plasmid fluid
diffusion
cap only regulate plasma protein movement = extent of diffusion is determined by conc gradient
bulk flow
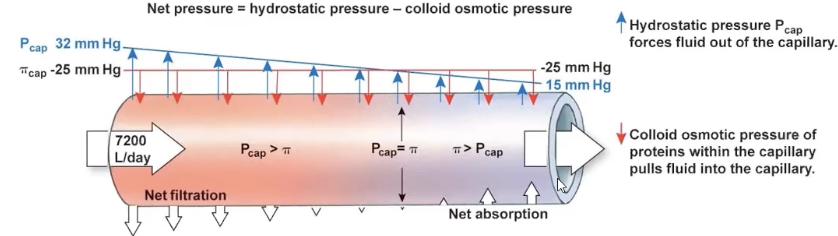
difference of hydrostatic pressure and colloid osmotic pressure
protein free plasma leaks from cap → mixes in ECF → reabsorbed in cap
pressure inside > outside = ultrafiltration/hydrostatic/pushing pressure
proteins are contained in the cap = inward pressure = osmotic/absorbing pressure
capillary flow
total cross sectional area is 750x greater than the aorta
blood slows considerably down to allow for diffusion and transport of glucose through channels
endothelial cells in cap
joined together w/ water filled pores = passage of water soluble substances
Na, K, glucose
lipid soluble pass thorugh lipid bilayer
O2, CO2
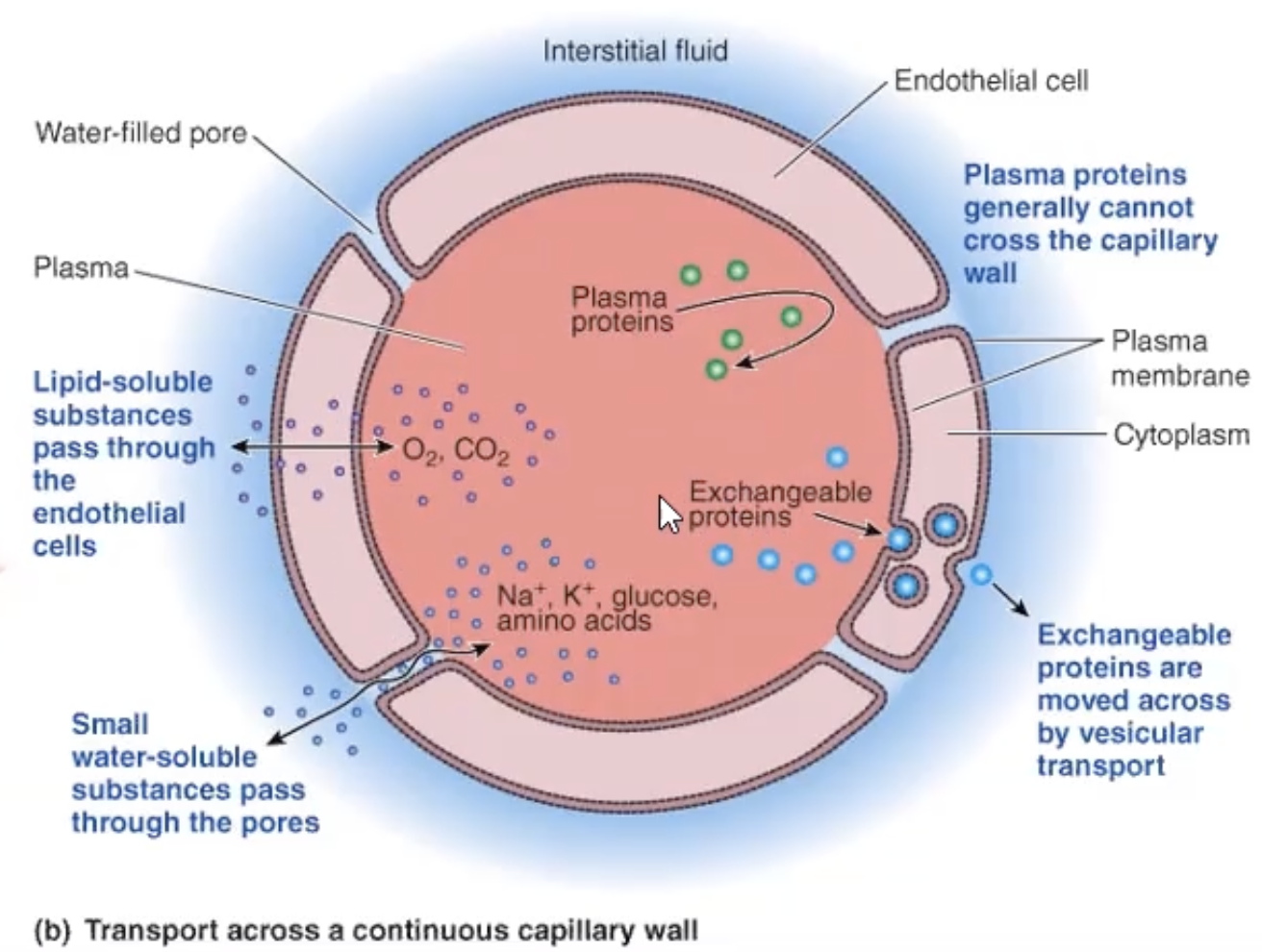
plasma proteins
transport things to organs (hormones)
dont want leaking into endo cells
losing = losing osmolarity
metarteriole
cluster of constricting mm between arteriole and venule
many caps are not open
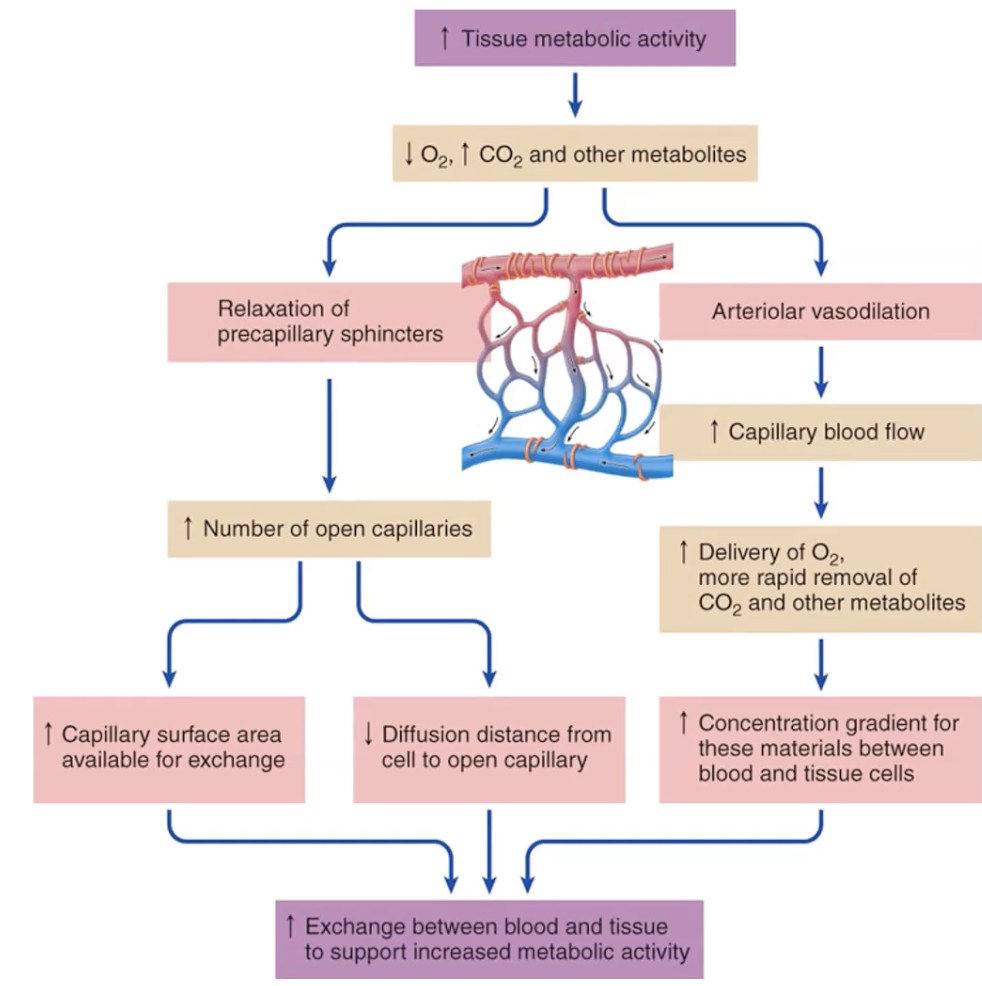
precap sphincter
not inn
sensitive to local and metab changes
high metabolic activity on cap
decrease in O2 = decrease in pH (acidic)
increase in O2 = increased conc gradient
extracellular fluid
20% = plasma
80% = bathes cells
fluid exchange
4 factors that influence movement
cap blood pressure (plasma) push out
plasma colloid osmotic pressure (plasma) push in
interstitial fluid hydrostatic pressure, push in
interstitial fluid colloid osmotic pressure, push out
cap blood pressure (plasma) Pcap
hydrostatic pressure pushing towards the interstitial fluid on cap walls
pushes fluid from cap into interstitial fluid
32 mmHg: higher in arterioles = net filtration
15 mmHg: decreases below colloid osmotic pressure in venules = net absorption
plasma colloid osmotic pressure (plasma) PI p
determined by protein conc in cap
pushes to move fluid into cap
-25 mmHg: remains the same in both arteries and venules (protein conc remain the same)
plasma fluid exchange
decreased plasma vol = decreased capillary BP
decrease in outward pressure = decrease ultrafiltration, increase reabsorption → fluid entering plasma
interstitial fluid hydrostatic pressure P if
pressure of interstitial fluid pushing on outside of vessel
interstitial fluid colloid osmotic pressure PI if
pressure of ISF pushing to leave vessel
very little to no leakage (plasma proteins)
negligible
complete calculation of fluid exchange
net exchange = (Pc + PI if) - (Pif + PI c)
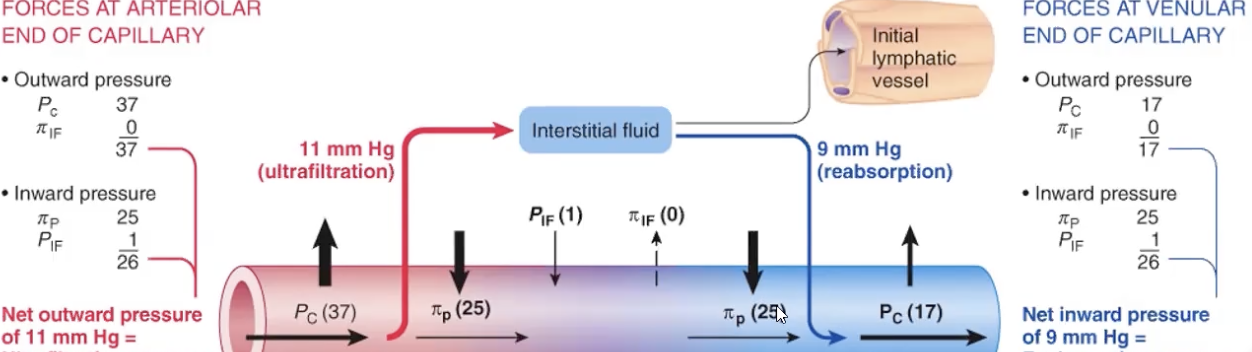
lymphatic sys
picks up excess fluid that was not reabsorbed by 1 way valve
immune fxn : passes lymph nodes on their way to the heart
transport of absorbed fat
return of filtered protein
blind end lymph cap
remove fluid and filtered proteins at dead ends on caps
edema causes
reduced conc of plasma proteins (low osmotic pressure)
increased permeability of capillary wall (plasma pro/fluids escaping)
incresaed venous pressure
lymph vessel blockage
edema solution
easiest = increase ECF hydrostatic pressure or
increase plasmid colloid osmotic pressure → fluid back into cap
veins
blood reservoir
low myogenic tone, low. elasticity, low recoil ability
easily distend w/ small increase in pressure
larger radius = smaller resistance
when reservoir is needed
constrict smooth mm
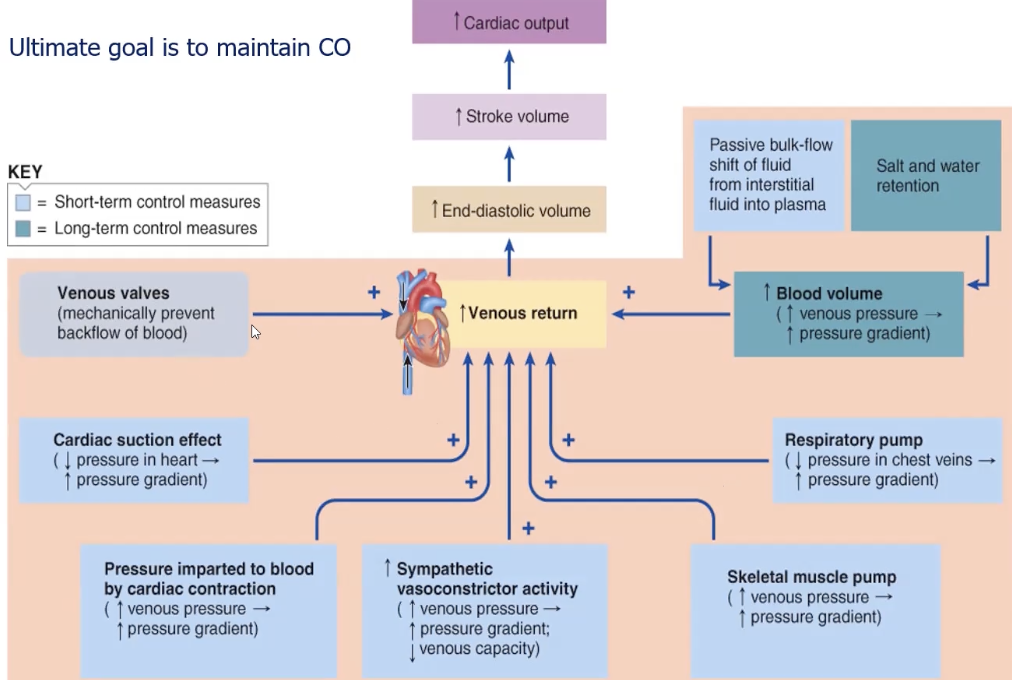
increased venous return
increased CO to heart (starlings law)
venous capacity
depends on
compliance/stretchability of vein walls
influence of external pressure (smooth mm, skeletal mm pump, cardiac pump)
increased symp activity on venous return
decreased venous capacity
more blood pumped out of heart and more pumped back = increased end diastolic volume = increased CO
difference in vasocon flow in A and V
in arteries = restricted flow from higher resistance
in veins = increased flow from decrease in capacity
factors enhancing venous return
cardiac contraction driving pressure
symp induced venous vasoconstriction
skeletal mm activity
venous valves
resp activity
cardiac suction
blood volume : bulk flow return to cap, no edema
cardiac contraction driving pressure
very very small almost negligable
symp induced venous vasoconstriction
nor binds a1 receptors on smooth mm
skeletal mm activity
mm squeezing on skin in intervals along the veins
veins under increased pressure (below heart) = increased capacity = increased blood pooling = decreased CO
venous valves
one way valves to keep blod from falling back
resp activity
pressure in chest is 5 mmHg lower than atmosphere
normal pressure in lower extremities = driving force for movement up
cardiac suction
ventricular contraction pulls on atria = small vacuum = artrial pressure below 0 = driving force for movement into atria
baroreflex
negative feedback that detects arterial stretch
synapses on NTS → CVLM + nAmb → RVLM
if blood pressure drops = no stretch on baroreceptors = no NTS and nAmb stimulus → foot off the break (parasym)
RVLM
rosteroventral lateral medulla
increases symp activity
CVLM
gabaergic → inhibits RVLM → decreases symp activity
nAmb
stims vagus → slows HR