ICU Drips
1/42
There's no tags or description
Looks like no tags are added yet.
Name | Mastery | Learn | Test | Matching | Spaced | Call with Kai |
|---|
No analytics yet
Send a link to your students to track their progress
43 Terms
What is half-life of a drug?
The half-life of a drug is an estimate of the time it takes for the concentration or amount in the body of that drug to be reduced by exactly one-half (50%).
For example, if 100mg of a drug with a half-life of 60 minutes is taken, the following is estimated:
60 minutes after administration, 50mg remains
120 minutes after administration, 25mg remains
180 minutes after administration, 12.5mg remains
240 minutes after administration, 6.25mg remains
300 minutes after administration, 3.125mg remains.
In theory, after 300 minutes almost 97% of this drug is expected to have been eliminated. Most drugs are considered to have a negligible effect after four-to-five half-lives.
However, this does not mean that won't be detectable, for example, during a drug test. Just that the drug has no effect
Vassopressors
Epinephrine
Norepinephrine/Levophed
Phenylephrine/Neosynephrine Dopamine/Inotropin
Angiotensin II/Giapreza
Vassopressin/Vasostrict
N-PAVED
Sedatives
Lorazepam/Ativan
Propofol/Diprivan
Midazolam/Versed
Dexmedetomidine/Precedex
LM-PD
Antiarrhythmics
Amiodarone/Cordarone
*Diltiazem/Cardizem
Isoproterenol/Isopenaline
Brevibloc/Esmolol
Is a calcium channel blocker that slows heart rate in pts with a-fib, not antiarrythmic
Heart rate controlling medications
Beta blockers (-lol) (slows HR)
-Metroprolol
-Carvedilol
Calcium channel blockers (-ipine) (slow HR & reduce strength of contraction)
-Diltiazem (cardizem)
Digoxin
Heart Rhythm Controlling Medications
Sodium channel blockers
- Lidocaine
- Flecainide (Tambocor®)
- Propafenone (Rythmol®)
- Quinidine (Various)
Potassium channel blockers
- Amiodarone
Vasodilators
Nitroglycerine
Labetolol
Nicardipine/Cardene
Inotropics
- Change the force of contraction of your heart
There are 2 kinds of inotropes:
Given to what kind of patients
Milrinone/Primacor
Dobutamine/Dobutrex
- Positive inotropes strengthen the force of the heartbeat. (cardiomyopathy, CHF, recent MI)
- Negative inotropes weaken the force of the heartbeat and slow HR (HTN, CHF, arrhythmias, chest pain)
Examples of positive and negative Inotropics
Positive Inotropics
- Digoxin
- help the heart pump more blood with fewer heartbeats. This means that although the heart beats less, it also beats with more force to meet the oxygen demands of your body.
Negative
- beta-blockers, calcium channel blockers, and antiarrhythmic medicines
Neuromuscular Block
Nimbex/Cisatracuruim
Analgesic/Sedatives
Ketamine
Fentanyl
What are the two main benzodiazepines used in the ICU?
Lorazepam and midazolam are the two main benzodiazepines used for sedation in the ICU
Propofol is also used very often!
Lorazepam
Type
Use
Dose-Titration
Half-Life
Considerations
Benzodiazepine (Ativan)
Long term sedation and Intermittent therapy
1-8mg/hr infusion
Oral ~ 12 hours/IV ~ 14 hours/IM ~ 13-18 hours
Propylene glycol toxicity (especially with infusion); Delirium;
Preferred benzo in cirrhosis
Used in emergency situations involving seizures
Recommended for sustained sedation of mechanically ventilated
Midazolam
Type
Use
Dose-Titration
Half-Life
Considerations
Benzodiazepine (Versed)
Short term sedation or frequent neuro checks
1-10mg/hr; Titrate by 1mg every 30 minutes
3 hours (2-4)
Accumulates in adipose tissue; Unpredictable elimination; Less hypotension than propofol and dexmedetomidine.
Diprivan
Type
Use
Dose-Titration
Half-Life
Considerations
General anesthetic (Propofol)
Short term sedation or frequent neuro checks
5 mcg/kg/min; Titrate by 5 mcg/kg every 5 minutes . Max 80 mcg/min
used to help you relax or sleep before and during surgery or other medical procedures.
Dexmedetomidine
Type
Use
Dose-Titration
Half-Life
Considerations
Sedative/General anesthetic (Precedex)
Used for sedation of initially intubated and mechanically ventilated patients; Used before, during, and after intubation in mechanically vented patients
Initiate at 0.2 mcg/kg/hr; Titrate by 0.1 mcg/kg/hr every 15 minutes. Max 1.5 mcg/kg/hr
Distribution ~ 6 minutes; Terminal ~ up to 3 hours
Has some analgesic effects; Can cause hypotension and bradycardia; Intended for light sedation; Expensive
Can be used to sedate patient for general surgeries/procedures
Norepinephrine
Type
Use
Dose-Titration
Half-Life
Considerations
Levophed: Alpha/Beta Adrenergic Agonist
Acute hypotension. Sepsis and Septic shock. Preferred vasopressor in most situations.
5 mcg/minute Titrate by 1-5 mcg/minute every 5 minutes to maintain MAP above 65 mm/Hg. Don't exceed 30 mcg/minute
2.4 minute
Notify provider if/when dose reaches 30 mcg/minute. Do not exceed 80 mcg/minute. Maximum doese may be increased with prescriber order. May be especially necessary in obese patients (usual max: 60 mcg/min)
Pitressin
Type
Use
Dose-Titration
Half-Life
Considerations
Synthetic ADH (Vasopressin)
Usually 2nd line add-on to norepinephrine (esp. in septic shock)
0.04 units/min. DO NOT TITRATE.
10 to 20 mins
Should not be used alone initially but can be used alone once catecholamine agent weaned off; higher doses have risk for GI ischemia; is typically not titrated (on or off)
works on V2 receptors stimulating the RAAS system, which increases blood volume, cardiac output, and arterial pressure.
Angiotensin II
Type
Use
Dose-Titration
Half-Life
Considerations
Angiotensin II Agonists (Giapreza)
Septic or Distributive shock
Initiate at 20ng/kg/min. Titrate by 15ng/kg/min every 5 min to maintain MAP above 65mmHg.
< 1 minute
Do not exceed 80ng/kg/min in first 3 hours. After 3 hours, dose should not exceed 40ng/kg/min. Doses as low as 1.25ng/kg/min have been used
Dopamine
Type
Use
Dose-Titration
Half-Life
Considerations
Inotropic Agent (Inotropin)
Hypotension with bradycardia; Shock (cardio/septic)
Initiate infusion at 5mcg/kg/min. Titrate by 2.5mcg/kg/min every 5 min to maintain MAP above 65 mmHg. Do not exceed 20mcg/kg/min
2 minutes
High risk for arrhythmias at high doses; shown to lead to worse outcomes in cardiogenic shock.
Phenylephrine
Type
Use
Dose-Titration
Half-Life
Considerations
Alpha-Adrenergic Agonist (Neosynephrine)
Hypotension with tachycardia and preserved cardiac output; neurogenic shock
Initiate infusion at 40mcg/min. Titrate by 20 mcg/min every 10 mins to maintain MAP above 65 mmHg. Do not exceed 200mcg/min
Alpha phase 5 minutes; Terminal phase 2 to 3 hours
May be preferred in patients with severe tachycardia; provides no inotropic support' max dose may be increased with provider order
Epinephrine
Type
Use
Dose-Titration
Half-Life
Considerations
Alpha/Beta Adrenergic Agonist
Cardiogenic or anaphylactic shock; can be 2nd line agent for septic shock; often used as salvage therapy.
Initiate infusion at 5mcg/min. Titrate by 2.5mcg/min every 5 min to maintain MAP above 65 mmHg. Do not exceed 30mcg/min.
< 5minutes
Least selective vasopressor; reported to cause more GI hypo-perfusion compared to norepinephrine.
Amiodarone
Type
Use
Dose-Titration
Half-Life
Considerations
Antiarrhythmic (Cordarone)
Atrial and ventricular arrhythmias
1mg/min x 6 hrs. Then 0.5mg/min for 18hrs. Half-life: 9-36 days
Extremely long half-life
May cause heart block, bradycardia/hypotension; Hepatotoxicity
Diltiazem
Type
Use
Dose-Titration
Half-Life
Considerations
Calcium Channel Blocker (Cardizem)
Atrial Fibrilation
5mg-15mg/hr
3.4 Hours
Contraindicated in acute decompensated heart failure
Isoproterenol
Type
Use
Dose-Titration
Half-Life
Considerations
Beta 1/Beta 2 Agonist (Isoprenaline)
Mild or transient heart block; cardiogenic shock
If titrating, initiate at 2mcg/min. Titrate by 1mcg/min every 10 min to maintain HR greater than *** bpm. Do not exceed 10mcg/min
2.5 to 5 minutes
Avoid use in patients with distributive shock; may reduce systemic vascular resistance (SVR) further resulting in hemodynamic compromise. Use with caution in patients with cardiovascular disease (eg, coronary artery disease); may increase myocardial oxygen demand resulting in ischemia.
Milrinone
Type
Use
Dose-Titration
Half-Life
Considerations
Inotrope (Primacor)
Heart Failure exacerbation or other myocardial dysfunction (Sepsis, s/p CABG)
0.375-0.75mcg/kg/min
2.3 to 2.4 hours
Can be used in patients receiving beta-blockers; causes more hypotension than dobutamine; should be adjusted for renal dysfunction; can cause thrombocytopenia.
Used with caution in patients with renal dysfunction!
Dobutamine
Type
Use
Dose-Titration
Half-Life
Considerations
Inotrope (Dobutrex)
Heart Failure exacerbation or other myocardial dysfunction (Sepsis, s/p CABG)
2.5mcg-20mcg/kg/min
2 minutes
Should not be used in patients receiving beta-blockers; may cause hypotension (esp. septic patients)
Labetolol
Type
Use
Dose-Titration
Half-Life
Considerations
Beta-Blocker; Antihypertensive
Acute CVA; Aortic Dissection; Hypertensive
Emergency Initiate infusion at 1 mg/min. Titrate by0.5mg/min every 20 min to maintain SBP less than ** mmHg or MAP less than**.
Do not exceed 6mg/min.
5.5 hours
Long half-life titrate slowly to avoid overdose; use with extreme caution in patients with bronchospastic lung disease; contraindicated in acute heart failure
Nitroglycerine
Type
Use
Dose-Titration
Half-Life
Considerations
Vasodilator
Acute Coronary Syndrome; Pulmonary edema
Initiate at 5mcg/min. Titrate by 5mcg/min up to 20mcg/min. Above 20mcg/min, titrate by 10mcg/min every 5 min to maintain SBP less than ** or MAP less than **. Do not exceed 200mcg/min
1 to 4 minutes
Common side effect is headache-titrate slowly to decrease incidence; contraindicated with right ventricular failure
Nicardipine
Type
Use
Dose-Titration
Half-Life
Considerations
Calcium Channel Blocker; Antihypertensive (Cardene)
Acute CVA (pressure control); Hypertensive emergency.
Dosage/Titration (High/Low Dose): Initiate infusion at 5mg/hr. Titrate by 2.5mg every 5 min to maintain SBP less than ** or MAP less than **. Do not exceed 15mg/hr.
3 to 45 minutes; up to 14 hours (with long-term infusion)
Can cause rebound tachycardia; contraindicated in advanced aortic stenosis; commonly accompanied by high infusion rate; peripheral infusion site should be changed every 12 hours.
Ketamine
Type
Use
Dose-Titration
Half-Life
Considerations
General Anesthetic
Analgesia; Procedural sedation
0.2-0.5mg/kg/hr infusion
2.5 hours
Sympathomimetic effects (increase BP/HR). Psychotropic effects; Respiratory depression with high doses; Hypersalivation
Fentanyl
Type
Use
Dose-Titration
Half-Life
Considerations
Analgesic
Analgesia and sedation
Initiate infusion at 25mcg/hr. Titrate by 10mcg/hr every 15 min to maintain CPOT less than ***. Do not exceed 200mcg/hr
2 to 4 hrs
Monitor for respiratory depression, hypotension
Start Pressors early if after adequate fluid resuscitation MAP remains <65 mmHg.
Pressors can be started and continued peripherally until patient is stabilized.
What med should you start with? Which one second?
Start with norepinephrine first.
Consider adding vasopressin or epinephrine next.
Agents that can be used as third pressors: epinephrine, dobutamine, phenylephrine.
Dopamine increases the rates of arrhythmias and should be used judiciously.
Which is most commonly used for neurosurgical or spinal injury?
Phenylephrine
In severe Congestive Heart Failure exacerbations ionotropic agents such as ..... can be used?
In severe Congestive Heart Failure exacerbations ionotropic agents such as Dobutamine and Milnirone can be used, however due to their Beta-2 receptor stimulation, hypotension can worsen and concominant use of norepinephrine may be needed.
Types of shock (6)
Cardiogenic shock (due to heart problems)
eg: heart attack or Heart Failure
Hypovolemic shock (caused by too little blood volume) eg: Heavy external or Internal bleeding or dehydration
Anaphylactic shock (caused by allergic reaction)
Septic shock (due to infections)
Neurogenic shock (caused by damage to the nervous system)
Obstructive shock (caused by something outside of the heart which prevents the heart from pumping enough blood)
What is shock?
Is a life-threatening condition that occurs when the body is not getting enough blood flow.
Lack of blood flow means the cells and organs do not get enough oxygen and nutrients to function properly.
Many organs can be damaged as a result.
Shock requires immediate treatment and can get worse very rapidly.
As many as 1 in 5 people in shock will die from it.
SIRS vs Sepsis vs Severe Sepsis vs Septic Shock
Systemic Inflammatory Response Syndrome (SIRS), need 2/4 positive (NO INFECTION, just inflammatory response!)
a. Leukocytosis (WBC >12,000 ), Leukopenia or (<4,000)
b. Fever >100.4F OR Hypothermia < 96.8F
c. Tachypnea >20 breaths per minute
d. Tachycardia >90bpm
Sepsis: SIRS + Suspected Infection
-Ex: PNA, UTI, cellulitis, abd infection)
Severe Sepsis: Sepsis + Evidence of Organ Dysfunction
Septic Shock: Severe sepsis + hypotension DESPITE adequate resuscitation or Pressor requirement is needed
Septic shock occurs when a bacterial infection causes low blood pressure, widening of the blood vessels (vasodilation) and organ failure.
A wide spread infection that causes organ failure and low blood pressure
Systemic Inflammatory Response Syndrome
Examples of stressors
is an exaggerated defense response from your body to a harmful stressor. It causes severe inflammation throughout your body. This can lead to reversible or irreversible organ failure and even death.
Examples:
Infection
Surgery
Acute (sudden and severe) inflammation
Ischemia (lack of blood flow to an area of your body)
Cancer
Sympathetic nervous system causes
Pupils:
Heart:
Arteries:
Lungs/Airway:
Stomach/Intestine:
Bladder:
Pupil dilation
Increase heart rate
Peripheral arteries constrict
Coronary artery vasodilation
Relax Airways
Inhibit stomach and intestine activity
Relax bladder (decreased urine output)
Increased sweating
Pathways originate from thoracic and lumbar nerves
Two pathways:
Preganglionic nerve secretes ACh --> post ganglionic nerve that secretes NE (ganglion is where synapses of pre/post are)
Preganglionic nerve secrete ACh on Adrenal gland which secretes NE and E into the blood stream
What organ secretes epinephrine and norepinephrine?
The adrenal medulla, the inner part of an adrenal gland secrete epinephrine and norepinephrine directly into the bloodstream and arrive to target organs
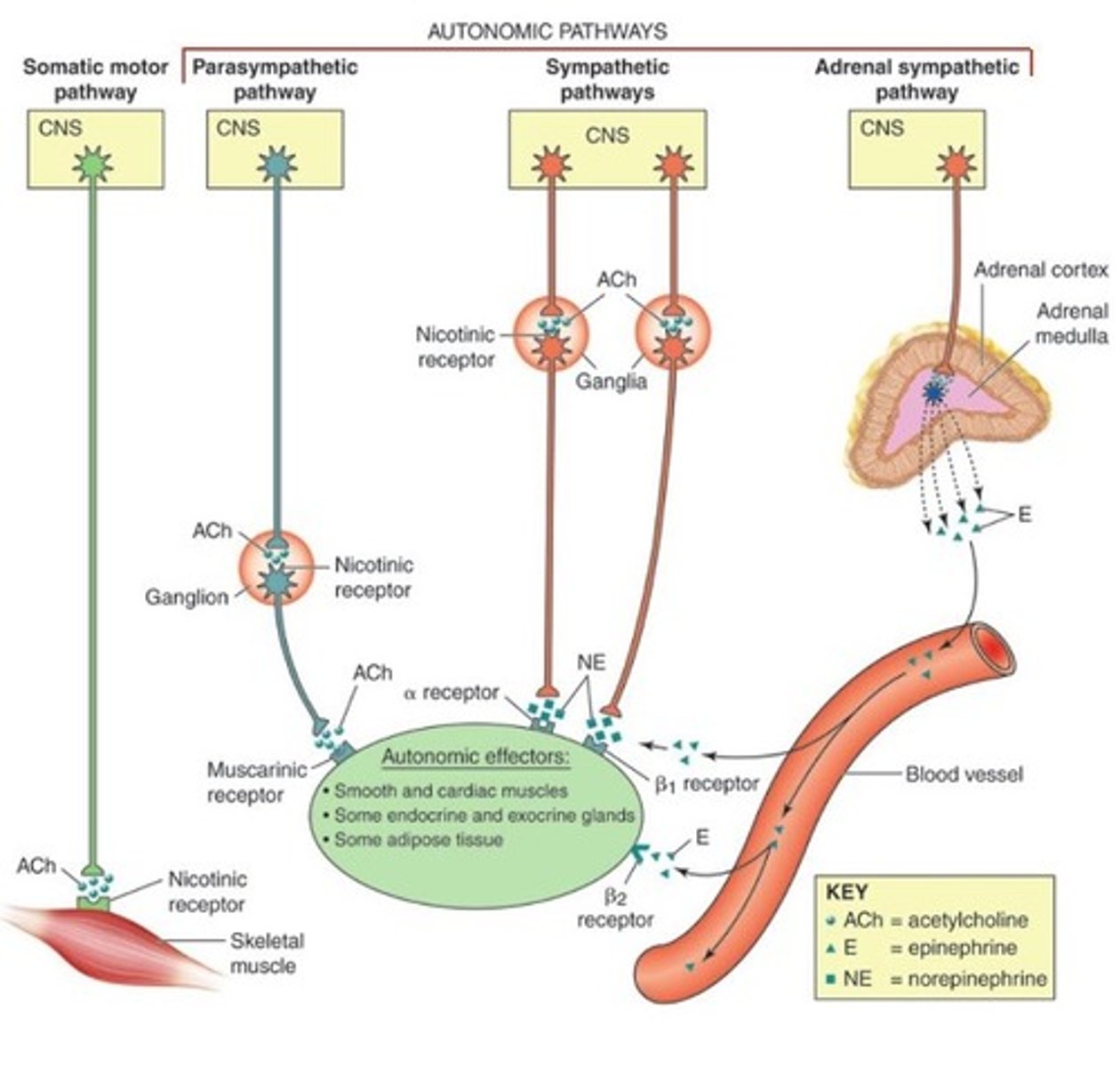
Cholinergic receptors
Adrenergic receptors
two basic categories of receptors associated with the PNS
Cholinergic bind to ACh (2 types)
- Nicotinic (ionotropic=ion channel)
- Muscarinic (metabotrophic= G protein coupled receptor)
Adrenergic bind to NE/E (metabotrophic)
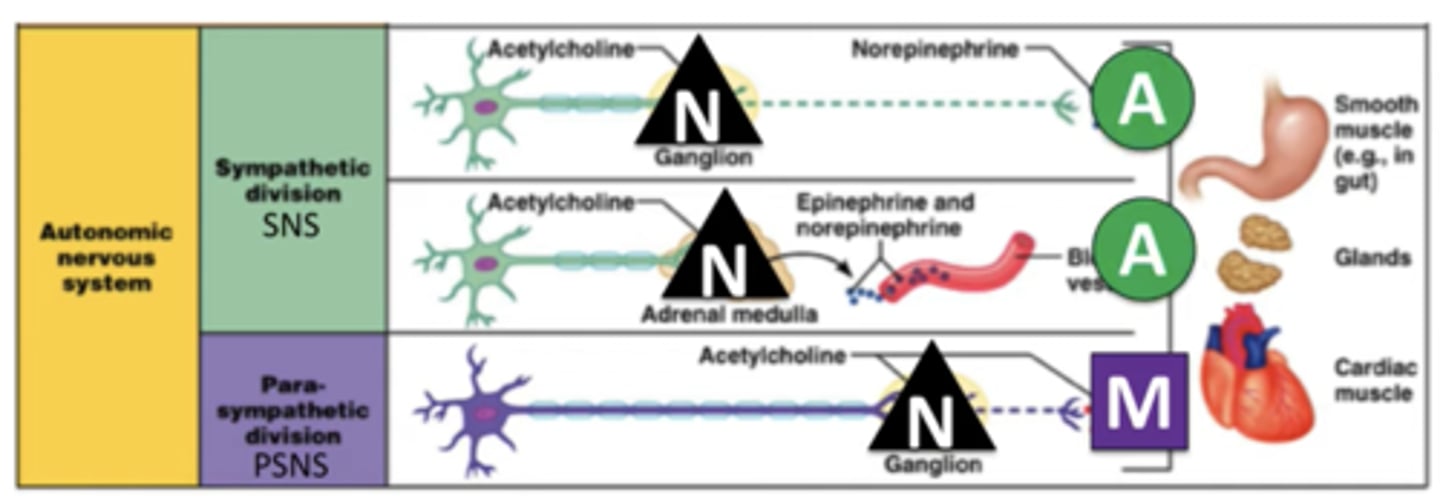
Parasympathetic
Pupils:
Heart:
Arteries:
Lungs/Airway:
Stomach/Intestine:
Bladder:
Pupil constriction
Slow heart rate
Peripheral arteries dilate
Coronary artery vasoconstriction
Constrict airway:
Stimulate activity of Stomach/Intestine
Contract bladder (increased urine output)
Pathways originate from cranial and sacral nerves
One pathway:
Long preganglionic nerve secretes ACh onto post ganglionic nerve which also secretes ACh