CL- Oxygenation and the eye
1/30
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
31 Terms
what is the partial pressure of oxygen in the cornea when the eye is open
> approx 155mmHg at corneal surface
> same as pp of O2 in air due to cornea’s direct exposure to atmospheric oxygen
what happens when eye is closed?
> pressure can significantly decrease when eye is closed or when wearing CL
> leading to potential corneal hypoxia
Sources of oxygen of epithelium
open eye:
Atmosphere
Closed eye:
Palpebral conjunctiva
Bulbar conjunctiva?
sources of oxygen of stroma?
open eye:
aqueous humour
closed eye:
aquous humour
Sources of oxygen of endothelium in open and closed eye?
Aqueous humour
sources of oxygen of aqueous humour in open and closed eye?
iris vasculature
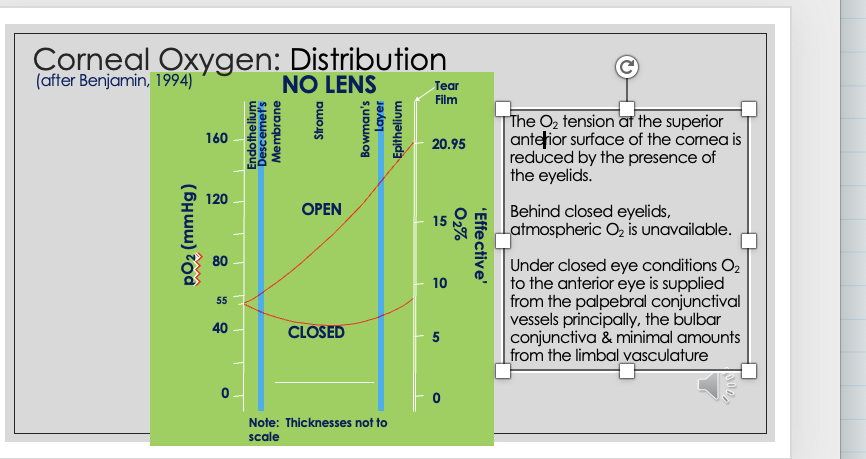
Corneal oxygen distribution with no CL
open eye :
155mmHg O2 available to cornea and drops to 55mHg at endothelium
in closed eye —> less - 55mHg available — eyelid blocks atmospheric O2
endothelium
homeostasis achieved without CL at 55mmHg
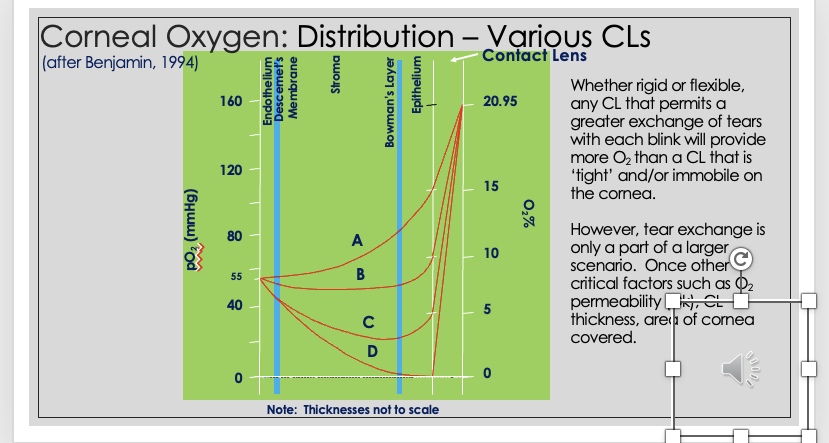
Corneal Oxygen distribution - various CL
CL acts as barrier to O2 diffusion
oxygen has to pass through CL→ Tear film→Cornea
O2 reaching cornea depends on :
O2 permeability of lens
lens thickness
area of cornea covered
O2 permeability equation
intrinsic material property - resistance to gas flow
Permeability P=Dk
D = diffusion coefficient
k= solubility coefficient of O2 in given material
Diffusion and solubility what everybody wants/needs in CL
want material that allows for rapid, direct and unimpeded passage of O2 through material
want material to be extremely high in solubility
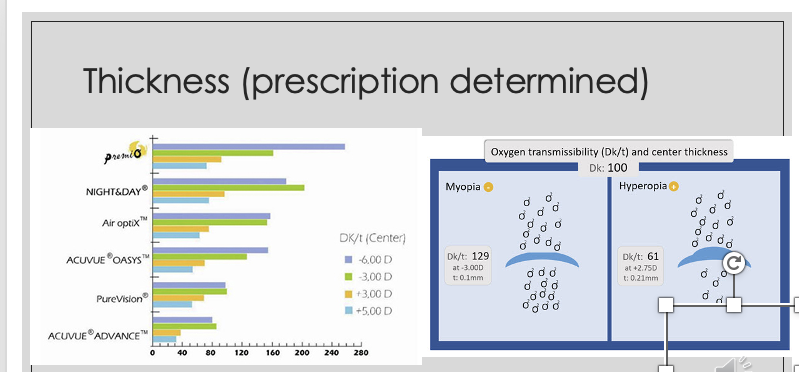
component of transmissibility —> Thickness
myopic lens → thinner in middle
hyperopic lens → thicker in middle
although material has same Dk , thickness influences Dk/t
thinner lens has higher Dk/t
different prescriptions have different Dk/t
When does Dk/t increase?
water content → fixed thickness
when does Dk/t decrease?
thickness - fixed water content
if CL a given thickness and more water → more O2 transmitted - hydrogel lens
when do you get a highest Dk/t
thin, mid-water CLs
what happens if not enough oxygen to eye?
> Hypoxia leading to …
reduction in aerobic glycolysis
lactate accumulation (stroma)
stromal acidosis
osmotic imbalance —> eye will tempt to reduce , eye transports water across membranes to stroma leading to swelling
oedema (swelling) - reduces transparency of eye - vision fuzzy
structural changes if not enough oxygen
epithelial and stromal oedema
decrease transparency
microcysts + vacuoles
striae
folds
endothelial blebs
endothelial polymegathism
vascularisation
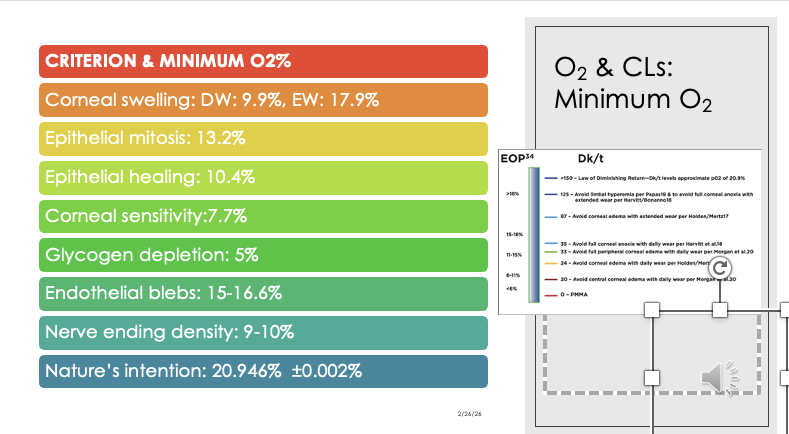
minimum Dk/t
100-120 that gives full oxygenation
at 90 → 5% of cells hypoxic
variability in amount of Dk/t determined to be minimum
silicon hydrogel - super Dk/t , more O2 , in excess
Hydrogel - 18 , very low Dk/t
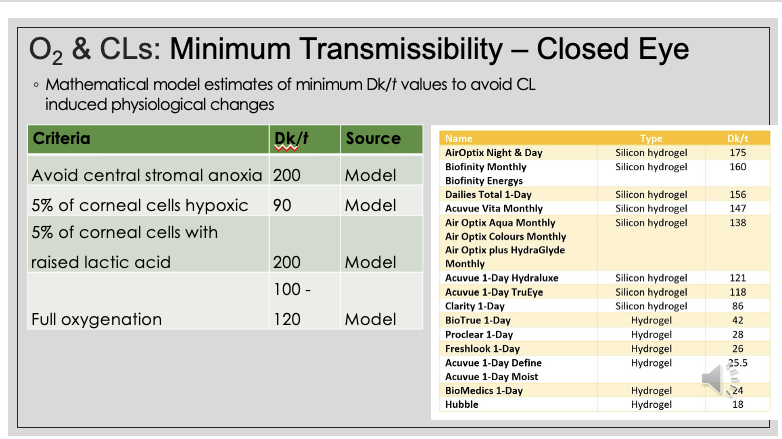
criterion and minimum O2% needed before we see changes in cornea
15-17% endothelial blebs
87 Dk/t → holden/mertz criteria
how are soft contact lenses categorised?
1) Low water, non-ionic
2) High water, non-ionic
3) Low water, ionic
4) High water,ionic
ionic meaning CL
CL with ionic materials have negatively charged surface, which can attract positively charged proteins in tears
Non-ionic meaning CL
CL with non-ionic materials have less reactive surfaces and treated to reduce their negative surface charge
makes them less likely to attract protein deposits
how are low water and high water CL considered?
CL with less than 50% of water content considered low water
CL with more than 50% water content considered high water
what are soft CLs made from and what are the important features they have?
hydrogel or silicone hydrogel material
Features:
comfort, wear time, O2 permeability, Handling (SiHy) easier to insert and remove , Vision
water content of hydrogel lens
hydrogel material extremely flexible(floppy) due to its water content
higher water content = higher Dk/t
Hydrogel most used is poly-HEMA
O2 permeability depends on water content
higher water content , more O2 can pass through lens
Silicone Hydrogel lenses
newer gen of lenses allows approx 5 times more O2 to reach eye than standard hydrogel lens
O2 permeability depends on amount of silicone used , not water content
earliest silicone hydrogel lens treated with coating to improve wettability → affects comfort + dryness of CL
some companies use plasma tx or specific wetting agents → increase hydrophilic properties of lens
Wettability angle
good indication of ability of tears to form stable layer on surface of material
wetting angle of greater than 180 - no wetting , droplets roll of surface of lens
ideally want angle slightly less than 90 → good wetting
Advantages of hydrogel lenses
highly flexible
good initial comfort
thinner lenses
affordable
available in variety of modalities - daily disposable, 2-week, monthly
available in dif designs (sphere, toric, multifocal)
disadvantages of hydrogel lenses
low O2 permeability
potentially higher risk for eye infections and other hypoxia-related issues
not ideal for overnight wear
Advantages of silicone hydrogel
High O2 permeability
easier to handle - new CL wearers
better durability
extended wear + overnight wear options available
available in variety of modalities
available in dif designs
Disadvantages of silicone hydrogel
early silicone hydrogel lenses sometimes had gettability challenges although newer have similar or better gettability than Hydrogel
early SiHy stiffer materials , newer have improved flexibility similar to hydrogels
potentially higher risk of Giant papillary conjunctivitis , newer less of a concern , low modulus monthly
slightly higher price
What materials are eye care practitioners prescribing?
72% soft CL SiHy internationally
majority wearing soft contact lenses - spherical, toric,MF